Diet Quality among Cancer Survivors and Participants without Cancer: A Population-Based, Cross-Sectional Study in the Atlantic Partnership for Tomorrow’s Health Project



Abstract
1. Introduction
2. Materials and Methods
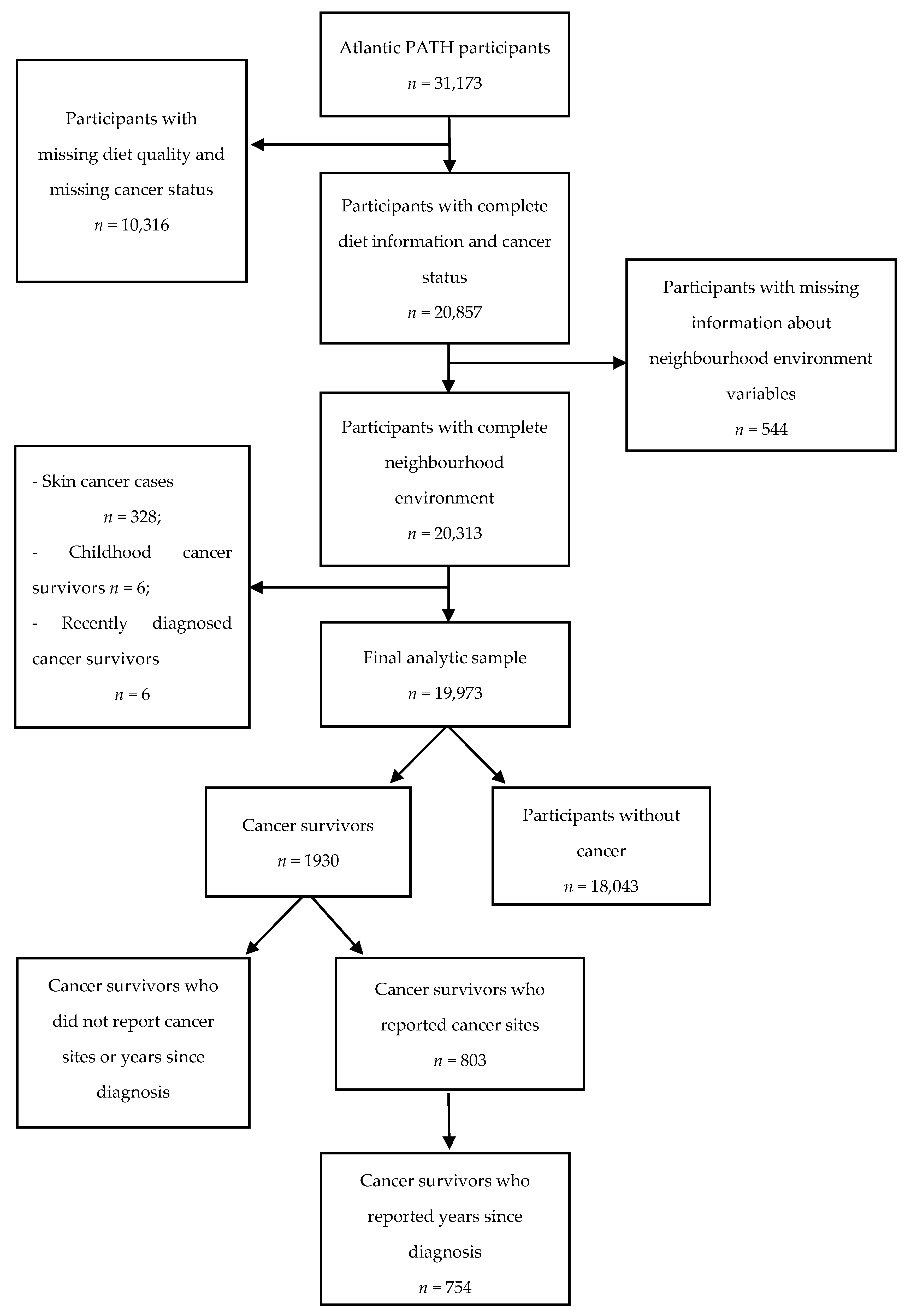
2.1. Study Participants
2.2. Dietary Intake
2.3. Cancer Status
2.4. Covariates
2.5. Statistical Analysis
3. Results
4. Discussion and Implications
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Canadian Cancer Society’s Advisory Committee on Cancer. Canadian Cancer Statistics 2017; Canadian Cancer Society: Toronto, ON, Canada, 2017. [Google Scholar]
- Miller, K.D.; Siegel, R.L.; Lin, C.C.; Mariotto, A.B.; Kramer, J.L.; Rowland, J.H.; Stein, K.D.; Alteri, R.; Jemal, A. Cancer treatment and survivorship statistics, 2016. CA Cancer J. Clin. 2016, 66, 271–289. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, C.; Weir, S.; Rangrej, J.; Krahn, M.D.; Mittmann, N.; Hoch, J.S.; Chan, K.K.W.; Peacock, S. The economic burden of cancer care in Canada: A population-based cost study. CMAJ Open 2018, 6, E1–E10. [Google Scholar] [CrossRef] [PubMed]
- Edwards, B.K.; Noone, A.M.; Mariotto, A.B.; Simard, E.P.; Boscoe, F.P.; Henley, S.J.; Jemal, A.; Cho, H.; Anderson, R.N.; Kohler, B.A.; et al. Annual Report to the Nation on the status of cancer, 1975–2010, featuring prevalence of comorbidity and impact on survival among persons with lung, colorectal, breast, or prostate cancer. Cancer 2014, 120, 1290–1314. [Google Scholar] [CrossRef] [PubMed]
- Sarfati, D.; Koczwara, B.; Jackson, C. The impact of comorbidity on cancer and its treatment. CA Cancer J. Clin. 2016, 66, 337–350. [Google Scholar] [CrossRef] [PubMed]
- Sogaard, M.; Thomsen, R.W.; Bossen, K.S.; Sorensen, H.T.; Norgaard, M. The impact of comorbidity on cancer survival: A review. Clin. Epidemiol. 2013, 5, 3–29. [Google Scholar] [CrossRef]
- Ewer, M.S.; Ewer, S.M. Cardiotoxicity of anticancer treatments: What the cardiologist needs to know. Nat. Rev. Cardiol. 2010, 7, 564–575. [Google Scholar] [CrossRef]
- Demark-Wahnefried, W.; Peterson, B.L.; Winer, E.P.; Marks, L.; Aziz, N.; Marcom, P.K.; Blackwell, K.; Rimer, B.K. Changes in weight, body composition, and factors influencing energy balance among premenopausal breast cancer patients receiving adjuvant chemotherapy. J. Clin. Oncol. 2001, 19, 2381–2389. [Google Scholar] [CrossRef]
