Assessment of Dietary Intake and Nutrient Gaps, and Development of Food-Based Recommendations, among Pregnant and Lactating Women in Zinder, Niger: An Optifood Linear Programming Analysis

 ,
,
Abstract
1. Introduction
2. Materials and Methods
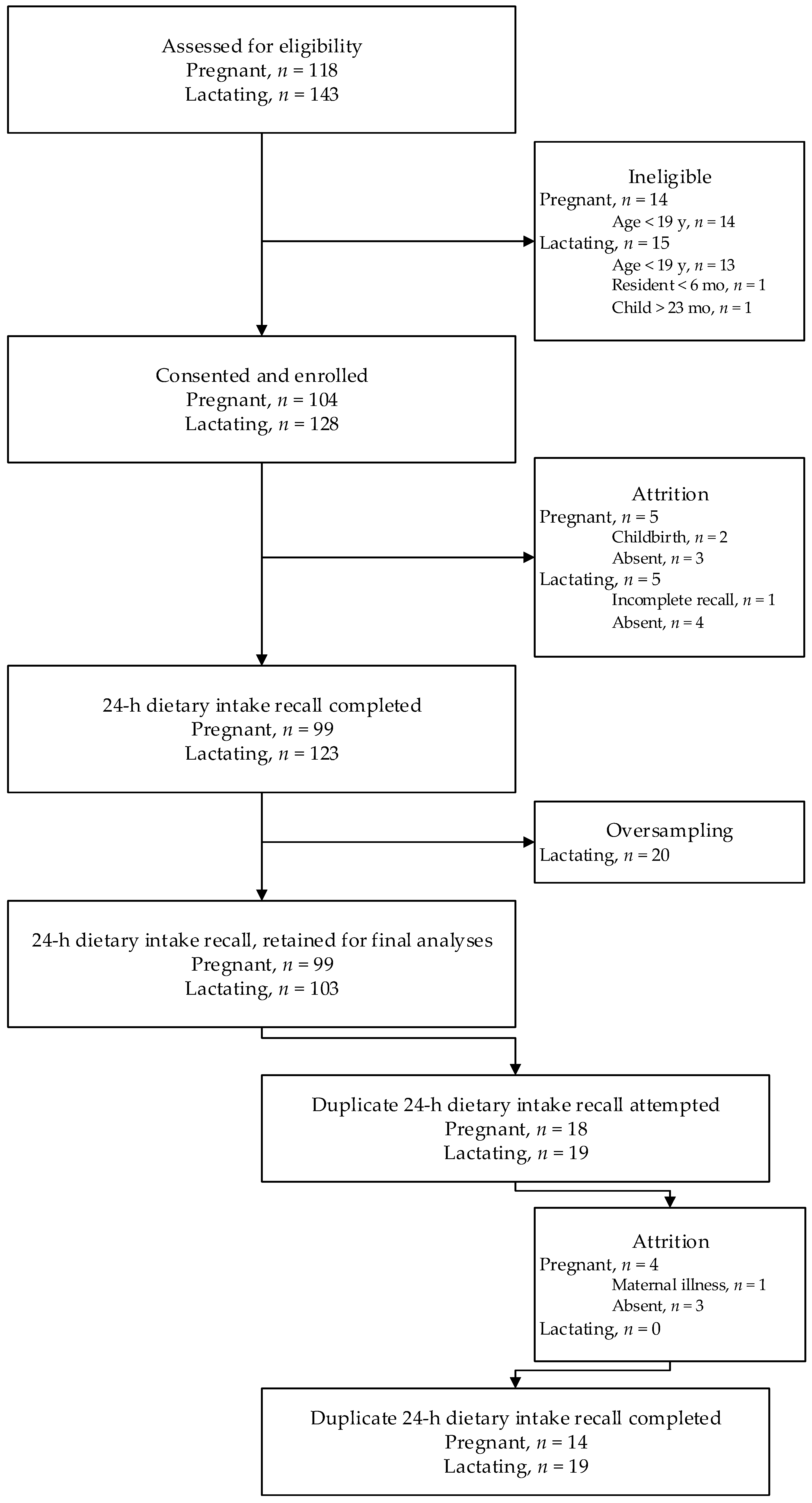
2.1. Study Design and Participants
2.2. Ethical Considerations
2.3. Data Collection
2.3.1. Socio-Demographic Characteristics and Anthropometry
2.3.2. 24 h Recall Data Collection
2.3.3. Market Survey
2.3.4. Food Composition Table
2.3.5. Dietary Reference Intakes
2.4. Data Analyses
2.5. Optifood Analyses
2.5.1. Preparation of Linear Programming Model Parameters
2.5.2. Development of Modelled Diets
2.6. Sample Size
3. Results
3.1. Usual Dietary Intakes
3.2. Optifood
3.2.1. Dietary Patterns and Linear Programming Model Parameters
3.2.2. Linear Programming
Reported Diet and Food-based Recommendations
“Added Meal” and Food-Based Recommendations
Intervention Products and Food-based Recommendations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AMDR | acceptable macronutrient distribution range |
| CSB+ | corn soy blend plus |
| DGLV | dark green leafy vegetables |
| DRI | dietary reference intake |
| EAR | estimated average requirement |
| ECVMA | National Survey on Living Conditions, Household and Agriculture |
| EER | estimated energy requirement |
| FBR | food based recommendation |
| FNB | Food and Nutrition Board |
| HFIAS | household food insecurity access scale |
| IFA | iron and folic acid |
| IOM | Institute of Medicine |
| MDD-W | minimum dietary diversity for women |
| MN | micronutrients |
| MUAC | mid-upper arm circumference |
| NCI | National Cancer Institute |
| NiMaNu | Niger Maternal Nutrition Project |
| PAL | physical activity level |
| RDA | recommended dietary allowance |
| SQ-LNS P&L | small quantity lipid-based nutrient supplement for pregnant and lactating women |
| UEMOA | West African Economic and Monetary Union |
| UNIMMAP | UNICEF/WHO/UNU international multiple micronutrient preparation |
| USDA | United States Department of Agriculture |
| USDA SR28 | USDA Nutrient Database for Standard Reference, Release 28 |
| WHO | World Health Organization |
References
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; De Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Dror, D.K.; Allen, L.H. Overview of nutrients in human milk. Adv. Nutr. 2018, 9, 278S–294S. [Google Scholar] [CrossRef] [PubMed]
