Beneficial Effects of Leucine Supplementation on Criteria for Sarcopenia: A Systematic Review



Abstract
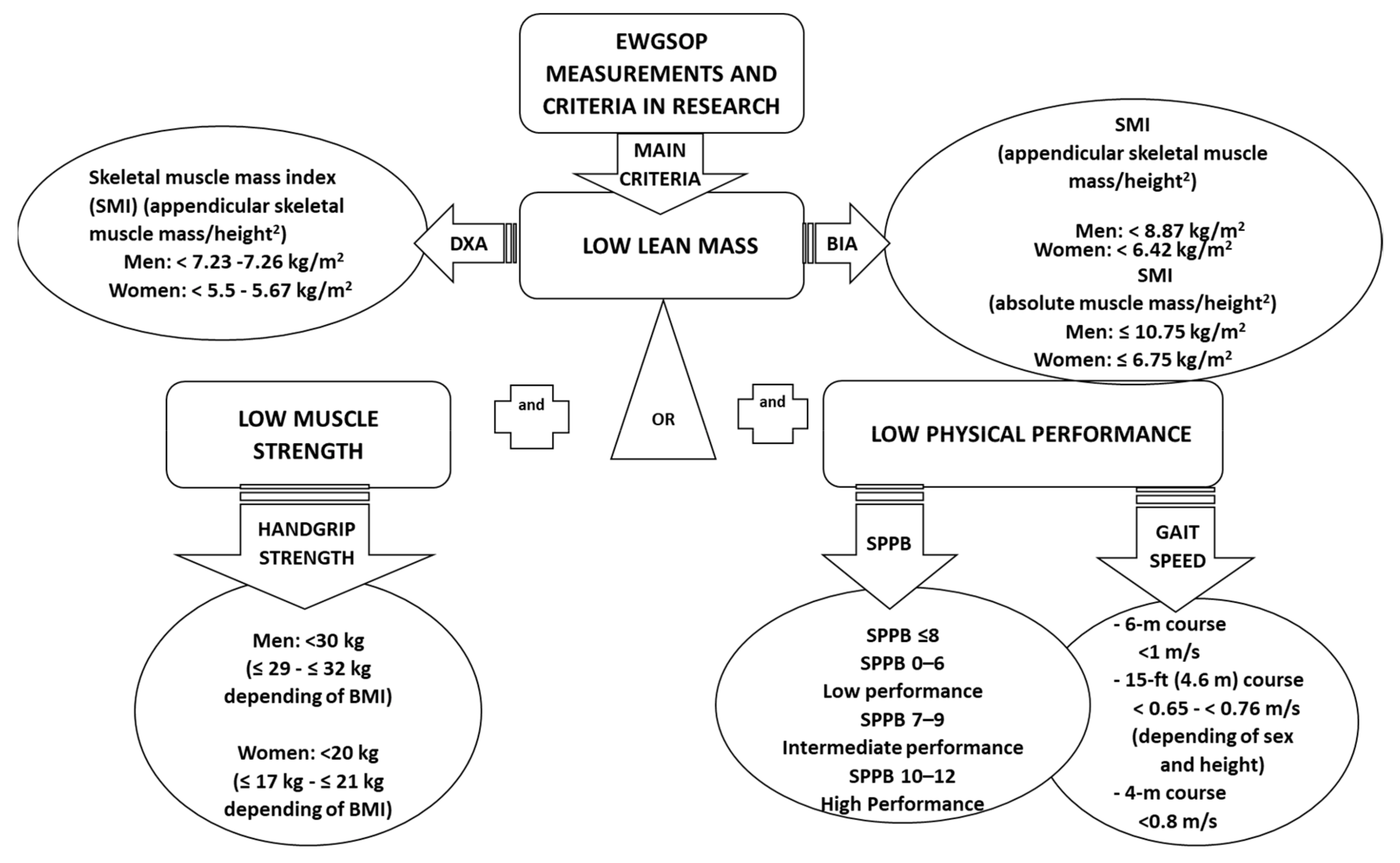
1. Introduction
2. Materials and Methods
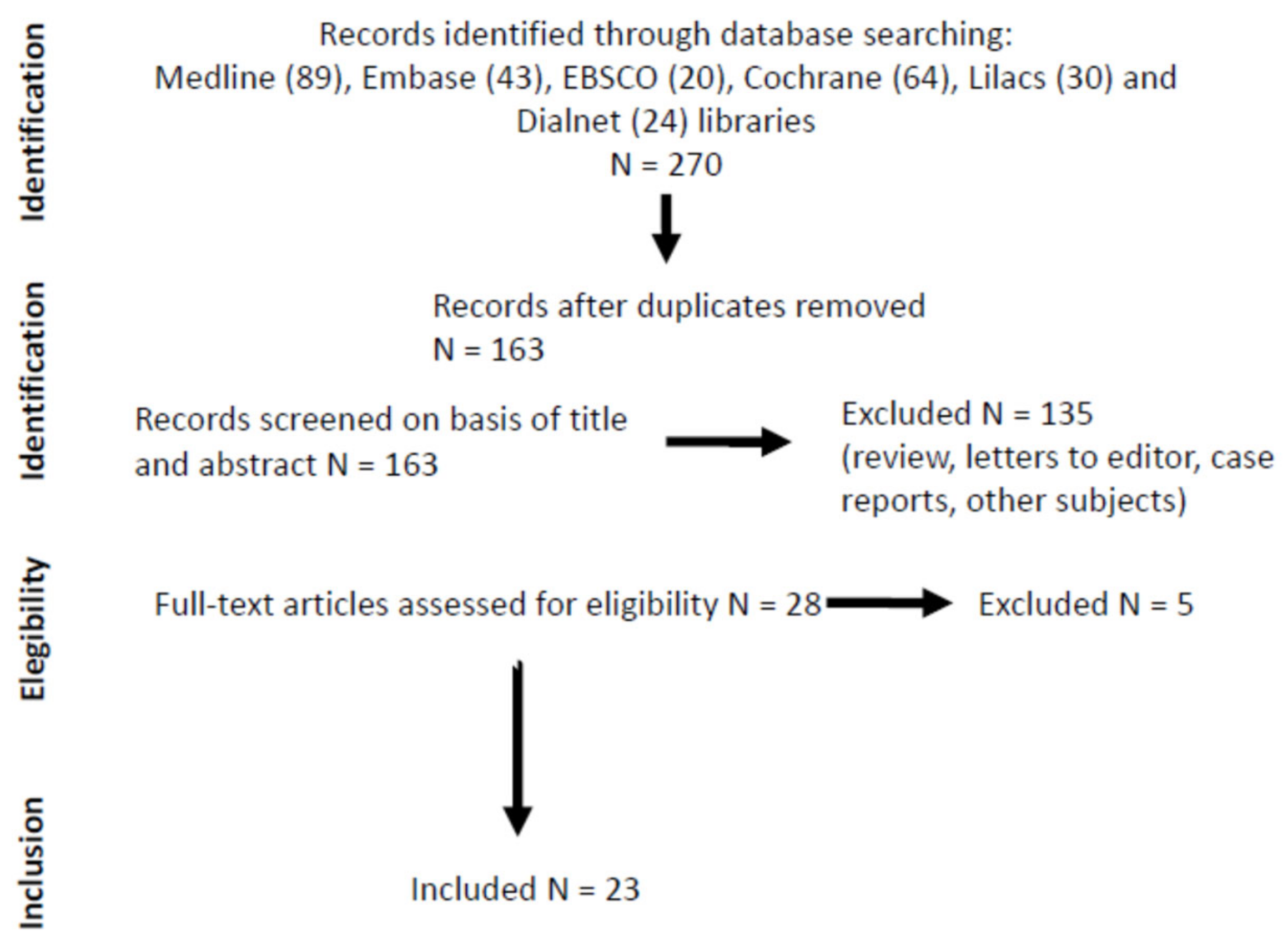
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection and Analysis
2.4. Assessment of Bias
3. Results
3.1. Summary of Identified Publications
3.2. Effect of Leucine Supplementation on Three Sarcopenia Criteria
3.3. Administration, Dose, Duration, and Safety of Leucine Supplementation
3.4. Analysis of Moderating Factors and Subgroups
3.5. The Effects of Leucine Supplementation on Secondary Outcomes
3.6. Bias Risk-Evaluation in Randomised Controlled Trials
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I. The epidemiology of sarcopenia. Clin. Geriatr. Med. 2011, 27, 355–363. [Google Scholar] [CrossRef]
- Tieland, M.; Trouwborst, I.; Clark, B.C. Skeletal muscle performance and ageing. J. Cachexia Sarcopenia Muscle 2018, 9, 3–19. [Google Scholar] [CrossRef] [PubMed]
- von Haehling, S.; Morley, J.E.; Anker, S.D. An overview of sarcopenia: Facts and numbers on prevalence and clinical impact. J. Cachexia Sarcopenia Muscle 2010, 1, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Kang, S.H.; Kim, M.Y.; Baik, S.K. Prognostic value of sarcopenia in patients with liver cirrhosis: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0186990. [Google Scholar] [CrossRef] [PubMed]
- Bone, A.E.; Hepgul, N.; Kon, S.; Maddocks, M. Sarcopenia and frailty in chronic respiratory disease. Chronic Respir. Dis. 2017, 14, 85–99. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.E.; Maddocks, M.; Kon, S.S.C.; Canavan, J.L.; Nolan, C.M.; Clark, A.L.; Polkey, M.I.; Man, W.D.-C. Sarcopenia in COPD: Prevalence, clinical correlates and response to pulmonary rehabilitation. Thorax 2015, 70, 213–218. [Google Scholar] [CrossRef]
- Umegaki, H. Sarcopenia and frailty in older patients with diabetes mellitus. Geriatr. Gerontol. Int. 2016, 16, 293–299. [Google Scholar] [CrossRef]
- Follis, S.; Cook, A.; Bea, J.W.; Going, S.B.; Laddu, D.; Cauley, J.A.; Shadyab, A.H.; Stefanick, M.L.; Chen, Z. Association Between Sarcopenic Obesity and Falls in a Multiethnic Cohort of Postmenopausal Women. J. Am. Geriatr. Soc. 2018, 66, 2314–2320. [Google Scholar] [CrossRef]
- Sim, M.; Prince, R.L.; Scott, D.; Daly, R.M.; Duque, G.; Inderjeeth, C.A.; Zhu, K.; Woodman, R.J.; Hodgson, J.M.; Lewis, J.R. Utility of four sarcopenia criteria for the prediction of falls-related hospitalization in older Australian women. Osteoporos. Int. 2019, 30, 167–176. [Google Scholar] [CrossRef]
- Marzetti, E.; Hwang, A.-C.; Tosato, M.; Peng, L.-N.; Calvani, R.; Picca, A.; Chen, L.-K.; Landi, F. Age-related changes of skeletal muscle mass and strength among Italian and Taiwanese older people: Results from the Milan EXPO 2015 survey and the I-Lan Longitudinal Aging Study. Exp. Gerontol. 2018, 102, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Srikanthan, P.; Karlamangla, A.S. Muscle mass index as a predictor of longevity in older adults. Am. J. Med. 2014, 127, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Cuthbertson, D.J.; Bell, J.A.; Ng, S.Y.; Kemp, G.J.; Kivimaki, M.; Hamer, M. Dynapenic obesity and the risk of incident Type 2 diabetes: The English Longitudinal Study of Ageing. Diabet. Med. 2016, 33, 1052–1059. [Google Scholar] [CrossRef] [PubMed]
- Srikanthan, P.; Hevener, A.L.; Karlamangla, A.S. Sarcopenia exacerbates obesity-associated insulin resistance and dysglycemia: Findings from the National Health and Nutrition Examination Survey III. PLoS ONE 2010, 5, e10805. [Google Scholar] [CrossRef]
- Deer, R.R.; Dickinson, J.M.; Fisher, S.R.; Ju, H.; Volpi, E. Identifying effective and feasible interventions to accelerate functional recovery from hospitalization in older adults: A randomized controlled pilot trial. Contemp. Clin. Trials 2016, 49, 6–14. [Google Scholar] [CrossRef]