- Demark-Wahnefried, W.; Clipp, E.C.; Morey, M.C.; Pieper, C.F.; Sloane, R.; Snyder, D.C.; Cohen, H.J. Lifestyle intervention development study to improve physical function in older adults with cancer: Outcomes from Project LEAD. J. Clin. Oncol. 2006, 24, 3465–3473. [Google Scholar] [CrossRef]
- Cerhan, J.R.; Potter, J.D.; Gilmore, J.M.; Janney, C.A.; Kushi, L.H.; Lazovich, D.; Anderson, K.E.; Sellers, T.A.; Folsom, A.R. Adherence to the AICR cancer prevention recommendations and subsequent morbidity and mortality in the Iowa Women’s Health Study cohort. Cancer Epidemiol. Biomarkers Prev. 2004, 13, 1114–1120. [Google Scholar]
- World Cancer Research Fund/American Institute for Cancer Research. Food Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective; AICR: Washington, DC, USA, 2007. [Google Scholar]
- Rock, C.L.; Doyle, C.; Demark-Wahnefried, W.; Meyerhardt, J.; Courneya, K.S.; Schwartz, A.L.; Bandera, E.V.; Hamilton, K.K.; Grant, B.; McCullough, M.; et al. Nutrition and physical activity guidelines for cancer survivors. CA Cancer J. Clin. 2012, 62, 243–274. [Google Scholar] [CrossRef]
- World Cancer Research Fund International. Food, Nutrition, Physical Activity and the Prevention of Cancer: A Global Perspective: A Summary of the Third Expert Report; World Cancer Research Fund International: Washington, DC, USA, 2018. [Google Scholar]
- Hawkins, N.A.; Smith, T.; Zhao, L.; Rodriguez, J.; Berkowitz, Z.; Stein, K.D. Health-related behavior change after cancer: Results of the American cancer society’s studies of cancer survivors (SCS). J. Cancer Surviv. 2010, 4, 20–32. [Google Scholar] [CrossRef] [PubMed]
- Patterson, R.E.; Neuhouser, M.L.; Hedderson, M.M.; Schwartz, S.M.; Standish, L.J.; Bowen, D.J. Changes in diet, physical activity, and supplement use among adults diagnosed with cancer. J. Am. Diet. Assoc. 2003, 103, 323–328. [Google Scholar] [PubMed]
- DeNysschen, C.; Brown, J.K.; Baker, M.; Wilding, G.; Tetewsky, S.; Cho, M.H.; Dodd, M.J. Healthy Lifestyle Behaviors of Breast Cancer Survivors. Clin. Nurs. Res. 2015, 24, 504–525. [Google Scholar] [CrossRef] [PubMed]
- Potter, J.L.; Collins, C.E.; Brown, L.J.; Hure, A.J. Diet quality of Australian breast cancer survivors: A cross-sectional analysis from the Australian Longitudinal Study on Women’s Health. J. Hum. Nutr. Diet. 2014, 27, 569–576. [Google Scholar] [CrossRef]