- Torheim, L.E.; Ferguson, E.L.; Penrose, K.; Arimond, M. Women in resource-poor settings are at risk of inadequate intakes of multiple micronutrients. J. Nutr. 2010, 140, 2051S–2058S. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. At a Glance: Niger. 2014. Available online: http://unicef.org/infobycountry/niger_statistics.html (accessed on 14 October 2014).
- Ouedraogo, C.; Young, R.; Wessells, K.; Hess, S. Prevalence and determinants of inadequate gestational weight gain among pregnant women in Zinder, Niger. Curr. Dev. Nutr. 2018, in press. [Google Scholar]
- Wessells, K.R.; Ouedraogo, C.T.; Young, R.R.; Faye, M.T.; Brito, A.; Hess, S.Y. Micronutrient status among pregnant women in Zinder, Niger and risk factors associated with deficiency. Nutrients 2017, 9. [Google Scholar] [CrossRef]
- Institut National de la Statistique du Niger et Banque Mondiale. Profil et Determinants de la Pauvrete au Niger en 2011. Premiers Resultats de l’enquete Nationale sur les Conditions de vie: Des Menages et l’agriculture au Niger (ECVMA). 2013. Available online: http://www.stat-niger.org/statistique/file/Annuaires_Statistiques/Profil_Pauvrete_2011_ECVMA.pdf (accessed on 6 March 2015).
- Imdad, A.; Bhutta, Z.A. Effect of balanced protein energy supplementation during pregnancy on birth outcomes. BMC Public Health 2011, 11, S17. [Google Scholar] [CrossRef]
- Ramakrishnan, U.; Grant, F.K.; Imdad, A.; Bhutta, Z.A.; Martorell, R. Effect of multiple micronutrient versus iron-folate supplementation during pregnancy on intrauterine growth. Nestle Nutr. Inst. Workshop Ser. 2013, 74, 53–62. [Google Scholar] [CrossRef]
- Ota, E.; Hori, H.; Mori, R.; Tobe-Gai, R.; Farrar, D. Antenatal dietary education and supplementation to increase energy and protein intake. Cochrane Database Syst. Rev. 2015, 6. [Google Scholar] [CrossRef]
- Kaestel, P.; Michaelsen, K.F.; Aaby, P.; Friis, H. Effects of prenatal multimicronutrient supplements on birth weight and perinatal mortality: A randomised, controlled trial in Guinea-Bissau. Eur. J. Clin. Nutr. 2005, 59, 1081–1089. [Google Scholar] [CrossRef]
- Adu-Afarwuah, S.; Lartey, A.; Dewey, K.G. Meeting nutritional needs in the first 1000 days: A place for small-quantity lipid-based nutrient supplements. Ann. N. Y. Acad. Sci. 2017, 1392, 18–29. [Google Scholar] [CrossRef]
- The Sackler Institute for Nutrition Science. Nutrition Modeling Tools for Advocacy, Decision-Making and Costing: A Workshop to Support Adoption and Utilization. April 27–28, 2017. Available online: https://www.nyas.org/programs/the-sackler-institute-for-nutrition-science/evidence-based-tools-for-decision-making-in-nutrition-programs/ (accessed on 4 December 2018).
