Nutrition and Liver Disease


{kind=link}
{kind=link}
Abstract
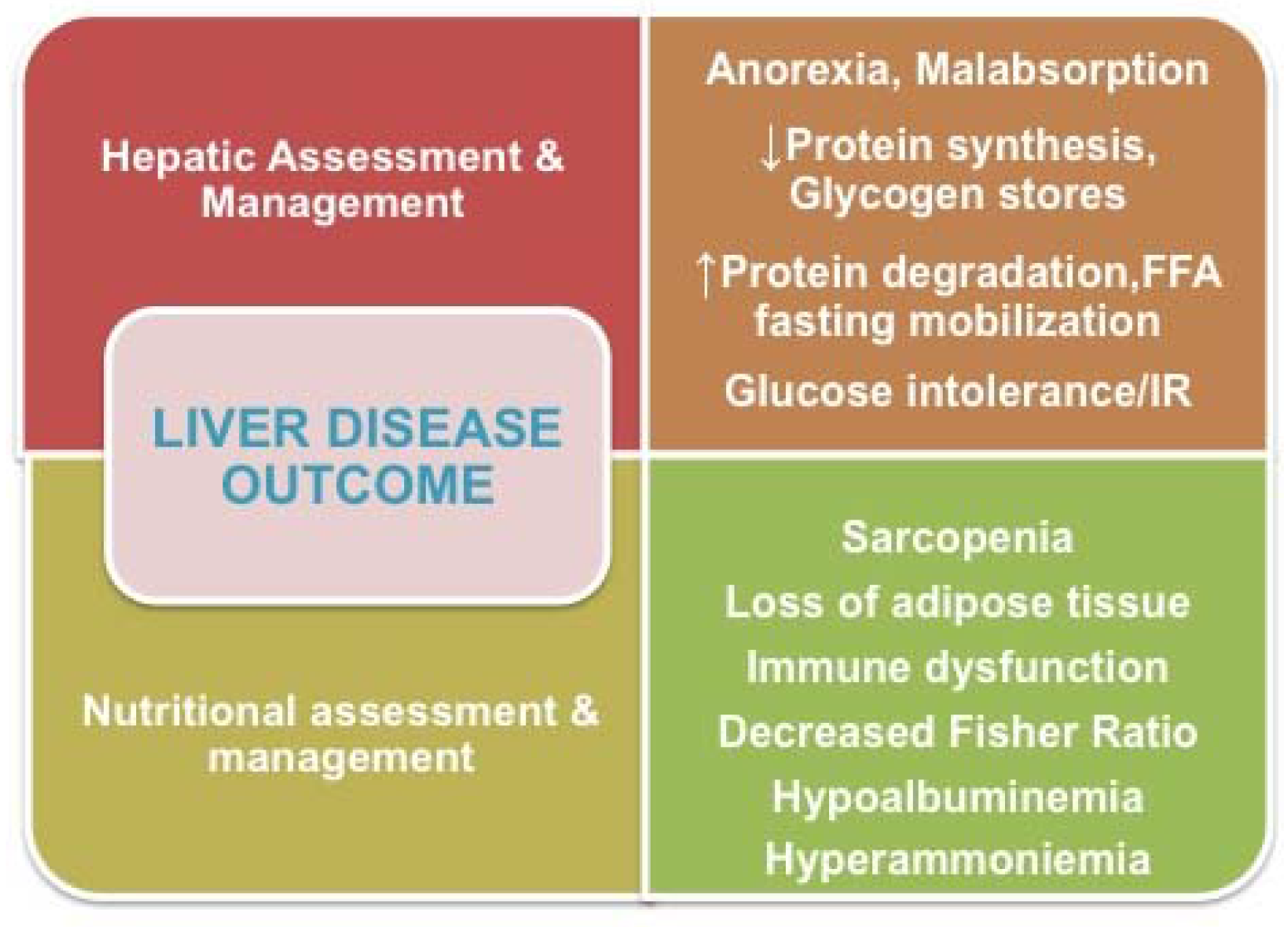
1. Skeletal Muscle Mass
- Strict interdependence exists between (1) the prevention of depletion of SMM,(2) the early diagnosis of and curative therapy for hepatocellular carcinoma (HCC),(3) the preservation of liver functional reserve, and (4) improved liver disease outcomes [1]. Age of male patients, female gender, a Child–Pugh score, and increased tumor size were significantly related to the SMM index, as measured at the third lumbar vertebra by transverse computed tomography (CT) imaging, which is a commonly used tool for HCC in the clinical setting. The results of the study by Imai et al. overall confirmed that sarcopenia negatively impacts the survival of patients with HCC, and is a valuable prognostic factor that might be impacted by liver functional reserve and the clinical stage of HCC.
