
Sustainable Healthcare Plastic Products: Application of the Transition Engineering Design Approach Yields a Novel Concept for Circularity and Sustainability



Abstract
1. Introduction
1.1. Background and Motivation
1.2. Research Gap and Research Question
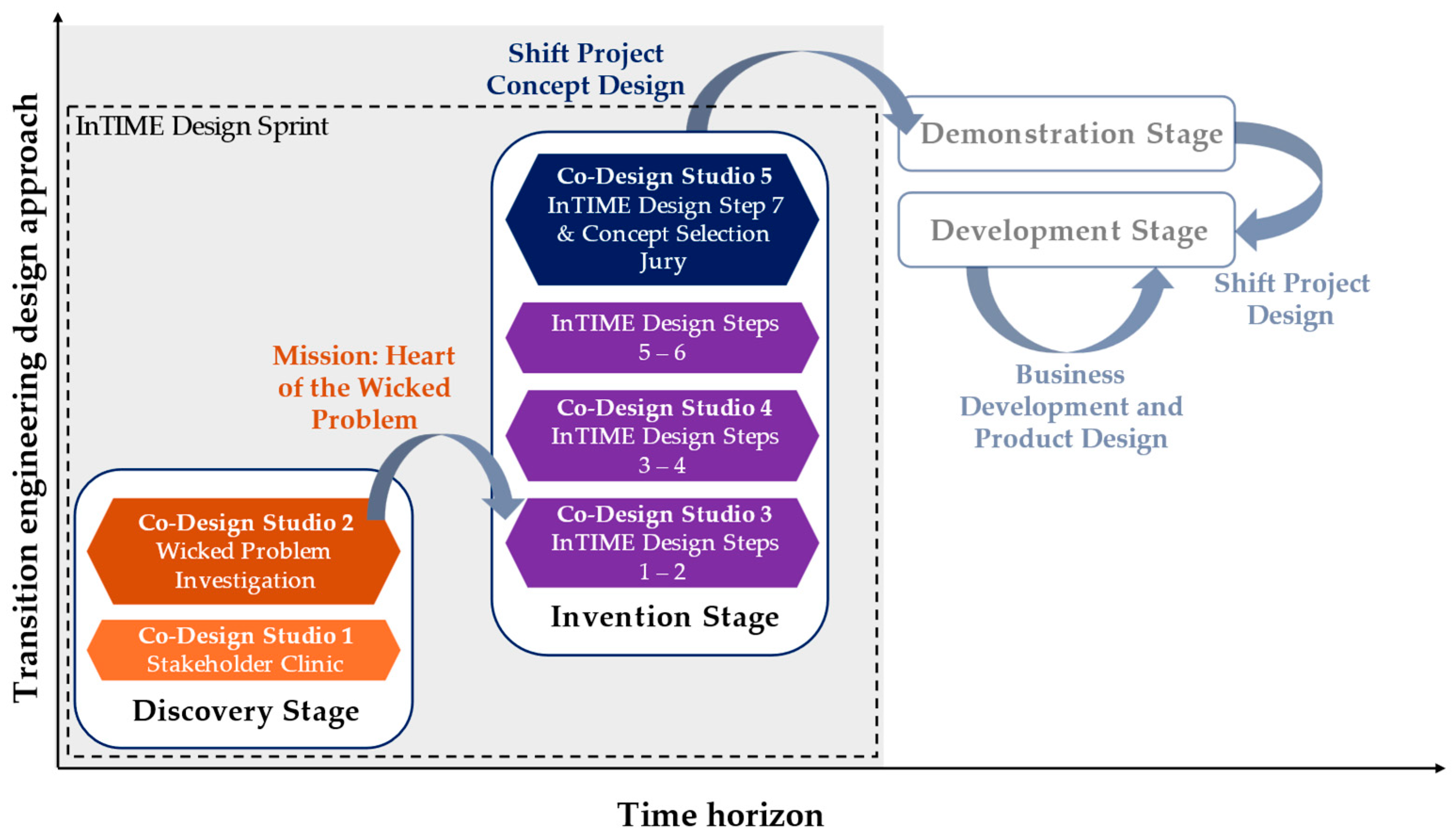
1.3. Approach
1.4. Contribution
2. Background Literature
2.1. General Sustainable Healthcare with Special Focus on Orthosis
- Social and cultural barriers, such as consumer expectations of new and unused products, the wasteful habitual behavior of staff, and the lack of perceived trust in sustainable medical equipment design;
- Engineering system barriers due to a lack of waste collection, sorting, and recycling facilities;
- Governance and organizational barriers caused by conflicting management aims and a lack of standardized directives;