- Ferguson, E.L.; Darmon, N.; Fahmida, U.; Fitriyanti, S.; Harper, T.B.; Premachandra, I.M. Design of optimal food-based complementary feeding recommendations and identification of key “problem nutrients” using goal programming. J. Nutr. 2006, 136, 2399–2404. [Google Scholar] [CrossRef] [PubMed]
- Skau, J.K.; Bunthang, T.; Chamnan, C.; Wieringa, F.T.; Dijkhuizen, M.A.; Roos, N.; Ferguson, E.L. The use of linear programming to determine whether a formulated complementary food product can ensure adequate nutrients for 6- to 11-month-old Cambodian infants. Am. J. Clin. Nutr. 2014, 99, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Hlaing, L.M.; Fahmida, U.; Htet, M.K.; Utomo, B.; Firmansyah, A.; Ferguson, E.L. Local food-based complementary feeding recommendations developed by the linear programming approach to improve the intake of problem nutrients among 12-23-month-old Myanmar children. Br. J. Nutr. 2016, 116, S16–S26. [Google Scholar] [CrossRef] [PubMed]
- Fahmida, U.; Santika, O.; Kolopaking, R.; Ferguson, E. Complementary feeding recommendations based on locally available foods in Indonesia. Food Nutr. Bull. 2014, 35, 1741S–1779S. [Google Scholar] [CrossRef] [PubMed]
- Vossenaar, M.; Knight, F.A.; Tumilowicz, A.; Hotz, C.; Chege, P.; Ferguson, E.L. Context-specific complementary feeding recommendations developed using Optifood could improve the diets of breast-fed infants and young children from diverse livelihood groups in northern Kenya. Public Health Nutr. 2017, 20, 971–983. [Google Scholar] [CrossRef]
- Tharrey, M.; Olaya, G.A.; Fewtrell, M.; Ferguson, E. Adaptation of new Colombian food-based complementary feeding recommendations using linear programming. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 667–672. [Google Scholar] [CrossRef]
- Hess, S.Y.; Ouedraogo, C.T. NiMaNu Project. Open Science Framework. 2016. Available online: Osf.io/4cenf (accessed on 30 June 2018).
- Begum, K.; Ouedraogo, C.T.; Wessells, K.R.; Young, R.R.; Faye, M.T.; Wuehler, S.E.; Hess, S.Y. Prevalence of and factors associated with antenatal care seeking and adherence to recommended iron-folic acid supplementation among pregnant women in Zinder, Niger. Mater. Child. Nutr. 2018, 14. [Google Scholar] [CrossRef]
- United Nations. Designing Household Survey Samples: Practical Guidelines. Available online: https://unstats.un.org/unsd/demographic/sources/surveys/Handbook23June05.pdf (accessed on 4 February 2014).
- Coates, J.; Swindale, A.; Bilinksky, P. Household Food Insecurity Access Scale (HFIAS) for Measurement of Household Food Access: Indicator Guide (v. 3). Washington, D.C.: FHI 360/FANTA. Available online: https://www.fantaproject.org/monitoring-and-evaluation/household-food-insecurity-access-scale-hfias (accessed on 7 November 2013).
- Ververs, M.T.; Antierens, A.; Sackl, A.; Staderini, N.; Captier, V. Which anthropometric indicators identify a pregnant woman as acutely malnourished and predict adverse birth outcomes in the humanitarian context? PLoS Curr. 2013, 5. [Google Scholar] [CrossRef]
- Papageorghiou, A.T.; Ohuma, E.O.; Gravett, M.G.; Hirst, J.; Da Silveira, M.F.; Lambert, A.; Jaffer, Y.A.; Bertino, E.; Gravett, M.G.; Purwar, M.; et al. International standards for symphysis-fundal height based on serial measurements from the Fetal Growth Longitudinal Study of the INTERGROWTH-21st Project: Prospective cohort study in eight countries. BMJ 2016, 355, i5662. [Google Scholar] [CrossRef]
- Gibson, R.; Ferguson, E. An Interactive 24-H Recall for Assessing the Adequacy of Iron and Zinc Intakes in Developing Countries. Harvest Plus Technical Monograph 8, 2002. Available online: http://www.harvestplus.org/node/544 (accessed on 17 October 2012).
- FAO and FHI 360. Minimum Dietary Diversity for Women: A Guide for Measurement; FAO: Rome, Italy, 2016; Available online: http://www.fao.org/nutrition/assessment/tools/minimum-dietary-diversity-women/en/ (accessed on 25 May 2016).
- Ministere de l’economie et des finances. Institut National de la Statistique. Troisieme Enquete Nationale sur le Budget et la Consommation des Menages au Niger. Manuel de l’enqueteur. 2007. Available online: http://catalog.ihsn.org/index.php/catalog/2300/download/36678 (accessed on 3 October 2013).
- US Department of Agriculture, Agricultural Research Service, Nutrient Data Laboratory. USDA National Nutrient Database for Standard Reference, Release 28 (Slightly revised). Version Current: May 2016. Available online: http://www.ars.usda.gov/ba/bhnrc/ndl (accessed on 25 January 2017).
