Micronutrient Deficiencies, Nutritional Status and the Determinants of Anemia in Children 0–59 Months of Age and Non-Pregnant Women of Reproductive Age in The Gambia

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
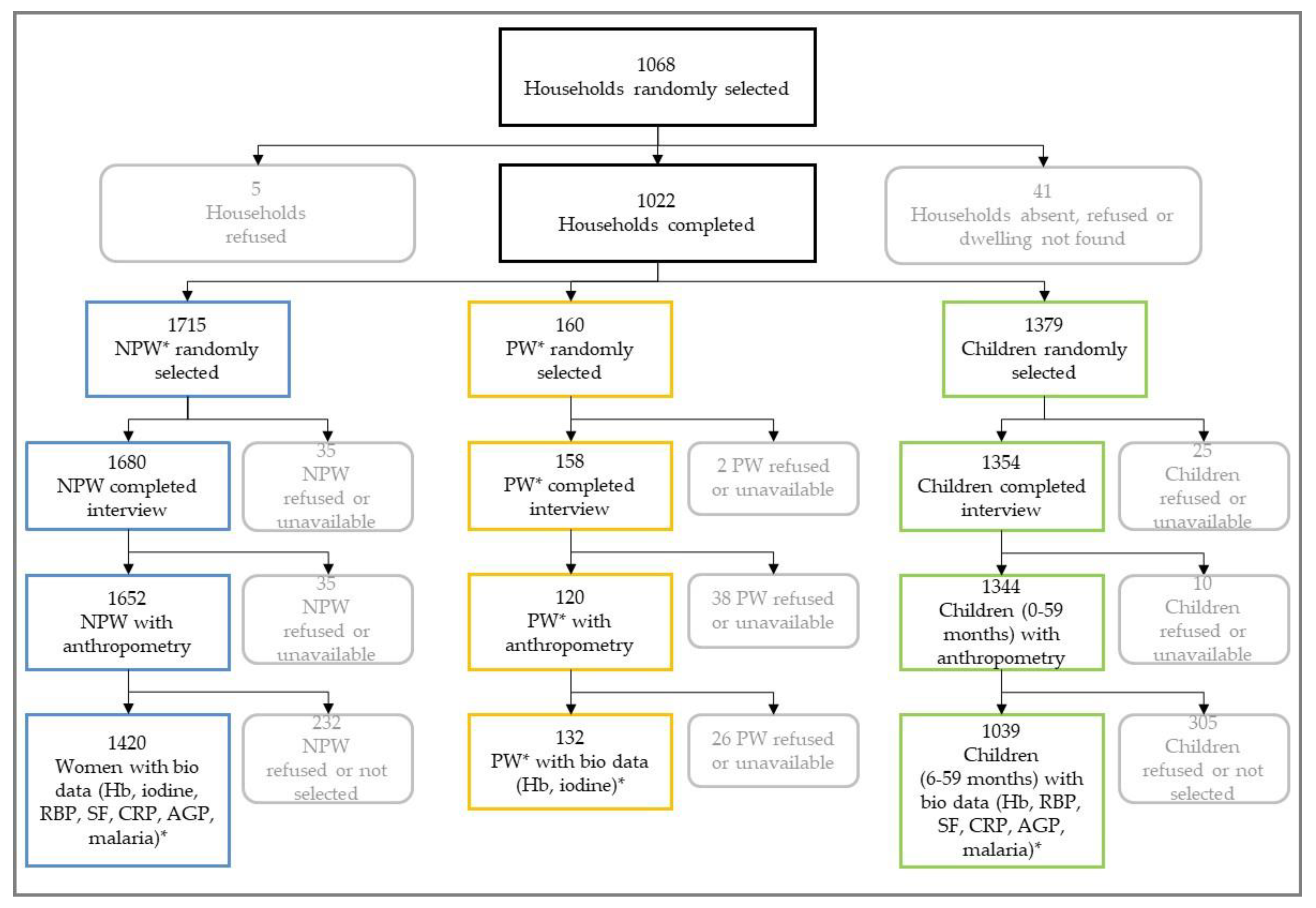
2.1. Survey Design and Participants
2.2. Data Collection
2.3. Anthropometric Measurements
2.4. Biofluid Collection and Laboratory Analyses
2.5. Parameters and Clinical Thresholds
2.6. Data Management and Statistical Analysis
2.7. Ethics and Consent
3. Results
3.1. Children
3.1.1. Anthropometric and Micronutrient Indicators
3.1.2. Bivariate Analyses of Anemia Risk Factors
3.1.3. Multivariate Analyses
3.2. Women
3.2.1. Anthropometric and Micronutrient Indicators
3.2.2. Bivariate Analyses of Anemia Risk Factors
3.2.3. Multivariate Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Stevens, G.A.; Finucane, M.M.; De-Regil, L.M.; Paciorek, C.J.; Flaxman, S.R.; Branca, F.; Peña-Rosas, J.P.; Bhutta, Z.A.; Ezzati, M.; Nutrition Impact Model Study Group. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: A systematic analysis of population-representative data. Lancet Glob. Heal. 2013. [Google Scholar] [CrossRef]
- WHO. Nutritional Anaemias: Tools for Effective Prevention and Control; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Allen, L.; DeBenoist, B.; Dary, O.; Hurrell, R. Guidelines on Food Fortification with Micronutrients; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Engle-Stone, R.; Aaron, G.J.; Huang, J.; Wirth, J.P.; Namaste, S.M.; Williams, A.M.; Peerson, J.M.; Rohner, F.; Varadhan, R.; Addo, O.Y.; et al. Predictors of anemia in preschool children: Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) project. AJCN 2017, 106, 402–415. [Google Scholar]
- Rohner, F.; Woodruff, B.A.; Aaron, G.J.; Yakes, E.A.; Lebanan, M.A.O.; Rayco-Solon, P.; Saniel, O.P. Infant and young child feeding practices in urban Philippines and their associations with stunting, anemia, and deficiencies of iron and vitamin A. Food Nutr. Bull. 2013, 34, S17–S34. [Google Scholar] [CrossRef] [PubMed]
- WHO. Worldwide Prevalence of Anaemia 1993–2005; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- WHO. The Global Prevalence of Anaemia in 2011; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Kassebaum, N.J.; Jasrasaria, R.; Naghavi, M.; Wulf, S.K.; Johns, N.; Lozano, R.; Regan, M.; Weatherall, D.; Chou, D.P.; Eisele, T.P.; et al. A systematic analysis of global anemia burden from 1990 to 2010. Blood 2014. [Google Scholar] [CrossRef] [PubMed]
- Petry, N.; Olofin, I.; Hurrell, R.; Boy, E.; Wirth, J.; Moursi, M.; Donahue Angel, M.; Rohner, F. The proportion of anemia associated with iron deficiency in low, medium, and high human development index countries: A systematic analysis of national surveys. Nutrients 2016, 8, 693. [Google Scholar] [CrossRef]
- Green, R.; Datta Mitra, A. Megaloblastic Anemias: Nutritional and Other Causes. Med. Clin. N. Am. 2017. [Google Scholar] [CrossRef] [PubMed]
- The Gambia Bureau of Statistics; ICF International. The Gambia Demographic and Health Survey 2013; The Gambia and Rockville: Banjul, Gambia, 2014.
