Diet-Quality and Socio-Demographic Factors Associated with Non-Nutritive Sweetener Use in the Australian Population


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Coding
2.3. Statistical Analysis
3. Results
3.1. Population Subgroups Comparisons
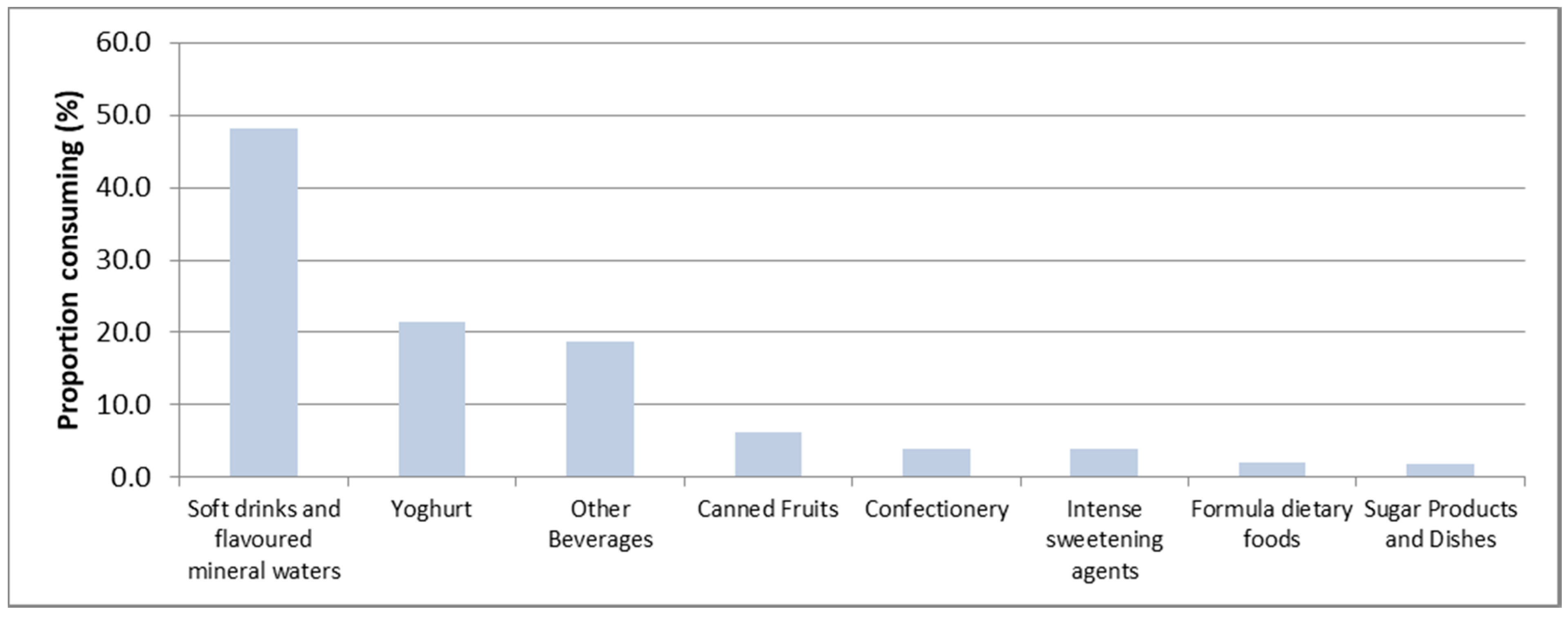
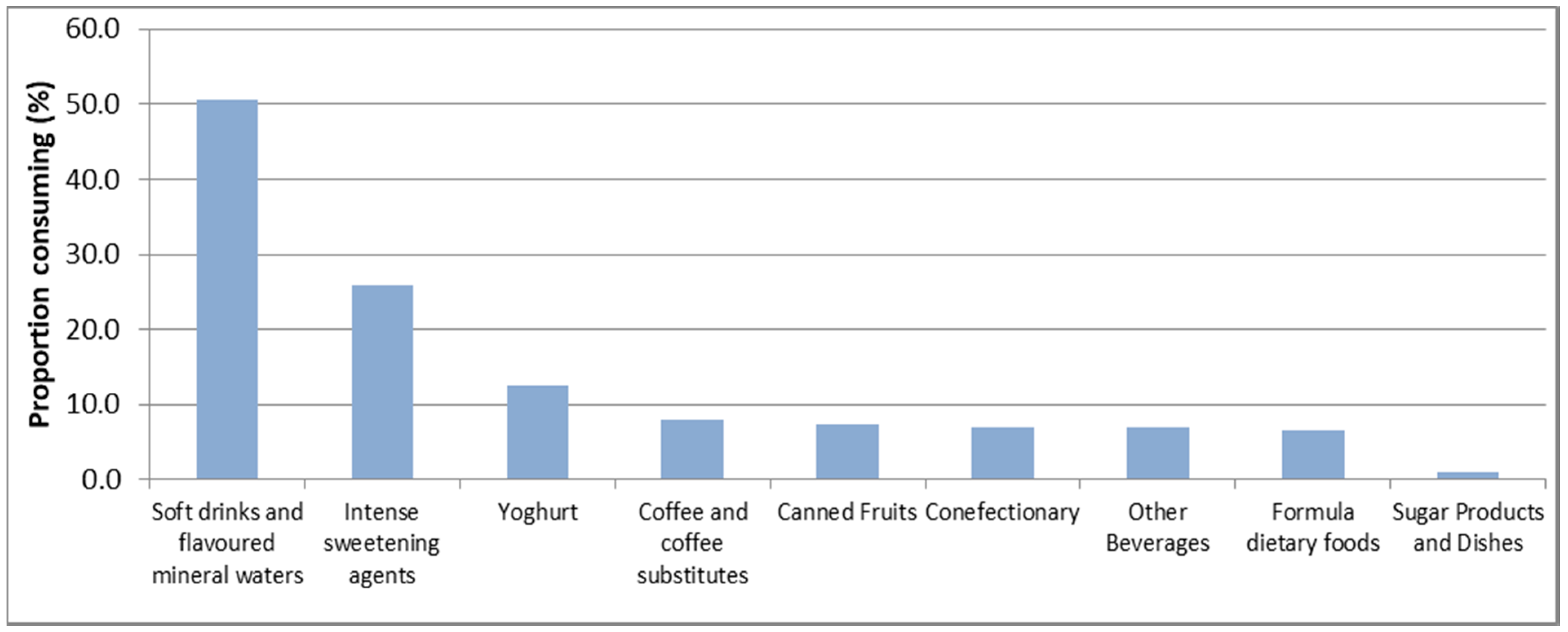
3.2. Major Dietary Sources of NNS
3.3. Food and Nutrient Intakes
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Conflicts of Interest
References
- Food Standards Australia New Zealand. Standard 1.2.4—Information Requirements—Statement of Ingredients; FSANZ: Canberra, Australia, 2015.
- Food Standards Australia New Zealand. Schedule 15—Substances that May Be Used as Food Additives; FSANZ: Canberra, Australia, 2015.
- Miller, P.E.; Perez, V. Low-calorie sweeteners and body weight and composition: A meta-analysis of randomized controlled trials and prospective cohort studies. Am. J. Clin. Nutr. 2014, 100, 765–777. [Google Scholar] [CrossRef] [PubMed]
- Peters, J.C.; Beck, J.; Cardel, M.; Wyatt, H.R.; Foster, G.D.; Pan, Z.; Wojtanowski, A.C.; Vander Veur, S.S.; Herring, S.J.; Brill, C.; et al. The effects of water and non-nutritive sweetened beverages on weight loss and weight maintenance: A randomized clinical trial. Obesity 2016, 24, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Romo-Romo, A.; Aguilar-Salinas, C.A.; Brito-Córdova, G.X.; Gómez Díaz, R.A.; Vilchis Valentín, D.; Almeda-Valdes, P. Effects of the non-nutritive sweeteners on glucose metabolism and appetite regulating hormones: Systematic review of observational prospective studies and clinical trials. PLoS ONE 2016, 11, e0161264. [Google Scholar] [CrossRef] [PubMed]
