Serum Trace Elements and Their Associations with Breast Cancer Subgroups in Korean Breast Cancer Patients

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ethical Approval and Informed Consent
2.3. Analytical Procedures
2.4. Statistical Analysis
3. Results
3.1. General Characteristics of the Study Population
3.2. Serum Trace Element Concentrations in Korean Breast Cancer Patients and Controls without Breast Cancer
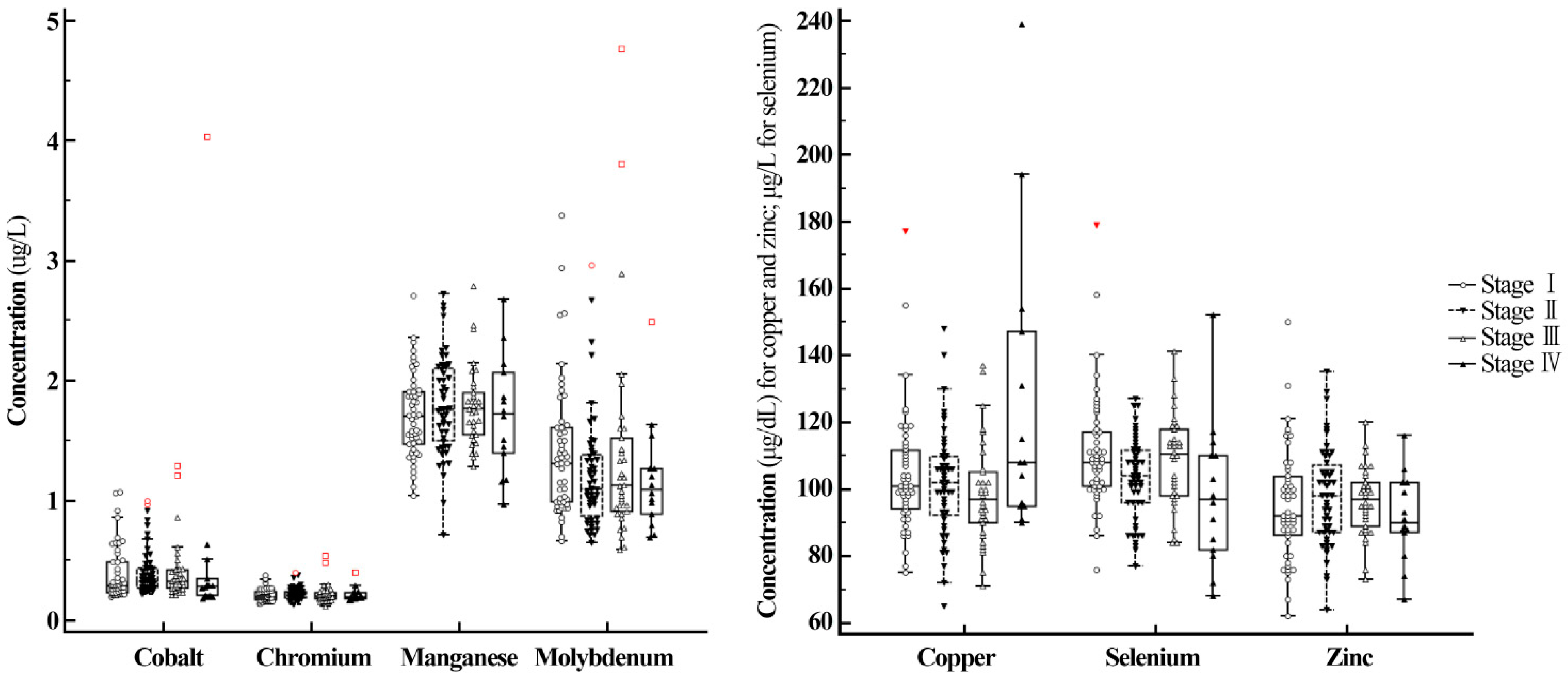
3.3. Subgroup Analysis—Serum Trace Element Concentrations in Breast Cancer Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ginsburg, O.; Bray, F.; Coleman, M.P.; Vanderpuye, V.; Eniu, A.; Kotha, S.R.; Sarker, M.; Huong, T.T.; Allemani, C.; Dvaladze, A.; et al. The global burden of women’s cancers: A grand challenge in global health. Lancet 2017, 389, 847–860. [Google Scholar] [CrossRef]
- Bhoo-Pathy, N.; Yip, C.H.; Hartman, M.; Uiterwaal, C.S.; Devi, B.C.; Peeters, P.H.; Taib, N.A.; van Gils, C.H.; Verkooijen, H.M. Breast cancer research in Asia: Adopt or adapt western knowledge? Eur. J. Cancer 2013, 49, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Leong, S.P.; Shen, Z.Z.; Liu, T.J.; Agarwal, G.; Tajima, T.; Paik, N.S.; Sandelin, K.; Derossis, A.; Cody, H.; Foulkes, W.D. Is breast cancer the same disease in Asian and western countries? World J. Surg. 2010, 34, 2308–2324. [Google Scholar] [CrossRef] [PubMed]
- Lappano, R.; Malaguarnera, R.; Belfiore, A.; Maggiolini, M. Recent advances on the stimulatory effects of metals in breast cancer. Mol. Cell. Endocrinol. 2017, 457, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Tang, J.; Xie, M. Serum and hair zinc levels in breast cancer: A meta-analysis. Sci. Rep. 2015, 5, 12249. [Google Scholar] [CrossRef] [PubMed]
- Burton, C.; Dan, Y.; Donovan, A.; Liu, K.; Shi, H.; Ma, Y.; Bosnak, C.P. Urinary metallomics as a novel biomarker discovery platform: Breast cancer as a case study. Clin. Chim. Acta. 2016, 452, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Burtis, C.A.; Ashwood, E.R.; Bruns, D.E. Tietz Textbook of Clinical Chemistry and Molecular Diagnostics; Elsevier Health Sciences: St. Louis, MO, USA, 2012. [Google Scholar]
- McPherson, R.A.; Pincus, M.R. Henry’s Clinical Diagnosis and Management by Laboratory Methods; Elsevier Health Sciences: St. Louis, MO, USA, 2016. [Google Scholar]
- Babaknejad, N.; Sayehmiri, F.; Sayehmiri, K.; Rahimifar, P.; Bahrami, S.; Delpesheh, A.; Hemati, F.; Alizadeh, S. The relationship between selenium levels and breast cancer: A systematic review and meta-analysis. Biol. Trace Elem. Res. 2014, 159, 1–7. [Google Scholar] [CrossRef]
- Ding, X.; Jiang, M.; Jing, H.; Sheng, W.; Wang, X.; Han, J.; Wang, L. Analysis of serum levels of 15 trace elements in breast cancer patients in Shandong, China. Environ. Sci. Pollut. Res. Int. 2015, 22, 7930–7935. [Google Scholar] [CrossRef]