- National Nutrition Agency (NaNA)-Gambia; UNICEF; GBOS; GroundWork. Gambia National Micronutrient Survey 2018; National Nutrition Agency: Banjul, Gambia, 2019.
- Erhardt, J.G.; Estes, J.E.; Pfeiffer, C.M.; Biesalski, H.K.; Craft, N.E. Combined measurement of ferritin, soluble transferrin receptor, retinol binding protein, and C-reactive protein by an inexpensive, sensitive, and simple sandwich enzyme-linked immunosorbent assay technique. J. Nutr. 2004. [Google Scholar] [CrossRef]
- Qiagen. QIAamp® DNA Mini and Blood Mini Handbook. 2016. Available online: https://www.qiagen.com/jp/resources/download.aspx?id=62a200d6-faf4-469b-b50f-2b59cf738962&lang=en (accessed on 19 September 2019).
- Hofmann, N.; Mwingira, F.; Shekalaghe, S.; Robinson, L.J.; Mueller, I.; Felger, I. Ultra-Sensitive Detection of Plasmodium falciparum by Amplification of Multi-Copy Subtelomeric Targets. PLoS Med. 2015. [Google Scholar] [CrossRef]
- Dunn, J.; Crutchfield, H.; Gutekunst, R.; Dunn, A.D. Two simple methods for Measuring Iodine in Urine. Thyroid J. 1993, 3, 119–123. [Google Scholar] [CrossRef]
- World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Namaste, S.; Rohner, F.; Huang, J.; Bhushan, N.L.; Flores-Ayala, R.; Kupka, R.; Mei, Z.; Rawat, R.; Williams, A.M.; Raiten, D.J.; et al. Approaches to understand and adjust ferritin concentrations in the presence of inflammation in preschool-aged children and women of reproductive age: A multi-country analysis. Am. J. Clin. Nutr. 2017, 106, 359S–371S. [Google Scholar]
- WHO/CDC. Assessing the Iron Status of a Population, Second Edition Including Literature Reviews; WHO/CDC: Geneva, Switzerland, 2007. [Google Scholar]
- Larson, L.M.; Namaste, S.M.; Williams, A.M.; Engle-Stone, R.; Addo, O.Y.; Suchdev, P.S.; Wirth, J.P.; Temple, V.; Serdula, M.; Northrop-Clewes, C.A. Adjusting retinol-binding protein concentrations for inflammation: Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) project. Am. J. Clin Nutr. 2017, 106, 390S–401S. [Google Scholar] [CrossRef] [PubMed]
- Tanumihardjo, S.A. Biomarkers of vitamin A status: What do they mean? World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Thurnham, D.I.; McCabe, G.P.; Northrop-Clewes, C.A.; Nestel, P. Effects of subclinical infection on plasma retinol concentrations and assessment of prevalence of vitamin a deficiency: Meta-analysis. Lancet 2003. [Google Scholar] [CrossRef]
- Rohner, F.; Zimmermann, M.; Jooste, P.; Pandav, C.; Caldwell, K.; Raghavan, R.; Raiten, D.J. Biomarkers of Nutrition for Development—Iodine Review. J. Nutr. 2014. [Google Scholar] [CrossRef] [PubMed]
- WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr. Suppl. 2006, 450, 76–85. [Google Scholar]
- WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards: Head Circumference-for-Age, Arm Circumference-for-Age, Triceps Skinfold-for-Age and Subscapular Skinfold-for-Age: Methods and Development; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Shetty, P.S.; James, W.P.T. Body Mass Index: A Measure of Chronic Energy Deficiency in Adults; Food and Agriculture Organization: Rome, Italy, 1994. [Google Scholar]
- Kolenikov, S. Epctile—Estimation and Inference for Percentiles. Available online: http://staskolenikov.net/stata (accessed on 19 September 2019).
