Search and Selection of Probiotics That Improve Mucositis Symptoms in Oncologic Patients. A Systematic Review


Abstract
1. Introduction
1.1. Pathogenesis
1.2. Assessment Scales Mucositis
1.3. Drugs
1.4. Microbiota
1.5. Probiotics
2. Materials and Methods
2.1. Source of Data Collection
2.2. Information Processing
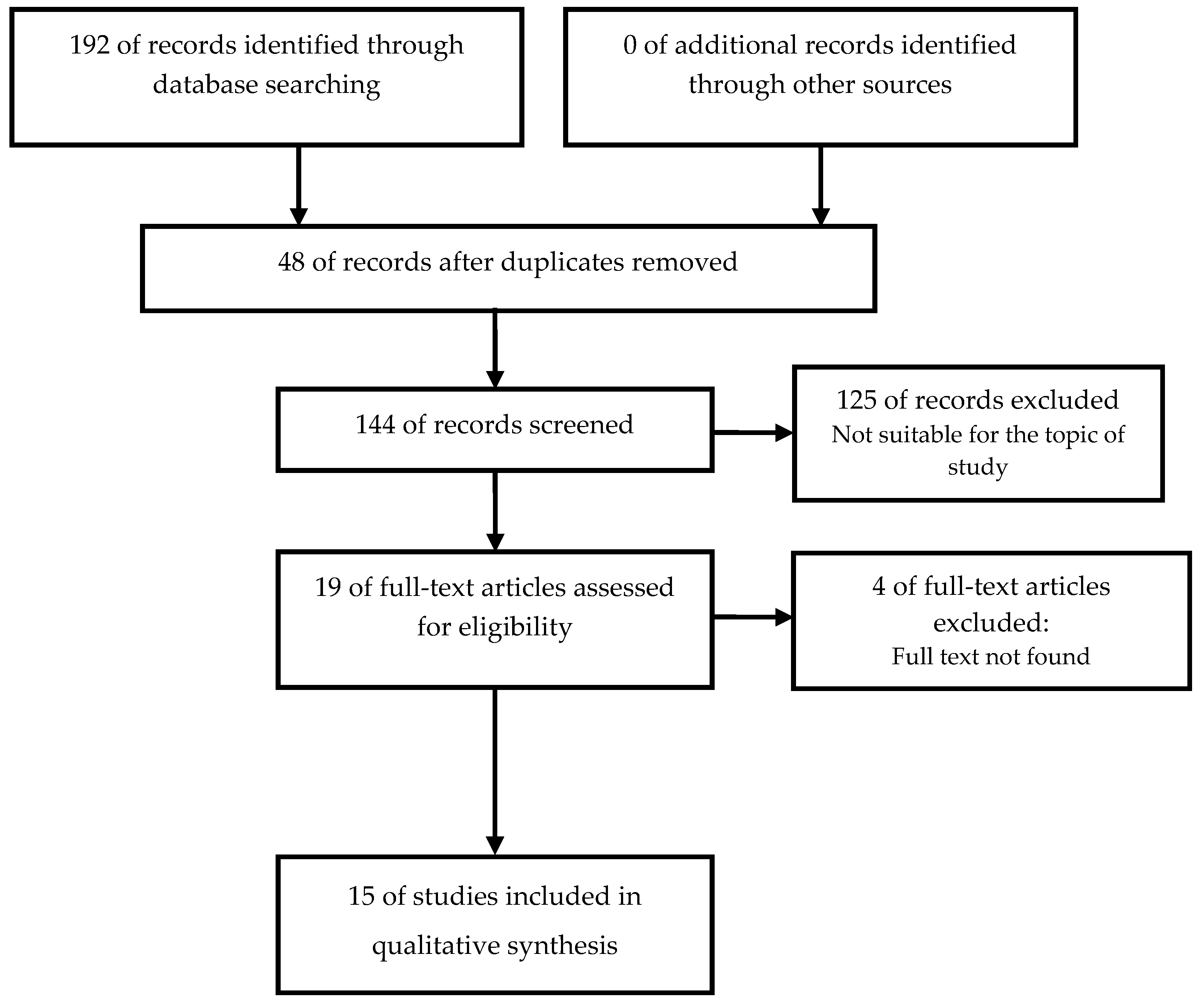
2.3. Final Selection of Articles
2.4. Data Extraction
3. Results
3.1. Probiotics and Healthy People
3.2. Probiotics and CRC
3.3. Probiotics and Mucositis
3.4. Probiotics and Other Intestinal Pathologies
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Touchefeu, Y.; Montassier, E.; Nieman, K.; Gastinne, T.; Potel, G.; Bruley Des Varannes, S.; Le Vacon, F.; de La Cochetière, M.F. Systematic review: The role of the gut microbiota in chemotherapy- or radiation-induced gastrointestinal mucositis-Current evidence and potential clinical applications. Aliment. Pharmacol. Ther. 2014, 40, 409–421. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.A.; Avritscher, E.B.C.; Cooksley, C.D.; Michelet, M.; Bekele, B.N.; Elting, L.S. Epidemiology of treatment-associated mucosal injury after treatment with newer regimens for lymphoma, breast, lung, or colorectal cancer. Support Care Cancer 2006, 14, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Vera-Llonch, M.; Oster, G.; Hagiwara, M.; Sonis, S. Oral mucositis in patients undergoing radiation treatment for head and neck carcinoma. Cancer 2006, 106, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Vera-Llonch, M.; Oster, G.; Ford, C.M.; Lu, J.; Sonis, S. Oral mucositis and outcomes of allogeneic hematopoietic stem-cell transplantation in patients with hematologic malignancies. Support Care Cancer 2007, 15, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Sonis, S.T. The pathobiology of mucositis. Nat. Rev. Cancer 2004, 4, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Criswell, T.; Leskov, K.; Miyamoto, S.; Luo, G.; Boothman, D.A. Transcription factors activated in mammalian cells after clinically relevant doses of ionizing radiation. Oncogene 2003, 22, 5813–5827. [Google Scholar] [CrossRef]
- Bamba, S.; Andoh, A.; Yasui, H.; Araki, Y.; Bamba, T.; Fujiyama, Y. Matrix metalloproteinase-3 secretion from human colonic subepithelial myofibroblasts: Role of interleukin-17. J. Gastroenterol. 2003, 38, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Naidu, M.U.R.; Ramana, G.V.; Rani, P.U.; Mohan, I.K.; Suman, A.; Roy, P. Chemotherapy-induced and/or radiation therapy-induced oral mucositis--complicating the treatment of cancer. Neoplasia (N. Y.) 2004, 6, 423–431. [Google Scholar] [CrossRef]
- Elting, L.S.; Cooksley, C.; Chambers, M.; Cantor, S.B.; Manzullo, E.; Rubenstein, E.B. The burdens of cancer therapy. Clinical and economic outcomes of chemotherapy-induced mucositis. Cancer 2003, 98, 1531–1539. [Google Scholar] [CrossRef] [PubMed]
- Trotti, A.; Bellm, L.A.; Epstein, J.B.; Frame, D.; Fuchs, H.J.; Gwede, C.K.; Komaroff, E.; Nalysnyk, L.; Zilberberg, M.D. Mucositis incidence, severity and associated outcomes in patients with head and neck cancer receiving radiotherapy with or without chemotherapy: A systematic literature review. Radiother. Oncol. 2003, 66, 253–262. [Google Scholar] [CrossRef]
- Elting, L.S.; Cooksley, C.D.; Chambers, M.S.; Garden, A.S. Risk, outcomes, and costs of radiation-induced oral mucositis among patients with head-and-neck malignancies. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 1110–1120. [Google Scholar] [CrossRef] [PubMed]