- Therelationship between the loss of SMM, as assessed by bioelectric impedance analysis (BIA), and liver fibrosis, as measured by virtual-touch-quantification (VTQ) and acoustic-radiation-force-impulse elastography in patients with chronic liver disease (CLD), was reported by Nishikawa et al. [2]. Interestingly, BCAAs-to-tyrosine ratio (BTR) showed the second strongest correlation with the VTQ level, and was an independent predictor for decreased SMM index.
- BothBTR and SMM, as evaluated by BIA, were also confirmed to be reliable predictors of outcome in patients with liver diseases in another study, which found that increased values of BTR and SMM were associated with the resolution of chronic hepatitis C in patients treated with interferon-free direct-acting-antiviral therapy [3].
- However, all that glitters is not gold, and these studies have both strengths and limitations. The study by Imai et al. [1] was based on imaging techniques, and, although these assessments are objective and not affected by defects in hepatic synthesis or retention of NaCl and water, they are either expensive or involve radiation and cannot easily be repeated to monitor progress. The other twostudies [2,3] that used BIA, which is based on a two-component model of body composition (fat and fat-free mass), may have drawbacks. As recently emphasized by Amodio et al. [4] the validity of this technique is in fact critically dependent on assumptions relating to tissue density and hydration.
2. Nutritional Assessment and Support
- The first article [8] recommends the performance of an accurate multidisciplinary assessment of malnutrition in order to optimize nutritional support, especially for those patients with elevated risk for malnutrition because of the severity of their native liver disease. The recommended daily requirements for nutrients and energy intake should be achieved through oral intake, oral supplementation, and enteral nutrition. Parenteral nutrition (PN) should be used for moderately or severely malnourished patients with cirrhosis who cannot be fed orally or enterally, or if they have fasted longer than 72 h [9].
- The important and difficult issues concerned with the careful assessment of nutritional status of patients who are candidates for liver transplantation were also emphasized in the articles by Ahmed Hammad et al. [10] and Yang et al. [11]. The perioperative nutritional interventions, including the use of synbiotics, micronutrients, branched-chain amino acid (BCAA) supplements, and immunonutrients; fluid and electrolyte balance, the partial substitution of conventional fats with medium-chain triglycerides, and carefully monitored supplementation using fat soluble vitamins for cholestasis were reviewed for both adult and pediatric patients. Children with chronic liver disease are particularly vulnerable to malnutrition, which can compromise growth and brain development. They should benefit from early intervention provided by a multidisciplinary team. Yang et al. in particular have focused on the nutritional needs and support of children with chronic liver disease [11]; they revised the issues by providing conclusions that are consistent with the most recent guidelines of the European Society of Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) [12].