- Woodruff, B.; Rohner, F.; Kupka, R. Statistical Considerations in the Analysis and Presentation of Urinary Iodine Concentration (UIC) in Population-Based Surveys. Presentation 0077; Micronutrient Forum 2016, Cancun, Mexico. Available online: https://micronutrientforum.org/content/user_files/gravity_forms/4-4d8669c7ff472a0ab6828d5f1def9322/2017/05/Statistics-of-iodine-status-measurement-FINAL-submit-to-MN-Forum.pdf (accessed on 19 September 2019).
- Sribney, W. Stepwise Regression with the Svy Commands. 2018. Available online: https://www.stata.com/support/faqs/statistics/stepwise-regression-with-svy-commands/ (accessed on 19 September 2019).
- Rockhill, B.; Newman, B.; Weinberg, C. Use and misuse of population attributable fractions. Am. J. Public Health 1998. [Google Scholar] [CrossRef] [PubMed]
- Engle-Stone, R.; Nankap, M. Plasma Ferritin and Soluble Transferrin Receptor Concentrations and Body Iron Stores Identify Similar Risk Factors for Iron Deficiency but Result in Different Estimates. J. Nutr. 2013. [Google Scholar] [CrossRef] [PubMed]
- Rohner, F.; Northrop-Clewes, C.; Tschannen, A.B.; Bosso, P.E.; Kouassi-Gohou, V.; Erhardt, J.G.; Bui, M.; Zimmermann, M.B.; Mascie-Taylor, C.N. Prevalence and public health relevance of micronutrient deficiencies and undernutrition in pre-school children and women of reproductive age in Côte d’Ivoire, West Africa. Public Health Nutr. 2014. [Google Scholar] [CrossRef]
- Wirth, J.P.; Rohner, F.; Woodruff, B.A.; Chiwile, F.; Yankson, H.; Koroma, A.S.; Russel, F.; Sesay, F.; Dominguez, E.; Petry, N.; et al. Anemia, micronutrient deficiencies, and malaria in children and women in Sierra Leone prior to the Ebola outbreak—Findings of a cross-sectional study. PLoS ONE 2016, 11. [Google Scholar] [CrossRef]
- UNICEF; Liberia Institute of Statistics. Liberia National Micronutrient Survey 2011 Selected Preliminary Findings; UNICEF: Monrovia, CA, USA, 2011. [Google Scholar]
- UoG; GroundWork; KEMRI; UNICEF. Ghana Micronutrient Survey 2017; UoG: Accra, Ghana, 2017. [Google Scholar]
- Thurnham, D.I.; McCabe, L.D.; Haldar, S.; Wieringa, F.T.; Northrop-Clewes, C.A.; McCabe, G.P. Adjusting plasma ferritin concentrations to remove the effects of subclinical inflammation in the assessment of iron deficiency: A meta-analysis. Am. J. Clin. Nutr. 2010, 92, 546–555. [Google Scholar] [CrossRef] [PubMed]
- Petry, N.; Egli, I.; Gahutu, J.B.; Tugirimana, P.L.; Boy, E.; Hurrell, R. Phytic Acid Concentration Influences Iron Bioavailability from Biofortified Beans in Rwandese Women with Low Iron Status. J. Nutr. 2014. [Google Scholar] [CrossRef]
- WHO. Global Prevalence of Vitamin A Deficiency in Populations at Risk 1995–2005: WHO Global Database on Vitamin A Deficiency; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Penniston, K.L.; Tanumihardjo, S.A. The acute and chronic toxic effects of vitamin A. Am. J. Clin. Nutr. 2006, 83, 191–201. [Google Scholar] [CrossRef] [PubMed]
- WHO. Assessment of Iodine Deficiency Disorders and Monitoring their Elimination: A Guide for Programme Managers; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- ICCIDD. National Iodine Deficiency Disorder Survey—The Gambia; ICCIDD: Banjul, Gambia, 1999. [Google Scholar]