- Villa, A.; Sonis, S.T. Mucositis: Pathobiology and management. Curr. Opin. Oncol. 2015, 27, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Blennow, O.; Ljungman, P.; Sparrelid, E.; Mattsson, J.; Remberger, M. Incidence, risk factors, and outcome of bloodstream infections during the pre-engraftment phase in 521 allogeneic hematopoietic stem cell transplantations. Transpl. Infect. Dis. 2014, 16, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Mego, M.; Holec, V.; Drgona, L.; Hainova, K.; Ciernikova, S.; Zajac, V. Probiotic bacteria in cancer patients undergoing chemotherapy and radiation therapy. Complement. Ther. Med. 2013, 21, 712–723. [Google Scholar] [CrossRef] [PubMed]
- Food and Agriculture Organization of the United Nations; World Health Organization. Probiotics in Food: Health and Nutritional Properties and Guidelines for Evaluation; FAO food and nutrition paper; Food and Agriculture Organization of the United Nations: Rome, Italy; World Health Organization: Geneva, Switzerland, 2006; p. 50. [Google Scholar]
- Byakika, S.; Mukisa, I.; Byenkya, Y.; Muyanja, C.; Byenkya Byaruhanga, Y. A Review of Criteria and Methods for Evaluating the Probiotic Potential of Microorganisms. Food Rev. Int. 2019, 427–466. [Google Scholar] [CrossRef]
- Wanden-Berghe, C.; Sanz-Valero, J. Systematic reviews in nutrition: Standardized methodology. Br. J. Nutr. 2012, 107 (Suppl. 2), S3–S7. [Google Scholar] [CrossRef] [PubMed]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. BMJ 2016, 355, i5239. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Jiang, C.; Wang, H.; Xia, C.; Dong, Q.; Chen, E.; Qiu, Y.; Su, Y.; Xie, H.; Zeng, L.; Kuang, J.; et al. A randomized, double-blind, placebo-controlled trial of probiotics to reduce the severity of oral mucositis induced by chemoradiotherapy for patients with nasopharyngeal carcinoma. Cancer 2019, 125, 1081–1090. [Google Scholar] [CrossRef]
- Gao, Z.; Guo, B.; Gao, R.; Zhu, Q.; Wu, W.; Qin, H. Probiotics modify human intestinal mucosa-associated microbiota in patients with colorectal cancer. Mol. Med. Rep. 2015, 12, 6119–6127. [Google Scholar] [CrossRef]
- Liu, Z.; Qin, H.; Yang, Z.; Xia, Y.; Liu, W.; Yang, J.; Zhang, H.; Yang, Z.; Wang, Y.; Zheng, Q. Randomised clinical trial: The effects of perioperative probiotic treatment on barrier function and post-operative infectious complications in colorectal cancer surgery-a double-blind study. Aliment. Pharmacol. Ther. 2011, 33, 50–63. [Google Scholar] [CrossRef] [PubMed]
- Gianotti, L.; Morelli, L.; Galbiati, F.; Rocchetti, S.; Coppola, S.; Beneduce, A.; Gilardini, C.; Zonenschain, D.; Nespoli, A.; Braga, M. A randomized double-blind trial on perioperative administration of probiotics in colorectal cancer patients. World J. Gastroenterol. 2010, 16, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Worthley, D.; Le Leu, R.; Whitehall, V.; Conlon, M.; Christophersen, C.; Belobrajdic, D.; Mallitt, K.A.; Hu, Y.; Irahara, N.; Ogino, S.; et al. A human, double-blind, placebo-controlled, crossover trial of prebiotic, probiotic, and synbiotic supplementation: Effects on luminal, inflammatory, epigenetic, and epithelial biomarkers of colorectal cancer. Am. J. Clin. Nutr. 2009, 90, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Friederich, P.; Verschuur, J.; van Heumen, B.; Roelofs, H.; Berkhout, M.; Nagtegaal, I.D.; van Oijen, M.G.H.; van Krieken, J.H.J.M.; Peters, W.H.M.; Nagengast, F.M. Effects of intervention with sulindac and inulin/VSL#3 on mucosal and luminal factors in the pouch of patients with familial adenomatous polyposis. Int. J. Colorectal. Dis. 2011, 26, 575–582. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lacouture, M.; Keefe, D.; Sonis, S.; Jatoi, A.; Gernhardt, D.; Wang, T.; Doherty, J.P.; Giri, N.; Nadanaciva, S.; O’Connell, J.; et al. A phase II study (ARCHER 1042) to evaluate prophylactic treatment of dacomitinib-induced dermatologic and gastrointestinal adverse events in advanced non-small-cell lung cancer. Ann. Oncol. 2016, 27, 1712–1718. [Google Scholar] [CrossRef] [PubMed]