3. Hepatopathies due to Inherited Metabolic/Genetic Defects
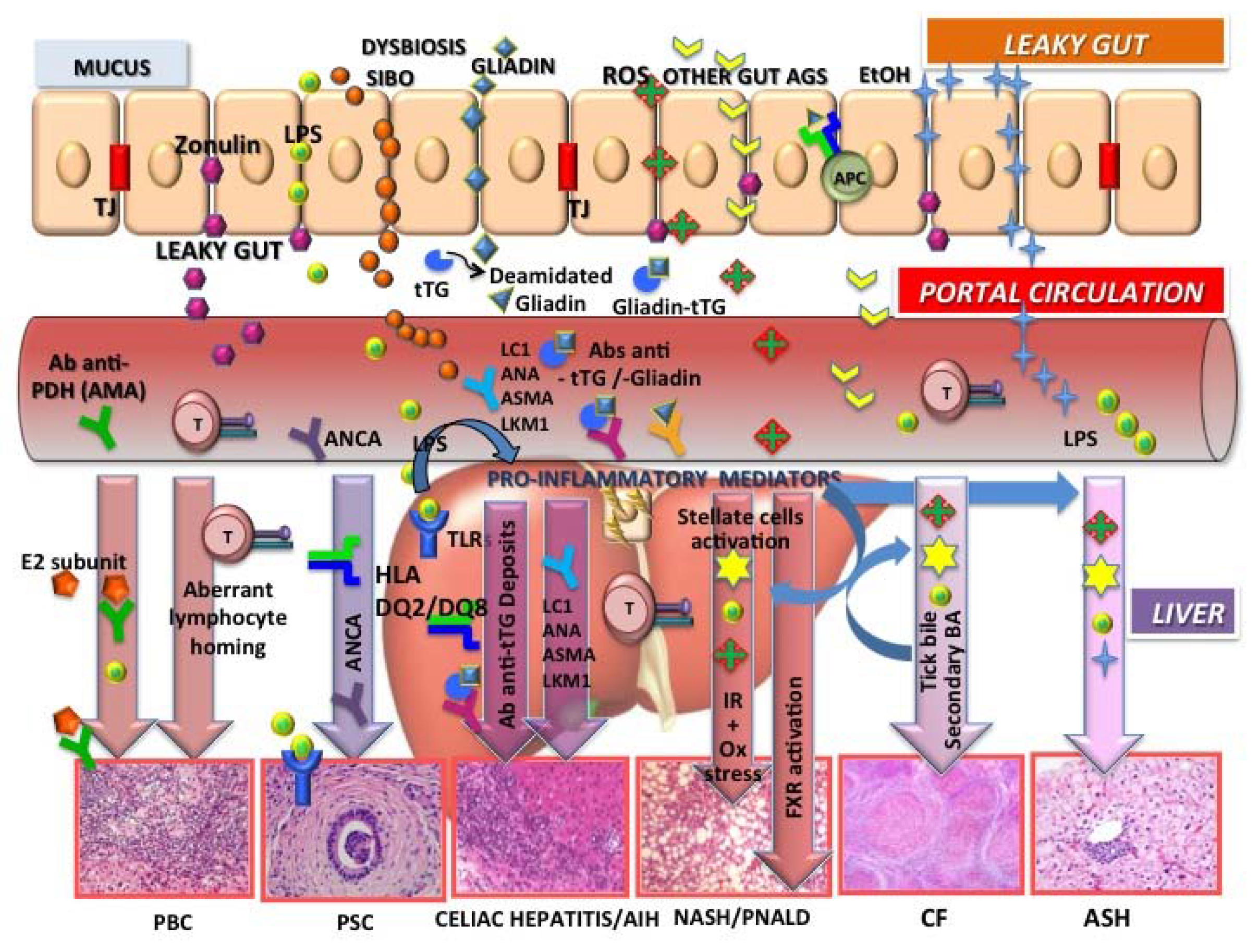
4. Hepatopathies Driven by Primary Nutritional/Intestinal Tract Diseases
- In this issue of Nutrients, Cahova et al. [28] reviewed studies of animal models and humans that suggested that chronic parenteral nutrition-related liver damage depends on intestinal failure and associated complications rather than PN administration per se. The prominent factors appear to be increased permeability of the intestinal barrier, which facilitates translocation of bacterial toxins and microorganisms into the portal circulation, mesenteric lymph nodes, and liver, and the overall proinflammatory status of the compromised intestine. The gut microbiota play a weighty role in the maintenance of the functional intestinal barrier and the establishment of either an immunotolerant or inflammatory intestinal setting [23,27]. Therapeutic strategies that focus on improving the composition of the microbiota through the targeted delivery of beneficial microbiota or by supplementation with immunomodulators are attractive areas of investigation.