- WHO. Nutrition Landscape Information System (NLIS): Country Profile Indicators—Interpretation Guide; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Lin, A.; Arnold, B.F.; Afreen, S.; Goto, R.; Huda, T.M.N.; Haque, R.; Raqib, R.; Unicomb, L.; Ahmed, T.; Colford, J.M., Jr.; et al. Household environmental conditions are associated with enteropathy and impaired growth in rural Bangladesh. Am. J. Trop. Med. Hyg. 2013, 89, 130. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.C.; Joshi, N.; Lohani, M.; Singh, R.; Bhatta, N.; Rogers, B.; Griffiths, J.K.; Ghosh, S.; Mahato, S.; Singh, P.; et al. Head growth of undernourished children in rural Nepal: Association with demographics, health and diet. Paediatr. Int. Child Health 2016. [Google Scholar] [CrossRef] [PubMed]
- Veena, S.R.; Krishnaveni, G.V.; Wills, A.K.; Kurpad, A.V.; Muthayya, S.; Hill, J.C.; Karat, S.C.; Nagarajaiah, K.K.; Fall, C.H.; Srinivasan, K. Association of birthweight and head circumference at birth to cognitive performance in 9-to 10-year-old children in South India: Prospective birth cohort study. Pediatr. Res. 2010. [Google Scholar] [CrossRef] [PubMed]
- Abarca-Gómez, L.; Abdeen, Z.A.; Hamid, Z.A.; Abu-Rmeileh, N.M.; Acosta-Cazares, B.; Acuin, C.; Adams, R.J.; Aekplakorn, W.; Afsana, K.; Aguilar-Salinas, C.A.; et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017. [Google Scholar] [CrossRef]
- Engle-Stone, R.; Williams, T.; Nankap, M.; Ndjebayi, A.; Gimou, M.M.; Oyono, Y.; Tarini, A.; Brown, K.; Green, R. Prevalence of inherited hemoglobin disorders and relationships with anemia and micronutrient status among children in Yaoundé and Douala, Cameroon. Nutrients 2017, 9, 693. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| National | Urban | Rural | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic a | N | % b / Mean/ Median | 95%CI c | N | % b / Mean/ Median | 95%CI | N | % b / Mean/ Median | 95%CI c | p-Value d |
| Nutritional status e | ||||||||||
| Stunting | ||||||||||
| HAZ, mean | 1337 | −0.71 | (−0.82, −0.60) | 543 | −0.57 | (−0.69, −0.44) | 794 | −0.97 | (−1.15, −0.78) | <0.001 |
| Any stunting, % | 1337 | 15.7 | (13.2, 18.4) | 543 | 11.8 | (8.9, 15.3) | 794 | 22.4 | (19.1, 26.2) | <0.005 |
| Severe stunting, % | 1337 | 4.9 | (3.3, 7.3) | 543 | 3.9 | (1.9, −8.0) | 794 | 6.6 | (5.1, 8.5) | 0.175 |
| Wasting | ||||||||||
| WHZ, mean | 1338 | −0.39 | (−0.48, −0.31) | 547 | −0.28 | (−0.37, 0.18) | 791 | −0.60 | (−0.70, −0.49) | <0.0001 |
| Any wasting, % | 1338 | 5.8 | (4.1, 8.1) | 547 | 4.4 | (2.4, 8.1) | 791 | 8.2 | (6.2, 10.7) | 0.07 |
| Severe wasting, % | 1338 | 1.2 | (0.7, 2.2) | 547 | 0.8 | (0.3, 2.3) | 791 | 1.9 | (1.0, 3.6) | 0.146 |
| Underweight | ||||||||||
| WAZ, mean | 1344 | −0.65 | (−0.74, −0.58) | 548 | −0.51 | (−0.59, −0.43) | 796 | −0.92 | (−1.03, −0.81) | <0.0001 |
| Any underweight, % | 1344 | 10.6 | (8.4, 13.2) | 548 | 7.8 | (5.1, 11.6) | 796 | 15.7 | (3.2, 18.6) | <0.005 |
| Severe underweight, % | 1344 | 1.9 | (1.2, 3.0) | 548 | 1.0 | (0.4, 2.5) | 796 | 3.4 | (2.2, 5.2) | <0.05 |
| Head circumference | ||||||||||