- Morais, J.A.; Jacob, K.W.; Chevalier, S. Effects of aging and insulin resistant states on protein anabolic responses in older adults. Exp. Gerontol. 2018, 108, 262–268. [Google Scholar] [CrossRef]
- Breen, L.; Phillips, S.M. Skeletal muscle protein metabolism in the elderly: Interventions to counteract the “anabolic resistance” of ageing. Nutr. Metab. (Lond.) 2011, 8, 68. [Google Scholar] [CrossRef]
- Paddon-Jones, D.; Campbell, W.W.; Jacques, P.F.; Kritchevsky, S.B.; Moore, L.L.; Rodriguez, N.R.; van Loon, L.J. Protein and healthy aging. Am. J. Clin. Nutr. 2015, 101, 1339S–1345S. [Google Scholar] [CrossRef]
- Murphy, C.H.; Oikawa, S.Y.; Phillips, S.M. Dietary Protein to Maintain Muscle Mass in Aging: A Case for Per-meal Protein Recommendations. J. Frailty Aging 2016, 5, 49–58. [Google Scholar]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Volpi, E.; Campbell, W.W.; Dwyer, J.T.; Johnson, M.A.; Jensen, G.L.; Morley, J.E.; Wolfe, R.R. Is the optimal level of protein intake for older adults greater than the recommended dietary allowance? J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 677–681. [Google Scholar] [CrossRef] [PubMed]
- De Bandt, J.-P. Leucine and Mammalian Target of Rapamycin-Dependent Activation of Muscle Protein Synthesis in Aging. J. Nutr. 2016, 146, 2616S–2624S. [Google Scholar] [CrossRef] [PubMed]
- Casperson, S.L.; Sheffield-Moore, M.; Hewlings, S.J.; Paddon-Jones, D. Leucine supplementation chronically improves muscle protein synthesis in older adults consuming the RDA for protein. Clin. Nutr. 2012, 31, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Wall, B.T.; van Loon, L.J.C. Nutritional strategies to attenuate muscle disuse atrophy. Nutr. Rev. 2013, 71, 195–208. [Google Scholar] [CrossRef]
- Rieu, I.; Balage, M.; Sornet, C.; Giraudet, C.; Pujos, E.; Grizard, J.; Mosoni, L.; Dardevet, D. Leucine supplementation improves muscle protein synthesis in elderly men independently of hyperaminoacidaemia. J. Physiol. (Lond.) 2006, 575, 305–315. [Google Scholar] [CrossRef]
- Balage, M.; Dardevet, D. Long-term effects of leucine supplementation on body composition. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 265–270. [Google Scholar] [CrossRef]
- van Loon, L.J.C.; Kruijshoop, M.; Menheere, P.P.C.A.; Wagenmakers, A.J.M.; Saris, W.H.M.; Keizer, H.A. Amino acid ingestion strongly enhances insulin secretion in patients with long-term type 2 diabetes. Diabetes Care 2003, 26, 625–630. [Google Scholar] [CrossRef]
- Hamarsland, H.; Nordengen, A.L.; Nyvik Aas, S.; Holte, K.; Garthe, I.; Paulsen, G.; Cotter, M.; Børsheim, E.; Benestad, H.B.; Raastad, T. Native whey protein with high levels of leucine results in similar post-exercise muscular anabolic responses as regular whey protein: A randomized controlled trial. J. Int. Soc. Sports Nutr. 2017, 14, 43. [Google Scholar] [CrossRef]
- Tang, J.E.; Moore, D.R.; Kujbida, G.W.; Tarnopolsky, M.A.; Phillips, S.M. Ingestion of whey hydrolysate, casein, or soy protein isolate: Effects on mixed muscle protein synthesis at rest and following resistance exercise in young men. J. Appl. Physiol. 2009, 107, 987–992. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Weissenfels, A.; Teschler, M.; Willert, S.; Bebenek, M.; Shojaa, M.; Kohl, M.; Freiberger, E.; Sieber, C.; von Stengel, S. Whole-body electromyostimulation and protein supplementation favorably affect sarcopenic obesity in community-dwelling older men at risk: The randomized controlled FranSO study. Clin. Interv. Aging 2017, 12, 1503–1513. [Google Scholar] [CrossRef] [PubMed]
- Kramer, I.F.; Verdijk, L.B.; Hamer, H.M.; Verlaan, S.; Luiking, Y.C.; Kouw, I.W.K.; Senden, J.M.; van Kranenburg, J.; Gijsen, A.P.; Bierau, J.; et al. Both basal and post-prandial muscle protein synthesis rates, following the ingestion of a leucine-enriched whey protein supplement, are not impaired in sarcopenic older males. Clin. Nutr. 2017, 36, 1440–1449. [Google Scholar] [CrossRef] [PubMed]