- Hegazy, S.; El-Bedewy, M. Effect of probiotics on pro-inflammatory cytokines and NF-kappaB activation in ulcerative colitis. World J. Gastroenterol. 2010, 16, 4145–4151. [Google Scholar] [CrossRef] [PubMed]
- Groeger, D.; O’Mahony, L.; Murphy, E.F.; Bourke, J.F.; Dinan, T.G.; Kiely, B.; Shanahan, F.; Quigley, E.M. Bifidobacterium infantis 35624 modulates host inflammatory processes beyond the gut. Gut Microbes 2013, 4, 325–339. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Rath, G.K.; Chaudhary, S.P.; Thakar, A.; Mohanti, B.K.; Bahadur, S. Lactobacillus brevis CD2 lozenges reduce radiation- and chemotherapy-induced mucositis in patients with head and neck cancer: A randomized double-blind placebo-controlled study. Eur. J. Cancer (Oxf. Engl. 1990) 2012, 48, 875–881. [Google Scholar] [CrossRef] [PubMed]
- DESanctis, V.; Belgioia, L.; Cante, D.; LAPorta, M.; Caspiani, O.; Guarnaccia, R.; Argenone, A.; Muto, P.; Musio, D.; DEFelice, F.; et al. Lactobacillus brevis CD2 for Prevention of Oral Mucositis in Patients With Head and Neck Tumors: A Multicentric Randomized Study. Anticancer Res. 2019, 39, 1935–1942. [Google Scholar] [CrossRef] [PubMed]
- Consoli, M.; Da Silva, R.; Nicoli, J.; Bruna-Romero, O.; Da Silva, R.; De Vasconcelos Generoso, S.; Correia, M.I. Randomized Clinical Trial: Impact of Oral Administration of Saccharomyces boulardii on Gene Expression of Intestinal Cytokines in Patients Undergoing Colon Resection. J. Parenter. Enter. Nutr. 2016, 40, 1114–1121. [Google Scholar] [CrossRef] [PubMed]
- Wada, M.; Nagata, S.; Saito, M.; Shimizu, T.; Yamashiro, Y.; Matsuki, T.; Asahara, T.; Nomoto, K. Effects of the enteral administration of Bifidobacterium breve on patients undergoing chemotherapy for pediatric malignancies. Support Care Cancer 2010, 18, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Mangell, P.; Thorlacius, H.; Syk, I.; Ahrné, S.; Molin, G.; Olsson, C.; Jeppsson, B. Lactobacillus plantarum 299v does not reduce enteric bacteria or bacterial translocation in patients undergoing colon resection. Dig. Dis. Sci. 2012, 57, 1915–1924. [Google Scholar] [CrossRef] [PubMed]
- Ouwehand, A.; Tiihonen, K.; Saarinen, M.; Putaala, H.; Rautonen, N. Influence of a combination of Lactobacillus acidophilus NCFM and lactitol on healthy elderly: Intestinal and immune parameters. Br. J. Nutr. 2009, 101, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Tomás-Casterá, V.; Sanz-Valero, J.; Juan-Quilis, V. Estudio bibliométrico de la producción científica y de consumo de las revistas sobre nutrición indizadas en la red SciELO. Nutr. Hosp. 2013, 28, 969–970. [Google Scholar] [CrossRef] [PubMed]
- Manterola, C.; Asenjo-Lobos, C.; Otzen, T. Jerarquización de la evidencia: Niveles de evidencia y grados de recomendación de uso actual. Rev. Chil. Infectol. 2014, 31, 705–718. [Google Scholar] [CrossRef] [PubMed]
- Franco-Lopez, A.; Sanz-Valero, J.; Culebras, J.M. Publicar en castellano, o en cualquier otro idioma que no sea inglés, negativo para el factor de impacto y citaciones. J. Negat. No Posit. Results 2016, 1, 65–70. [Google Scholar] [CrossRef]
- Sanz-Valero, J.; Gil, Á.; Wanden-Berghe, C.; Martínez de Victoria, E. Análisis bibliométrico y temático de la producción científica sobre ácidos grasos omega-3 indizada en las bases de datos internacionales sobre ciencias de la salud. Nutr. Hosp. 2012, 27, 41–48. [Google Scholar] [CrossRef]
- Gibson, R.J.; Keefe, D.M.K.; Lalla, R.V.; Bateman, E.; Blijlevens, N.; Fijlstra, M.; King, E.E.; Stringer, A.M.; van der Velden, W.J.; Yazbeck, R.; et al. Systematic review of agents for the management of gastrointestinal mucositis in cancer patients. Support Care Cancer 2013, 21, 313–326. [Google Scholar] [CrossRef]