- Policy and regulation barriers based on a lack of enforcement policies and legal support for sustainable and circular practices;
- Supply chain and industry barriers caused by incumbency in training and business models and a lack of demand and supply for eco-friendly alternatives;
- Economic barriers due to the high costs of new infrastructure, technology, and training;
- Hygiene barriers, with the sterilization requirement of some products precluding their reuse;
- Procedural barriers, with current siloed approaches being unlikely to successfully resolve systemic wicked problems;
- Safety barriers, as improper handling of recycled or refurbished products can impact human health, with manufacturers consequently often favoring single-use equipment for its economic advantages.
2.2. Sustainable Orthopedics with a Focus on Orthoses
3. Method
3.1. Aim and Research Design
3.2. Co-Designers
3.3. Data Collection
4. Results
4.1. Co-Design Studio 1: Transition Clinic
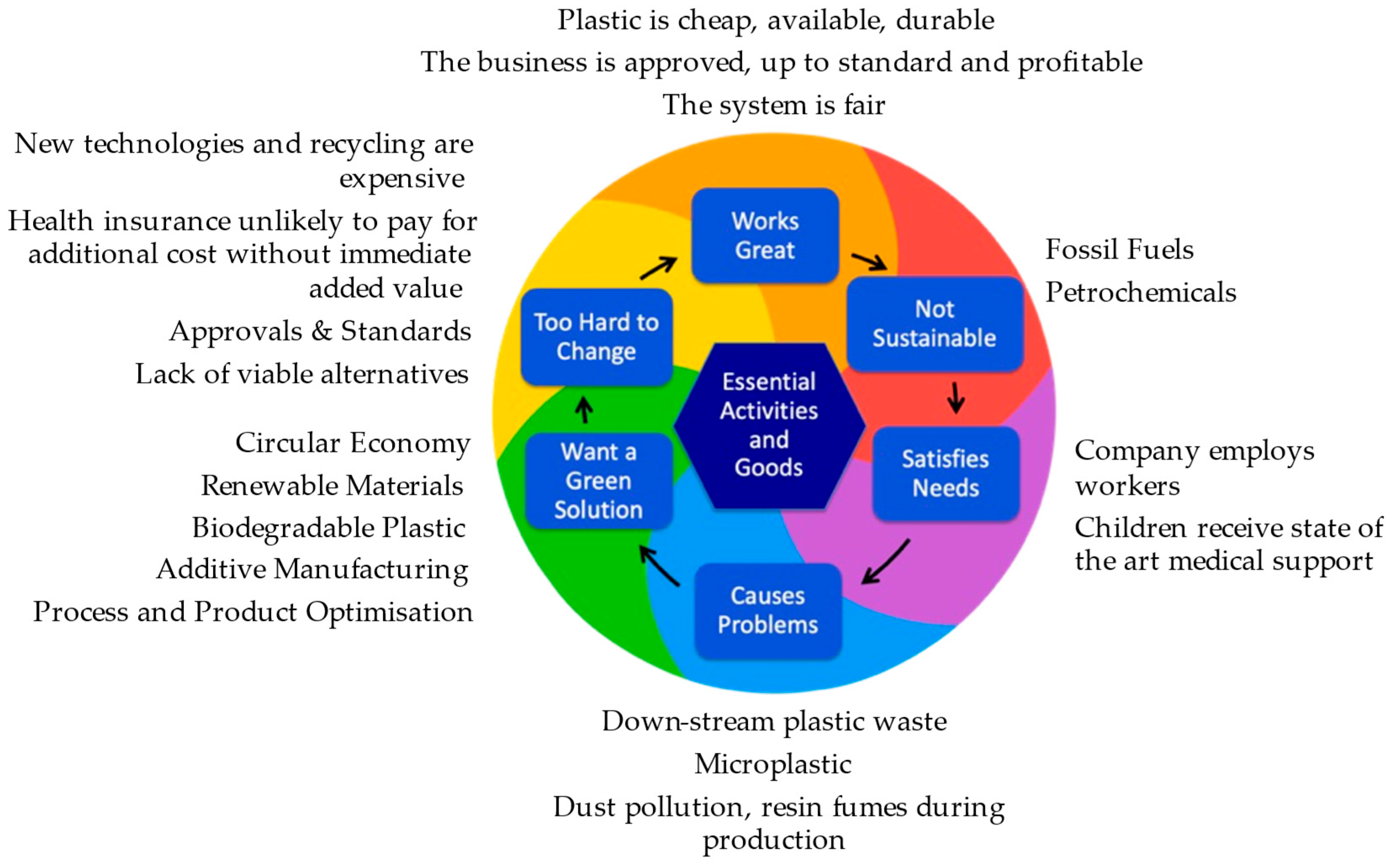
4.2. Co-Design Studio 2: Wicked Problem Investigation
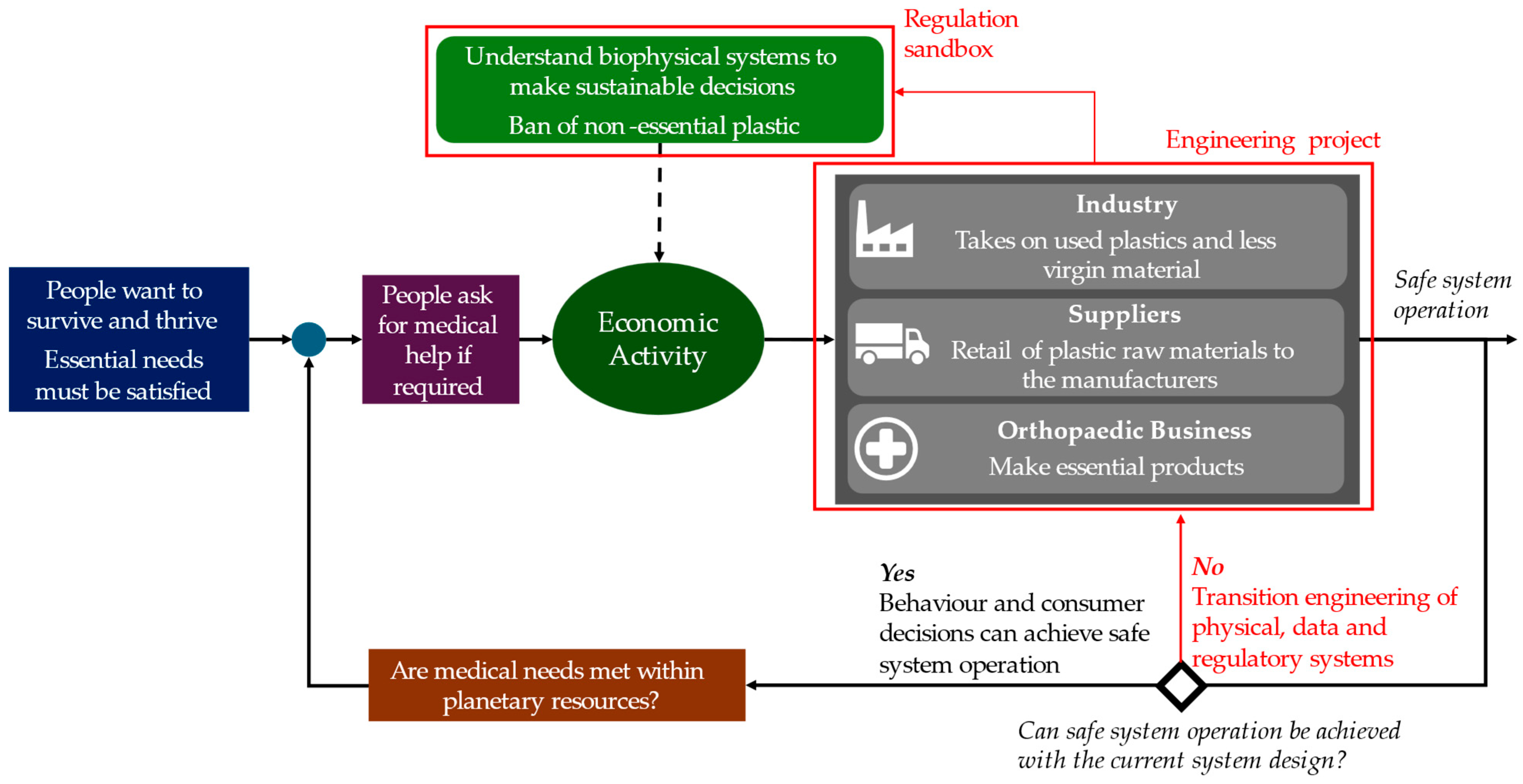
4.3. Co-Design Studio 3: InTIME Design Management Phase
- Step 1: History
- Step 2: Today
4.4. Co-Design Studio 4: InTIME Design Invention and Engineering Stages
- Step 3: Future Scenarios
- Using alternative plastics as feedstock (biodegradable, recyclable etc.);
- Optimizing the material and energy consumption in the production process (i.e., additive manufacturing, renewable energies);