- Leenders, M.; Verdijk, L.B.; van der Hoeven, L.; van Kranenburg, J.; Hartgens, F.; Wodzig, W.K.W.H.; Saris, W.H.M.; van Loon, L.J.C. Prolonged leucine supplementation does not augment muscle mass or affect glycemic control in elderly type 2 diabetic men. J. Nutr. 2011, 141, 1070–1076. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, S.S.I.; Phillips, B.E.; Wilkinson, D.J.; Limb, M.C.; Rankin, D.; Mitchell, W.K.; Kobayashi, H.; Greenhaff, P.L.; Smith, K.; Atherton, P.J. Intake of low-dose leucine-rich essential amino acids stimulates muscle anabolism equivalently to bolus whey protein in older women at rest and after exercise. Am. J. Physiol. Endocrinol. Metab. 2015, 308, E1056–E1065. [Google Scholar] [CrossRef] [PubMed]
- Devries, M.C.; McGlory, C.; Bolster, D.R.; Kamil, A.; Rahn, M.; Harkness, L.; Baker, S.K.; Phillips, S.M. Protein leucine content is a determinant of shorter- and longer-term muscle protein synthetic responses at rest and following resistance exercise in healthy older women: A randomized, controlled trial. Am. J. Clin. Nutr. 2018, 107, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Abe, S.; Ezaki, O.; Suzuki, M. Medium-Chain Triglycerides in Combination with Leucine and Vitamin D Increase Muscle Strength and Function in Frail Elderly Adults in a Randomized Controlled Trial. J. Nutr. 2016, 146, 1017–1026. [Google Scholar] [CrossRef]
- Bauer, J.M.; Verlaan, S.; Bautmans, I.; Brandt, K.; Donini, L.M.; Maggio, M.; McMurdo, M.E.T.; Mets, T.; Seal, C.; Wijers, S.L.; et al. Effects of a vitamin D and leucine-enriched whey protein nutritional supplement on measures of sarcopenia in older adults, the PROVIDE study: A randomized, double-blind, placebo-controlled trial. J. Am. Med. Dir. Assoc. 2015, 16, 740–747. [Google Scholar] [CrossRef]
- Björkman, M.P.; Pilvi, T.K.; Kekkonen, R.A.; Korpela, R.; Tilvis, R.S. Similar effects of leucine rich and regular dairy products on muscle mass and functions of older polymyalgia rheumatica patients: A randomized crossover trial. J. Nutr. Health Aging 2011, 15, 462–467. [Google Scholar] [CrossRef]
- Chanet, A.; Verlaan, S.; Salles, J.; Giraudet, C.; Patrac, V.; Pidou, V.; Pouyet, C.; Hafnaoui, N.; Blot, A.; Cano, N.; et al. Supplementing Breakfast with a Vitamin D and Leucine-Enriched Whey Protein Medical Nutrition Drink Enhances Postprandial Muscle Protein Synthesis and Muscle Mass in Healthy Older Men. J. Nutr. 2017, 147, 2262–2271. [Google Scholar] [CrossRef]
- Evans, M.; Guthrie, N.; Pezzullo, J.; Sanli, T.; Fielding, R.A.; Bellamine, A. Efficacy of a novel formulation of L-Carnitine, creatine, and leucine on lean body mass and functional muscle strength in healthy older adults: A randomized, double-blind placebo-controlled study. Nutr. Metab. (Lond.) 2017, 14, 7. [Google Scholar] [CrossRef] [PubMed]
- Holwerda, A.M.; Paulussen, K.J.M.; Overkamp, M.; Goessens, J.P.B.; Kramer, I.-F.; Wodzig, W.K.W.H.; Verdijk, L.B.; de Groot, L.C.P.G.M.; van Loon, L.J.C. Leucine co-ingestion augments the muscle protein synthetic response to the ingestion of 15 g protein following resistance exercise in older men. Am. J. Physiol. Endocrinol. Metab. 2019. [Google Scholar] [CrossRef] [PubMed]
- Ispoglou, T.; White, H.; Preston, T.; McElhone, S.; McKenna, J.; Hind, K. Double-blind, placebo-controlled pilot trial of L-Leucine-enriched amino-acid mixtures on body composition and physical performance in men and women aged 65–75 years. Eur. J. Clin. Nutr. 2016, 70, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.K.; Suzuki, T.; Saito, K.; Yoshida, H.; Kobayashi, H.; Kato, H.; Katayama, M. Effects of exercise and amino acid supplementation on body composition and physical function in community-dwelling elderly Japanese sarcopenic women: A randomized controlled trial. J. Am. Geriatr. Soc. 2012, 60, 16–23. [Google Scholar] [CrossRef]
