Effects of Multivitamin, Multimineral and Phytonutrient Supplementation on Nutrient Status and Biomarkers of Heart Health Risk in a Russian Population: A Randomized, Double Blind, Placebo Controlled Study

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
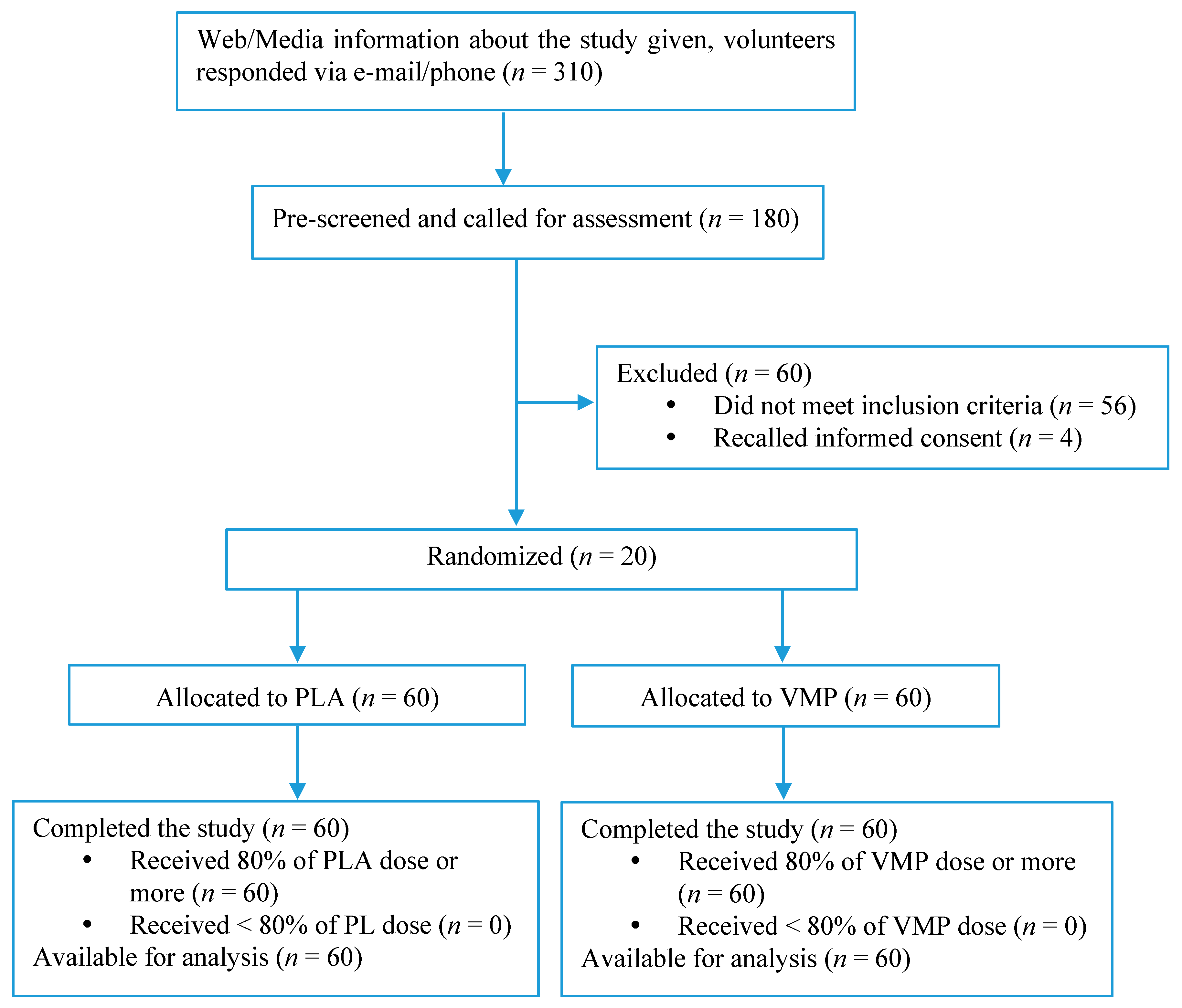
2.1. Study Population and Design
2.2. Study Samples
2.3. Questionnaires
2.4. Nutrient Analysis
2.5. Biomarkers of Heart Health Risk
2.6. Data Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A
References
- Zhang, D.; Cogswell, M.E.; Wang, G.; Bowman, B.A. Evidence of dietary improvement and preventable costs of cardiovascular disease. Am. J. Cardiol. 2017, 120, 1681–1688. [Google Scholar] [CrossRef] [PubMed]
- Egert, S.; Bosy-Westphal, A.; Seiberl, J.; Kurbitz, C.; Settler, U.; Plachta-Danielzik, S.; Wagner, A.E.; Frank, J.; Schrezenmeir, J.; Rimbach, G.; et al. Quercetin reduces systolic blood pressure and plasma oxidised low-density lipoprotein concentrations in overweight subjects with a high-cardiovascular disease risk phenotype: A double-blinded, placebo-controlled cross-over study. Br. J. Nutr. 2009, 102, 1065–1074. [Google Scholar] [CrossRef] [PubMed]
- Jagtap, S.; Meganathan, K.; Wagh, V.; Winkler, J.; Hescheler, J.; Sachinidis, A. Chemoprotective mechanism of the natural compounds, epigallocatechin-3-o-gallate, quercetin and curcumin against cancer and cardiovascular diseases. Curr. Med. Chem. 2009, 16, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.; Chandra, S.; Alexander, S.; Soble, J.; Williams, K.A., Sr. Plant-based nutrition: An essential component of cardiovascular disease prevention and management. Cur. Cardiol. Rep. 2017, 19, 104. [Google Scholar] [CrossRef] [PubMed]
- Assies, J.; Mocking, R.J.; Lok, A.; Ruhe, H.G.; Pouwer, F.; Schene, A.H. Effects of oxidative stress on fatty acid- and one-carbon-metabolism in psychiatric and cardiovascular disease comorbidity. Acta Psychiatr. Scand. 2014, 130, 163–180. [Google Scholar] [CrossRef] [PubMed]
- Ventura, E.; Durant, R.; Jaussent, A.; Picot, M.C.; Morena, M.; Badiou, S.; Dupuy, A.M.; Jeandel, C.; Cristol, J.P. Homocysteine and inflammation as main determinants of oxidative stress in the elderly. Free Radic. Biol. Med. 2009, 46, 737–744. [Google Scholar] [CrossRef] [PubMed]
- Lai, W.K.; Kan, M.Y. Homocysteine-induced endothelial dysfunction. Ann. Nutr. Metab. 2015, 67, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Jansen, E.; Beekhof, P.; Tamosiunas, A.; Luksiene, D.; Baceviciene, M. Biomarkers of oxidative stress and redox status in a short-term low-dosed multivitamin and mineral supplementation study in two human age groups. Biogerontology 2015, 16, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Waskiewicz, A.; Sygnowska, E.; Broda, G. Dietary intake of vitamins b6, b12 and folate in relation to homocysteine serum concentration in the adult polish population—Wobasz project. Kardiol. Pol. 2010, 68, 275–282. [Google Scholar] [PubMed]