- Using circular economy strategies such as design for X (i.e., X = reuse, repurpose, avoid).
- Step 4: New Century
- Connected data and physical infrastructure systems for managing and allocating resource flows between system actors in a circular economy;
- Product design for low energy and resource consumption, through use of principles of reusability, repairability, sufficiency, and frugality;
- An economic system, including markets, that can operate with energy and material limits and use plastic opportunistically for essential applications;
- A societal paradigm that can understand the essentiality of plastic with a non-acceptability of single-use plastic;
- New business models that operate within the biophysical limits of a renewable energy system with a fraction of today’s virgin material extraction. Propositions were “DIY construction stores” for reusing and repurposing used goods and production machinery, along with a deposit system where orthopedic companies could take back used products for reuse, refurbishment, or repurposing.
- Step 5: Backcasting and Trigger
- Step 6: Shift Project Concepts
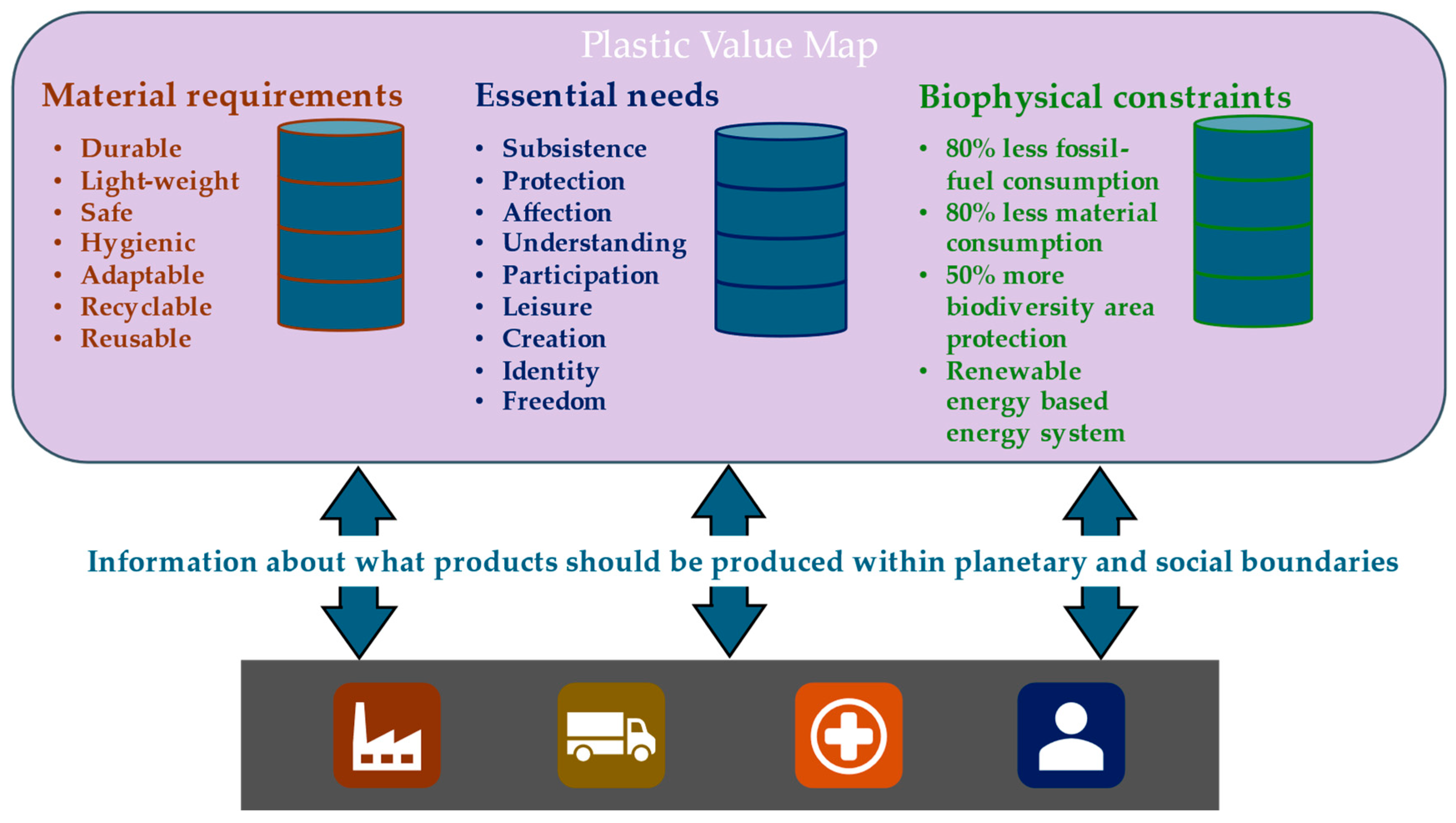
- (1)
- Plastics Value Map
- The availability of recycled plastics based the energy consumption of recycling processes and the available surplus energy from a renewable-energy-based system with drastically downshifted fossil fuel in compliance with climate failure limits;
- The availability of virgin plastic material based on downshifted petrochemical feedstocks;
- The availability of used plastics for reuse, refurbishment, and repurposing.