| Head circumference, mean | 1324 | −0.47 | (−0.55, −0.38) | 535 | −0.43 | (−0.53, −0.33) | 789 | −0.53 | (−0.67, −0.39) | 0.234 |
| Microcephaly, % | 1324 | 7.4 | (5.1, 10.7) | 535 | 5.8 | (2.9, 11.5) | 789 | 10.0 | (8.2, 12.1) | 0.13 |
| Micronutrient status f | ||||||||||
| Hemoglobin concentration | ||||||||||
| Hemoglobin (g/L), mean | 1014 | 107.9 | (106.7, 109.1) | 399 | 109.3 | (107.6, 110.9) | 615 | 105.7 | (103.9, 107.5) | <0.001 |
| Any anemia f, % | 1014 | 50.4 | (45.9, 54.8) | 399 | 46.0 | (40.1, 51.9) | 615 | 57.5 | (51.1, 63.6) | <0.05 |
| Severe anemia f, % | 1014 | 0.9 | (0.4, 2.1) | 399 | 0.9 | (0.2, 3.3) | 615 | 0.9 | (0.5, 1.7) | 0.9865 |
| Iron status g, h | ||||||||||
| Ferritin (µg/L), median | 1012 | 9.17 | (7.34, 10.68) | 399 | 10.8 | (8.30, 13.23) | 613 | 8.03 | (7.40, 8.66) | |
| Iron deficiency, % | 1012 | 59.0 | (51.3, 66.4) | 399 | 54.0 | (42.5, 65.1) | 613 | 67.1 | (61.2, 72.5) | <0.05 |
| Iron deficiency anemia, % | 1007 | 38.5 | (33.7, 43.5) | 396 | 33.8 | (27.4, 40.8) | 611 | 46.0 | (40.0, 52.0) | <0.01 |
| Vitamin A status g, i | ||||||||||
| RBP (µmol/L), mean | 1012 | 0.93 | (0.89, 0.97) | 399 | 0.97 | (0.91, 1.03) | 613 | 0.87 | (0.85, 0.89) | <0.01 |
| Vitamin A deficiency | 1012 | 18.3 | (14.5, 22.8) | 399 | 13.8 | (8.5, 21.6) | 613 | 25.5 | (21.4, 30.0) | <0.05 |
| Characteristic | N | Anemia %a, b | (95% CI)c | Chi-Square p-Value d |
|---|---|---|---|---|
| Age group (in months) | ||||
| 6–11 | 103 | 64.2 | (43.0, 81.0) | <0.005 |
| 12–23 | 230 | 59.0 | (43.7, 72.7) | |
| 24–35 | 216 | 63.2 | (57.3, 68.7) | |
| 36–47 | 257 | 36.2 | (28.0, 45.3) | |
| 48–59 | 208 | 35.6 | (26.4, 46.1) | |
| Sex | ||||
| Male | 523 | 55.4 | (48.9, 61.8) | <0.05 |
| Female | 491 | 44.9 | (38.8, 51.2) | |
| Residence | ||||
| Urban | 399 | 46.0 | (40.1, 51.9) | <0.05 |
| Rural | 615 | 57.5 | (51.1, 63.6) | |
| Region | ||||
| Banjul | 92 | 41.9 | (32.4, 52.1) | <0.005 |
| Kanifing | 90 | 42.5 | (35.8, 49.6) | |
| Brikama | 123 | 54.7 | (44.0, 65.0) | |
| Mansakonko | 148 | 68.1 | (62.2, 73.4) | |
| Kuntaur | 122 | 57.5 | (50.0, 64.7) | |
| Kerewan | 93 | 60.7 | (44.7, 74.6) | |
| Janjanbureh | 182 | 56.1 | (45.3, 66.3) | |
| Basse | 164 | 50.4 | (45.9, 54.8) | |
| Wealth Quintile | ||||
| Lowest | 363 | 58.4 | (49.6, 66.8) | 0.26 |
| Second | 226 | 51.3 | (40.0, 62.6) | |
| Middle | 177 | 52.5 | (37.9, 66.6) | |
| Fourth | 104 | 45.1 | (31.5, 59.5) | |
| Highest | 144 | 39.0 | (29.9, 48.8) | |
| Household sanitation e | ||||
| Inadequate | 640 | 51.9 | (45.2, 58.5) | 0.41 |
| Adequate | 374 | 48.3 | (42.9, 53.7) | |
| Diarrhea in the past 2 weeks f | ||||
| Yes | 249 | 51.7 | (42.6, 60.7) | 0.79 |
| No | 743 | 50.7 | (46.4, 55.0) | |
| Child had cough in past 2 weeks f | ||||
| Yes | 225 | 51.1 | (43.8, 58.3) | 0.91 |
| No | 769 | 50.5 | (44.5, 56.5) | |
| Child had fever in past 2 weeks f | ||||
| Yes | 247 | 57.7 | (50.8, 64.4) | <0.05 |
| No | 746 | 48.5 | (43.2, 53.7) | |
| Malaria infection g | ||||
| Yes | 84 | 52.1 | (43.3,60.9) | 0.731 |
| No | 912 | 50.6 | (45.9, 55.3) | |
| Consumed fortified baby foods h | ||||
| Yes | 44 | 64.9 | (46.8, 79.6) | 0.84 |
| No | 283 | 63.0 | (50.8, 73.7) | |