- Buts, J.P.; De Keyser, N. Effects of Saccharomyces boulardii on intestinal mucosa. Dig. Dis. Sci. 2006, 51, 1485–1492. [Google Scholar] [CrossRef]
- Sazawal, S.; Hiremath, G.; Dhingra, U.; Malik, P.; Deb, S.; Black, R.E. Efficacy of probiotics in prevention of acute diarrhoea: A meta-analysis of masked, randomised, placebo-controlled trials. Lancet Infect. Dis. 2006, 6, 374–382. [Google Scholar] [CrossRef]
- Szajewska, H.; Skórka, A.; Dylag, M. Meta-analysis: Saccharomyces boulardii for treating acute diarrhoea in children. Aliment. Pharmacol. Ther. 2007, 25, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Szajewska, H.; Skórka, A.; Ruszczyński, M.; Gieruszczak-Białek, D. Meta-analysis: Lactobacillus GG for treating acute diarrhoea in children. Aliment. Pharmacol. Ther. 2007, 25, 871–881. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.R.; Vargas, A.J. Probiotics for the Prevention of Pediatric Antibiotic-Associated Diarrhea. Explore (N. Y.) 2016, 12, 463–466. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Zhao, C.; Du, Y.; Zhang, Y.; Zhao, M.; Zhao, Q. Comparative efficacy and tolerability of probiotics for antibiotic-associated diarrhea: Systematic review with network meta-analysis. United Eur. Gastroenterol. J. 2018, 6, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Andrew, H.; Kirschner, B.S.; Guandalini, S. Is lactobacillus GG helpful in children with Crohn’s disease? Results of a preliminary, open-label study. J. Pediatr. Gastroenterol. Nutr. 2000, 31, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Lamprecht, M.; Bogner, S.; Schippinger, G.; Steinbauer, K.; Fankhauser, F.; Hallstroem, S.; Schuetz, B.; Greilberger, J.F. Probiotic supplementation affects markers of intestinal barrier, oxidation, and inflammation in trained men; a randomized, double-blinded, placebo-controlled trial. J. Int. Soc. Sports Nutr. 2012, 9, 45. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.D.; Suckling, C.A.; Peedle, G.Y.; Murphy, J.A.; Dawkins, T.G.; Roberts, M.G. An Exploratory Investigation of Endotoxin Levels in Novice Long Distance Triathletes, and the Effects of a Multi-Strain Probiotic/Prebiotic, Antioxidant Intervention. Nutrients 2016, 8, 733. [Google Scholar] [CrossRef]
- Shing, C.M.; Peake, J.M.; Lim, C.L.; Briskey, D.; Walsh, N.P.; Fortes, M.B.; Ahuja, K.D.; Vitetta, L. Effects of probiotics supplementation on gastrointestinal permeability, inflammation and exercise performance in the heat. Eur. J. Appl. Physiol. 2014, 114, 93–103. [Google Scholar] [CrossRef]
- Cremonini, F.; Di Caro, S.; Covino, M.; Armuzzi, A.; Gabrielli, M.; Santarelli, L.; Nista, E.C.; Cammarota, G.; Gasbarrini, G.; Gasbarrini, A. Effect of different probiotic preparations on anti-helicobacter pylori therapy-related side effects: A parallel group, triple blind, placebo-controlled study. Am. J. Gastroenterol. 2002, 97, 2744–2749. [Google Scholar] [CrossRef]
- Armuzzi, A.; Cremonini, F.; Bartolozzi, F.; Canducci, F.; Candelli, M.; Ojetti, V.; Cammarota, G.; Anti, M.; De Lorenzo, A.; Pola, P.; et al. The effect of oral administration of Lactobacillus GG on antibiotic-associated gastrointestinal side-effects during Helicobacter pylori eradication therapy. Aliment. Pharmacol. Ther. 2001, 15, 163–169. [Google Scholar] [CrossRef]
- Nista, E.C.; Candelli, M.; Cremonini, F.; Cazzato, I.A.; Zocco, M.A.; Franceschi, F.; Cammarota, G.; Gasbarrini, G.; Gasbarrini, A. Bacillus clausii therapy to reduce side-effects of anti-Helicobacter pylori treatment: Randomized, double-blind, placebo controlled trial. Aliment. Pharmacol. Ther. 2004, 20, 1181–1188. [Google Scholar] [CrossRef] [PubMed]