- Kirk, B.; Mooney, K.; Amirabdollahian, F.; Khaiyat, O. Exercise and Dietary-Protein as a Countermeasure to Skeletal Muscle Weakness: Liverpool Hope University—Sarcopenia Aging Trial (LHU-SAT). Front. Physiol. 2019, 10, 445. [Google Scholar] [CrossRef]
- Kouw, I.W.; Holwerda, A.M.; Trommelen, J.; Kramer, I.F.; Bastiaanse, J.; Halson, S.L.; Wodzig, W.K.; Verdijk, L.B.; van Loon, L.J. Protein Ingestion before Sleep Increases Overnight Muscle Protein Synthesis Rates in Healthy Older Men: A Randomized Controlled Trial. J. Nutr. 2017, 147, 2252–2261. [Google Scholar] [CrossRef]
- Dal Negro, R.W.; Testa, A.; Aquilani, R.; Tognella, S.; Pasini, E.; Barbieri, A.; Boschi, F. Essential amino acid supplementation in patients with severe COPD: A step towards home rehabilitation. Monaldi Arch. Chest Dis. 2012, 77, 67–75. [Google Scholar] [CrossRef]
- Rondanelli, M.; Klersy, C.; Terracol, G.; Talluri, J.; Maugeri, R.; Guido, D.; Faliva, M.A.; Solerte, B.S.; Fioravanti, M.; Lukaski, H.; et al. Whey protein, amino acids, and vitamin D supplementation with physical activity increases fat-free mass and strength, functionality, and quality of life and decreases inflammation in sarcopenic elderly. Am. J. Clin. Nutr. 2016, 103, 830–840. [Google Scholar] [CrossRef]
- Soriano, G.; Román, E.; Torrades, M.T.; Cárdenas, G.; Córdoba, J.; Blanco, M.J.N.; Nieto, J.C.; Vidal, S.; Villanueva, C.; Ambrós, H.B.; et al. Estudio del beneficio de un programa de ejercicio físico y suplementos de aminoácidos ramificados en la dieta dirigido a pacientes con cirrosis hepática. Trauma 2013, 24, 6–11. [Google Scholar]
- van de Bool, C.; Rutten, E.P.A.; van Helvoort, A.; Franssen, F.M.E.; Wouters, E.F.M.; Schols, A.M.W.J. A randomized clinical trial investigating the efficacy of targeted nutrition as adjunct to exercise training in COPD. J. Cachexia Sarcopenia Muscle 2017, 8, 748–758. [Google Scholar] [CrossRef]
- Verhoeven, S.; Vanschoonbeek, K.; Verdijk, L.B.; Koopman, R.; Wodzig, W.K.W.H.; Dendale, P.; van Loon, L.J.C. Long-term leucine supplementation does not increase muscle mass or strength in healthy elderly men. Am. J. Clin. Nutr. 2009, 89, 1468–1475. [Google Scholar] [CrossRef] [PubMed]
- Verlaan, S.; Maier, A.B.; Bauer, J.M.; Bautmans, I.; Brandt, K.; Donini, L.M.; Maggio, M.; McMurdo, M.E.T.; Mets, T.; Seal, C.; et al. Sufficient levels of 25-hydroxyvitamin D and protein intake required to increase muscle mass in sarcopenic older adults—The PROVIDE study. Clin. Nutr. 2018, 37, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Verreijen, A.M.; Verlaan, S.; Engberink, M.F.; Swinkels, S.; de Vogel-van den Bosch, J.; Weijs, P.J.M. A high whey protein-, leucine-, and vitamin D-enriched supplement preserves muscle mass during intentional weight loss in obese older adults: A double-blind randomized controlled trial. Am. J. Clin. Nutr. 2015, 101, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, Y.; Bise, T.; Shimazu, S.; Tanoue, M.; Tomioka, Y.; Araki, M.; Nishino, T.; Kuzuhara, A.; Takatsuki, F. Effects of a leucine-enriched amino acid supplement on muscle mass, muscle strength, and physical function in post-stroke patients with sarcopenia: A randomized controlled trial. Nutrition 2019, 58, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Beaudart, C.; Zaaria, M.; Pasleau, F.; Reginster, J.-Y.; Bruyère, O. Health Outcomes of Sarcopenia: A Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0169548. [Google Scholar] [CrossRef]
- Cerri, A.P.; Bellelli, G.; Mazzone, A.; Pittella, F.; Landi, F.; Zambon, A.; Annoni, G. Sarcopenia and malnutrition in acutely ill hospitalized elderly: Prevalence and outcomes. Clin. Nutr. 2015, 34, 745–751. [Google Scholar] [CrossRef]
- Fielding, R.A.; Vellas, B.; Evans, W.J.; Bhasin, S.; Morley, J.E.; Newman, A.B.; Abellan van Kan, G.; Andrieu, S.; Bauer, J.; Breuille, D.; et al. Sarcopenia: An undiagnosed condition in older adults. Current consensus definition: Prevalence, etiology, and consequences. International working group on sarcopenia. J. Am. Med. Dir. Assoc. 2011, 12, 249–256. [Google Scholar] [CrossRef]