- Alcoholic liver disease (ALD) is a strong predictor of malnutrition because of the numerous risk factors for malnutrition that are associated with both acute and chronic alcohol abuse. Due to complicated pathogenetic mechanisms, therapies for ALD and especially for severe alcoholic hepatitis (AH) are thorny problems in clinical practice. For severe acute AH, specific drug treatments, including glucorticoids and pentoxifylline, have been identified and currently are recommended by international guidelines. However, further elucidation of the mechanisms of pathogenesis is still needed [29]. In this context, the article by Xuchong Tang et al. [30] in this issue of Nutrients is particularly welcome. The study revealed that an artichoke extract exhibited significant preventive hepatoprotective effects not only for the carbon-tetrachloride-induced hepatoxicity [31,32] and NAFLD/NASH [33] as previously demonstrated but also against acute alcohol-induced liver injury (ASH). The effects probably depend on the ability of components of the extract not only to attenuate oxidative stress but also to suppress the toll-like receptor 4/nuclear factor kappa-light-chain-enhancer of activated Bcells (TLR4/NFkB) inflammatory pathway, a signaling pathway suggested to be one of the mechanisms of pathogenesis also of NAFLD through the overexpression of hepcidin [34].
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Imai, K.; Takai, K.; Watanabe, S.; Hanai, T.; Suetsugu, A.; Shiraki, M.; Shimizu, M. Sarcopenia Impairs Prognosis of Patients with Hepatocellular Carcinoma: The Role of Liver Functional Reserve and Tumor-Related Factors in Loss of Skeletal Muscle. Nutrients 2017, 9, 1054. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Nishimura, T.; Enomoto, H.; Iwata, Y.; Ishii, A.; Miyamoto, Y.; Ishii, N.; Yuri, Y.; Takata, R.; Hasegawa, K.; et al. Impact of Virtual Touch Quantification in Acoustic Radiation Force Impulse for Skeletal Muscle Mass Loss in Chronic Liver Diseases. Nutrients 2017, 9, 620. [Google Scholar] [CrossRef] [PubMed]
- Yoh, K.; Nishikawa, H.; Enomoto, H.; Ishii, A.; Iwata, Y.; Miyamoto, Y.; Ishii, N.; Yuri, Y.; Hasegawa, K.; Nakano, C.; et al. Predictors Associated with Increase in Skeletal Muscle Mass after Sustained Virological Response in Chronic Hepatitis C Treated with Direct Acting Antivirals. Nutrients 2017, 9, 1135. [Google Scholar] [CrossRef] [PubMed]
- Amodio, P.; Bemeur, C.; Butterworth, R.; Cordoba, J.; Kato, A.; Montagnese, S.; Uribe, M.; Vilstrup, H.; Morgan, M.Y. The nutritional management of hepatic encephalopathy in patients with cirrhosis: International Society for Hepatic Encephalopathy and Nitrogen Metabolism Consensus. Hepatology 2013, 58, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Lopez-Jaramillo, P.; Avezum, A., Jr.; Orlandini, A.; Seron, P.; Ahmed, S.H.; Rosengren, A.; Kelishadi, R.; et al. Prognostic value of grip strength: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015, 386, 266–273. [Google Scholar] [CrossRef]
- Huisman, E.J.; Trip, E.J.; Siersema, P.D.; van Hoek, B.; van Erpecum, K.J. Protein energy malnutrition predicts complications in liver cirrhosis. Eur. J. Gastroenterol. Hepatol. 2011, 23, 982–989. [Google Scholar] [CrossRef] [PubMed]
- Dasarathy, S. Consilience in sarcopenia of cirrhosis. J. Cachexia Sarcopenia Muscle 2012, 3, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Perumpail, B.J.; Li, A.A.; Cholankeril, G.; Kumari, R.; Ahmed, A. Optimizing the Nutritional Support of Adult Patients in the Setting of Cirrhosis. Nutrients 2017, 9, 1114. [Google Scholar] [CrossRef] [PubMed]