| Consumed vitamin/mineral supplements h | ||||
| Yes | 39 | 33.1 | (18.0, 52.6) | <0.005 |
| No | 327 | 66.9 | (54.4, 77.4) | |
| Consumed infant formula h | ||||
| Yes | 14 | 31.2 | (13.5, 56.9) | <0.05 |
| No | 312 | 64.7 | (52.6, 75.2) | |
| Wasting | ||||
| Yes (WHZ ≤ −2) | 74 | 51.5 | (35.5, 67.2) | 0.894 |
| No (WHZ > −2) | 933 | 50.3 | (45.7, 55.0) | |
| Stunting | ||||
| Yes (HAZ ≤ −2) | 197 | 65.8 | (50.8, 78.2) | <0.05 |
| No (HAZ > −2) | 809 | 47.1 | (41.8, 52.5) | |
| Underweight | ||||
| Yes (WAZ ≤ −2) | 155 | 63.1 | (50.6, 74.0) | <0.05 |
| No (WAZ > −2) | 855 | 48.6 | (44.0, 53.2) | |
| Microcephaly | ||||
| Yes (HCAZ ≤ −2) | 92 | 65.7 | (53.6, 76.1) | <0.05 |
| No (HCAZ > −2 to ≤ +2) | 918 | 49.3 | (44.5, 54.0) | |
| Iron status i | ||||
| Deficient (serum ferritin < 12 µg/L) | 632 | 65.7 | (59.2, 71.6) | <0.0001 |
| Sufficient (serum ferritin ≥ 12 µg/L) | 375 | 29.4 | (22.7, 37.1) | |
| Vitamin A status i | ||||
| Deficient (RBP < 0.70 μmol/L) | 217 | 60.6 | (51.9, 68.5) | <0.005 |
| Sufficient (RBP ≥ 0.70 μmol/L) | 790 | 48.4 | (43.9, 53.1) | |
| Inflammation j | ||||
| None | 720 | 47.7 | (43.5, 51.9) | <0.05 |
| CRP and/or AGP elevated | 387 | 57.7 | (48.3, 66.7) |
| Characteristic | Category | N | Crude (Bivariate Analysis) | Adjusted (Poisson Regression) a | Population Attributable Fraction b | ||
|---|---|---|---|---|---|---|---|
| Relative Risk | 95% CI | Relative Risk | 95% CI | ||||
| N = 1012 | |||||||
| Iron status | Deficient | 645 | 1.82 | (1.63, 2.03) | 2.11 | (1.79, 2.49) | 39.4% |
| Not deficient | 386 | referent | referent | ||||
| Vitamin A status | Deficient | 220 | 1.51 | (1.18, 1.92) | 1.21 | (1.08, 1.37) | 3.8% |
| Not deficient | 811 | referent | referent | ||||
| Inflammation | Yes | 292 | 1.67 | (1.35, 2.05) | 1.29 | (1.17, 1.44) | 7.6% |
| No | 739 | referent | referent | ||||
| Stunting | Yes | 198 | 1.68 | (1.29, 2.19) | 1.17 | (1.00, 1.26) | 2.4% |
| No | 821 | referent | referent | ||||
| National | Urban | Rural | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | N | % a/ Mean/ Median | 95%CI b | N | % a / Mean/ Median | 95%CI b, IQR | N | % a / Mean/ Median | 95%CI b | p-Value c |
| Non- pregnant women | ||||||||||
| Nutritional status d | ||||||||||
| BMI, mean | 1651 | 23.2 | (22.8, 23.8) | 872 | 23.5 | (23.0, 24.1) | 779 | 22.6 | (21.7, 23.6) | 0.103 |
| Underweight | ||||||||||
| Any underweight, % | 1651 | 15.4 | (12.4, 19.0) | 872 | 14.6 | (10.8, 19.4) | 779 | 17.3 | (13.3, 22.2) | 0.375 |
| Severe underweight, % | 1651 | 1.4 | (0.8, 2.6) | 872 | 1.4 | (0.6, 3.1) | 779 | 1.5 | (0.8, 3.1) | 0.907 |
| Overweight or obesity | ||||||||||
| Overweight and obesity, % | 1651 | 29.7 | (25.7, 34.0) | 872 | 32.6 | (28.0, 37.7) | 779 | 22.8 | (16.0, 31.3) | <0.05 |
| Micronutrient status | ||||||||||
| Hemoglobin concentration | ||||||||||
| Hemoglobin (g/L), mean | 1420 | 118.5 | (116.9, 120.0) | 787 | 119.1 | (117.1, 121.1) | 643 | 116.8 | (114.6, 119.0) | 0.126 |
| Any anemia f, % | 1420 | 50.9 | (45.5, 56.4) | 787 | 49.9 | (42.8, 57.1) | 643 | 53.5 | (47.2, 59.7) | 0.45 |
| Severe anemia f, % | 1420 | 1.3 | (0.7, 2.6) | 787 | 1.0 | (0.3, 3.2) | 643 | 2.0 | (1.0, 4.3) | 0.309 |