- Wu, H.D.; Chou, S.Y.; Chen, D.R.; Kuo, H.W. Differentiation of serum levels of trace elements in normal and malignant breast patients. Biol. Trace Elem. Res. 2006, 113, 9–18. [Google Scholar] [CrossRef]
- Alatise, O.I.; Schrauzer, G.N. Lead exposure: A contributing cause of the current breast cancer epidemic in Nigerian women. Biol. Trace Elem. Res. 2010, 136, 127–139. [Google Scholar] [CrossRef]
- Kotsopoulos, J.; Sukiennicki, G.; Muszynska, M.; Gackowski, D.; Kaklewski, K.; Durda, K.; Jaworska, K.; Huzarski, T.; Gronwald, J.; Byrski, T.; et al. Plasma micronutrients, trace elements, and breast cancer in brca1 mutation carriers: An exploratory study. Cancer Causes Control 2012, 23, 1065–1074. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.F.; Lu, L.; Zeng, P.; Yang, Y.H.; Luo, J.; Yang, Y.W.; Wang, D. Serum total oxidant/antioxidant status and trace element levels in breast cancer patients. Int. J. Clin. Oncol. 2012, 17, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Pavithra, V.; Sathisha, T.G.; Kasturi, K.; Mallika, D.S.; Amos, S.J.; Ragunatha, S. Serum levels of metal ions in female patients with breast cancer. J. Clin. Diagn. Res. 2015, 9, BC25–BC27. [Google Scholar] [CrossRef] [PubMed]
- Adeoti, M.L.; Oguntola, A.S.; Akanni, E.O.; Agodirin, O.S.; Oyeyemi, G.M. Trace elements; copper, zinc and selenium, in breast cancer afflicted female patients in LAUTECH Osogbo, Nigeria. Indian J. Cancer 2015, 52, 106–109. [Google Scholar] [CrossRef] [PubMed]
- Saleh, F.; Behbehani, A.; Asfar, S.; Khan, I.; Ibrahim, G. Abnormal blood levels of trace elements and metals, DNA damage, and breast cancer in the state of Kuwait. Biol. Trace Elem. Res. 2011, 141, 96–109. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.K.; Jyoti; Singh, S.; Mehrotra, P.K.; Singh, K.; Sarangi, R. Comparison of some trace elements concentration in blood, tumor free breast and tumor tissues of women with benign and malignant breast lesions: An indian study. Environ. Int. 2006, 32, 630–637. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.; Wang, C.; Yu, W.; Fan, W.; Wang, S.; Shen, N.; Wu, P.; Li, X.; Wang, F. Selenium exposure and cancer risk: An updated meta-analysis and meta-regression. Sci. Rep. 2016, 6, 19213. [Google Scholar] [CrossRef]
- Borella, P.; Bargellini, A.; Caselgrandi, E.; Piccinini, L. Observations on the use of plasma, hair and tissue to evaluate trace element status in cancer. J. Trace Elem. Med. Biol. 1997, 11, 162–165. [Google Scholar] [CrossRef]
- Singh, P.; Kapil, U.; Shukla, N.K.; Deo, S.; Dwivedi, S.N. Association between breast cancer and vitamin c, vitamin e and selenium levels: Results of a case-control study in India. Asian Pac. J. Cancer Prev. 2005, 6, 177–180. [Google Scholar]
- Joo, N.S.; Kim, S.M.; Jung, Y.S.; Kim, K.M. Hair iron and other minerals’ level in breast cancer patients. Biol. Trace Elem. Res. 2009, 129, 28–35. [Google Scholar] [CrossRef]