- Karalexi, M.A.; Mitrogiorgou, M.; Georgantzi, G.G.; Papaevangelou, V.; Fessatou, S. Non-nutritive sweeteners and metabolic health outcomes in children: A systematic review and meta-analysis. J. Pediatr. 2018, 197, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Gardner, C.; Wylie-Rosett, J.; Gidding, S.S.; Steffen, L.M.; Johnson, R.K.; Reader, D.; Lichtenstein, A.H. Nonnutritive sweeteners: Current use and health perspectives: A scientific statement from the American heart association and the American diabetes association. Circulation 2012, 126, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Rogers, P.; Hogenkamp, P.; De Graaf, C.; Higgs, S.; Lluch, A.; Ness, A.; Penfold, C.; Perry, R.; Putz, P.; Yeomans, M. Does low-energy sweetener consumption affect energy intake and body weight? A systematic review, including meta-analyses, of the evidence from human and animal studies. Int. J. Obes. 2016, 40, 381. [Google Scholar] [CrossRef] [PubMed]
- Sylvetsky, A.C.; Rother, K.I. Nonnutritive sweeteners in weight management and chronic disease: A review. Obesity 2018, 26, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Chattopadhyay, S.; Raychaudhuri, U.; Chakraborty, R. Artificial sweeteners—A review. J. Food Sci. Technol. 2014, 51, 611–621. [Google Scholar] [CrossRef] [PubMed]
- Whitehouse, C.R.; Boullata, J.; McCauley, L.A. The potential toxicity of artificial sweeteners. AAOHN J. Off. J. Am. Assoc. Occup. Health Nurses 2008, 56, 251–259. [Google Scholar] [CrossRef]
- Fowler, S.P.; Williams, K.; Resendez, R.G.; Hunt, K.J.; Hazuda, H.P.; Stern, M.P. Fueling the obesity epidemic? Artificially sweetened beverage use and long-term weight gain. Obesity 2008, 16, 1894–1900. [Google Scholar] [CrossRef] [PubMed]