- Ciaccio, M.; Bellia, C. Hyperhomocysteinemia and cardiovascular risk: Effect of vitamin supplementation in risk reduction. Curr. Clin. Pharmacol. 2010, 5, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Agrawal, B.K.; Varma, M.; Jadhav, A.A. Antioxidant status and smoking habits: Relationship with diet. Singap. Med. J. 2009, 50, 624–627. [Google Scholar]
- Bloomer, R.J. Decreased blood antioxidant capacity and increased lipid peroxidation in young cigarette smokers compared to nonsmokers: Impact of dietary intake. Nutr. J. 2007, 6, 39. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, S. Alcohol and its relation to all-cause and cardiovascular mortality. Acta Cardiol. 2000, 55, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Zabina, H.; Schmid, T.L.; Glasunov, I.; Potemkina, R.; Kamardina, T.; Deev, A.; Konstantinova, S.; Popovich, M. Monitoring behavioral risk factors for cardiovascular disease in Russia. Am. J. Public Health 2001, 91, 1613–1614. [Google Scholar] [CrossRef] [PubMed]
- Margetts, B. Fao/who launch expert report on diet, nutrition and prevention of chronic diseases. Public Health Nutr. 2003, 6, 323–325. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.N.; Moore, S.; Harper, S.B.; Lynch, J.W. Global variability in fruit and vegetable consumption. Am. J. Prev. Med. 2009, 36, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Goryakin, Y.; Rocco, L.; Suhrcke, M.; Roberts, B.; McKee, M. Fruit and vegetable consumption in the former soviet union: The role of individual- and community-level factors. Public Health Nutr. 2015, 18, 2825–2835. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.J.; Gan, R.Y.; Li, S.; Zhou, Y.; Li, A.N.; Xu, D.P.; Li, H.B. Antioxidant phytochemicals for the prevention and treatment of chronic diseases. Molecules 2015, 20, 21138–21156. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K.; Schatzkin, A.; Graubard, B.I.; Schairer, C. A prospective study of diet quality and mortality in women. JAMA 2000, 283, 2109–2115. [Google Scholar] [CrossRef] [PubMed]
- Blokhina, L.V.; Kondakova, N.M.; Pogozheva, A.V.; Baturin, A.K. Multilevel study of actual nutrition in the complex analysis of nutritial status of patients with obesity. Voprosy Pitaniia 2009, 78, 35–39. [Google Scholar] [PubMed]
- Thibeault, D.; Su, H.; MacNamara, E.; Schipper, H.M. Isocratic rapid liquid chromatographic method for simultaneous determination of carotenoids, retinol, and tocopherols in human serum. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2009, 877, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, T.M.; Gao, M. Simplified fluorometric assay of total selenium in plasma and urine. Clin. Chem. 1990, 36, 2124–2126. [Google Scholar] [PubMed]