- Suzana, S.; Cham, B.G.; Ahmad Rohi, G.; Mohd Rizal, R.; Fairulnizal, M.N.; Normah, H.; Fatimah, A. Relationship between selenium and breast cancer: A case-control study in the klang valley. Singap. Med. J. 2009, 50, 265–269. [Google Scholar]
- Sharhar, S.; Normah, H.; Fatimah, A.; Fadilah, R.N.; Rohi, G.A.; Amin, I.; Cham, B.G.; Rizal, R.M.; Fairulnizal, M.N. Antioxidant intake and status, and oxidative stress in relation to breast cancer risk: A case-control study. Asian Pac. J. Cancer Prev. 2008, 9, 343–349. [Google Scholar] [PubMed]
- Benderli Cihan, Y.; Sozen, S.; Ozturk Yildirim, S. Trace elements and heavy metals in hair of stage III breast cancer patients. Biol. Trace Elem. Res. 2011, 144, 360–379. [Google Scholar] [CrossRef] [PubMed]
- Kilic, E.; Saraymen, R.; Demiroglu, A.; Ok, E. Chromium and manganese levels in the scalp hair of normals and patients with breast cancer. Biol. Trace Elem. Res. 2004, 102, 19–25. [Google Scholar] [CrossRef]
- Kotsopoulos, J.; Chen, Z.; Vallis, K.A.; Poll, A.; Ghadirian, P.; Kennedy, G.; Ainsworth, P.; Narod, S.A. Toenail selenium status and DNA repair capacity among female brca1 mutation carriers. Cancer Causes Control 2010, 21, 679–687. [Google Scholar] [CrossRef]
- Moradi, M.; Hassan Eftekhari, M.; Talei, A.; Rajaei Fard, A. A comparative study of selenium concentration and glutathione peroxidase activity in normal and breast cancer patients. Public Health Nutr. 2009, 12, 59–63. [Google Scholar] [CrossRef]
- Memon, A.U.; Kazi, T.G.; Afridi, H.I.; Jamali, M.K.; Arain, M.B.; Jalbani, N.; Syed, N. Evaluation of zinc status in whole blood and scalp hair of female cancer patients. Clin. Chim. Acta 2007, 379, 66–70. [Google Scholar] [CrossRef]
- Freeland-Graves, J.H.; Sanjeevi, N.; Lee, J.J. Global perspectives on trace element requirements. J. Trace Elem. Med. Biol. 2015, 31, 135–141. [Google Scholar] [CrossRef]
- Evans, D.M.; Zhu, G.; Dy, V.; Heath, A.C.; Madden, P.A.; Kemp, J.P.; McMahon, G.; St Pourcain, B.; Timpson, N.J.; Golding, J.; et al. Genome-wide association study identifies loci affecting blood copper, selenium and zinc. Human Mol. Genet. 2013, 22, 3998–4006. [Google Scholar] [CrossRef]
- Harbeck, N.; Gnant, M. Breast cancer. Lancet 2017, 389, 1134–1150. [Google Scholar] [CrossRef]
- Qiu, S.Q.; Zeng, H.C.; Zhang, F.; Chen, C.; Huang, W.H.; Pleijhuis, R.G.; Wu, J.D.; van Dam, G.M.; Zhang, G.J. A nomogram to predict the probability of axillary lymph node metastasis in early breast cancer patients with positive axillary ultrasound. Sci. Rep. 2016, 6, 21196. [Google Scholar] [CrossRef] [PubMed]
- Bundred, N.J.; Barnes, N.L.; Rutgers, E.; Donker, M. Is axillary lymph node clearance required in node-positive breast cancer? Nat. Rev. Clin. Oncol. 2015, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; Gelber, R.D.; Piccart-Gebhart, M.; Thurlimann, B.; Senn, H.J. Personalizing the treatment of women with early breast cancer: Highlights of the St Gallen international expert consensus on the primary therapy of early breast cancer 2013. Ann. Oncol. 