- De Koning, L.; Malik, V.S.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Sugar-sweetened and artificially sweetened beverage consumption and risk of type 2 diabetes in men. Am. J. Clin. Nutr. 2011, 93, 1321–1327. [Google Scholar] [CrossRef] [PubMed]
- Imamura, F.; O’Connor, L.; Ye, Z.; Mursu, J.; Hayashino, Y.; Bhupathiraju, S.N.; Forouhi, N.G. Consumption of sugar sweetened beverages, artificially sweetened beverages, and fruit juice and incidence of type 2 diabetes: Systematic review, meta-analysis, and estimation of population attributable fraction. BMJ 2015, 351, h3576. [Google Scholar] [CrossRef] [PubMed]
- Sylvetsky, A.C.; Welsh, J.A.; Brown, R.J.; Vos, M.B. Low-calorie sweetener consumption is increasing in the United States. Am. J. Clin. Nutr. 2012, 96, 640–646. [Google Scholar] [CrossRef] [PubMed]
- Sylvetsky, A.C.; Jin, Y.; Clark, E.J.; Welsh, J.A.; Rother, K.I.; Talegawkar, S.A. Consumption of low-calorie sweeteners among children and adults in the united states. J. Acad. Nutr. Diet. 2017, 117, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Food Standards Australia New Zealand. Consumption of Intense Sweeteners in Australia and New Zealand; FSANZ: Canberra, Australia, 2004.
- Australian Bureau of Statistics. 4363.0.55.001—Australian Health Survey: User’s Guide, 2011–13; ABS: Canberra, Australia, 2013.
- Food Standards Australia New Zealand. Ausnut 2011–13 Food Nutrient Database; FSANZ: Canberra, Australia, 2014.
- Food Standards Australia New Zealand. Ausnut 2011–13 Food Details File; FSANZ: Canberra, Australia, 2016.