- Stracke, B.A.; Rufer, C.E.; Bub, A.; Seifert, S.; Weibel, F.P.; Kunz, C.; Watzl, B. No effect of the farming system (organic/conventional) on the bioavailability of apple (malus domestica bork., cultivar golden delicious) polyphenols in healthy men: A comparative study. Eur. J. Nutr. 2010, 49, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Lee, S.H.; Kim, J.E.; Han, K.D.; Kwack, T.E.; Kim, B.S.; Kim, J.E.; Jo, E.B.; Park, Y.K.; Lee, K.S. The association between taking dietary supplements and healthy habits among korean adults: Results from the fifth korea national health and nutritional examination survey (2010–2012). Korean J. Fam. Med. 2016, 37, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Rock, C.L. Multivitamin-multimineral supplements: Who uses them? Am. J. Clin. Nutr. 2007, 85, 277S–279S. [Google Scholar] [PubMed]
- Reinert, A.; Rohrmann, S.; Becker, N.; Linseisen, J. Lifestyle and diet in people using dietary supplements: A german cohort study. Eur. J. Nutr. 2007, 46, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Tetens, I.; Biltoft-Jensen, A.; Spagner, C.; Christensen, T.; Gille, M.B.; Bugel, S.; Banke Rasmussen, L. Intake of micronutrients among Danish adult users and non-users of dietary supplements. Food Nutr. Res. 2011, 55, 7153. [Google Scholar] [CrossRef] [PubMed]
- Getz, G.S.; Reardon, C.A. Nutrition and cardiovascular disease. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 2499–2506. [Google Scholar] [CrossRef] [PubMed]
- Graham, I.; Atar, D.; Borch-Johnsen, K.; Boysen, G.; Burell, G.; Cifkova, R.; Dallongeville, J.; De Backer, G.; Ebrahim, S.; Gjelsvik, B.; et al. European guidelines on cardiovascular disease prevention in clinical practice: Executive summary. Atherosclerosis 2007, 194, 1–45. [Google Scholar] [CrossRef] [PubMed]
- Loria, C.M.; Ingram, D.D.; Feldman, J.J.; Wright, J.D.; Madans, J.H. Serum folate and cardiovascular disease mortality among us men and women. Arch. Intern. Med. 2000, 160, 3258–3262. [Google Scholar] [CrossRef] [PubMed]
- Porter, K.; Hoey, L.; Hughes, C.F.; Ward, M.; McNulty, H. Causes, consequences and public health implications of low b-vitamin status in ageing. Nutrients 2016, 8, 725. [Google Scholar] [CrossRef] [PubMed]
- Barron, E.; Lara, J.; White, M.; Mathers, J.C. Blood-borne biomarkers of mortality risk: Systematic review of cohort studies. PLoS ONE 2015, 10, e0127550. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.S. Folate, homocysteine, and neurological function. Nutr. Clin. Care 2002, 5, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Dong, C.; Yoon, W.; Goldschmidt-Clermont, P.J. DNA methylation and atherosclerosis. J. Nutr. 2002, 132, 2406S–2409S. [Google Scholar] [CrossRef] [PubMed]
- Mattson, M.P.; Shea, T.B. Folate and homocysteine metabolism in neural plasticity and neurodegenerative disorders. Trends Neurosci. 2003, 26, 137–146. [Google Scholar] [CrossRef]
- Tracy, R.P. Emerging relationships of inflammation, cardiovascular disease and chronic diseases of aging. Int. J. Obes. Relat. Metab. Disord. 2003, 27 (Suppl. 3), S29–S34. [Google Scholar] [CrossRef] [PubMed]
- Parnetti, L.; Bottiglieri, T.; Lowenthal, D. Role of homocysteine in age-related vascular and non-vascular diseases. Aging Clin. Exp. Res. 1997, 9, 241–257. [Google Scholar] [CrossRef]