- Tolone, S.; Pellino, V.; Vitaliti, G.; Lanzafame, A.; Tolone, C. Evaluation of Helicobacter Pylori eradication in pediatric patients by triple therapy plus lactoferrin and probiotics compared to triple therapy alone. Ital. J. Pediatr. 2012, 38, 63. [Google Scholar] [CrossRef]
- Ahmad, K.; Fatemeh, F.; Mehri, N.; Maryam, S. Probiotics for the treatment of pediatric helicobacter pylori infection: A randomized double blind clinical trial. Iran. J. Pediatr. 2013, 23, 79–84. [Google Scholar] [PubMed]
- Hauser, G.; Salkic, N.; Vukelic, K.; JajacKnez, A.; Stimac, D. Probiotics for standard triple Helicobacter pylori eradication: A randomized, double-blind, placebo-controlled trial. Medicine (Baltim.) 2015, 94, e685. [Google Scholar] [CrossRef]
- Chang, C.W.; Liu, C.Y.; Lee, H.C.; Huang, Y.H.; Li, L.H.; Chiau, J.S.C.; Wang, T.E.; Chu, C.H.; Shih, S.C.; Tsai, T.H.; et al. Lactobacillus casei Variety rhamnosus Probiotic Preventively Attenuates 5-Fluorouracil/Oxaliplatin-Induced Intestinal Injury in a Syngeneic Colorectal Cancer Model. Front. Microbiol. 2018, 9, 983. [Google Scholar] [CrossRef] [PubMed]
- Justino, P.F.C.; Melo, L.F.M.; Nogueira, A.F.; Costa, J.V.G.; Silva, L.M.N.; Santos, C.M.; Mendes, W.O.; Costa, M.R.; Franco, A.X.; Lima, A.A.; et al. Treatment with Saccharomyces boulardii reduces the inflammation and dysfunction of the gastrointestinal tract in 5-fluorouracil-induced intestinal mucositis in mice. Br. J. Nutr. 2014, 111, 1611–1621. [Google Scholar] [CrossRef]
- Justino, P.F.C.; Melo, L.F.M.; Nogueira, A.F.; Morais, C.M.; Mendes, W.O.; Franco, A.X.; Souza, E.P.; Ribeiro, R.A.; Souza, M.H.; Soares, P.M. Regulatory role of Lactobacillus acidophilus on inflammation and gastric dysmotility in intestinal mucositis induced by 5-fluorouracil in mice. Cancer Chemother. Pharmacol. 2015, 75, 559–567. [Google Scholar] [CrossRef]
- Kato, S.; Hamouda, N.; Kano, Y.; Oikawa, Y.; Tanaka, Y.; Matsumoto, K.; Amagase, K.; Shimakawa, M. Probiotic Bifidobacterium bifidum G9-1 attenuates 5-fluorouracil-induced intestinal mucositis in mice via suppression of dysbiosis-related secondary inflammatory responses. Clin. Exp. Pharmacol. Physiol. 2017, 44, 1017–1025. [Google Scholar] [CrossRef]
- Tang, Y.; Wu, Y.; Huang, Z.; Dong, W.; Deng, Y.; Wang, F.; Li, M.; Yuan, J. Administration of probiotic mixture DM#1 ameliorated 5-fluorouracil-induced intestinal mucositis and dysbiosis in rats. Nutrition 2017, 33, 96–104. [Google Scholar] [CrossRef]
- Mi, H.; Dong, Y.; Zhang, B.; Wang, H.; Peter, C.C.K.; Gao, P.; Fu, H.; Gao, Y. Bifidobacterium Infantis Ameliorates Chemotherapy-Induced Intestinal Mucositis Via Regulating T Cell Immunity in Colorectal Cancer Rats. Cell. Physiol. Biochem. 2017, 42, 2330–2341. [Google Scholar] [CrossRef]
- Yuan, K.T.; Yu, H.L.; Feng, W.D.; Chong, P.; Yang, T.; Xue, C.L.; Yu, M.; Shi, H.P. Bifidobacterium infantis has a beneficial effect on 5-fluorouracil-induced intestinal mucositis in rats. Benef. Microbes 2015, 6, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Bowen, J.M.; Stringer, A.M.; Gibson, R.J.; Yeoh, A.S.J.; Hannam, S.; Keefe, D.M.K. VSL#3 probiotic treatment reduces chemotherapy-induced diarrhea and weight loss. Cancer Biol. Ther. 2007, 6, 1449–1454. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority. Update of the List of QPS-Recommended Biological Agents Intentionally Added to Food or Feed as Notified to EFSA 10: Suitability of Taxonomic Units Notified to EFSA until March 2019. 2019. Available online: https://www.efsa.europa.eu/en/efsajournal/pub/5753 (accessed on 16 August 2019).
- Vásquez-Morales, A.; Sanz-Valero, J.; Wanden-Berghe, C. Ejercicio excéntrico como recurso físico preventivo en personas mayores de 65 años: Revisión sistemática de la literatura científica. Enferm. Clín. 2013, 23, 48–55. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Grade 0 | Grade 1 | Grade 2 | Grade 3 | Grade 4 |