- Plauth, M.; Cabré, E.; Campillo, B.; Kondrup, J.; Marchesini, G.; Schütz, T.; Shenkin, A.; Wendon, J.; ESPEN. ESPEN Guidelines on Parenteral Nutrition: Hepatology. Clin. Nutr. 2009, 28, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Hammad, A.; Kaido, T.; Aliyev, V.; Mandato, C.; Uemoto, S. Nutritional Therapy in Liver Transplantation. Nutrients 2017, 9, 1126. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.H.; Perumpail, B.J.; Yoo, E.R.; Ahmed, A.; Kerner, J.A., Jr. Nutritional Needs and Support for Children with Chronic Liver Disease. Nutrients 2017, 9, 1127. [Google Scholar] [CrossRef] [PubMed]
- McLin, V.A.; Allen, U.; Boyer, O.; Bucuvalas, J.; Colledan, M.; Cuturi, M.C.; d’Antiga, L.; Debray, D.; Dezsofi, A.; Goyet, J.V.; et al. Early and Late Factors Impacting Patient and Graft Outcome in Pediatric Liver Transplantation: Summary of an ESPGHAN Monothematic Conference. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Guercio Nuzio, S.; Ann Tizzard, S.; Vajro, P. Tips and hints for the transition: What adult hepatologists should know when accept teens with a pediatric hepatobiliary disease. Clin. Res. Hepatol. Gastroenterol. 2014, 38, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Thompson, R.J.; Azevedo, R.A.; Galoppo, C.; Lewindon, P.; McKiernan, P. Cholestatic and metabolic liver diseases: Working Group report of the second World Congress of Pediatric Gastroenterology, Hepatology, and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2004, 39, 611–615. [Google Scholar] [CrossRef]
- Péanne, R.; de Lonlay, P.; Foulquier, F.; Kornak, U.; Lefeber, D.J.; Morava, E.; Pérez, B.; Seta, N.; Thiel, C.; Van Schaftingen, E.; et al. Congenital disorders of glycosylation (CDG): Quo vadis? Eur. J. Med. Genet. 2017. [Google Scholar] [CrossRef]
- Witters, P.; Cassiman, D.; Morava, E. Nutritional Therapies in Congenital Disorders of Glycosylation (CDG). Nutrients 2017, 9, 1222. [Google Scholar] [CrossRef] [PubMed]
- Morelle, W.; Potelle, S.; Witters, P.; Wong, S.; Climer, L.; Lupashin, V.; Matthijs, G.; Gadomski, T.; Jaeken, J.; Cassiman, D.; et al. Galactose supplementation in patients with tmem165-CDG rescues the glycosylation defects. J. Clin. Endocrinol. Metab. 2017, 102, 1375–1386. [Google Scholar] [CrossRef] [PubMed]
- Morava, E. Galactose supplementation in phosphoglucomutase-1 deficiency; review and outlook for a novel treatable CDG. Mol. Genet. Metab. 2014, 112, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.Y.; Gadomski, T.; van Scherpenzeel, M.; Honzik, T.; Hansikova, H.; Holmefjord, K.S.B.; Mork, M.; Bowling, F.; Sykut-Cegielska, J.; Koch, D.; et al. Oral D-galactose supplementation in PGM1-CDG. Genet. Med. 2017, 19, 1226–1235. [Google Scholar] [CrossRef] [PubMed]
- Poeta, M.; Pierri, L.; Vajro, P. Gut-Liver Axis Derangement in Non-Alcoholic Fatty Liver Disease. Children 2017, 4, 66. [Google Scholar] [CrossRef] [PubMed]
- Troisi, J.; Pierri, L.; Landolfi, A.; Marciano, F.; Bisogno, A.; Belmonte, F.; Palladino, C.; Guercio Nuzio, S.; Campiglia, P.; Vajro, P. Urinary Metabolomics in Pediatric Obesity and NAFLD Identifies Metabolic Pathways/Metabolites Related to Dietary Habits and Gut-Liver Axis Perturbations. Nutrients 2017, 9, 485. [Google Scholar] [CrossRef] [PubMed]