- Beketova, N.A.; Spiricheva, T.V.; Pereverzeva, O.G.; Kosheleva, O.V.; Brzhesinskaia, O.A.; Kharitonchik, L.A.; Kodentsova, V.M.; Spirichev, V.B. The influence of age and sex on fat- and water-soluble vitamins sufficiency of adulthood. Voprosy Pitaniia 2009, 78, 53–59. [Google Scholar] [PubMed]
- McNulty, H.; Pentieva, K.; Hoey, L.; Ward, M. Homocysteine, b-vitamins and cvd. Proc. Nutr. Soc. 2008, 67, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wang, X.; Chen, Z.; Zhang, L.; Zhu, M. Distribution of high-sensitivity c-reactive protein and its relationship with other cardiovascular risk factors in the middle-aged chinese population. Int. J. Environ. Res. Public Health 2016, 13, 872. [Google Scholar] [CrossRef] [PubMed]
- Vu, T.H.; Liu, K.; Lloyd-Jones, D.M.; Stamler, J.; Pirzada, A.; Shah, S.J.; Garside, D.B.; Daviglus, M.L. Favorable levels of all major cardiovascular risk factors at younger ages and high-sensitivity c-reactive protein 39 years later—The Chicago healthy aging study. Prev. Med. Rep. 2015, 2, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Liu, J.; Li, C.; Gao, J.; Li, X.; Chen, S.; Wu, S.; Ding, H.; Fan, H.; Hou, S. Cumulative exposure to high-sensitivity c-reactive protein predicts the risk of cardiovascular disease. J. Am. Heart Assoc. 2017, 6, e005610. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.Y.; Xu, X.; Li, X.C. Cardiovascular diseases: Oxidative damage and antioxidant protection. Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 3091–3096. [Google Scholar] [PubMed]
- Farias, J.G.; Molina, V.M.; Carrasco, R.A.; Zepeda, A.B.; Figueroa, E.; Letelier, P.; Castillo, R.L. Antioxidant therapeutic strategies for cardiovascular conditions associated with oxidative stress. Nutrients 2017, 9, 966. [Google Scholar] [CrossRef] [PubMed]
- Ibarra, M.; Moreno, L.; Vera, R.; Cogolludo, A.; Duarte, J.; Tamargo, J.; Perez-Vizcaino, F. Effects of the flavonoid quercetin and its methylated metabolite isorhamnetin in isolated arteries from spontaneously hypertensive rats. Planta Medica 2003, 69, 995–1000. [Google Scholar] [PubMed]
- Ajay, M.; Achike, F.I.; Mustafa, A.M.; Mustafa, M.R. Effect of quercetin on altered vascular reactivity in aortas isolated from streptozotocin-induced diabetic rats. Diabetes Res. Clin. Pract. 2006, 73, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Williams, R.J.; Spencer, J.P.; Rice-Evans, C. Flavonoids: Antioxidants or signalling molecules? Free Radic. Biol. Med. 2004, 36, 838–849. [Google Scholar] [CrossRef] [PubMed]
- Marunaka, Y.; Marunaka, R.; Sun, H.; Yamamoto, T.; Kanamura, N.; Inui, T.; Taruno, A. Actions of quercetin, a polyphenol, on blood pressure. Molecules 2017, 22, 209. [Google Scholar] [CrossRef] [PubMed]