- Drewnowski, A.; Rehm, C.D. Socio-demographic correlates and trends in low-calorie sweetener use among adults in the United States from 1999 to 2008. Eur. J. Clin. Nutr. 2015, 69, 1035–1041. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Rehm, C. The use of low-calorie sweeteners is associated with self-reported prior intent to lose weight in a representative sample of US adults. Nutr. Diabetes 2016, 6, e202. [Google Scholar] [CrossRef] [PubMed]
- Hedrick, V.E.; Passaro, E.M.; Davy, B.M.; You, W.; Zoellner, J.M. Characterization of non-nutritive sweetener intake in rural southwest Virginian adults living in a health-disparate region. Nutrients 2017, 9, 757. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Haase, A.M.; Steptoe, A.; Nillapun, M.; Jonwutiwes, K.; Bellisie, F. Gender differences in food choice: The contribution of health beliefs and dieting. Ann. Behav. Med. 2004, 27, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Rehm, C.D. Consumption of low-calorie sweeteners among us adults is associated with higher healthy eating index (HEI 2005) scores and more physical activity. Nutrients 2014, 6, 4389–4403. [Google Scholar] [CrossRef] [PubMed]
- Romo-Romo, A.; Almeda-Valdés, P.; Brito-Córdova, G.X.; Gómez-Pérez, F.J. Prevalence of non-nutritive sweeteners consumption in a population of patients with diabetes in mexico. Gac. Med. Mex. 2017, 153. [Google Scholar]
- Tey, S.L.; Salleh, N.B.; Henry, J.; Forde, C.G. Effects of aspartame-, monk fruit-, stevia- and sucrose-sweetened beverages on postprandial glucose, insulin and energy intake. Int. J. Obes. 2017, 41, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Mandrioli, D.; Kearns, C.E.; Bero, L.A. Relationship between research outcomes and risk of bias, study sponsorship, and author financial conflicts of interest in reviews of the effects of artificially sweetened beverages on weight outcomes: A systematic review of reviews. PLoS ONE 2016, 11, e0162198. [Google Scholar] [CrossRef] [PubMed]
- Gibson, S.A.; Horgan, G.W.; Francis, L.E.; Gibson, A.A.; Stephen, A.M. Low calorie beverage consumption is associated with energy and nutrient intakes and diet quality in British adults. Nutrients 2016, 8, 9. [Google Scholar] [CrossRef] [PubMed]
- Winther, R.; Aasbrenn, M.; Farup, P.G. Intake of non-nutritive sweeteners is associated with an unhealthy lifestyle: A cross-sectional study in subjects with morbid obesity. BMC Obes. 2017, 4, 41. [Google Scholar] [CrossRef] [PubMed]
- Grech, A.; Sui, Z.; Siu, H.Y.; Zheng, M.; Allman-Farinelli, M.; Rangan, A. Socio-demographic determinants of diet quality in australian adults using the validated healthy eating index for Australian adults (Heifa-2013). Healthcare 2017, 5, 7. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Australian Health Survey: Consumption of Added Sugars, 2011–12; ABS: Canberra, Australia, 2016.
- Subar, A.F.; Freedman, L.S.; Tooze, J.A.; Kirkpatrick, S.I.; Boushey, C.; Neuhouser, M.L.; Thompson, F.E.; Potischman, N.; Guenther, P.M.; Tarasuk, V. Addressing current criticism regarding the value of self-report dietary data. J. Nutr. 2015, 145, 2639–2645. [Google Scholar] [CrossRef] [PubMed]