- Wang, Z.; McLoone, P.; Morrison, D.S. Diet, exercise, obesity, smoking and alcohol consumption in cancer survivors and the general population: A comparative study of 16 282 individuals. Br. J. Cancer 2015, 112, 572–575. [Google Scholar] [CrossRef]
- Rogers, L.Q.; Courneya, K.S.; Paragi-Gururaja, R.; Markwell, S.J.; Imeokparia, R. Lifestyle behaviors, obesity, and perceived health among men with and without a diagnosis of prostate cancer: A population-based, cross-sectional study. BMC Public Health 2008, 8, 23. [Google Scholar] [CrossRef]
- Nayak, P.; Paxton, R.J.; Holmes, H.; Thanh Nguyen, H.; Elting, L.S. Racial and ethnic differences in health behaviors among cancer survivors. Am. J. Prev. Med. 2015, 48, 729–736. [Google Scholar] [CrossRef]
- Nakamura, S.; Narimatsu, H.; Ito Sasahara, Y.; Sho, R.; Kawasaki, R.; Yamashita, H.; Kubota, I.; Ueno, Y.; Kato, T.; Yoshioka, T.; et al. Health management in cancer survivors: Findings from a population-based prospective cohort study-the Yamagata Study (Takahata). Cancer Sci. 2015, 106, 1607–1615. [Google Scholar] [CrossRef]
- Coups, E.J.; Ostroff, J.S. A population-based estimate of the prevalence of behavioral risk factors among adult cancer survivors and noncancer controls. Prev. Med. 2005, 40, 702–711. [Google Scholar] [CrossRef]
- Eakin, E.G.; Youlden, D.R.; Baade, P.D.; Lawler, S.P.; Reeves, M.M.; Heyworth, J.S.; Fritschi, L. Health behaviors of cancer survivors: Data from an Australian population-based survey. Cancer Causes Control. 2007, 18, 881–894. [Google Scholar] [CrossRef]
- Milliron, B.J.; Vitolins, M.Z.; Tooze, J.A. Usual dietary intake among female breast cancer survivors is not significantly different from women with no cancer history: Results of the National Health and Nutrition Examination Survey, 2003–2006. J. Acad. Nutr. Diet. 2014, 114, 932–937. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.F.; Liu, S.; John, E.M.; Must, A.; Demark-Wahnefried, W. Diet quality of cancer survivors and noncancer individuals: Results from a national survey. Cancer 2015, 121, 4212–4221. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, E.; Cui, Y.; DeClercq, V.; Devichand, P.; Forbes, C.; Grandy, S.; Hicks, J.M.T.; Keats, M.; Parker, L.; Thompson, D.; et al. Cohort Profile: The Atlantic Partnership for Tomorrow’s Health (Atlantic PATH) Study. Int. J. Epidemiol. 2017, 46, 1762–1763. [Google Scholar] [CrossRef] [PubMed]