- Djeffal, A.; Messarah, M.; Boumendjel, A.; Kadeche, L.; Feki, A.E. Protective effects of vitamin c and selenium supplementation on methomyl-induced tissue oxidative stress in adult rats. Toxicol. Ind. Health 2015, 31, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Meng, B.; Gao, W.; Wei, J.; Pu, L.; Tang, Z.; Guo, C. Quercetin increases hepatic homocysteine remethylation and transsulfuration in rats fed a methionine-enriched diet. BioMed Res. Int. 2015, 2015, 815210. [Google Scholar] [CrossRef] [PubMed]
- Paunovic, M.G.; Ognjanovic, B.I.; Matic, M.M.; Stajn, A.S.; Saicic, Z.S. Protective effects of quercetin and vitamin c against nicotine-induced toxicity in the blood of wistar rats. Arhiv za Higijenu Rada i Toksikologiju 2016, 67, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Kunutsor, S.K.; Apekey, T.A.; Khan, H. Liver enzymes and risk of cardiovascular disease in the general population: A meta-analysis of prospective cohort studies. Atherosclerosis 2014, 236, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Strasak, A.M.; Kelleher, C.C.; Klenk, J.; Brant, L.J.; Ruttmann, E.; Rapp, K.; Concin, H.; Diem, G.; Pfeiffer, K.P.; Ulmer, H.; et al. Longitudinal change in serum gamma-glutamyltransferase and cardiovascular disease mortality: A prospective population-based study in 76,113 austrian adults. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 1857–1865. [Google Scholar] [CrossRef] [PubMed]
- Sesso, H.D.; Christen, W.G.; Bubes, V.; Smith, J.P.; MacFadyen, J.; Schvartz, M.; Manson, J.E.; Glynn, R.J.; Buring, J.E.; Gaziano, J.M. Multivitamins in the prevention of cardiovascular disease in men: The physicians’ health study ii randomized controlled trial. JAMA 2012, 308, 1751–1760. [Google Scholar] [CrossRef] [PubMed]
- Hercberg, S.; Galan, P.; Preziosi, P.; Bertrais, S.; Mennen, L.; Malvy, D.; Roussel, A.M.; Favier, A.; Briancon, S. The su.Vi.Max study: A randomized, placebo-controlled trial of the health effects of antioxidant vitamins and minerals. Arch. Intern. Med. 2004, 164, 2335–2342. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.L.; Fakhouri, T.H.; Park, Y.; Dwyer, J.T.; Thomas, P.R.; Gahche, J.J.; Miller, P.E.; Dodd, K.W.; Sempos, C.T.; Murray, D.M. Multivitamin-mineral use is associated with reduced risk of cardiovascular disease mortality among women in the united states. J. Nutr. 2015, 145, 572–578. [Google Scholar] [CrossRef] [PubMed]
- Rautiainen, S.; Akesson, A.; Levitan, E.B.; Morgenstern, R.; Mittleman, M.A.; Wolk, A. Multivitamin use and the risk of myocardial infarction: A population-based cohort of Swedish women. Am. J. Clin. Nutr. 2010, 92, 1251–1256. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion Criteria: |
| Generally healthy men and women aged from 40 to 70 years of age preferable smokers and who regularly consumes alcohol, and consuming fewer than 12 items found on the Recommended Foods Checklist (see below) per week. |
| Individual should be judged to be in good general health based on an interview and abbreviated physical exam. |
| Individual understands the procedures and agrees to participate in the study. |
| Individual is able and willing to provide written informed consent and confidentiality agreement. |
| Exclusion Criteria: |