2013, 24, 2206–2223. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.P.; Soave, D.F.; Ribeiro-Silva, A.; Poletti, M.E. Trace elements as tumor biomarkers and prognostic factors in breast cancer: A study through energy dispersive x-ray fluorescence. BMC Res. Notes 2012, 5, 194. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Prabhu, K.S.; Mastro, A.M. Is selenium a potential treatment for cancer metastasis? Nutrients 2013, 5, 1149–1168. [Google Scholar] [CrossRef]
- Kuo, H.W.; Chen, S.F.; Wu, C.C.; Chen, D.R.; Lee, J.H. Serum and tissue trace elements in patients with breast cancer in taiwan. Biol. Trace Elem. Res. 2002, 89, 1–11. [Google Scholar] [CrossRef]
- Blockhuys, S.; Celauro, E.; Hildesjo, C.; Feizi, A.; Stal, O.; Fierro-Gonzalez, J.C.; Wittung-Stafshede, P. Defining the human copper proteome and analysis of its expression variation in cancers. Metallomics 2017, 9, 112–123. [Google Scholar] [CrossRef]
- Florea, A.M.; Busselberg, D. Metals and breast cancer: Risk factors or healing agents? J. Toxicol. 2011, 2011, 159619. [Google Scholar] [CrossRef]
- Greenlee, H.; Hershman, D.L.; Jacobson, J.S. Use of antioxidant supplements during breast cancer treatment: A comprehensive review. Breast Cancer Res. Treat. 2009, 115, 437–452. [Google Scholar] [CrossRef]
- Lee, E.; Levine, E.A.; Franco, V.I.; Allen, G.O.; Gong, F.; Zhang, Y.; Hu, J.J. Combined genetic and nutritional risk models of triple negative breast cancer. Nutr. Cancer 2014, 66, 955–963. [Google Scholar] [CrossRef]
- Xu, L.; Yin, S.; Banerjee, S.; Sarkar, F.; Reddy, K.B. Enhanced anticancer effect of the combination of cisplatin and trail in triple-negative breast tumor cells. Mol. Cancer Ther. 2011, 10, 550–557. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| 1st Dataset for Discovery Cohort | 2nd Dataset for Validation Cohort | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Control | Breast Cancer | p-Value a | Control | Breast Cancer | p-Value a | |||||||||
| n | Median | IQR | n | Median | IQR | n | Median | IQR | n | Median | IQR | |||
| Age (years) | 137 | 48.00 | 42.75–56.00 | 150 | 46.00 | 40.00–53.00 | 0.1860 | 63 | 41.00 | 31.00–48.00 | 79 | 47.00 | 43.00–53.75 | <0.0001 |
| Body Mass Index (kg/m2) | 137 | 21.40 | 19.80–23.80 | 150 | 22.54 | 20.80–24.53 | 0.0007 | 63 | 21.45 | 19.86–23.23 | 79 | 23.11 | 21.32–24.82 | 0.0008 |
| Serum Total Protein (g/dL) | 137 | 7.10 | 6.80–7.40 | 150 | 7.30 | 7.10–7.60 | 0.0001 | 63 | 7.30 | 7.00–7.50 | 79 | 7.40 | 7.10–7.70 | 0.0390 |
| Serum Albumin (g/dL) | 137 | 4.30 | 4.20–4.60 | 150 | 4.70 | 4.50–4.80 | <0.0001 | 63 | 4.60 | 4.50–4.78 | 79 | 4.60 | 4.50–4.80 | 0.8262 |
| Serum Total Cholesterol (mg/dL) | 137 | 193.00 | 172.00–218.00 | 150 | 184.50 | 163.00–210.00 | 0.0331 | 63 | 169.00 | 157.50–192.50 | 79 | 177.00 | 163.00–202.75 | 0.1664 |
| Aspartate Transaminase (IU/L) | 137 | 20.00 | 17.00–24.00 | 150 | 18.00 | 15.00–21.00 | 0.0047 | 63 | 17.00 | 15.00–21.00 | 79 | 17.00 | 15.00–21.00 | 0.9311 |