- Wessells, K.R.; Singh, G.M.; Brown, K.H. Estimating the global prevalence of inadequate zinc intake from national food balance sheets: Effects of methodological assumptions. PLoS ONE 2012, 7, e50565. [Google Scholar] [CrossRef]
- US Department of Agriculture. USDA table of nutrient retention factors, release 6. Available online: https://www.ars.usda.gov/ARSUserFiles/80400525/Data/retn/retn06.pdf (accessed on 1 May 2016).
- Portant application obligatoire des normes nigériennes relatives aux huiles comestibles raffinées de palme, palmiste et d’arachide enrichies en vitamine A; Arrête conjoint N 65 MM/DI/MSP/MF du 25 Avril 2012; Ministère des Mines et du Développement Industriel, Ministère de la Santé Publique, Ministère des Finances: Niamey, République du Niger, 2012.
- Portant application obligatoire de la norme nigérienne relative à la farine de blé tendre enrichie en fer et acide folique; Arrête conjoint N 89 MM/DI//MSP/MF du 31 Mai 2012; Ministère des Mines et du Développement Industriel, Ministère de la Santé Publique, Ministère des Finances: Niamey, République du Niger, 2012.
- Food Fortification Initiative. Country Profile - Niger. Available online: http://ffinetwork.org/country_profiles/country.php?record=158 (accessed on 4 September 2018).
- Luo, H.; Stewart, C.; Vosti, S.; Brown, K.; Engle-Stone, R. Predicted effects of current and potential micronutrient intervention programs on adequacy of iron intake in a national sample of women and young children in Cameroon. In Proceedings of the Micronutrient Forum, Cancun, Mexico, October 2016. [Google Scholar]
- Institute of Medicine. Food and Nutrition Board. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium and Carotenoids; National Academy Press: Washington, DC, USA, 2000. [Google Scholar]
- Institute of Medicine. Food and Nutrition Board. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academy Press: Washington, DC, USA, 2001. [Google Scholar]
- Institute of Medicine. Food and Nutrition Board. Dietary Reference Intakes for Calcium and Vitamin D. Available online: https://ods.od.nih.gov/Health_Information/Dietary_Reference_Intakes.aspx (accessed on 4 July 2018).
- Institute of Medicine. Food and Nutrition Board. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids. Available online: https://ods.od.nih.gov/Health_Information/Dietary_Reference_Intakes.aspx (accessed on 3 February 2010).
- Institute of Medicine. Food and Nutrition Board. Dietary Reference Intakes: Thiamin, Riboflavin, Niacin, Vitamin B6, Vitamin B12, Pantothenic Acid, Biotin, and Choline; National Academy Press: Washington, DC, USA, 1998. [Google Scholar]
- World Health Organization, Food and Agriculture Organization. Vitamin and Mineral Requirements in Human Nutrition. Report of a Joint FAO/WHO Expert Consultation; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Arimond, M.; Vitta, B.S.; Martin-Prevel, Y.; Moursi, M.; Dewey, K.G. Local foods can meet micronutrient needs for women in urban Burkina Faso, but only if rarely consumed micronutrient-dense foods are included in daily diets: A linear programming exercise. Mater. Child. Nutr. 2018, 14. [Google Scholar] [CrossRef]
- Tooze, J.A.; Kipnis, V.; Buckman, D.W.; Carroll, R.J.; Freedman, L.S.; Guenther, P.M.; Krebs-Smith, S.M.; Subar, A.F.; Dodd, K.W. A mixed-effects model approach for estimating the distribution of usual intake of nutrients: The NCI method. Stat. Med. 2010, 29, 2857–2868. [Google Scholar] [CrossRef] [PubMed]
- Tooze, J.A.; Midthune, D.; Dodd, K.W.; Freedman, L.S.; Krebs-Smith, S.M.; Subar, A.F.; Guenther, P.M.; Carroll, R.J.; Kipnis, V. A new statistical method for estimating the usual intake of episodically consumed foods with application to their distribution. J. Am. Diet. Assoc. 2006, 106, 1575–1587. [Google Scholar] [CrossRef] [PubMed]
- Daelmans, B.; Ferguson, E.; Lutter, C.K.; Singh, N.; Pachon, H.; Creed-Kanashiro, H.; Woldt, M.; Mangasaryan, N.; Cheung, E.; Mir, R.; et al. Designing appropriate complementary feeding recommendations: Tools for programmatic action. Mater. Child. Nutr. 2013, 9, 116–130. [Google Scholar] [CrossRef] [PubMed]
- Guyon, A.B.; Quinn, V.J. Booklet on Key Essential Nutrition Actions Messages. Available online: http://www.thp.org/files/Booklet_of_Key_ENA_Messages_complete_for_web.pdf (accessed on 14 January 2015).
- FANTA. Development of Evidence-Based Dietary Recommendations for Children, Pregnant Women, and Lactating Women Living in the Western Highlands in Guatemala. 2014. Available online: https://www.fantaproject.org/countries/guatemala/optifood-report-2014 (accessed on 24 February 2015).