- DeClercq, V.; Cui, Y.; Forbes, C.; Grandy, S.A.; Keats, M.; Parker, L.; Sweeney, E.; Yu, Z.M.; Dummer, T.J.B. Association between Diet Quality and Adiposity in the Atlantic PATH Cohort. Nutrients 2017, 9, 1155. [Google Scholar] [CrossRef]
- Yu, Z.M.; Parker, L.; Dummer, T.J. Depressive symptoms, diet quality, physical activity, and body composition among populations in Nova Scotia, Canada: Report from the Atlantic Partnership for Tomorrow’s Health. Prev. Med. 2014, 61, 106–113. [Google Scholar] [CrossRef]
- Garriguet, D. Diet quality in Canada. Health Rep. 2009, 20, 41–52. [Google Scholar]
- Jessri, M.; Ng, A.P.; L’Abbe, M.R. Adapting the Healthy Eating Index 2010 for the Canadian Population: Evidence from the Canadian National Nutrition Survey. Nutrients 2017, 9, 910. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- IPAQ Scoring Protocol—International Physical Activity Questionnaire. Available online: https://sites.google.com/site/theipaq/scoring-protocol (accessed on 30 March 2017).
- Statistics Canada. Postal Code Conversion File Plus (PCCF+) Version 6C, August 2015 Postal Codes. 2016. Available online: http://hdl.handle.net/11272/10350 (accessed on 22 July 2018).
- Pampalon, R.; Raymond, G. A deprivation index for health and welfare planning in Quebec. Chronic Dis. Can. 2000, 21, 104–113. [Google Scholar]
- Pampalon, R.; Gamache, P.; Hamel, D.; Institut National de Santé Publique du Québec. The Québec Index of Material and Social Deprivation: Methodological Follow-Up, 1991 through 2006; Institut National de Santé Publique du Québec: Sainte-Foy, QC, Canada, 2011; Available online: http://www.deslibris.ca/ID/229931 (accessed on 1 March 2018).
- Pampalon, R.; Hamel, D.; Gamache, P.; Philibert, M.D.; Raymond, G.; Simpson, A. An area-based material and social deprivation index for public health in Quebec and Canada. Can. J. Public Health 2012, 103 (Suppl. 2), S17–S22. [Google Scholar] [CrossRef]
- Buuren, S.; van Groothuis-Oudshoorn, K. mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45. [Google Scholar] [CrossRef]
- Graham, J.W. Missing Data: Analysis and Design; Statistics for Social and Behavioral Sciences; Springer: New York, NY, USA, 2012; Available online: http://www.springer.com/gp/book/9781461440178 (accessed on 22 June 2018).