| Use of dietary supplements within one week of Day 1. Supplements include any vitamins, minerals, and herbal products, including herbal drinks. |
| Presence of cardiovascular disease, hypercholesterolemia, cancer, diabetes mellitus, or any other chronic health condition identified from the findings of the interview. |
| Currently treated for uncontrolled hypertension or blood pressure greater >140 mm Hg systolic or >90 mm Hg diastolic during seated, resting measurement on two consecutive occasions during visit 1. |
| Therapeutic uses of coumadin, aspirin, or other medications that influence hemostasis within four weeks of Day 1. |
| Participation in another clinical trial within 30 days of enrollment into the study. |
| History or current abuse of drugs or alcohol, or intake >4 alcoholic beverages per day. |
| Known hypersensitivity to study product or any ingredient in study product. |
| A change in hormone therapy, including oral contraceptives, within 4 weeks prior to screening, or unwilling to maintain current hormone therapy/oral contraceptive use throughout the course of the study. |
| Pregnant or lactating women, or pre-menopausal women not using a medically approved form of birth control. |
| Any condition that the Principal Investigators believe may put the subject at undue risk. |
| Study Measurements | Office Visit 1 | Office Visit 2 | Office Visit 3 | Office Visit 4 | Office Visit 5 | Office Visit 6 | Phone Interview |
|---|---|---|---|---|---|---|---|
| Day 0 | Day 1 | Day 14 | Day 28 | Day 42 | Day 56 | Day 57–60 | |
| Informed Consent | X | ||||||
| Pregnancy test (urine) | X | ||||||
| Recommended Foods Checklist | X | X | |||||
| Physical Exam | X | X | |||||
| Medical History, Family Medical History, Dietary Behavior and Lifestyle Questionnaires | X | X | |||||
| Food Frequency Questionnaire | X | X | |||||
| Blood lipid profile determination | X | X | |||||
| Blood concentrations of selected nutrients determined | X | X | X | ||||
| Biomarkers of Heart health risk determined | X | X | |||||
| Safety measurements (Serum Chemistry Panel, Hematology, and Urinalysis) | X | ||||||
| Adverse Events Questionnaire | X | X | X | X | X | X | |
| Inform subject’s eligibility | X | ||||||
| Follow-up as Good Clinical Practice | X | ||||||
| Dispense the product | X | X | |||||
| Collect the product | X | X | X | X |
| Variable | PLA Group (n = 60) | VMP Group (n = 60) | p-Value |
|---|---|---|---|
| Male/Female (n) | 9/51 | 12/48 | 0.630 |
| Age (year) | 48.9 ± 7.6 | 49.5 ± 7.6 | 0.660 |
| Smokers, (n) (%) | 14 (23%) | 16 (27%) | 0.830 |
| Alcohol consumers, (n) (%) | 39 (65%) | 30 (50%) | 0.140 |
| Physically active, (n) (%) | 26 (43%) | 22 (36%) | 0.580 |
| Anthropomorphic Measurement | |||
| Weight (kg) | 74.27 ± 15.94 | 75.72 ± 15.47 | 0.615 |
| BMI (kg/m2) | 26.58 ± 5.72 | 26.89 ± 4.92 | 0.739 |
| Waist/Hip ratio | 0.87 ± 0.13 | 0.88 ± 0.15 | 0.516 |
| Systolic blood pressure (mmHg) | 116.30 ± 9.05 | 117.83 ± 9.76 | 0.374 |