- Santika, O.; Fahmida, U.; Ferguson, E.L. Development of food-based complementary feeding recommendations for 9- to 11-month-old peri-urban Indonesian infants using linear programming. J. Nutr. 2009, 139, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Levesque, S.; Delisle, H.; Agueh, V. Contribution to the development of a food guide in Benin: Linear programming for the optimization of local diets. Public Health Nutr. 2015, 18, 622–631. [Google Scholar] [CrossRef] [PubMed]
- Termote, C.; Raneri, J.; Deptford, A.; Cogill, B. Assessing the potential of wild foods to reduce the cost of a nutritionally adequate diet: An example from eastern Baringo District, Kenya. Food Nutr. Bull. 2014, 35, 458–479. [Google Scholar] [CrossRef]
- Biehl, E.; Klemm, R.D.; Manohar, S.; Webb, P.; Gauchan, D.; West, K.P., Jr. What does it cost to improve household diets in Nepal? Using the cost of the diet method to model lowest cost dietary changes. Food Nutr. Bull. 2016, 37, 247–260. [Google Scholar] [CrossRef]
- World Bank. Republic of Niger: Measuring Poverty Trends. Available online: https://openknowledge.worldbank.org/handle/10986/22808 (accessed on 3 March 2018).
- Miller, V.; Yusuf, S.; Chow, C.K.; Dehghan, M.; Corsi, D.J.; Lock, K.; Popkin, B.; Rangarajan, S.; Khatib, R.; Lear, S.A.; et al. Availability, affordability, and consumption of fruits and vegetables in 18 countries across income levels: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet Glob. Health. 2016, 4, e695–e703. [Google Scholar] [CrossRef]
- Rosen, J.G.; Clermont, A.; Kodish, S.R.; Matar Seck, A.; Salifou, A.; Grais, R.F.; Isanaka, S. Determinants of dietary practices during pregnancy: A longitudinal qualitative study in Niger. Mater. Child. Nutr. 2018, 14, e12629. [Google Scholar] [CrossRef]


{kind=link}
| Pregnant Women | Lactating Women | |||
|---|---|---|---|---|
| Model Energy Constraint 2 (kcal/day) | Modeled Intervention Product (per day) | Model Energy Constraint 2 (kcal/day) | Modeled Intervention Product (per day) | |
| Reported diet | 1811.9 | --- | 2279.5 | --- |
| Reported diet + IFA (standard of care) | 1811.9 | 1 IFA | --- | --- |
| Added meal diet | 2414.8 | --- | 2622.0 | --- |
| Added meal diet + IFA | 2414.8 | 1 IFA | --- | --- |
| Added meal diet + UNIMMAP 3 | 2418.8 | 1 UNIMMAP | 2622.0 | 1 UNIMMAP |
| Added meal diet + Supercereal (CSB+) 3,4 | 2418.8 | 1 serving of CSB+ (500 kcal) | 2622.0 | 1 serving of CSB+ (500 kcal) |
| Added meal diet + SQ-LNS (P&L) 3 | 2418.8 | 1 serving of SQ-LNS (118 kcal) | 2622.0 | 1 serving of SQ-LNS (118 kcal) |
| Added meal diet + Plumpy’Mum 3 | 2418.8 | 1 serving of Plumpy’Mum (515 kcal/day) | 2622.0 | 1 serving of Plumpy’Mum (515 kcal/day) |
| Variable | Pregnant | Lactating |
|---|---|---|
| Participants (n) | 99 | 103 |
| Age (years) 2 | 27.8 ± 6.2 | 26.5 ± 6.4 |
| Gravidity (n) | 7.2 ± 3.3 | --- |
| Current pregnancy trimester | ||
| Second, n (%) | 59 (59.6) | --- |
| Third, n (%) | 40 (40.4) | --- |
| Attended ANC in current pregnancy, n (%) | 65 (65.7) | --- |
| Age of breastfed child (months) | --- | 8.3 ± 5.6 |
| Menses resumed, n (%) | --- | 26 (25.5) |
| Household food insecurity access scale (HFIAS), n (%) | ||