- Poslusna, K.; Ruprich, J.; de Vries, J.H.; Jakubikova, M.; van‘t Veer, P. Misreporting of energy and micronutrient intake estimated by food records and 24 hour recalls, control and adjustment methods in practice. Br. J. Nutr. 2009, 101, S73–S85. [Google Scholar] [CrossRef] [PubMed]
- Thompson, F.E.; Kirkpatrick, S.I.; Subar, A.F.; Reedy, J.; Schap, T.E.; Wilson, M.M.; Krebs-Smith, S.M. The national cancer institute’s dietary assessment primer: A resource for diet research. J. Acad. Nutr. Diet. 2015, 115, 1986–1995. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Prevalence (%) | p-Value |
|---|---|---|
| All | 8.5 | - |
| Age (years) | ||
| 2–3 (n = 464) | 4.8 | <0.0001 * |
| 4–8 (n = 789) | 4.9 | |
| 9–13 (n = 787) | 9.7 | |
| 14–18 (n = 772) | 11.4 | |
| Gender | ||
| Male (n = 1420) | 8.0 | 0.3105 |
| Female (n = 1392) | 9.0 | |
| Socioeconomic status | ||
| Low (n = 478) | 6.0 | 0.0773 |
| Medium (n = 1626) | 9.3 | |
| High (n = 708) | 8.4 | |
| Country of birth | ||
| Australia (n = 2530) | 7.9 | <0.0001 * |
| Other English-speaking countries (n = 123) | 20.8 | |
| Other (n = 159) | 8.8 | |
| Body mass index (BMI) status | ||
| Underweight (n = 123) | 9.9 | 0.0231 |
| Normal (n = 1595) | 7.5 | |
| Overweight (n = 427) | 11.3 | |
| Obese (n = 158) | 12.3 | |
| Physical activity | ||
| Meets recommendations (n = 1195) | 7.9 | 0.6567 |
| Does not meet recommendations (n = 1617) | 7.4 | |
| Energy reporting status | ||
| Low (n = 261) | 14.8 | 0.0005 |
| Plausible (n = 1956) | 8.1 | |
| High (n = 101) | 4.8 |
| Characteristics | Prevalence (%) | p-Value |
|---|---|---|
| All | 18.2 | - |
| Age (years) | ||
| 19–30 (n = 1592) | 16.0 | 0.0178 |
| 31–50 (n = 3565) | 18.5 | |
| 51–70 (n = 2906) | 19.4 | |
| 71 and over (n = 1278) | 19.0 | |
| Gender | ||
| Male (n = 4282) | 16.8 | <0.0003 * |
| Female (n = 5059) | 19.7 | |
| Socioeconomic status | ||
| Low (n = 1760) | 19.4 | 0.3347 |
| Medium (n = 5547) | 18.1 | |
| High (n = 2134) | 17.6 | |
| Education | ||
| High school or less (n = 3636) | 18.3 | 0.0854 |
| Vocational college (n = 2193) | 18.0 | |
| University (n = 3369) | 18.6 | |
| Country of birth | ||
| Australia (n = 6627) | 20.2 | <0.0001 * |
| Other English-speaking countries (n = 1152) | 17.6 | |
| Other (n = 1562) | 11.9 | |
| BMI status | ||
| Underweight (n = 116) | 7.2 | <0.0001 * |
| Normal (n = 2678) | 12.6 | |
| Overweight (n = 2883) | 18.9 | |
| Obese (n = 2196) | 25.7 | |
| Physical activity | ||
| Meets recommendations (n = 4593) | 19.1 | 0.0423 |
| Does not meet recommendations (n = 4678) | 17.4 | |
| Self-reported diabetes | ||
| Yes (n = 640) | 38.4 | <0.0001 * |
| No (n = 8701) | 17.0 | |
| Weight-loss diet | ||
| Yes (n = 615) | 35.1 | <0.0001 * |
| No (n = 8726) | 17.0 | |
| Smoking | ||
| Yes (n = 1769) | 17.3 | 0.2846 |
| No (n = 7572) | 18.4 | |
| Energy reporting status | ||
| Low (n = 1587) | 24.0 | <0.0001 * |
| Plausible (n = 6200) | 17.3 | |
| High (n = 137) | 10.3 |
| Male | Female | |||||
|---|---|---|---|---|---|---|
| C | NC | p-value | C | NC | p-value | |
| Dietary component | ||||||
| Energy (kJ) | 8300 | 8578 | 0.3117 | 7404 | 7212 | 0.3896 |
| Nutrients | ||||||
| Carbohydrates (%E) | 48.1 | 50.1 | 0.0045 | 50.6 | 49.9 | 0.2880 |
| Total Sugars (%E) | 21.2 | 22.7 | 0.0276 | 24.4 | 23.0 | 0.0387 |