- Sinclair, M.; Gow, P.J.; Grossmann, M.; Angus, P.W. Review article: Sarcopenia in cirrhosis—Aetiology, implications and potential therapeutic interventions. Aliment. Pharmacol. Ther. 2016, 43, 765–777. [Google Scholar] [CrossRef]
- Choi, K.M. Sarcopenia and sarcopenic obesity. Korean J. Intern. Med. 2016, 31, 1054–1060. [Google Scholar] [CrossRef]
- Poggiogalle, E.; Migliaccio, S.; Lenzi, A.; Donini, L.M. Treatment of body composition changes in obese and overweight older adults: Insight into the phenotype of sarcopenic obesity. Endocrine 2014, 47, 699–716. [Google Scholar] [CrossRef]
- Morley, J.E. Frailty and Sarcopenia: The New Geriatric Giants. Rev. Investig. Clin. 2016, 68, 59–67. [Google Scholar]
- Makanae, Y.; Fujita, S. Role of Exercise and Nutrition in the Prevention of Sarcopenia. J. Nutr. Sci. Vitaminol. 2015, 61, S125–S127. [Google Scholar] [CrossRef] [PubMed]
- Coelho-Júnior, H.J.; de Oliveira Gonçalvez, I.; Sampaio, R.A.C.; Sewo Sampaio, P.Y.; Cadore, E.L.; Izquierdo, M.; Marzetti, E.; Uchida, M.C. Periodized and non-periodized resistance training programs on body composition and physical function of older women. Exp. Gerontol. 2019, 121, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Osuka, Y.; Kojima, N.; Wakaba, K.; Miyauchi, D.; Tanaka, K.; Kim, H. Effects of resistance training and/or beta-hydroxy-beta-methylbutyrate supplementation on muscle mass, muscle strength and physical performance in older women with reduced muscle mass: Protocol for a randomised, double-blind, placebo-controlled trial. BMJ Open 2019, 9, e025723. [Google Scholar] [CrossRef] [PubMed]
- Tsuzuku, S.; Kajioka, T.; Sakakibara, H.; Shimaoka, K. Slow movement resistance training using body weight improves muscle mass in the elderly: A randomized controlled trial. Scand. J. Med. Sci. Sports 2018, 28, 1339–1344. [Google Scholar] [CrossRef]
- Komar, B.; Schwingshackl, L.; Hoffmann, G. Effects of leucine-rich protein supplements on anthropometric parameter and muscle strength in the elderly: A systematic review and meta-analysis. J. Nutr. Health Aging 2015, 19, 437–446. [Google Scholar] [CrossRef]
- Antoniak, A.E.; Greig, C.A. The effect of combined resistance exercise training and vitamin D3 supplementation on musculoskeletal health and function in older adults: A systematic review and meta-analysis. BMJ Open 2017, 7, e014619. [Google Scholar] [CrossRef]
- Spira, D.; Buchmann, N.; König, M.; Rosada, A.; Steinhagen-Thiessen, E.; Demuth, I.; Norman, K. Sex-specific differences in the association of vitamin D with low lean mass and frailty: Results from the Berlin Aging Study II. Nutrition 2019, 62, 1–6. [Google Scholar] [CrossRef]
- McGregor, R.A.; Cameron-Smith, D.; Poppitt, S.D. It is not just muscle mass: A review of muscle quality, composition and metabolism during ageing as determinants of muscle function and mobility in later life. Longev. Healthspan 2014, 3, 9. [Google Scholar] [CrossRef]
- Häkkinen, K.; Kraemer, W.J.; Kallinen, M.; Linnamo, V.; Pastinen, U.M.; Newton, R.U. Bilateral and unilateral neuromuscular function and muscle cross-sectional area in middle-aged and elderly men and women. J. Gerontol. A Biol. Sci. Med. Sci. 1996, 51, B21–B29. [Google Scholar] [CrossRef]
- Schols, A.M.; Ferreira, I.M.; Franssen, F.M.; Gosker, H.R.; Janssens, W.; Muscaritoli, M.; Pison, C.; Rutten-van Mölken, M.; Slinde, F.; Steiner, M.C.; et al. Nutritional assessment and therapy in COPD: A European Respiratory Society statement. Eur. Respir. J. 2014, 44, 1504–1520. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Studenski, S.A.; Peters, K.W.; Alley, D.E.; Cawthon, P.M.; McLean, R.R.; Harris, T.B.; Ferrucci, L.; Guralnik, J.M.; Fragala, M.S.; Kenny, A.M.; et al. The FNIH sarcopenia project: Rationale, study description, conference recommendations, and final estimates. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 547–558. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Mean Age (years) | Sample Size | Percentage of Women | Country | Characteristics of the Sample | Assessment of Sarcopenia with Recommended Tools | Lean Mass | Handgrip | Physical Performance Assessment | |