| Food secure or mildly food insecure | 48 (48.5) | 43 (42.2) |
| Moderately food insecure | 26 (26.3) | 32 (31.3) |
| Severely food insecure | 25 (25.3) | 27 (26.5) |
| Daily per capita reported cost of foods consumed, € 3 | 0.35 (0.28, 0.45) | 0.39 (0.30, 0.49) |
| Daily per capita reported cost of foods below the national poverty line, % 4 | 72.3 | 63.0 |
| Received food rations in prior month, n (%) | 6 (10.9) 5 | 3 (2.9) |
| Adequate minimum dietary diversity – women (MDD-W), n (%) | 16 (16.3) | 15 (14.6) |
| Nutritional and health status | ||
| Weight (kg) | 56.4 ± 8.4 | 52.4 ± 9.0 |
| BMI (kg/m2) | --- | 20.9 ± 3.2 |
| Underweight (BMI < 18.5 kg/m2) | --- | 22 (21.4) |
| Overweight (BMI > 25 kg/m2) | --- | 9 (8.7) |
| Mid-upper arm circumference (cm) | 25.1 ± 2.7 | 26.0 ± 2.9 |
| MUAC < 23 cm | 20 (20.3) | 3 (2.9) |
| Pregnant Women (n = 99) | Lactating Women (n = 103) | |||||
|---|---|---|---|---|---|---|
| EAR 2 | Intake | Prevalence of Inadequacy (%) | EAR | Intake | Prevalence of Inadequacy (%) | |
| Energy, kcal | 2674.5 | 1759.7 (1475.5, 2101.3) | 2622.2 | 2209.7 (1841.3, 2640.0) | ||
| Vitamin A, µg RAE | 550 | 536.1 3 (378.4, 741.1) | 52.1 | 900 | 504.9 (349.8, 701.6) 3 | 88.8 |
| Vitamin C, mg | 70 | 25.9 (16.2, 39.7) | 95.2 | 100 | 30.8 (19.3, 46.7) | 97.9 |
| Thiamin, mg | 1.2 | 0.8 (0.7, 1.0) | 89.3 | 1.2 | 1.0 (0.8, 1.2) | 71.8 |
| Riboflavin, mg | 1.2 | 0.8 (0.6, 1.0) | 91.8 | 1.3 | 0.9 (0.7, 1.2) | 85.7 |
| Niacin, mg | 14 | 7.5 (6.4, 8.9) | 98.4 | 13 | 9.1 (7.7, 10.8) | 95.3 |
| Vitamin B6, mg | 1.6 | 1.6 (1.3, 1.9) | 52.1 | 1.7 | 2.0 (1.7, 2.5) | 26.9 |
| Folate, µg DFE | 520 | 307.3 3(221.4, 414.7) | 88.8 | 450 | 294.1 3 (208.4, 398.8) | 83.0 |
| Vitamin B12, µg | 2.2 | 0.2 (0.1, 0.4) | 100.0 | 2.4 | 0.3 (0.2, 0.5) | 100.0 |
| Iron, mg | 22 | 22.6 3 (17.5, 28.9) | 46.7 | 11.7 | 30.1 3 (23.6, 37.4) | 1.0 |
| Zinc, mg | 9.5 | 11.0 (8.8, 13.7) | 32.6 | 10.4 | 14.8 (11.9, 18.3) | 14.3 |
| Calcium, mg | 800 | 330.3 (301.5, 361.5) | 100.0 | 800 | 384.8 (351.0, 420.2) | 100.0 |
| % of RDA | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Analysis 3 | Vitamin A | Vitamin C | Thiamin | Riboflavin | Niacin | Vitamin B6 | Folate | Vitamin B12 | Iron | Zinc | Calcium 4 | No. MN Adequate | Cost of Diet (€/day) |
| Reported energy intake | |||||||||||||
| Best-case scenario | 79.2 | 39.6 | 82.7 | 78.9 | 57.6 | 113.0 | 70.6 | 24.7 | 133.4 | 177.2 | 53.5 | 3 | |
| Worst-case scenario | 0 | 0.1 | 38.6 | 23.3 | 27.9 | 50.2 | 7.1 | 1.8 | 32.9 | 78.8 | 2.4 | 1 | |
| Reported energy intake + IFA | |||||||||||||
| Best-case scenario | 79.2 | 39.6 | 83.4 | 79.6 | 57.6 | 113.5 | 184.1 | 25.0 | 355.9 | 177.3 | 53.5 | 4 | |
| Worst-case scenario | 0 | 0.1 | 39.3 | 24.0 | 27.9 | 50.7 | 120.3 | 2.1 | 254.8 | 78.9 | 2.4 | 3 | |
| Added meal | |||||||||||||
| Best-case scenario | 111.8 | 65.6 | 122.6 | 121.9 | 87.0 | 154.9 | 116.6 | 47.1 | 188.2 | 267.7 | 87.4 | 7 | |
| Worst-case scenario | 0 | 0.1 | 50.5 | 25.7 | 38.1 | 62.8 | 9.9 | 2.4 | 32.8 | 100.1 | 1.4 | 1 | |
| Best modeled FBR (worst-case scenario) | 74.5 | 26.3 | 77.5 | 80.9 | 52.5 | 107.4 | 73.9 | 39.8 | 106.7 | 209.9 | 66.4 | 8 | 0.43 |
| Added meal + IFA | |||||||||||||