| Diastolic blood pressure (mmHg) | 75.08 ± 8.49 | 75.58 ± 6.89 | 0.724 |
| Heart Health Biomarkers | |||
| Homocysteine (µmol/L) | 15.98 ± 6.62 | 18.55 ± 10.53 | 0.112 |
| hs-CRP (ng/mL) | 1922 ± 1937 | 2551 ± 2594 | 0.135 |
| Oxidized LDL (ng/mL) | 3939 ± 4109 | 3546 ± 3011 | 0.552 |
| GGT (U/L) | 22.41 ± 12.62 | 26.18 ± 18.71 | 0.199 |
| Uric acid (µmol/L) | 236 ± 83 | 241 ± 68 | 0.725 |
| Total Cholesterol (mmol/L) | 5.13 ± 0.93 | 5.10 ± 1.02 | 0.863 |
| HDL cholesterol (mmol/L) | 1.61 ± 0.46 | 1.57 ± 0.41 | 0.571 |
| LDL cholesterol (mmol/L) | 3.37 ± 0.76 | 3.29 ± 0.80 | 0.590 |
| Triglycerides (mmol/L) | 1.04 ± 0.58 | 1.06 ± 0.66 | 0.818 |
| Variable | PLA Group | VMP Group | p-Value |
|---|---|---|---|
| RFS | 8.8 ± 1.3 | 8.8 ± 1.3 | 0.943 |
| Calories (kcal/day) | 2449 ± 759 | 2481 ± 828 | 0.825 |
| Protein (g/day) | 87 ± 31 | 85 ± 37 | 0.712 |
| Carbohydrate (g/day) | 220 ± 100 | 244 ± 130 | 0.252 |
| Sugar (g/day) | 64 ± 52 | 74 ± 69 | 0.352 |
| Fat (g/day) | 117 ± 44 | 117 ± 47 | 0.999 |
| Saturated fat (g/day) | 39 ± 16 | 39 ± 14 | 0.842 |
| Polyunsaturated fat (g/day) | 28 ± 15 | 27 ± 15 | 0.800 |
| ω-6 (g/day) | 25 ± 14 | 25 ± 14 | 0.936 |
| ω-3 (g/day) | 3.2 ± 1.5 | 3.0 ± 1.6 | 0.544 |
| Cholesterol (mg/day) | 266 ± 137 | 281 ± 208 | 0.636 |
| Na (mg/day) | 3888 ± 1532 | 3805 ± 1660 | 0.777 |
| K (mg/day) | 3643 ± 1709 | 3515 ± 1691 | 0.682 |
| Ca (mg/day) | 1137 ± 480 | 1147 ± 515 | 0.913 |
| P (mg/day) | 1520 ± 496 | 1512 ± 575 | 0.929 |
| Mg (mg/day) | 378 ± 144 | 378 ± 167 | 0.986 |
| Fe (mg/day) | 17.8 ± 8.6 | 17.61 ± 9.77 | 0.893 |
| Vit A (mg/day) | 0.34 ± 0.24 | 0.42 ± 0.24 | 0.090 |
| Vit B1 (mg/day) | 1.03 ± 0.42 | 1.06 ± 0.55 | 0.720 |
| Vit B2 (mg/day) | 1.57 ± 0.56 | 1.61 ± 0.70 | 0.736 |
| Niacin (mg/day) | 15.0 ± 6.8 | 14.7 ± 7.4 | 0.821 |
| Vit C (mg/day) | 191 ± 147 | 187 ± 137 | 0.874 |
| Blood Nutrients | |||
| β-Carotene (µg/dL) | 138 ± 66 | 133 ± 54 | 0.662 |
| Total tocopherols (mg/dL) | 1.88 ± 0.43 | 1.87 ± 0.48 | 0.872 |
| Vit C (mg/dL) | 11.76 ± 8.68 | 9.66 ± 8.07 | 0.173 |
| RBC Folate (µg/L) | 7.24 ± 2.98 | 7.10 ± 3.04 | 0.798 |
| Vit B6 (µg/L) | 12.7 ± 5.1 | 11.6 ± 5.2 | 0.277 |
| Vit B12 (ng/mL) | 332 ± 174 | 339 ± 215 | 0.848 |
| Selenium (µg/L) | 96.2 ± 9.3 | 98.6 ± 9.1 | 0.158 |
| Zinc (µmol/L) | 15.0 ± 3.0 | 15.7 ± 2.9 | 0.159 |
| Magnesium (mmol/L) | 15.0 ± 8.7 | 15.0 ± 8.7 | 0.786 |
| Quercetin (ng/mL) | 13.9 ± 7.0 | 13.4 ± 8.0 | 0.727 |
| Blood Nutrients | Intervention Period | PLA Group | VMP Group | p-Value ‡ |
|---|---|---|---|---|
| β-Carotene (µg/dL) | Day 1–Day 28 | 11.02 ± 41.44 * | 6.90 ± 51.87 | 0.684 |
| Day 1–Day 56 | 0.00 ± 54.70 | 0.24 ± 56.07 | 0.491 | |
| Total tocopherol (mg/dL) | Day 1–Day 28 | −0.07 ± 0.53 | 0.06 ± 0.63 | 0.112 |
| Day 1–Day 56 | −0.06 ± 0.55 | −0.01 ± 0.57 | 0.324 | |
| Vit C (mg/dL) | Day 1–Day 28 | 0.36 ± 10.28 | −0.99 ± 8.76 | 0.780 |
| Day 1–Day 56 | 2.97 ± 9.09 | 8.21 ± 9.27 | 0.001 | |
| RBC Folate (µg/L) | Day 1–Day 28 | 0.71 ± 5.86 | 3.40 ± 5.88 * | 0.007 |