|---|---|---|---|---|---|---|---|---|---|
| Abe et al. 2016 [37] | 86.6 ± 4.8 | 38 | 71,05% | Japan | Nursing home residents | NO | Arm muscle area and calf circumference. | Handgrip dynamometry | Knee extension time and 10m test. |
| Bauer et al., 2015 [38] | 77.7 | 380 | 65,52% | Netherlands registered (sample: 6 European countries) | Community-dwelling individuals | YES (EWGSOP) | Skeletal muscle mass index adjusted by BMI by BIA and DXA. (Janssen criteria) Use of cut-off values | Handgrip dynamometry | SPPB score |
| Bjorkman et al., 2011 [39] | 69.6 | 47 | 89,36% | Finland | Non-specified residence. Polymialgia rheumatica patients | YES (EWGSOP) | Skeletal muscle mass index by DXA. | Handgrip dynamometry | Walking speed 10 m-test. |
| Bukhari et al., 2015 [35] | 66 ± 25 | 16 | 100% | United Kingdom | Non-specified residence | YES(EWGSOP) | Appendicular muscle mass and skeletal muscle mass index by DXA (Janssen criteria) | Not determined | Not determined |
| Chanet et al., 2017 [40] | 71 ± 4 | 24 | 0% | France | Non-specified residence | YES (EWGSOP) | Skeletal muscle mass index by DXA. | Handgrip dynamometry | SPPB score |
| De Vries et al., 2018 [36] | 68.5 | 22 | 100% | Canada | Community-dwelling individuals | NO | Skeletal muscle mass in kg by DXA. | Knee extension strength. | Estimated physical activity by pedometer in leg and accelerometer in arm |
| Evans et al., 2017 [41] | 57.6 | 42 | 64,29% | Canada | Community-dwelling individuals | YES (EWGSOP but only for handgrip criterion) | Skeletal muscle mass in kg by DXA. | Handgrip dynamometry. | 6-min walking test |
| Holwerda et al., 2019 [42] | 70 ± 1 | 41 | 0% | Netherlands | Community-dwelling individuals. | YES (EWGSOP but only for muscle mass and physical performance criteria)) | Skeletal muscle mass index by DXA. | Knee extension and leg press strength | SPPB score |
| Ispoglou et al., 2016 [43] | 71.5 | 25 | 56% | United Kingdom | Community-dwelling individuals | YES (EWGSOP but only for handgrip criterion) | Skeletal muscle mass in kg by DXA. | Handgrip dynamometry. | 6-min walking test |
| Kemmler et al., 2017 [32] | 77.6 | 100 | 0% | Germany | Community-dwelling individuals | YES FNIH criteria) | Skeletal muscle mass index by BIA Use of cut-off values | Handgrip dynamometry Use of cut-off values | Late life function and disability instrument (LLFDI) and physical activity index. |
| Kim et al., 2012 [44] | 79.3 | 155 | 100% | Japan | Non-specified residence | YES (EWGSOP but only for muscle mass criterion) | Skeletal muscle mass index by BIA. Use of cut-off values | Knee extension strength Use of cut-off values | Usual walking speed. Use of cut-off values |
| Kirk et al., 2019 [45] | 68 ± 5 | 46 | 54,3% | United Kingdom | Community-dwelling individuals | NO | Not determined. | Leg press strength | SPPB score |
| Kouw et al., 2017 [46] | 71 | 48 | 0% | Netherlands | Non-specified residence | YES (EWGSOP but only for muscle mass criterion) | Skeletal muscle mass index by DXA. | Not determined | Not determined |
| Kramer et al., 2017 [33] | 75 | 30 | 0% | Netherlands | Community-dwelling individuals | YES (EWGSOP criteria) | Skeletal muscle mass index by DXA. Use of cut-off values. | Handgrip dynamometry Use of cut-off values | Walking speed 4 m-test Use of cut-off values |
| Dal Negro et al., 2012 [47] | 74.6 | 88 | 30,7% | Italy | Community-dwelling individuals. COPD patients. | NO | Skeletal muscle mass index by BIA. (Baarends criteria). Use of cut-off values | Handgrip dynamometry | Physical activity by daily steps. |