| Alanine Transaminase (IU/L) | 137 | 15.00 | 11.00–20.25 | 150 | 14.00 | 11.00–21.00 | 0.3931 | 63 | 12.00 | 10.00–17.75 | 79 | 14.00 | 12.00–18.00 | 0.0436 |
| Alkaline Phosphatase (U/L) | 137 | 54.00 | 44.00–67.00 | 149 | 57.00 | 47.00–72.00 | 0.1220 | 63 | 52.00 | 43.00–67.75 | 79 | 53.00 | 45.25–64.00 | 0.6192 |
| HDL (mg/dL) | 129 | 62.00 | 53.00–72.25 | 75 | 58.00 | 50.00–67.00 | 0.1095 | 42 | 68.50 | 60.00–78.00 | 72 | 62.50 | 51.00–73.00 | 0.0181 |
| LDL (mg/dL) | 130 | 117.00 | 98.00–138.00 | 75 | 115.00 | 95.50–135.75 | 0.7899 | 42 | 102.50 | 93.00–124.00 | 72 | 109.00 | 95.00–135.00 | 0.2218 |
| Cobalt (µg/L) | 137 | 0.24 | 0.18–0.36 | 150 | 0.31 | 0.25–0.43 | <0.0001 | 63 | 0.45 | 3.23–0.59 | 79 | 0.41 | 0.25–0.56 | 0.1787 |
| Chromium (µg/L) | 137 | 0.20 | 0.18–0.23 | 150 | 0.21 | 0.18–0.24 | 0.0767 | 63 | 0.18 | 0.15–0.23 | 79 | 0.27 | 0.20–0.31 | <0.0001 |
| Copper (µg/dL) | 137 | 95.00 | 87.00–103.00 | 150 | 100.00 | 93.00–111.00 | 0.0002 | 63 | 92.00 | 81.25–102.50 | 79 | 90.00 | 82.00–96.75 | 0.2805 |
| Manganese (µg/L) | 137 | 1.54 | 1.04–1.71 | 150 | 1.75 | 1.49–2.00 | <0.0001 | 63 | 0.58 | 0.53–0.68 | 79 | 0.64 | 0.56–0.78 | 0.0099 |
| Molybdenum (µg/L) | 137 | 1.05 | 0.88–1.30 | 150 | 1.16 | 0.95–1.50 | 0.0039 | 63 | 1.10 | 0.90–1.20 | 79 | 1.20 | 0.93–1.40 | 0.0056 |
| Selenium (µg/L) | 137 | 109.00 | 102.00–119.00 | 150 | 107.00 | 98.00–114.00 | 0.0241 | 63 | 102.00 | 95.00–112.00 | 79 | 98.00 | 92.00–112.50 | 0.0845 |
| Zinc (µg/dL) | 137 | 110.00 | 97.75–126.00 | 150 | 95.00 | 87.00–104.00 | <0.0001 | 63 | 75.00 | 67.00–85.00 | 79 | 76.00 | 72.00–82.75 | 0.5961 |
| Lymph Node Metastasis | Stage IV Breast Cancer | Triple-Negative Cancer | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No (n = 66) | Yes (n = 84) | p-Value | No (n = 136) | Yes (n = 14) | p-Value | No (n = 126) | Yes (n = 24) | p-Value | |||||||
| Median | IQR | Median | IQR | Median | IQR | Median | IQR | Median | IQR | Median | IQR | ||||
| Cobalt (µg/L) | 0.30 | 0.25–0.49 | 0.32 | 0.26–0.43 | 0.6699 | 0.31 | 0.26–0.44 | 0.29 | 0.21–0.35 | 0.1328 | 0.31 | 0.26–0.44 | 0.27 | 0.25–0.38 | 0.2463 |
| Chromium (µg/L) | 0.21 | 0.18–0.24 | 0.21 | 0.18–0.24 | 0.7977 | 0.21 | 0.18–0.24 | 0.20 | 0.18–0.23 | 0.5707 | 0.21 | 0.18–0.24 | 0.20 | 0.19–0.23 | 0.3862 |
| Copper (µg/dL) | 101.00 | 93.00–111.00 | 100.00 | 93.00–110.00 | 0.6908 | 100.00 | 92.00–110.00 | 108.00 | 95.00–147.00 | 0.0479 b | 100.50 | 93.00–110.00 | 99.00 | 92.50–112.00 | 0.8818 |
| Manganese (µg/L) | 1.72 | 1.49–2.01 | 1.75 | 1.49–1.99 | 0.8011 a | 1.75 | 1.50–1.99 | 1.73 | 1.40–2.07 | 0.6716 a | 1.76 | 1.49–2.02 | 1.63 | 1.48–1.83 | 0.2243 a |
| Molybdenum (µg/L) | 1.22 | 0.95–1.57 | 1.13 | 0.95–1.44 | 0.2899 | 1.18 | 0.96–1.50 | 1.10 | 0.89–1.27 | 0.4009 | 1.19 | 0.96–1.50 | 1.02 | 0.93–1.50 | 0.5183 |