| Day 1–Day 56 | −0.23 ± 6.01 | 3.20 ± 7.18 | 0.003 | |
| Vit B6 (µg/L) | Day 1–Day 28 | −4.58 ± 6.48 * | −0.02 ± 7.26 | 0.0002 |
| Day 1–Day 56 | −6.83 ± 7.58 * | −2.46 ± 7.87 | 0.001 | |
| Vit B12 (ng/mL) | Day 1–Day 28 | −90 ± 193 * | −87 ± 227 * | 0.470 |
| Day 1–Day 56 | −84 ± 206 * | −39 ± 239 | 0.136 | |
| Zinc (µmol/L) | Day 1–Day 28 | 0.49 ± 2.70 | −0.45 ± 2.30 | 0.978 |
| Day 1–Day 56 | −0.11 ± 2.96 | −0.72 ± 2.84 | 0.872 | |
| Selenium (µg/L) | Day 1–Day 28 | 1.60 ± 9.07 | 1.30 ± 8.18 | 0.575 |
| Day 1–Day 56 | 1.23 ± 7.99 | −0.40 ± 10.09 | 0.836 | |
| Quercetin (ng/mL) | Day 1–Day 56 | −0.08 ± 9.45 | 4.28 ± 8.58 * | 0.005 |
| Heart Health Biomarkers | PLA Group | VMP Group | p-Value ‡ |
|---|---|---|---|
| Hcy (µmol/L) | −0.82 ± 8.16 | −3.97 ± 10.09 * | 0.031 |
| hs-CRP (ng/mL) | 515 ± 2642 | 134 ± 3507 | 0.251 |
| Oxidized LDL (ng/mL) | 1821 ± 4172 * | 1907 ± 4264 * | 0.544 |
| GGT (U/L) | 1.99 ± 9.86 | −1.68 ± 14.53 * | 0.054 |
| Uric acid (µmol/L) | 2.45 ± 50.37 | −7.52 ± 62.20 | 0.168 |
| Total cholesterol (mmol/L) | −0.18 ± 0.93 | −0.16 ± 0.82 | 0.563 |
| HDL cholesterol (mmol/L) | −0.08 ± 0.34 | −0.04 ± 0.33 | 0.232 |
| LDL cholesterol (mmol/L) | −0.17 ± 0.79 | −0.12 ± 0.76 | 0.625 |
| Triglycerides (mmol/L) | 0.10 ± 0.42 | 0.02 ± 0.44 | 0.159 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isakov, V.A.; Bogdanova, A.A.; Bessonov, V.V.; Sentsova, T.B.; Tutelyan, V.A.; Lin, Y.; Kazlova, V.; Hong, J.; Velliquette, R.A. Effects of Multivitamin, Multimineral and Phytonutrient Supplementation on Nutrient Status and Biomarkers of Heart Health Risk in a Russian Population: A Randomized, Double Blind, Placebo Controlled Study. Nutrients 2018, 10, 120. https://doi.org/10.3390/nu10020120
Isakov VA, Bogdanova AA, Bessonov VV, Sentsova TB, Tutelyan VA, Lin Y, Kazlova V, Hong J, Velliquette RA. Effects of Multivitamin, Multimineral and Phytonutrient Supplementation on Nutrient Status and Biomarkers of Heart Health Risk in a Russian Population: A Randomized, Double Blind, Placebo Controlled Study. Nutrients. 2018; 10(2):120. https://doi.org/10.3390/nu10020120
Chicago/Turabian StyleIsakov, Vasily A., Alexandra A. Bogdanova, Vladimir V. Bessonov, Tatiana B. Sentsova, Victor A. Tutelyan, Yumei Lin, Valentina Kazlova, Jina Hong, and Rodney A. Velliquette. 2018. "Effects of Multivitamin, Multimineral and Phytonutrient Supplementation on Nutrient Status and Biomarkers of Heart Health Risk in a Russian Population: A Randomized, Double Blind, Placebo Controlled Study" Nutrients 10, no. 2: 120. https://doi.org/10.3390/nu10020120
APA StyleIsakov, V. A., Bogdanova, A. A., Bessonov, V. V., Sentsova, T. B., Tutelyan, V. A., Lin, Y., Kazlova, V., Hong, J., & Velliquette, R. A. (2018). Effects of Multivitamin, Multimineral and Phytonutrient Supplementation on Nutrient Status and Biomarkers of Heart Health Risk in a Russian Population: A Randomized, Double Blind, Placebo Controlled Study. Nutrients, 10(2), 120. https://doi.org/10.3390/nu10020120