| Leenders et al., 2011 [34] | 71 ± 1 | 60 | 0% | Netherlands | Non-specified residence. Diabetes mellitus type 2 individuals. | NO | Skeletal muscle mass in kg by DXA. | Knee extension and leg press strength | Habitual physical activity register in METs. |
| Rondanelli et al., 2016 [48] | 80.3 | 130 | 59,23% | Italy | Nursing home residents | YES (EWGSOP but only for muscle mass criterion) | Skeletal muscle mass index by DXA Use of cut-off values | Handgrip dynamometry | Physical activity by activities of daily living. |
| Soriano et al., 2013 [49] | 62 | 17 | 29,4% | Spain | Non-specified residence. Patients with liver cirrhosis. | NO | Arm muscle area and quadriceps perimeter. | Not determined | 6-min walking test |
| Van den Bool et al., 2017 [50] | 62.6 | 81 | 49% | Netherlands | Community-dwelling individuals. COPD patients. | NO | Skeletal muscle mass in kg by DXA. | Knee extension strength and respiratory muscle strength | 6-min walking test |
| Verhoeven et al., 2009 [51] | 71 ± 4 | 30 | 0% | Netherlands | Community-dwelling individuals. | NO | Skeletal muscle mass in kg by DXA. | Knee extension and leg press strength. | Not determined |
| Verlaan et al., 2018 [52] | 77.7 | 380 | 65% | Netherlands registered (multicenter several countries) (18 centers) | Community-dwelling individuals | YES (EWGSOP but only for muscle mass criterion) | Skeletal muscle mass index adjusted by BMI by BIA (Janssen criteria) Use of cut-off values | Handgrip dynamometry | SPPB score. |
| Verreijen et al., 2015 [53] | 63.4 | 80 I (40) C (40) | 53% | Netherlands | Non-specified residence | YES (EWGSOP) | Skeletal muscle mass index by DXA. | Handgrip dynamometry. | Walking speed 4 m-test |
| Yoshimura et al., 2019 [54] | 79.8 | 44 | 68.2% | Japan | Non-specified residence. Post-stroke patients | YES (AWGS) | Skeletal muscle mass index by BIA Use of cut-off values | Handgrip dynamometry Use of cut-off values | FIM score |
| Leucine Dose (g/day) | Additional Supplementation Intervention Constituents (g/day) | Control Group | Treatment Duration | Effect on Muscle Strength | Effect on Lean Mass | Effect on Walking Speed | |
|---|---|---|---|---|---|---|---|
| Abe 2016 [37] | 1.2 | Group 1: EAAs (3 g), vit-D (800IU), medium-chain TGs (6 g); Group 2: EAAs (3 g), vit-D (800IU), or long-chain TGs (6 g) | No placebo group | 13 weeks | Improved | Not determined | Improved |
| Bauer 2015 [38] | 6 | Whey protein (40 g), carbohydrates (18 g), fat (6 g), vit-D (1600 IU) and mixture of vitamins, minerals and fibers | Isocaloric product without protein content | 13 weeks | Not altered | Improved | Not altered |
| Bjorkman 2011 [39] | 19.2 (Group 1) or 16.8 (Group 2) – calculated | Group 1: Whey protein (160 g) and casein (40 g) Group 2: Whey protein (40 g) and casein (160 g) | No placebo group | 8 weeks (and crossover) | Decreased | Not altered | Improved |
| Chanet 2017 [40] | 3 | Protein (21 g), carbohydrates (9.5 g), fat (3 g), vit-D (20 µg) and mixture of vitamins, minerals and fibers | Flavored watery placebo drink | 6 weeks | Not altered | Improved | Not altered |
| Evans 2017 [41] | 2 (Group 1) | Group 1: Leucine (2 g), L-Carnitine (1.5 g), creatine monohydrates (3 g), Vit-D (400 IU); Group 2: L-Carnitine (1,5 g) | Placebo dissolved in orange juice | 8 weeks | Not altered | Improved (only in Group 1) | Not determined |
| Holwerda 2019 [42] | 2,8 (Group 1) | Group 1: Whey protein (20,7 g, with 2.8 g leucine), exercise (3 times/week) | Isocaloric product without protein content and exercise (3 times/week) | 12 weeks | Not altered | Not altered | Not altered |
| Ispoglou 2016 [43] | 3 (Group 1) or 6 (Group 2) – calculated | Group 1: EAA mixture (15 g); Group 2: EAA mixture leucine-enriched (15 g) | Isocaloric lactose placebo | 13 weeks | Not altered | Improved (only in group 2) | Not determined |
| Kim 2012 [44] | 2.5 (Group 1 and 3) | Group 1: EAA (6 g), exercise (2 times/week); Group 2: Exercise (2 times/week); Group 3: EAA (6 g);Group 4: Health education | Health education program | 13 weeks | Improved (only in Group1) | Improved (only in Group 1) | Improved (in Groups 1 and 2) |