| Iron status g, h | ||||||||||
| Ferritin (µg/L), median | 1401 | 18.6 | (17.4, 19.8) | 764 | 21.5 | (19.6, 23.4) | 637 | 13.9 | (11.5, 16.2) | - |
| Iron deficiency, % | 1401 | 41.4 | (37.6, 45.4) | 764 | 37.0 | (32.3, 41.9) | 637 | 52.6 | (45.2, 60.0) | <0.001 |
| Iron deficiency anemia, % | 1392 | 28.1 | (24.5, 32.1) | 756 | 24.5 | (20.4, 29.2) | 636 | 37.3 | (30.7, 44.3) | <0.01 |
| Vitamin A status i | ||||||||||
| RBP (µmol/L), mean | 1391 | 1.36 | (1.31, 1.41) | 764 | 1.42 | (1.35, 1.48) | 637 | 1.22 | (1.14, 1.29) | <0.001 |
| Vitamin A deficiency | 1391 | 1.8 | (1.2, 2.8) | 764 | 0.6 | (0.3, 1.4) | 637 | 4.9 | (2.9, 8.0) | <0.0001 |
| Vitamin A insufficiency | 1391 | 21.6 | (18.2, 25.4) | 764 | 17.6 | (14.0, 21.9) | 637 | 31.7 | (25.5, 38.8) | <0.001 |
| Iodine status | ||||||||||
| Urinary iodine (µg/L), median | 1287 | 156.2 | (149.4, 163.0) | 716 | 163.6 | (154.6, 172.6) | 571 | 126.6 | (114.3, 138.9) | 0.283 |
| Pregnant women | ||||||||||
| Nutritional status | ||||||||||
| Mean MUAC | 120 | 26.6 | (25.8, 27.4) | 50 | 27.6 | (26.1, 29.1) | 70 | 26.0 | (25.2, 26.8) | 0.28 |
| Undernourished, MUAC <23 cm, % | 120 | 7.5 | (4.1, 13.4) | 50 | 6.0 | (2.0, 16.8) | 70 | 8.6 | (4.1, 16.9) | 0.58 |
| Micronutrient status | ||||||||||
| Hemoglobin concentration | ||||||||||
| Hemoglobin (g/L), mean | 132 | 107.3 | (104.4, 110.1) | 62 | 110.0 | (105.4, 114.7) | 70 | 104.8 | (101.6, 107.9) | 0.065 |
| Any anemia j, % | 132 | 56.8 | (47.2, 66.0) | 62 | 50.0 | (35.5, 64.5) | 70 | 62.9 | (50.9, 73.4) | 0.18 |
| Iodine status | ||||||||||
| Urinary iodine (µg/L), median | 118 | 113.5 | (50.1, 205.9) | 54 | 136.5 | (92.6, 236.7) | 64 | 88.8 | (41.3, 162.8) | <0.05 |
| Characteristic | Number of Women | Anemia %a, b | (95% CI)c | Chi-Square p-Value d |
|---|---|---|---|---|
| Age group (in years) | ||||
| 15–19 | 337 | 41.0 | (34.6, 47.7) | 0.06 |
| 20–24 | 263 | 51.5 | (42.9, 60.1) | |
| 25–29 | 231 | 55.3 | (44.4, 65.7) | |
| 30–34 | 198 | 58.3 | (45.6, 70.0) | |
| 35–39 | 188 | 46.8 | (39.6, 54.2) | |
| 40–44 | 116 | 62.4 | (45.5, 76.7) | |
| 45–49 | 87 | 49.1 | (36.6, 61.7) | |
| Residence | ||||
| Urban | 787 | 49.9 | (42.8, 57.1) | 0.45 |
| Rural | 643 | 53.5 | (47.2, 59.7) | |
| Region | ||||
| Banjul | 224 | 32.3 | (24.2, 41.7) | 0.05 |
| Kanifing | 202 | 44.1 | (37.6, 50.7) | |
| Brikama | 185 | 53.6 | (42.1, 64.8) | |
| Mansakonko | 164 | 59.3 | (54.3, 64.1) | |
| Kuntaur | 113 | 67.0 | (60.0, 73.3) | |
| Kerewan | 148 | 37.9 | (25.2, 52.6) | |
| Janjanbureh | 201 | 50.8 | (40.0, 61.5) | |
| Basse | 193 | 57.1 | (47.0, 66.6) | |
| Woman’s Education | ||||
| Never at school | 590 | 58.2 | (53.6, 62.8) | 0.06 |
| Primary school | 220 | 46.1 | (35.1, 57.4) | |
| Lower Secondary | 269 | 47.2 | (36.6, 58.1) | |
| Upper Secondary | 227 | 44.5 | (33.4, 56.2) | |
| Higher | 93 | 48.2 | (36.5, 60.2) | |
| Wealth Quintile | ||||
| Lowest | 350 | 60.1 | (51.5, 68.1) | 0.36 |
| Second | 266 | 52.7 | (43.2, 62.1) | |
| Middle | 249 | 50.3 | (44.2, 56.3) | |
| Fourth | 196 | 46.7 | (28.9, 65.4) | |
| Highest | 369 | 46.5 | (39.6, 53.7) | |
| Household sanitation e | ||||