| Best-case scenario | 111.8 | 65.6 | 123.3 | 122.7 | 87.1 | 155.4 | 230.1 | 47.4 | 410.8 | 267.8 | 87.4 | 7 | |
| Worst-case scenario | 0 | 0.1 | 51.2 | 26.4 | 38.1 | 63.4 | 123.1 | 2.7 | 254.7 | 100.2 | 1.4 | 3 | |
| Best modeled FBR (worst-case scenario) | 74.4 | 26.1 | 70.6 | 79.9 | 52.2 | 106.3 | 167.3 | 40.0 | 323.7 | 205.2 | 65.1 | 8 | 0.42 |
| Added meal + UNIMMAP | |||||||||||||
| Best-case scenario | 215.8 | 148.0 | 222.7 | 222.1 | 187.2 | 255.1 | 230.1 | 147.2 | 299.5 | 404.2 | 87.4 | 10 | |
| Worst-case scenario | 103.8 | 82.3 | 150.3 | 125.6 | 137.9 | 162.7 | 123.1 | 102.2 | 143.8 | 236.3 | 1.4 | 10 | |
| Best modeled FBR (worst-case scenario) | 134.1 | 108.3 | 169.8 | 179.0 | 152.0 | 205.6 | 167.3 | 139.5 | 212.7 | 341.3 | 65.1 | 11 | 0.40 |
| Added meal + Supercereal (CSB+) | |||||||||||||
| Best-case scenario | 239.1 | 151.4 | 146.3 | 221.0 | 132.8 | 204.6 | 135.9 | 123.5 | 208.3 | 300.7 | 136.8 | 11 | |
| Worst-case scenario | 142.4 | 85.9 | 73.6 | 131.1 | 86.0 | 117.3 | 30.1 | 78.9 | 66.6 | 139.9 | 51.7 | 9 | |
| Best modeled FBR (worst-case scenario) | 152.6 | 100.5 | 86.7 | 140.5 | 89.9 | 128.3 | 71.1 | 79.2 | 78.7 | 145.9 | 68.9 | 11 | 0.19 |
| Added meal + SQ-LNS P & L | |||||||||||||
| Best-case scenario | 215.8 | 183.4 | 319.4 | 319.5 | 284.9 | 349.5 | 229.1 | 247.2 | 259.5 | 532.0 | 115.0 | 11 | |
| Worst-case scenario | 103.8 | 117.5 | 245.5 | 223.7 | 235.5 | 256.8 | 122.1 | 201.9 | 103.9 | 362.6 | 29.1 | 10 | |
| Best modeled FBR (worst-case scenario) | 128.0 | 141.8 | 248.0 | 248.5 | 244.7 | 278.6 | 126.9 | 220.5 | 112.5 | 396.6 | 71.1 | 11 | 0.28 |
| Added meal + Plumpy’Mum | |||||||||||||
| Best-case scenario | 226.3 | 149.2 | 218.4 | 221.0 | 193.1 | 236.4 | 243.1 | 145.7 | 293.2 | 384.2 | 96.7 | 10 | |
| Worst-case scenario | 114.3 | 83.5 | 142.3 | 129.7 | 144.3 | 144.5 | 136.4 | 100.7 | 149.5 | 217.3 | 11.3 | 10 | |
| Best modeled FBR (worst-case scenario) | 144.5 | 109.0 | 146.9 | 164.3 | 157.8 | 166.5 | 142.2 | 137.7 | 158.2 | 287.3 | 68.6 | 11 | 0.30 |
| % of RDA | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Analysis 3 | Vitamin A | Vitamin C | Thiamin | Riboflavin | Niacin | Vitamin B6 | Folate | Vitamin B12 | Iron | Zinc | Calcium 4 | No. MN Adequate | Cost of Diet (€/day) |
| Current energy intake | |||||||||||||
| Best-case scenario | 52.3 | 40.9 | 95.4 | 83.3 | 72.3 | 128.0 | 81.7 | 21.9 | 245.1 | 199.8 | 54.8 | 3 | |
| Worst-case scenario | 0.0 | 0.0 | 51.9 | 29.8 | 38.0 | 64.2 | 11.0 | 2.1 | 82.0 | 96.5 | 4.0 | 2 | |
| Additional meal | |||||||||||||
| Best-case scenario | 80.9 | 67.4 | 128.0 | 118.5 | 97.8 | 155.3 | 135.3 | 40.7 | 306.4 | 270.7 | 89.0 | 6 | |
| Worst-case scenario | 0.0 | 0.1 | 53.2 | 25.4 | 42.1 | 61.5 | 11.7 | 2.4 | 59.9 | 98.1 | 1.9 | 1 | |
| Best modeled FBR (worst-case scenario) | 13.7 | 15.1 | 78.4 | 69.3 | 56.7 | 111.6 | 69.9 | 37.0 | 181.9 | 207.2 | 65.4 | 7 | 0.43 |
| Additional meal + UNIMMAP | |||||||||||||
| Best-case scenario | 142.6 | 125.8 | 228.1 | 206.1 | 203.9 | 250.5 | 271.4 | 133.7 | 473.3 | 395.9 | 89.0 | 10 | |
| Worst-case scenario | 61.5 | 58.3 | 153.0 | 112.8 | 147.8 | 156.3 | 147.5 | 95.1 | 226.3 | 222.9 | 1.9 | 8 | |
| Best modeled FBR (worst-case scenario) | 75.2 | 73.3 | 178.2 | 156.7 | 162.4 | 206.5 | 205.7 | 129.7 | 348.3 | 332.0 | 65.4 | 11 | 0.43 |