- Hox, J.J. Multilevel Analysis: Techniques and Applications; Mahwah, N.J., Ed.; Quantitative Methodology Series; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2002; 304p. [Google Scholar]
- Budtz-Jorgensen, E.; Keiding, N.; Grandjean, P.; Weihe, P. Confounder selection in environmental epidemiology: Assessment of health effects of prenatal mercury exposure. Ann. Epidemiol. 2007, 17, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Gibson, T.M.; Park, Y.; Robien, K.; Shiels, M.S.; Black, A.; Sampson, J.N.; Purdue, M.P.; Freeman, L.E.; Andreotti, G.; Weinstein, S.J.; et al. Body mass index and risk of second obesity-associated cancers after colorectal cancer: A pooled analysis of prospective cohort studies. J. Clin. Oncol. 2014, 32, 4004–4011. [Google Scholar] [CrossRef] [PubMed]
- Lewis, C.M.; Wolf, W.A.; Xun, P.; Sandler, R.S.; He, K. Racial differences in dietary changes and quality of life after a colorectal cancer diagnosis: A follow-up of the Study of Outcomes in Colorectal Cancer Survivors cohort. Am. J. Clin. Nutr. 2016, 103, 1523–1530. [Google Scholar] [CrossRef]
- Koutoukidis, D.A.; Beeken, R.J.; Lopes, S.; Knobf, M.T.; Lanceley, A. Attitudes, challenges and needs about diet and physical activity in endometrial cancer survivors: A qualitative study. Eur. J. Cancer Care (Engl.) 2017, 26. [Google Scholar] [CrossRef]
- Wayne, S.J.; Baumgartner, K.; Baumgartner, R.N.; Bernstein, L.; Bowen, D.J.; Ballard-Barbash, R. Diet quality is directly associated with quality of life in breast cancer survivors. Breast Cancer Res. Treat. 2006, 96, 227–232. [Google Scholar] [CrossRef]
- Canadian Cancer Society. Prostate Cancer Statistics. 2017. Available online: http://www.cancer.ca/en/cancer-information/cancer-type/prostate/statistics/?region=bc (accessed on 4 May 2017).
- Keating, N.L.; O’Malley, A.; Freedland, S.J.; Smith, M.R. Diabetes and cardiovascular disease during androgen deprivation therapy: Observational study of veterans with prostate cancer. J. Natl. Cancer Inst. 2012, 104, 1518–1523. [Google Scholar] [CrossRef]
- Jessri, M.; Lou, W.Y.; L’Abbe, M.R. Evaluation of different methods to handle misreporting in obesity research: Evidence from the Canadian national nutrition survey. Br. J. Nutr. 2016, 115, 147–159. [Google Scholar] [CrossRef]


{kind=link}
| Low-to-Intermediate Diet Quality | High Diet Quality | p-Value | |
|---|---|---|---|
| N = 14,965 N (%) | N = 5008 N (%) | ||
| Cancer survivor | 0.36 | ||
| Yes | 1429 (9.55) | 501 (10.0) | |
| No | 13,536 (90.5) | 4507 (90.0) | |
| Age group, N (%) | <0.001 | ||
| 35–39 | 1440 (9.62) | 567 (11.3) | |
| 40–44 | 1698 (11.4) | 671 (13.4) | |
| 45–49 | 2199 (14.7) | 857 (17.1) | |
| 50–54 | 2692 (18.0) | 857 (17.1) | |
| 55–59 | 2788 (18.6) | 820 (16.4) | |
| 60–64 | 2534 (16.9) | 788 (15.7) | |
| 65–69 | 1614 (10.8) | 448 (8.95) | |
| Sex | <0.001 | ||
| Female | 9705 (64.9) | 4092 (81.7) | |
| Male | 5260 (35.2) | 916 (18.3) | |
| Marital status | 0.97 | ||
| Living without partners | 2856 (19.1) | 960 (19.2) | |