| Inadequate | 794 | 52.0 | (46.2, 57.8) | 0.51 |
| Adequate | 636 | 49.7 | (42.6, 56.8) | |
| Iron status f | ||||
| Deficient (serum ferritin < 12 µg/L) | 628 | 67.8 | (60.8, 74.1) | <0.0001 |
| Sufficient (serum ferritin ≥ 12 µg/L) | 764 | 37.4 | (30.1, 45.4) | |
| Vitamin A status | ||||
| Insufficient (RBP < 1.05 μmol/L) | 370 | 64.5 | (56.4, 71.9) | <0.01 |
| Sufficient (RBP ≥ 1.05 μmol/L) | 1022 | 46.0 | (39.1, 53.3) | |
| Malaria infection g | ||||
| Yes | 72 | 57.9 | (42.4, 72.0) | 0.328 |
| No | 1184 | 50.5 | (43.9, 57.0) | |
| Inflammation h | ||||
| None | 1143 | 50.1 | (43.4, 56.7) | 0.99 |
| CRP and/or AGP elevated | 249 | 49.9 | (42.0, 57.9) | |
| Nutritional status | ||||
| Underweight (BMI < 18.5) | 224 | 53.1 | (41.3, 64.6) | 0.70 |
| Normal weight (BMI 18.5–24.9) | 781 | 51.5 | (45.5, 57.4) | |
| Overweight/Obesity (BMI > 25) | 391 | 49.2 | (41.3, 57.2) | |
| Minimal dietary diversity | ||||
| Yes (≥ 5 food groups) | 991 | 49.8 | (44.9, 54.8) | 0.53 |
| No (0–4 food groups) | 415 | 52.7 | (42.8, 62.4) |
| Characteristic | Category | N | Crude (Bivariate Analysis) | Adjusted (Poisson Regression) | Population Attributable Fraction a | ||
|---|---|---|---|---|---|---|---|
| Relative Risk | 95% CI | Relative Risk | 95% CI | ||||
| N = 1422 | |||||||
| Iron status | Deficient | 641 | 2.37 | (2.08, 2.71) | 2.08 | (1.85, 2.34) | 33.4% |
| Not deficient | 781 | referent | - | referent | |||
| Vitamin A status | Insufficient | 380 | 1.92 | (1.59, 2.28) | 1.26 | (1.14, 1.39) | 7.3% |
| Not insufficient | 1042 | referent | - | referent | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petry, N.; Jallow, B.; Sawo, Y.; Darboe, M.K.; Barrow, S.; Sarr, A.; Ceesay, P.O.; Fofana, M.N.; Prentice, A.M.; Wegmüller, R.; et al. Micronutrient Deficiencies, Nutritional Status and the Determinants of Anemia in Children 0–59 Months of Age and Non-Pregnant Women of Reproductive Age in The Gambia. Nutrients 2019, 11, 2275. https://doi.org/10.3390/nu11102275
Petry N, Jallow B, Sawo Y, Darboe MK, Barrow S, Sarr A, Ceesay PO, Fofana MN, Prentice AM, Wegmüller R, et al. Micronutrient Deficiencies, Nutritional Status and the Determinants of Anemia in Children 0–59 Months of Age and Non-Pregnant Women of Reproductive Age in The Gambia. Nutrients. 2019; 11(10):2275. https://doi.org/10.3390/nu11102275
Chicago/Turabian StylePetry, Nicolai, Bakary Jallow, Yankuba Sawo, Momodou K. Darboe, Samba Barrow, Aminatta Sarr, Pa Ousman Ceesay, Malang N. Fofana, Andrew M. Prentice, Rita Wegmüller, and et al. 2019. "Micronutrient Deficiencies, Nutritional Status and the Determinants of Anemia in Children 0–59 Months of Age and Non-Pregnant Women of Reproductive Age in The Gambia" Nutrients 11, no. 10: 2275. https://doi.org/10.3390/nu11102275
APA StylePetry, N., Jallow, B., Sawo, Y., Darboe, M. K., Barrow, S., Sarr, A., Ceesay, P. O., Fofana, M. N., Prentice, A. M., Wegmüller, R., Rohner, F., Phall, M. C., & Wirth, J. P. (2019). Micronutrient Deficiencies, Nutritional Status and the Determinants of Anemia in Children 0–59 Months of Age and Non-Pregnant Women of Reproductive Age in The Gambia. Nutrients, 11(10), 2275. https://doi.org/10.3390/nu11102275