| Selenium (µg/L) | 107.00 | 100.00–115.00 | 107.50 | 96.00–114.00 | 0.4133 | 108.00 | 99.00–114.50 | 97.00 | 82.00–110.00 | 0.0437 b | 107.50 | 99.00–114.00 | 103.50 | 97.50–119.00 | 0.8899 |
| Zinc (µg/dL) | 95.00 | 87.00–106.00 | 95.00 | 87.00–104.00 | 0.6801 a | 96.00 | 87.00–105.00 | 90.00 | 87.00–102.00 | 0.2190 a | 96.00 | 87.00–105.00 | 91.50 | 87.00–101.00 | 0.6517 |
| Region | n of Breast Cancer | n of Controls | Specimen | Tested Trace Elements | Significantly Low in Breast Cancer | Significantly High in Breast Cancer | Specific Subgroups of Breast Cancer a | Reference |
|---|---|---|---|---|---|---|---|---|
| Nigeria | 12 | 12 | whole blood, hair | whole blood: Cu, Zn, Pb, Se, Cd, Hg, As, Mn, Sr, Ca, Mg, Li, Co hair: Pb, Cd, Hg, As, Cu, Zn, Se, Mn, Sr, Ca, Mg, Li, Co, I, S, P, Ag, Fe, Cr, V, Mo, B, Na, K, Ba, Be, Bi, Ni, Tl, Th, U, Ti, Sn, Al | blood: none hair: Se, Sr, Ca, Co, Na | blood: Cu, Pb, Li hair: Cd, Cu | - | [12] |
| Italy | 80 | 58 | plasma, hair | Cu, Zn, Se | plasma: Se, Zn hair: none | plasma: none hair: none | - | [20] |
| India | 25 | 25 | whole blood | Pb, Cu, Zn, Ca, Fe | Cu | Zn, Fe, Ca | - | [18] |
| India | 160 | 160 | plasma | Se | - | - | - | [21] |
| Taiwan | 25 | 26 | serum | Se, Zn, Cd, Co, Ni, Mn, Fe, Cr, Mg, Al, Ca, Cu, Ag | Se, Zn, Mn, Mg | Cd, Ni, Fe, Cr, Al, Cu | - | [11] |
| Nigeria | 30 | 30 | serum | Cu, Zn, Se | Cu, Zn, Se | - | - | [16] |
| India | 54 | 54 | serum | Ca, Cu, Mg, Fe, P, Zn | Zn | Cu, Fe, P, Ca | - | [15] |
| China | 88 | 84 | serum | Zn, Mn, Al, Cd, Fe, Mg, Ca, Pb, Cu, Se, Ni, Ti, Co, Li, Cr | Mn, Al, Fe, Ti | Cd, Mg, Cu, Co, Li | - | [10] |
| China | 56 | 20 | serum | Cu, Zn, Fe, Se, Mg, Mn | Zn, Se, Mg, Mn | Cu, Fe | - | [14] |
| Korea | 40 | 144 | hair | Ca, Mg, Na, K, Fe, Zn, Cu, Mn, Se, As, P, Cr, U, Cd, Pb, Al, Hg | Ca, Mg, Fe, Zn, Cu, Mn, Pb | Na, K, As | - | [22] |
| Korea | 229 | 200 | serum | Co, Cr, Cu, Mn, Mo, Se, Zn | - | Mn, Mo | - | This study |
| Malaysia | 64 | 127 | hair, toenail | Se | - | - | - | [23] |
| Malaysia | 57 | 139 | hair, toenail | Se | hair: Se toenail: Se | - | - | [24] |
| Kuwait | 50 | 50 | whole blood | Cu, Zn, Se, Cd | Cu, Zn, Se | Cd | Stage I | [17] |
| Turkey | 52 | 52 | hair | Ag, Al, As, Au, B, Ba, Be, Bi, Ca, Cd, Ce, Co, Cr, Cs, Cu, Fe, Ga, Hg, K, Li, Mg, Mn, Na, Ni, Pb, Pd, Rb, Rh, Sb, Sc, Se, Sn, Sr, Ti, V, Zn | Ag, Au, Ba, Be, Bi, Ca, Ga, Hg, Mg, Ni, Pb, Pd, Se, Sn, Sr, Ti, Zn | Al, As, B, Cd, Ce, Co, Cr, Cs, Cu, Fe, K, Li, Mn, Na, Rb, Rh, Sb, V | Stage III | [25] |
| Turkey | 26 | 27 | hair | Cr, Mn | Mn | Cr | Stage III | [26] |
| Canada | 48 | 96 | plasma | Sb, As, Ca, Cd, Cr, Cu, Fe, Mg, Se, Zn | Fe | - | BRCA1 mutation carriers | [13] |
| Canada | 25 | 50 | toenail | Se | - | - | BRCA1 mutation carriers | [27] |
| Trace Elements | Region | n of Breast Cancer | n of Controls | Specimen | Concentration in Breast Cancer | Concentration in Controls | p-value | Values | References |
|---|---|---|---|---|---|---|---|---|---|