- (2)
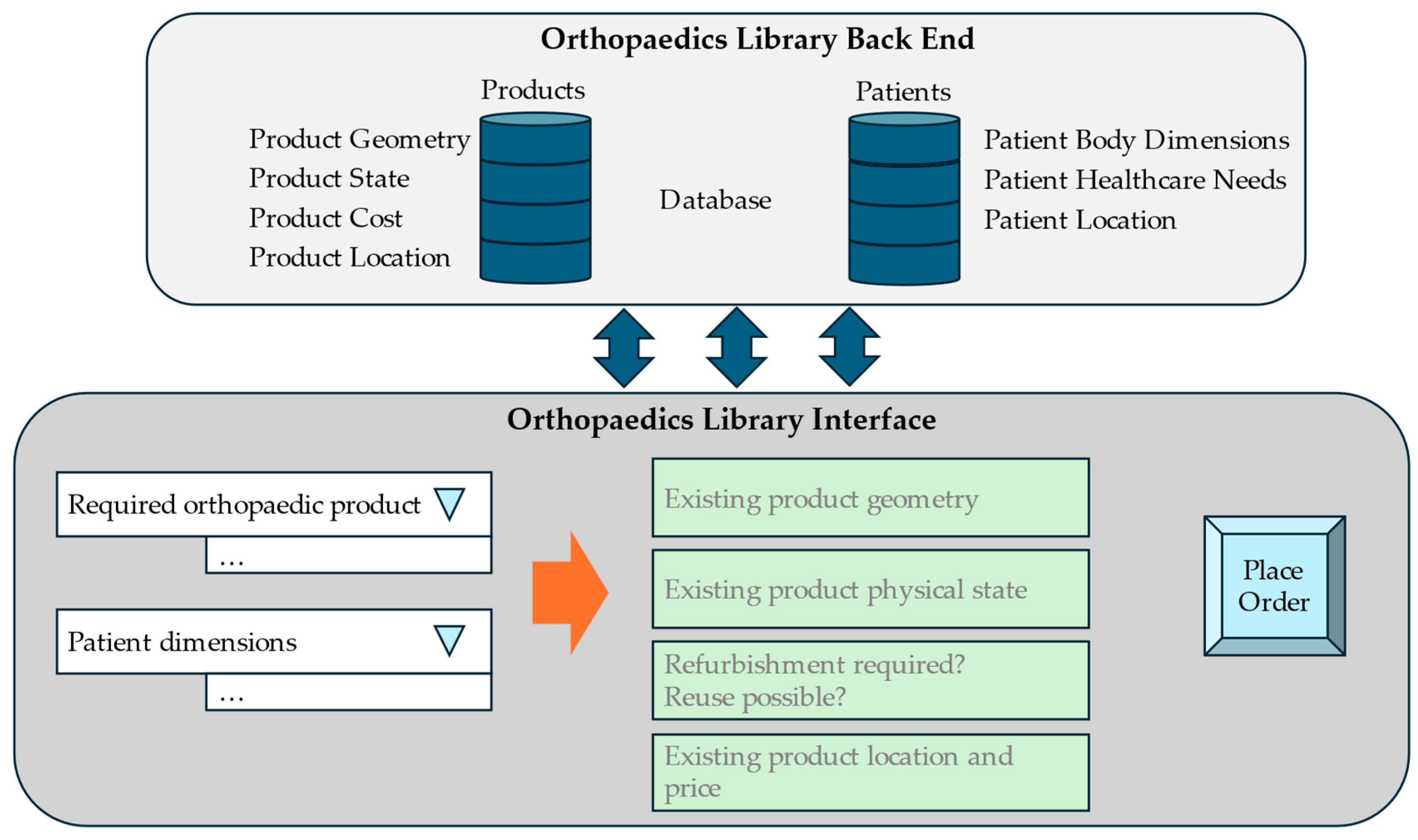
- Orthopedics Library
4.5. Co-Design Studio 5: Transition Foresight and Stakeholder Jury
- Research student: “I enjoyed the vision into the future, because I believe that society thinks that sustainability is essential, but sustainability is not a concrete goal. The future vision enabled us to understand what sustainability would actually mean. The back casting then allowed us to think about ‘how can we reach this future?’. This is also why the process broadened our perspectives beyond engineering and technology solutions by also thinking about social and societal aspects”.
- R&D engineer: “I found the way of getting to the shift project concepts really interesting. We came across points that we were not thinking about before. Especially the history and future steps made me aware of what we want to reach in the future but also how things worked in the past. I liked the general approach to the process. During our workshops we came across problems and solutions that were not looked at before. I also liked the step-by-step way of approaching the problem”.
5. Discussion
- Maintain (or improve) quality, function and usability of the original device when introducing circular strategies—the needs-based approach of the system transitioneering process enabled the co-design to maintain the quality, function, and usability of the essential activity;
- Combine different circular strategies as much as possible—the co-designed shift projects demonstrated principles of the reuse, refurbishment, and reduction of single-use products;
- When integrating circular strategies, make sure to mitigate safety risks for intended use of the device/material/system—in Co-Design Studio 5, the co-designers identified potential risks arising from the shift projects;
- Increase device value and lifetime where possible—the orthopedics library was developed to increase the value and lifetime of the orthoses by enabling reuse and repurpose.