|---|---|---|---|---|
| No signs or symptoms | Painless ulcers, edema or mild pain | Painful erythema, edema or ulcers but the patient can eat | Idem grade 2 but unable to eat | Parenteral or enteral feeding is needed |
| Author, Year | Design | Country | Patients | Pathology | Monitoring | Intervention | Results |
|---|---|---|---|---|---|---|---|
| Jiang 2008 [20] | Randomized, double-blind, placebo-controlled trial monocentric | China | 99 M/F = 58/35 Median age = 51 years | Advanced NC and undergoing CCRT | seven weeks | CCRT and B.longum, L.lactis, E.faecium. (six capsules/day) OM incidence, the short-term curative effect, the immune index, and fecal flora changes. | Probiotic combination reduced the incidence of grade 3 OM and had significantly enhanced the immunity of patients and was beneficial for restoring microbial diversity after the end of CCRT. |
| Gao 2015 [21] | Randomized prospective placebo-controlled trial. | China | 22 M/F = 12/10 Median age = 70 years | CRC | five days perioperative surgery | B.longum L.acidophyllus, Efaecalis (1:1:1). 6 × 107 CFU/day. Oral probiotics were able to alter the microbial composition and improve gut microbiota in patients with CRC. | Probiotic supplements can effectively alter the composition, richness, and diversity of the gut microbiota |
| Liu 2010 [22] | Randomized, double-blind, placebo-controlled, prospective trial | China | 100 M/F = 59/41 Median age = 65 years | CRC | 16 days (six days pre-and 10 days post-operative) | L.acidophillus, L.plantarum, B.longum (1 × 1014 CFU/day). Preoperative administration could prevent post-operative alterations in intestinal permeability, integrity and microbiota. | Probiotics can improve the integrity of the gut mucosal barrier and balance of the gut microbiota, and they play a role in decreasing the infectious rate. |
| Gianotti 2010 [23] | Prospective, randomized, double-blind, clinical trial | Italia | 31 M/F = 22/11 Median age = 64 years | CRC | six days (three pre- and three post-operative) | B.longum and L.johnsonii (2 × 107 and 2 × 109 CFU/day). Assess adhesion to the colonic mucosa, reduce concentration of pathogens in stools, and modulate local immune function. | L.johnsonii but not B.longum, adhere to the colonic mucosa, affect intestinal microbiota by reducing the concentration of pathogens, and modulate local immunity. |
| Worthley 2009 [24] | Randomized, double-blind, placebo-controlled crossover trial | Australian | 20 M/F = 13/7 Median age = 65.5 years | Healthy | 16 weeks | (B.animalis sub.lactis 5 × 109 CFU/day + 25 g/day HAMS), Synbiotic. Characterized the luminal and biological consequences of these supplements and placed them in the context of colorectal carcinogenesis. | Synbiotic generated a significantly different fecal bacteria profile when compared with either HAMS or B.animalis sub.lactis supplementation alone. |
| Friederich 2011 [25] | Randomized pilot study | Netherlands | 31 M/F = 20/11 Median age = 37 years | FAP and IPAA | six weeks | Sulindac (300 mg/day), VSL#3 (9 × 1011 CFU/day) + Inulin (12g/day). Endpoints: Risk parameters cell proliferation and GST detoxification capacity in the pouch mucosa. SCFA contents, pH, and cytotoxicity of fecal water. | Study revealed non-significant decreased cell proliferation and increased detoxification capacity after treatment with sulindac or VSL#3/inulin (prebiotic). |