| Free Sugar (%E) | 11.3 | 13.2 | 0.0048 | 13.4 | 12.7 | 0.3064 |
| Total Fat (%E) | 30.9 | 31.0 | 0.9586 | 30.7 | 31.2 | 0.4039 |
| Saturated Fat (%E) | 13.5 | 13.7 | 0.6564 | 13.8 | 13.6 | 0.5630 |
| MUFA (%E) | 11.5 | 11.3 | 0.5186 | 10.9 | 11.4 | 0.0970 |
| PUFA (%E) | 4.1 | 4.1 | 0.8603 | 4.0 | 4.2 | 0.1458 |
| Protein (%E) | 18.1 | 16.1 | <0.0001 * | 15.7 | 16.1 | 0.3869 |
| Sodium (mg) | 2479 | 2489 | 0.8964 | 2002 | 2038 | 0.5795 |
| Fibre (%E) | 2.0 | 2.0 | 0.3230 | 2.0 | 2.1 | 0.1348 |
| Food Groups | ||||||
| Discretionary Foods (%E) | 32.7 | 37.0 | 0.0132 | 36.9 | 36.1 | 0.6092 |
| Grains and Cereals (serves) | 4.8 | 4.8 | 0.8514 | 3.9 | 3.9 | 0.6923 |
| Meat & Alternatives (serves) | 1.6 | 1.2 | <0.0001 * | 0.9 | 1.0 | 0.3615 |
| Dairy & alternatives (serves) | 2.1 | 1.6 | 0.0001 * | 1.5 | 1.4 | 0.3213 |
| Fruit (serves) | 1.5 | 1.8 | 0.1438 | 1.8 | 1.6 | 0.2588 |
| Vegetables (serves) | 1.7 | 1.9 | 0.2168 | 1.3 | 1.6 | 0.0195 |
| Male | Female | |||||
|---|---|---|---|---|---|---|
| C | NC | p-value | C | NC | p-value | |
| Dietary component | ||||||
| Energy (kJ) | 9665 | 9863 | 0.1573 | 7238 | 7408 | 0.0684 |
| Nutrients | ||||||
| Carbohydrates (%E) | 42.8 | 43.4 | 0.1154 | 42.3 | 43.8 | <0.0001 * |
| Total Sugars (%E) | 18.1 | 18.7 | 0.0789 | 19.2 | 19.9 | 0.0209 |
| Free Sugar (%E) | 9.2 | 10.7 | <0.0001 * | 9.2 | 10.3 | <0.0001 * |
| Total Fat (%E) | 30.5 | 30.3 | 0.5978 | 31.1 | 31.3 | 0.4329 |
| Saturated Fat (%E) | 11.9 | 12.0 | 0.4937 | 11.9 | 12.2 | 0.1099 |
| MUFA (%E) | 11.8 | 11.6 | 0.2112 | 11.9 | 11.9 | 0.8910 |
| PUFA (%E) | 4.7 | 4.6 | 0.1968 | 5.0 | 5.0 | 0.5831 |
| Protein (%E) | 19.5 | 17.9 | <0.0001 * | 19.9 | 18.1 | <0.0001 * |
| Sodium (mg) | 2838 | 2677 | 0.0005 * | 2112 | 2062 | 0.0979 |
| Fibre (%E) | 2.2 | 2.1 | 0.2967 | 2.3 | 2.4 | 0.0613 |
| Food Groups | ||||||
| Discretionary Foods (%E) | 33.7 | 34.4 | 0.307 | 30.4 | 30.6 | 0.8011 |
| Grains and Cereals (serves) | 5.0 | 5.2 | 0.0912 | 3.7 | 3.9 | 0.0011 |
| Meat and Alternatives (serves) | 2.2 | 2.1 | 0.3305 | 1.7 | 1.6 | 0.0139 |
| Dairy and alternatives (serves) | 1.7 | 1.4 | <0.0001 * | 1.5 | 1.3 | <0.0001 * |
| Fruit (serves) | 1.7 | 1.5 | 0.0496 | 1.4 | 1.5 | 0.0474 |
| Vegetables (serves) | 2.9 | 3.2 | 0.0013 | 2.8 | 3.0 | 0.0034 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grech, A.; Kam, C.O.; Gemming, L.; Rangan, A. Diet-Quality and Socio-Demographic Factors Associated with Non-Nutritive Sweetener Use in the Australian Population. Nutrients 2018, 10, 833. https://doi.org/10.3390/nu10070833
Grech A, Kam CO, Gemming L, Rangan A. Diet-Quality and Socio-Demographic Factors Associated with Non-Nutritive Sweetener Use in the Australian Population. Nutrients. 2018; 10(7):833. https://doi.org/10.3390/nu10070833
Chicago/Turabian StyleGrech, Amanda, Chi On Kam, Luke Gemming, and Anna Rangan. 2018. "Diet-Quality and Socio-Demographic Factors Associated with Non-Nutritive Sweetener Use in the Australian Population" Nutrients 10, no. 7: 833. https://doi.org/10.3390/nu10070833
APA StyleGrech, A., Kam, C. O., Gemming, L., & Rangan, A. (2018). Diet-Quality and Socio-Demographic Factors Associated with Non-Nutritive Sweetener Use in the Australian Population. Nutrients, 10(7), 833. https://doi.org/10.3390/nu10070833