| Additional meal + Supercereal (CSB+) | |||||||||||||
| Best-case scenario | 156.4 | 128.2 | 151.9 | 204.7 | 146.1 | 201.8 | 158.3 | 111.7 | 325.7 | 300.3 | 138.4 | 11 | |
| Worst-case scenario | 84.5 | 60.8 | 80.9 | 117.5 | 93.8 | 116.5 | 37.5 | 73.4 | 111.2 | 139.1 | 51.9 | 8 | |
| Best modeled FBR (worst-case scenario) | 88.9 | 69.7 | 91.3 | 123.6 | 97.1 | 129.1 | 74.6 | 73.6 | 125.2 | 143.3 | 69.7 | 11 | 0.21 |
| Additional meal + SQ-LNS P & L | |||||||||||||
| Best-case scenario | 142.6 | 150.9 | 324.8 | 291.1 | 307.4 | 340.1 | 270.3 | 226.6 | 406.9 | 513.0 | 116.6 | 11 | |
| Worst-case scenario | 61.5 | 83.3 | 249.5 | 198.4 | 251.2 | 246.3 | 146.8 | 187.7 | 166.5 | 340.6 | 29.4 | 9 | |
| Best modeled FBR (worst-case scenario) | 71.5 | 96.9 | 251.7 | 213.3 | 259.9 | 265.1 | 150.4 | 204.8 | 174.9 | 372.5 | 69.9 | 11 | 0.30 |
| Additional meal + Plumpy’Mum | |||||||||||||
| Best-case scenario | 148.8 | 126.7 | 224.5 | 204.9 | 210.3 | 232.5 | 287.0 | 132.3 | 454.0 | 377.5 | 98.2 | 10 | |
| Worst-case scenario | 67.7 | 59.1 | 149.8 | 116.2 | 155.3 | 143.2 | 165.1 | 93.7 | 235.0 | 209.3 | 11.5 | 9 | |
| Best modeled FBR (worst-case scenario) | 81.3 | 73.7 | 153.0 | 139.6 | 168.6 | 162.4 | 169.5 | 128.0 | 243.4 | 274.0 | 67.3 | 11 | 0.32 |
| Pregnant Women | No. MN Adequate 2 | Lactating Women | No. MN Adequate | |
|---|---|---|---|---|
| Reported diet 3 | --- | --- | ||
| Reported diet + IFA (standard of care) | --- | --- | ||
| Added meal diet |
| 8 |
| 7 |
| Added meal diet + IFA |
| 8 | --- | |
| Added meal diet + UNIMMAP |
| 11 |
| 11 |
| Added meal diet + Supercereal (CSB+) |
| 11 |
| 11 |
| Added meal + SQ-LNS (P&L) |
| 11 |
| 11 |
| Added meal diet + Plumpy’Mum |
| 11 |
| 11 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wessells, K.R.; Young, R.R.; Ferguson, E.L.; Ouédraogo, C.T.; Faye, M.T.; Hess, S.Y. Assessment of Dietary Intake and Nutrient Gaps, and Development of Food-Based Recommendations, among Pregnant and Lactating Women in Zinder, Niger: An Optifood Linear Programming Analysis. Nutrients 2019, 11, 72. https://doi.org/10.3390/nu11010072
Wessells KR, Young RR, Ferguson EL, Ouédraogo CT, Faye MT, Hess SY. Assessment of Dietary Intake and Nutrient Gaps, and Development of Food-Based Recommendations, among Pregnant and Lactating Women in Zinder, Niger: An Optifood Linear Programming Analysis. Nutrients. 2019; 11(1):72. https://doi.org/10.3390/nu11010072
Chicago/Turabian StyleWessells, K. Ryan, Rebecca R. Young, Elaine L. Ferguson, Césaire T. Ouédraogo, M. Thierno Faye, and Sonja Y. Hess. 2019. "Assessment of Dietary Intake and Nutrient Gaps, and Development of Food-Based Recommendations, among Pregnant and Lactating Women in Zinder, Niger: An Optifood Linear Programming Analysis" Nutrients 11, no. 1: 72. https://doi.org/10.3390/nu11010072
APA StyleWessells, K. R., Young, R. R., Ferguson, E. L., Ouédraogo, C. T., Faye, M. T., & Hess, S. Y. (2019). Assessment of Dietary Intake and Nutrient Gaps, and Development of Food-Based Recommendations, among Pregnant and Lactating Women in Zinder, Niger: An Optifood Linear Programming Analysis. Nutrients, 11(1), 72. https://doi.org/10.3390/nu11010072