| Lacouture 2016 [26] | Multicenter, double cohort placebo-controlled randomized phase II trial | USA and Republic. of Korea | 173 M/F = 98/75 Median age = 66 years | Advanced NSCLC | four to eight weeks according to treatment | Dacomitinib all cohorts Cohort I: Doxycycline + placebo. Cohort II: AD+ VSL#3. Cohorts I and II assessment incidence of all grade and grade ≥ 2 SDAEI and QoL. Cohort II assessment incidence of all grade and grade ≥ 2 diarrhea and mucositis | Doxycycline was effective as a prophylactic treatment for dacomitinib-induced grade ≥ 2 SDAEI. Both doxycycline and AD reduced the negative impact in patient-reported dermatologic AEs. The probiotic was not effective for preventing diarrhea or mucositis |
| Hegazy 2010 [27] | Multicenter, placebo-controlled randomized | Egypt | 40 M/F = 29/11 Median age = 47 years | UC | eight weeks | L.delbruekii and L.fermentum 1 × 1010 CFU/day. Effect in patients with ulcerative colitis (UC), and their effect on inflammatory mediators and NF-κB activation | Oral supplementation with probiotics could be helpful in maintaining remission and preventing relapse of UC |
| Groeger 2013 [28] | Randomized, double-blind, placebo-controlled | Ireland | 118 M and F = 48 (UC and Psoriasis) F = 83 (CFS and healthy) | UC. Psoriasis. CFS. Healthy. | six - eight weeks | B. infantis strain 35,624 1 × 1010 CFU/day Assessed the impact on inflammatory biomarker and plasma cytokine levels in UC, CFS, and psoriasis | B.infantis strain 35,624, was enough to reduce systemic inflammatory biomarkers in both gastrointestinal and extra-intestinal inflammatory disorders. |
| Sharma 2012 [29] | Randomized, double-blind, single center, placebo controlled | India | 200 M/F = 188/12 Median age = 51 years | HNSCC stage II–IVA | 25 months | L.brevis strain CD2 2 × 109 efficacy in preventing oral mucositis in patients receiving CRT for HNSCC. | L.brevis strain CD2 proved to be safe and efficacious in reducing the incidence of severe oral mucositis in patients with HNSCC undergoing combination radiation and chemotherapy |
| D Sanctis 2019 [30] | Multicentric, phase III, open label, randomized controlled | Italy | 68 M/F = 53/15 Median age = 60 years | HNC | 39 months | L.brevis strain CD2 2 × 109 primary endpoint was the incidence of grade 3 or 4 oropharyngeal mucositis during radiotherapy treatment | L.brevis strain CD2 not able to confirm the beneficial effects in reducing the rate of grade 3–4 RT-induced OM in patients with HNC. |
| Consoli 2015 [31] | Randomized controlled | Brazil | 33 M/F = 15/18 Median age = 55 years | RC | seven days before surgery and was interrupted on the operation day. | S.boulardii 0.5 × 109 CFU to assess the role of preoperative treatment on mRNA levels for immunomodulatory cytokines in the colonic mucosa of patients. | S.boulardii downregulates both pro- and anti-inflammatory cytokines in the intestinal colonic mucosa with no statistical impact on postoperative infection rates. |
| Wada 2009 [32] | Randomized, placebo-controlled single-blinded | Japan | 40 M/F = 16/24Median age = 6.5 years | IC | one to five weeks | B.breve strain Yakult 109 CFU, on its ability to prevent infection, fecal micro flora, and intestinal environments in cancer patients on chemotherapy. | B.breve strain Yakult could be an effective approach for achieving clinical benefits in immunocompromised hosts by improving their intestinal environments (mucositis, fever, diarrhea and bacteremia). |
| Mangell 2012 [33] | Randomized double-blinded, placebo-controlled | Sweden | 64 M/F = 36/28Median age = 72 years | RC | six months | L.plantarum strain 299v 1011 CFU on the intestinal load of potentially pathogenic bacteria, bacterial translocation, and cell proliferation in elective colon surgery. | L.plantarum strain 299v was established in the intestine, but no inhibitory effect on enteric bacteria, bacterial translocation, or postoperative complications was found |