| Living with partners | 12,077 (80.7) | 4038 (80.6) | |
| Missing | 32 (0.2) | 10 (0.2) | |
| Ethnicity | 0.08 | ||
| White | 13,006 (86.9) | 4412 (88.1) | |
| Non-white | 975 (6.52) | 304 (6.07) | |
| Missing | 984 (6.58) | 292 (5.83) | |
| Household income | <0.001 | ||
| 0–24,999 | 679 (4.54) | 173 (3.45) | |
| 25,000–49,999 | 2483 (16.6) | 730 (14.6) | |
| 50,000–74,999 | 3057 (20.4) | 916 (18.3) | |
| 75,000–149,999 | 6109 (40.8) | 2193 (43.8) | |
| >150,000 | 1784 (11.9) | 711 (14.2) | |
| Missing | 853 (5.70) | 285 (5.69) | |
| Education | <0.001 | ||
| ≤high school | 3140 (21.0) | 696 (13.9) | |
| college | 6182 (41.3) | 1913 (38.2) | |
| ≥Bachelor’s degree | 5585 (37.3) | 2390 (47.7) | |
| Missing | 58 (0.39) | 9 (0.18) | |
| Smoking status ‡ | <0.001 | ||
| Never | 7319 (48.9) | 2748 (54.9) | |
| Former | 5894 (39.4) | 1881 (37.6) | |
| Occasional | 380 (2.54) | 120 (2.40) | |
| Regular | 1243 (8.31) | 217 (4.33) | |
| Missing | 129 (0.86) | 42 (0.84) | |
| Alcohol consumption § | <0.001 | ||
| Abstainer | 646 (4.32) | 184 (3.67) | |
| Former drinker | 1048 (7.00) | 284 (5.67) | |
| Occasional drinker | 6134 (41.0) | 2145 (42.8) | |
| Regular drinker | 4592 (30.7) | 1662 (33.2) | |
| Habitual drinker | 2456 (16.4) | 714 (14.3) | |
| Missing | 89 (0.59) | 19 (0.38) | |
| Physical activity | <0.001 | ||
| Low | 3338 (22.3) | 641 (12.8) | |
| Moderate | 4482 (30.0) | 1394 (27.8) | |
| High | 6511 (43.5) | 2785 (55.6) | |
| Missing | 634 (4.24) | 188 (3.75) | |
| BMI | <0.001 | ||
| Normal | 2825 (18.9) | 1169 (23.3) | |
| Underweight | 55 (0.37) | 22 (0.44) | |
| Overweight | 3725 (24.9) | 1197 (23.9) | |
| Obese | 2975 (19.9) | 972 (19.4) | |
| Missing | 5385 (36.0) | 1648 (32.9) | |
| Diabetes | 0.90 | ||
| Yes | 749 (5.01) | 249 (4.97) | |
| No | 14068 (94.0) | 4713 (94.1) | |
| Missing | 148 (0.99) | 46 (0.92) | |
| Myocardial infarction | 0.01 | ||
| Yes | 288 (1.92) | 65 (1.30) | |
| No | 14,577 (97.4) | 4912 (98.1) | |
| Missing | 100 (0.67) | 31 (0.62) | |
| Urbanicity | 0.03 | ||
| Urban | 10,689 (71.4) | 3658 (73.0) | |
| Rural | 4276 (28.6) | 1350 (27.0) | |
| Province | <0.001 | ||
| NL | 1993 (13.3) | 519 (10.4) | |
| PEI | 290 (1.94) | 87 (1.74) | |
| NS | 9394 (62.8) | 3177 (63.4) | |
| NB | 3288 (22.0) | 1225 (24.5) | |
| Social deprivation | 0.14 | ||
| Low | 5407 (36.1) | 1880 (37.5) | |
| Intermediate | 4944 (33.0) | 1646 (32.9) | |
| High | 4614 (30.8) | 1482 (29.6) | |
| Material deprivation | 0.003 | ||
| Low | 6705 (44.8) | 2371 (47.3) | |
| Intermediate | 4793 (32.0) | 1572 (31.4) | |
| High | 3467 (23.2) | 1065 (21.3) | |
| Population density | 0.12 | ||
| Low | 4144 (27.7) | 1375 (27.5) | |
| Intermediate | 4912 (32.8) | 1720 (34.4) | |
| High | 5909 (39.5) | 1913 (38.2) |
| N | Mean (SD) | Mean Difference (95% CI) | OR (95% CI) | |||
|---|---|---|---|---|---|---|
| Model 1 | Model 2a | Model 1 | Model 2b | |||
| Cancer status | ||||||
| Non-cancer | 18,043 | 38.9 (8.63) | reference | reference | reference | reference |