| Co (µg/L) | Korea | 150 | 137 | serum | 0.42 (0.18–4.03) | 0.31 (0.12–1.21) | <0.0001 | mean (range) | This study a |
| Co (µg/L) | Korea | 79 | 63 | serum | 0.48 (0.12–2.39) | 0.21 (0.12–0.51) | 0.1787 | mean (range) | This study b |
| Co (µg/L) | Taiwan | 25 | 26 | serum | 0.51 ± 0.05 | 0.49 ± 0.08 | NS | mean ± SD | [11] |
| Co (µg/L) | China c | 88 | 84 | serum | 2.12 ± 1.33 | 1.69 ± 0.54 | 0.006 | mean ± SD | [10] |
| Co (µg/L) | Nigeria | 12 | 12 | blood | 0.42 (0.2–1.1) | 0.53 (0.2–0.9) | 0.91 | mean (range) | [12] |
| Cr (µg/L) | Korea | 150 | 137 | serum | 0.22 (0.12–0.54) | 0.21 (0.12–0.51) | 0.0767 | mean (range) | This study a |
| Cr (µg/L) | Korea | 79 | 63 | serum | 0.32 (0.14–4.05) | 0.19 (0.10–0.31) | <0.0001 | mean (range) | This study b |
| Cr (µg/L) | Taiwan | 25 | 26 | serum | 1.36 ± 0.26 | 0.64 ± 0.20 | <0.01 | mean ± SD | [11] |
| Cr (µg/L) | China | 88 | 84 | serum | 15.0 ± 5.4 | 13.3 ± 5.4 | 0.052 | mean ± SD | [10] |
| Cr (µg/L) | Canada | 48 | 96 | plasma | 3.03 (2.12–4.19) | 3.11 (2.12–6.00) | 0.35 | mean (range) | [13] |
| Cu (µg/dL) | Korea | 150 | 137 | serum | 104.18 (65.00–239.00) | 96.18 (63.00–149.00) | 0.0002 | mean (range) | This study a |
| Cu (µg/dL) | Korea | 79 | 63 | serum | 90.00 (58.00–128.00) | 92.67 (63.00–129.00) | 0.2805 | mean (range) | This study b |
| Cu (µg/dL) | Taiwan c | 25 | 26 | serum | 125.2 ± 15.1 | 96.5 ± 7.0 | <0.01 | mean ± SD | [11] |
| Cu (µg/dL) | Nigeria | 30 | 30 | serum | 95.3 ± 4.9 | 65.2 ± 15.0 | <0.01 | mean ± SD | [16] |
| Cu (µg/dL) | India | 54 | 54 | serum | 202.21 ± 89.18 | 109.56 ± 30.72 | <0.001 | mean ± SD | [15] |
| Cu (µg/dL) | China c | 88 | 84 | serum | 137.2 ± 36.2 | 113.2 ± 13.6 | <0.001 | mean ± SD | [10] |
| Cu (µg/dL) | China c | 56 | 20 | serum | 115.9 (92.4–14.0) | 101.6 (80.5–115.8) | <0.01 | mean (range) | [14] |
| Cu (µg/dL) | Canada c | 48 | 96 | plasma | 115.4 (36.7–170.6) | 113.9 (79.9–237.1) | 0.74 | mean (range) | [13] |
| Cu (µg/dL) | Nigeria | 12 | 12 | blood | 132.5 (105–157) | 98.9 (76–145) | <0.001 | mean (range) | [12] |
| Cu (µg/dL) | India d | 25 | 25 | blood | 65.0 (30.0–150.0) | 68.0 (45–130.0) | NS | mean (range) | [18] |
| Cu (µg/dL) | Kuwait e | 50 | 50 | blood | 133.0 ± 34.0 | 147.0 ± 45.0 | 0.0006 | mean ± SD | [17] |
| Mn (µg/L) | Korea | 150 | 137 | serum | 1.76 (0.71–2.79) | 1.43 (0.61–2.27) | <0.0001 | mean (range) | This study a |
| Mn (µg/L) | Korea | 79 | 63 | serum | 0.68 (0.37–1.08) | 0.64 (0.40–1.66) | 0.0099 | mean (range) | This study b |
| Mn (µg/L) | China | 88 | 84 | serum | 7.4 ± 7.9 | 19.9 ± 11.0 | <0.001 | mean ± SD | [10] |
| Mn (µg/L) | China | 56 | 20 | serum | 8.30 (5.38–11.75) | 10.95 (8.55–12.28) | <0.01 | mean (range) | [14] |
| Mo (µg/L) | Korea | 150 | 137 | serum | 1.32 (0.59–4.77) | 1.10 (0.48–1.99) | 0.0039 | mean (range) | This study a |
| Mo (µg/L)Se (µg/L) | Korea | 79 | 63 | serum | 1.30 (0.70–8.30) | 1.08 (0.50–2.20) | 0.0056 | mean (range) | This study b |