| Ouwehan. 2008 [34] | Randomized double-blinded, placebo-controlled | Finland | 47 M/F = 12/35Median age = 71 years | Healthy and regular use of NSAID | six weeks | Synbiotic (lactitol + 2 × 109 CFU L.acidophyllus strain NCFM) on improve bowel function and immune function. | Synbiotic twice daily was associated with modest improvement in stool frequency without any side-effects and improved microbiota composition and mucosal. |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | T | % | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Jiang [20] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.75 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0.8 | 1 | 1 | 0.5 | 1 | 22.5 | 90 |
| Gao [21] | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 0.5 | 0 | 0.5 | 0.5 | 1 | 1 | 0.5 | 0.5 | 1 | 1 | NA | 0.5 | 0 | 1 | 1 | 0 | 0 | 1 | 15 | 62 |
| Liu [22] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 24.5 | 98 |
| Gianotti [23] | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0.5 | NA | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 18.5 | 77 |
| Worthley [24] | 0 | 0.5 | 0.5 | 1 | 1 | 0.5 | 0 | 0 | 0 | 1 | 0.5 | 1 | 0.5 | 0 | 0 | 1 | 0.5 | NA | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 15 | 62 |
| Lacouture [26] | 0.5 | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 0 | 0 | 0 | 0.5 | 1 | 0.75 | 0 | 1 | 1 | 0.5 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 16.2 | 65 |
| Hegazy [27] | 0.5 | 1 | 0.5 | 1 | 1 | 0.5 | 0 | 0 | 0 | 0 | 0 | 0.5 | 0 | 0 | 1 | 1 | 0.5 | 1 | 0 | 0 | 1 | 0.5 | 0 | 0 | 0 | 9.5 | 38 |
| Groeger [28] | 0.5 | 1 | 0.5 | 1 | 1 | 0.5 | 0 | 0 | 0 | 1 | 0.5 | 1 | 0 | 0 | 0 | 1 | 0.5 | NA | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 10.5 | 44 |
| Sharma [29] | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 | 1 | 1 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 0.5 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 22 | 88 |
| De Sanctis [30] | 0.5 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | NA | 1 | 0.75 | 1 | 1 | 1 | 0.5 | 1 | 1 | 1 | 0.5 | 1 | 1 | 0 | 1 | 20.2 | 84 |
| Consoli [31] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | NA | 0.5 | 1 | 0 | 1 | 1 | 0.5 | NA | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 20 | 87 |
| Wada [32] | 0.5 | 1 | 1 | 1 | 1 | 1 | 0 | 0.5 | 0 | 0 | 0 | 1 | 0.5 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 1 | 0.5 | 1 | 0 | 0 | 0 | 14 | 56 |
| Mangell [33] | 0.5 | 1 | 1 | 1 | 1 | 0.5 | 1 | 0 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0 | 1 | 1 | 0.5 | NA | 1 | 1 | 0.5 | 1 | 0 | 0 | 1 | 16.5 | 69 |
| Ouwehand [34] | 0.5 | 1 | 1 | 1 | 1 | 0.5 | 0 | 0 | 0 | 1 | 0.5 | 0.5 | 0.5 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 14.5 | 58 |
| Friederich [25] | 0.5 | 1 | 0.5 | 1 | 1 | 0.5 | 0 | 0 | 0 | 1 | 0 | 0.5 | 0.5 | 0.5 | 1 | 1 | 0.5 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 16 | 64 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Picó-Monllor, J.A.; Mingot-Ascencao, J.M. Search and Selection of Probiotics That Improve Mucositis Symptoms in Oncologic Patients. A Systematic Review. Nutrients 2019, 11, 2322. https://doi.org/10.3390/nu11102322
Picó-Monllor JA, Mingot-Ascencao JM. Search and Selection of Probiotics That Improve Mucositis Symptoms in Oncologic Patients. A Systematic Review. Nutrients. 2019; 11(10):2322. https://doi.org/10.3390/nu11102322
Chicago/Turabian StylePicó-Monllor, José Antonio, and José Manuel Mingot-Ascencao. 2019. "Search and Selection of Probiotics That Improve Mucositis Symptoms in Oncologic Patients. A Systematic Review" Nutrients 11, no. 10: 2322. https://doi.org/10.3390/nu11102322
APA StylePicó-Monllor, J. A., & Mingot-Ascencao, J. M. (2019). Search and Selection of Probiotics That Improve Mucositis Symptoms in Oncologic Patients. A Systematic Review. Nutrients, 11(10), 2322. https://doi.org/10.3390/nu11102322