| Cancer survivors | 1930 | 39.1 (8.82) | 0.34 (−0.06, 0.75) | 0.45 (0.07, 0.84) * | 1.05 (0.95, 1.17) | 1.08 (0.97, 1.21) |
| N | Mean (SD) | Mean Difference (95% CI) | OR (95% CI) | |||
|---|---|---|---|---|---|---|
| Model 1 | Model 2a | Model 1 | Model 2b | |||
| Females | ||||||
| Cancer status/site | ||||||
| Non-cancer | 12,393 | 40.0 (8.26) | Reference | Reference | Reference | Reference |
| Breast | 226 | 41.2 (7.49) | 1.13 (0.04, 2.22) * | 1.52 (0.47, 2.57) * | 1.24 (0.94, 1.64) | 1.42 (1.06, 1.90) * |
| Cervical | 129 | 39.3 (8.57) | −0.62 (−2.05, 0.80) | −0.31 (−1.69, 1.07) | 0.80 (0.54, 1.20) | 0.86 (0.57, 1.30) |
| Colorectal | 39 | 40.0 (7.42) | 0.13 −2.45, 2.72) | 0.84 (−1.65, 3.33) | 0.84 (0.41, 1.74) | 1.05 (0.50, 2.19) |
| Thyroid | 39 | 42.0 (7.34) | 1.93 (−0.66, 4.51) | 1.87 (−0.62, 4.36) | 1.65 (0.87, 3.13) | 1.72 (0.89, 3.31) |
| Uterine | 34 | 41.0 (8.50) | 1.24 (−1.53, 4.01) | 1.56 (−1.11, 4.24) | 0.76 (0.34, 1.69) | 0.85 (0.38, 1.92) |
| Males | ||||||
| Non-cancer | 5650 | 36.0 (8.79) | Reference | Reference | Reference | Reference |
| Prostate | 65 | 36.2 (7.57) | 0.17 (−1.97, 2.32) | 0.38 (−1.72, 2.48) | 0.80 (0.38, 1.69) | 0.82 (0.39, 1.76) |
| N | Mean Diet Quality (SD) | Mean Difference (95% CI) | OR (95% CI) | |||
|---|---|---|---|---|---|---|
| Model 1 | Model 2a | Model 1 | Model 2b | |||
| Years since cancer diagnosis | ||||||
| >10 years | 286 | 39.4 (8.49) | Reference | Reference | Reference | Reference |
| >5 years ≤10 years | 181 | 39.5 (7.83) | 0.04 (−1.50, 1.57) | 0.34 (−1.08, 1.76) | 0.99 (0.64, 1.53) | 1.11 (0.71, 1.73) |
| >2 years ≤5 years | 166 | 39.5 (8.24) | 0.06 (−1.52, 1.64) | 0.83 (−0.62, 2.28) | 1.26 (0.82, 1.93) | 1.45 (0.94, 2.26) |
| ≤2 years | 121 | 39.9 (8.34) | 0.43 (−1.32, 2.18) | 1.95 (0.32, 3.59) * | 1.36 (0.85, 2.18) | 1.71 (1.05, 2.80) * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gu, Q.; Dummer, T.B.J.; Spinelli, J.J.; Murphy, R.A. Diet Quality among Cancer Survivors and Participants without Cancer: A Population-Based, Cross-Sectional Study in the Atlantic Partnership for Tomorrow’s Health Project. Nutrients 2019, 11, 3027. https://doi.org/10.3390/nu11123027
Gu Q, Dummer TBJ, Spinelli JJ, Murphy RA. Diet Quality among Cancer Survivors and Participants without Cancer: A Population-Based, Cross-Sectional Study in the Atlantic Partnership for Tomorrow’s Health Project. Nutrients. 2019; 11(12):3027. https://doi.org/10.3390/nu11123027
Chicago/Turabian StyleGu, Qianqian, Trevor B. J. Dummer, John J. Spinelli, and Rachel A. Murphy. 2019. "Diet Quality among Cancer Survivors and Participants without Cancer: A Population-Based, Cross-Sectional Study in the Atlantic Partnership for Tomorrow’s Health Project" Nutrients 11, no. 12: 3027. https://doi.org/10.3390/nu11123027
APA StyleGu, Q., Dummer, T. B. J., Spinelli, J. J., & Murphy, R. A. (2019). Diet Quality among Cancer Survivors and Participants without Cancer: A Population-Based, Cross-Sectional Study in the Atlantic Partnership for Tomorrow’s Health Project. Nutrients, 11(12), 3027. https://doi.org/10.3390/nu11123027