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rizan, C.; Mortimer, F.; Stancliffe, R.; Bhutta, M.F. Plastics in Healthcare: Time for a Re-Evaluation. J. R. Soc. Med. 2020, 113, 49–53. [Google Scholar] [CrossRef] [PubMed]
- NHS England. NHS Clinical Waste Strategy; NHS England: London, UK, 2023.
- German Association of the Plastics Converters German Association of the Plastics Converters Website. Available online: https://www.gkv.de/en/about-us (accessed on 10 September 2024).
- Plastics Europe Plastics Europe Website. Available online: https://plasticseurope.org (accessed on 10 September 2024).
- NHS England. Delivering a ‘Net Zero’ National Health Service; NHS England: London, UK, 2020.
- NHS Scotland. Climate Emergency & Sustainability Strategy 2022–2026; NHS Scotland: Edinburgh, Scotland, 2022.
- Powlesland, D.; Joyce, C. NHS Wales Decarbonisation Strategic Delivery Plan 2021–2030; The Carbon Trust: London, UK, 2021. [Google Scholar]
- UK Government. Health and Care Act 2022; UK Government: London, UK, 2022.
- International Hospital Federation Sustainability Guides. Available online: https://ihf-fih.org/what-we-do/geneva-sustainability-centre/sustainability-guides (accessed on 10 September 2024).
- Leal Filho, W.; Luetz, J.M.; Thanekar, U.D.; Dinis, M.A.P.; Forrester, M. Climate-Friendly Healthcare: Reducing the Impacts of the Healthcare Sector on the World’s Climate. Sustain. Sci. 2024, 19, 1103–1109. [Google Scholar] [CrossRef]
- Davis, F.; Chan, G.; Bendall, S.; Rogers, B.A. Sustainable Orthopaedics: The Needs and Challenges. Orthop. Trauma 2024, 38, 156–161. [Google Scholar] [CrossRef]
- Stacey, I.; Vilà, G.; Torres-Claramunt, R.; Puig, L.; Torrens, C. Plastic Waste in Major Orthopaedic Surgical Procedures: Descriptive and Sources of Improvement. Int. Orthop. 2024, 48, 1701–1706. [Google Scholar] [CrossRef]
- Olatunji, O. Re-Envisioning Plastics Role in the Global Society: Perspectives on Food, Urbanization, and Environment; Springer: Cham, Switzerland, 2024; ISBN 978-3-031-48944-0. [Google Scholar]
- Rittel, H.W.J.; Webber, M.M. Dilemmas in a General Theory of Planning. Policy Sci. 1973, 4, 155–169. [Google Scholar] [CrossRef]
- Fischer, M. Fit for the Future? A New Approach in the Debate about What Makes Healthcare Systems Really Sustainable. Sustainability 2014, 7, 294–312. [Google Scholar] [CrossRef]
- Seager, T.; Selinger, E.; Wiek, A. Sustainable Engineering Science for Resolving Wicked Problems. J. Agric. Environ. Ethics 2012, 25, 467–484. [Google Scholar] [CrossRef]
- Engler, I.D.; Curley, A.J. Environmental Sustainability in Orthopaedic Surgery–Where We Are and Where We Are Going. Oper. Tech. Orthop. 2022, 32, 100995. [Google Scholar] [CrossRef]
- McAleese, T.; Jagiella-Lodise, O.; Roopnarinesingh, R.; Cleary, M.; Rowan, F. Sustainable Orthopaedic Surgery: Initiatives to Improve Our Environmental, Social and Economic Impact. Surgeon 2024, 22, 215–220. [Google Scholar] [CrossRef]
- Moldovan, F.; Moldovan, L. Sustainable Waste Management in Orthopedic Healthcare Services. Sustainability 2024, 16, 5214. [Google Scholar] [CrossRef]