- Marciano, F.; Savoia, M.; Vajro, P. Celiac disease-related hepatic injury: Insights into associated conditions and underlying pathomechanisms. Dig. Liver Dis. 2016, 48, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Vajro, P.; Paolella, G.; Fasano, A. Microbiota and gut-liver axis: Their influences on obesity and obesity-related liver disease. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Zhou, Q.; Li, H. Gut Microbiota and Nonalcoholic Fatty Liver Disease: Insights on Mechanisms and Therapy. Nutrients 2017, 9, 1124. [Google Scholar] [CrossRef] [PubMed]
- Vavricka, S.R.; Schoepfer, A.; Scharl, M.; Lakatos, P.L.; Navarini, A.; Rogler, G. Extraintestinal Manifestations of Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2015, 21, 1982–1992. [Google Scholar] [CrossRef] [PubMed]
- Debray, D.; Narkewicz, M.R.; Bodewes, F.A.J.A.; Colombo, C.; Housset, C.; de Jonge, H.R.; Jonker, J.W.; Kelly, D.A.; Ling, S.C.; Poynard, T.; et al. Cystic Fibrosis–related Liver Disease: Research Challenges and Future Perspectives. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Orso, G.; Mandato, C.; Veropalumbo, C.; Cecchi, N.; Garzi, A.; Vajro, P. Pediatric parenteral nutrition-associated liver disease and cholestasis: Novel advances in pathomechanisms-based prevention and treatment. Dig. Liver Dis. 2016, 48, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Cahova, M.; Bratova, M.; Wohl, P. Parenteral Nutrition-Associated Liver Disease: The Role of the Gut Microbiota. Nutrients 2017, 9, 987. [Google Scholar] [CrossRef] [PubMed]
- Abenavoli, L.; Masarone, M.; Federico, A.; Rosato, V.; Dallio, M.; Loguercio, C.; Persico, M. Alcoholic Hepatitis: Pathogenesis, Diagnosis and Treatment. Rev. Recent. Clin. Trials. 2016, 11, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Wei, R.; Deng, A.; Lei, T. Protective Effects of Ethanolic Extracts from Artichoke, an Edible Herbal Medicine, against Acute Alcohol-Induced Liver Injury in Mice. Nutrients 2017, 9, 1000. [Google Scholar] [CrossRef] [PubMed]
- Colak, E.; Ustuner, M.C.; Tekin, N.; Colak, E.; Burukoglu, D.; Degirmenci, I.; Gunes, H.V. The hepatocurative effects of Cynara scolymus L. leaf extract on carbon tetrachloride-induced oxidative stress and hepatic injury in rats. Springerplus 2016, 5, 216. [Google Scholar] [CrossRef] [PubMed]
- Mehmetçik, G.; Ozdemirler, G.; Koçak-Toker, N.; Cevikbaş, U.; Uysal, M. Effect of pretreatment with artichoke extract on carbon tetrachloride-induced liver injury and oxidative stress. Exp. Toxicol. Pathol. 2008, 60, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Rangboo, V.; Noroozi, M.; Zavoshy, R.; Rezadoost, S.A.; Mohammadpoorasl, A. The Effect of Artichoke Leaf Extract on Alanine Aminotransferase and Aspartate Aminotransferase in the Patients with Nonalcoholic Steatohepatitis. Int. J. Hepatol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Wang, X.; Huang, L.; Liu, B. Hepcidin in non-alcoholic fatty liver disease regulated by the TLR4/NF-κB signaling pathway. Exp. Ther. Med. 2016, 11, 73–76. [Google Scholar] [CrossRef] [PubMed]


© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mandato, C.; Di Nuzzi, A.; Vajro, P. Nutrition and Liver Disease. Nutrients 2018, 10, 9. https://doi.org/10.3390/nu10010009
Mandato C, Di Nuzzi A, Vajro P. Nutrition and Liver Disease. Nutrients. 2018; 10(1):9. https://doi.org/10.3390/nu10010009
Chicago/Turabian StyleMandato, Claudia, Antonella Di Nuzzi, and Pietro Vajro. 2018. "Nutrition and Liver Disease" Nutrients 10, no. 1: 9. https://doi.org/10.3390/nu10010009
APA StyleMandato, C., Di Nuzzi, A., & Vajro, P. (2018). Nutrition and Liver Disease. Nutrients, 10(1), 9. https://doi.org/10.3390/nu10010009