| Kirk 2019 [45] | 7 - estimated | Group 1: Whey protein (1,5 g/kg/day), exercise (3 times/week) Group 2: Exercise (3 times/week) | No placebo group | 16 weeks | Not altered | Not determined | Not altered |
| Dal Negro 2012 [47] | 2.5 | EAA (8 g) | Isocaloric product without protein content | 12 weeks | Improved | Not altered | Not determined |
| Leenders 2011 [34] | 7.5 | Leucine alone | Wheat flour | 24 weeks | Not altered | Not altered | Not determined |
| Rondanelli 2016 [48] | 4 | Whey protein (32 g with 10,9 g of EAA), Vit-D (100IU), exercise (3 times/week) | Isocaloric maltodextrine placebo (32 g) | 12 weeks | Improved | Improved | Not determined |
| Soriano 2013 [49] | 10 | Group 1: Leucine and nutritional assessment; Group 2: Leucine, nutritional assessment and exercise | No placebo group | 13 weeks | Not determined | Not determined | Improved |
| Van de Bool 2017 [50] | 1.8 or 2.7 - calculated | Protein (between 18.74 and 28.11 g) | Flavored non-caloric protein-free aqueous placebo | 17 weeks | Not determined | Not altered | Not determined |
| Verhoeven 2009 [51] | 7.5 | Leucine alone | Wheat flour | 12 weeks | Not altered | Not altered | Not determined |
| Verlaan 2018 [52] | 6 | Whey protein (20 g), Vit-D (800 IU) | Isocaloric product without protein content | 13 weeks | Not determined | Improved | Not determined |
| Verreijen 2015 [53] | 2,8 | Whey protein (20.7 g with 10.6 g of EAA), vit-D (20 µg), exercise (3 times/week) | Isocaloric product without protein content | 13 weeks | Not altered | Improved | Not determined |
| Yoshimura 2019 [54] | 3 | Group 1: EAA (7.5 g), exercise (7 times/week) Group 2: Exercise (7 times/week) | No placebo group | 8 weeks | Improved | Improved | Not determined |
| Bias Domain | Selection Bias | Performance Bias | Detection Bias | Attrition Bias | Reporting Bias | |
|---|---|---|---|---|---|---|
| Source of Bias | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting |
| RCT Report | ||||||
| Bauer et al. 2015 [38] | low | low | low | unclear | Low | low |
| Chanet et al. 2017 [40] | low | low | low | high | Unclear | low |
| Evans et al. 2017 [41] | unclear | low | low | unclear | Low | low |
| Holwerda et al. 2019 [42] | high | low | low | unclear | Low | unclear |
| Ispoglou et al. 2016 [43] | high | low | unclear | unclear | Low | unclear |
| Kim et al. 2012 [44] | low | low | low | unclear | Low | unclear |
| Dal Negro et al. 2012 [47] | high | high | low | high | Unclear | low |
| Leenders et al. 2011 [34] | high | high | low | unclear | Unclear | low |
| Rondanelli et al. 2016 [48] | unclear | low | low | unclear | Unclear | low |
| Van de Bool et al. 2017 [50] | low | low | low | unclear | Low | low |
| Verhoeven et al. 2009 [51] | high | high | low | low | Unclear | low |
| Verlaan et al. 2018 [52] | low | low | low | low | Unclear | unclear |
| Verreijen et al. 2014 [53] | low | low | low | unclear | Low | unclear |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Arnau, F.M.; Fonfría-Vivas, R.; Cauli, O. Beneficial Effects of Leucine Supplementation on Criteria for Sarcopenia: A Systematic Review. Nutrients 2019, 11, 2504. https://doi.org/10.3390/nu11102504
Martínez-Arnau FM, Fonfría-Vivas R, Cauli O. Beneficial Effects of Leucine Supplementation on Criteria for Sarcopenia: A Systematic Review. Nutrients. 2019; 11(10):2504. https://doi.org/10.3390/nu11102504
Chicago/Turabian StyleMartínez-Arnau, Francisco M., Rosa Fonfría-Vivas, and Omar Cauli. 2019. "Beneficial Effects of Leucine Supplementation on Criteria for Sarcopenia: A Systematic Review" Nutrients 11, no. 10: 2504. https://doi.org/10.3390/nu11102504
APA StyleMartínez-Arnau, F. M., Fonfría-Vivas, R., & Cauli, O. (2019). Beneficial Effects of Leucine Supplementation on Criteria for Sarcopenia: A Systematic Review. Nutrients, 11(10), 2504. https://doi.org/10.3390/nu11102504