| Korea | 150 | 137 | serum | 106.63 (68.00–179.00) | 110.99 (84.00–197.00) | 0.0241 | mean (range) | This study a | |
| Se (µg/L) | Korea | 79 | 63 | serum | 100.75 (75.00–154.00) | 104.67 (81.00–153.00) | 0.0845 | mean (range) | This study b |
| Se (µg/L) | Nigeria | 30 | 30 | serum | 45.0 ± 4.6 | 76.4 ± 8.9 | <0.01 | mean ± SD | [16] |
| Se (µg/L) | China | 88 | 84 | serum | 91.4 ± 20.0 | 95.8 ± 22.7 | 0.236 | mean ± SD | [10] |
| Se (µg/L) | China | 56 | 20 | serum | 71.4 (59.2–83.9) | 81.3 (72.3–95.3) | <0.01 | mean (range) | [14] |
| Se (µg/L) | Canada | 48 | 96 | plasma | 100.0 (47.76–1161.2) | 85.90 (49.74–933.4) | 0.57 | mean (range) | [13] |
| Se (µg/L) | Kuwait | 50 | 50 | blood | 64.06 ± 16.05 | 88.64 ± 19.03 | <0.0001 | mean ± SD | [17] |
| Se (µg/L) | Iran | 45 | 45 | plasma | 138.40 ± 40.36 | 132.15 ± 35.37 | NS | mean ± SD | [28] |
| Zn (µg/dL) | Korea | 150 | 137 | serum | 96.07 (62.00–150.00) | 113.52 (76.00–159.00) | <0.0001 | mean (range) | This study a |
| Zn (µg/dL) | Korea | 79 | 63 | serum | 77.49 (54.00–111.00) | 76.68 (60.00–107.00) | 0.5961 | mean (range) | This study b |
| Zn (µg/dL) | Nigeria | 30 | 30 | serum | 62.7 ± 15.7 | 93.5 ± 7.2 | <0.01 | mean ± SD | [16] |
| Zn (µg/dL) | Pakistan c | 65 | 50 | blood | 59.7 ± 3.5 | 100.9 ± 7.5 | <0.001 | mean ± SD | [29] |
| Zn (µg/dL) | China c | 88 | 84 | serum | 111.0 ± 23.6 | 113.1 ± 21.5 | 0.824 | mean ± SD | [10] |
| Zn (µg/dL) | China c | 56 | 20 | serum | 93.9 (77.1–111.0) | 106.1 (92.8–119.7) | <0.01 | mean (range) | [14] |
| Zn (µg/dL) | Canada c | 48 | 96 | plasma | 80.5 (21.9–191.1) | 77.2 (57.7–137.9) | 0.36 | mean (range) | [13] |
| Zn (µg/dL) | Kuwait e | 50 | 50 | blood | 99.0 ± 39.0 | 360 ± 110.0 | <0.0001 | mean ± SD | [17] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, R.; Kim, M.-J.; Sohn, I.; Kim, S.; Kim, I.; Ryu, J.M.; Choi, H.J.; Kim, J.-M.; Lee, S.K.; Yu, J.; et al. Serum Trace Elements and Their Associations with Breast Cancer Subgroups in Korean Breast Cancer Patients. Nutrients 2019, 11, 37. https://doi.org/10.3390/nu11010037
Choi R, Kim M-J, Sohn I, Kim S, Kim I, Ryu JM, Choi HJ, Kim J-M, Lee SK, Yu J, et al. Serum Trace Elements and Their Associations with Breast Cancer Subgroups in Korean Breast Cancer Patients. Nutrients. 2019; 11(1):37. https://doi.org/10.3390/nu11010037
Chicago/Turabian StyleChoi, Rihwa, Min-Ji Kim, Insuk Sohn, Serim Kim, Isaac Kim, Jai Min Ryu, Hee Jun Choi, Jae-Myung Kim, Se Kyung Lee, Jonghan Yu, and et al. 2019. "Serum Trace Elements and Their Associations with Breast Cancer Subgroups in Korean Breast Cancer Patients" Nutrients 11, no. 1: 37. https://doi.org/10.3390/nu11010037
APA StyleChoi, R., Kim, M.-J., Sohn, I., Kim, S., Kim, I., Ryu, J. M., Choi, H. J., Kim, J.-M., Lee, S. K., Yu, J., Kim, S. W., Nam, S. J., Lee, J. E., & Lee, S.-Y. (2019). Serum Trace Elements and Their Associations with Breast Cancer Subgroups in Korean Breast Cancer Patients. Nutrients, 11(1), 37. https://doi.org/10.3390/nu11010037