- Meese, H.; Kent, L.; Rowe, W. Transforming Healthcare: The Role of Engineering in Delivering a Net Zero Health Service 2024; Rutledge: London, UK, 2024. [Google Scholar]
- Wognum, N.; Bil, C.; Elgh, F.; Peruzzini, M.; Stjepandić, J.; Verhagen, W.J.C. Transdisciplinary Systems Engineering: Implications, Challenges and Research Agenda. Int. J. Agile Syst. Manag. 2019, 12, 58. [Google Scholar] [CrossRef]
- Ahrens, F.; Boulton, J.; Cherubini, P.; Krumdieck, S. School Run to Net Zero: A Transition Engineering Labs Use Case Report. In Advances in Transdisciplinary Engineering; Cooper, A., Trigos, F., Stjepandić, J., Curran, R., Lazar, I., Eds.; IOS Press: Amsterdam, The Netherlands, 2024. [Google Scholar]
- Krumdieck, S. Transition Engineering: Building a Sustainable Future, 1st ed.; CRC Press: Boca Raton, FL, USA, 2019; ISBN 978-0-367-34126-8. [Google Scholar]
- Lang, D.J.; Wiek, A.; Bergmann, M.; Stauffacher, M.; Martens, P.; Moll, P.; Swilling, M.; Thomas, C.J. Transdisciplinary Research in Sustainability Science: Practice, Principles, and Challenges. Sustain. Sci. 2012, 7, 25–43. [Google Scholar] [CrossRef]
- Ahrens, F.; Krumdieck, S.; Kenning, D. Interdisciplinary Transition Innovation, Management, and Engineering (InTIME) Design: An Intersection Analysis of Design Approaches for Whole-System Sustainability. In Proceedings of the Design Society; Cambridge University Press: Cambridge, UK, 2024; Volume 4, pp. 1169–1178. [Google Scholar]
- Barbero, S.; Pallaro, A. Systemic Design for Sustainable Healthcare. Des. J. 2017, 20, S2473–S2485. [Google Scholar] [CrossRef]
- Pereno, A.; Tamborrini, P. Design for Sustainable Healthcare in a European Context; EDIS-Publishing Institution of the University of Zilina: Zilina, Slovakia, 2016; pp. 234–238. [Google Scholar]
- Smith, C.L.; Rojas, C.; Zurynski, Y.; Partington, A.; Braithwaite, J. From Policy to Practice: Building a Resilient, Climate Aware Health System from the Ground Up. Clim. Change 2025, 178, 69. [Google Scholar] [CrossRef]
- Alfina, K.N.; Ratnayake, R.M.C. Role of Manufacturing Industry for Minimizing the Barriers to Circular Transition in the Health Sector: A Framework. In Advances in Production Management Systems. Production Management Systems for Responsible Manufacturing, Service, and Logistics Futures; Alfnes, E., Romsdal, A., Strandhagen, J.O., Von Cieminski, G., Romero, D., Eds.; Springer: Cham, Switzerland, 2023; Volume 690, pp. 479–496. [Google Scholar]
- Blom, I.M.; Otieno, M.A.; Mayhew, S.; Spicer, N.; Haines, A.; Whitmee, S. Towards a Net-Zero Healthcare System in Kenya: Stakeholder Perspectives on Opportunities, Challenges and Priorities. J. Clim. Change Health 2025, 22, 100417. [Google Scholar] [CrossRef]
- Harding, C.; Moons, I.; Watts, R.; De Win, G.; Du Bois, E. Surveying Factors That Influence Healthcare Personnel in the Transition to Reusable Surgical Gowns. In Proceedings of the Design Society; Cambridge University Press: Cambridge, UK, 2024; Volume 4, pp. 1587–1596. [Google Scholar]
- Hoveling, T.; Svindland Nijdam, A.; Monincx, M.; Faludi, J.; Bakker, C. Circular Economy for Medical Devices: Barriers, Opportunities and Best Practices from a Design Perspective. Resour. Conserv. Recycl. 2024, 208, 107719. [Google Scholar] [CrossRef]
- Mahjoob, A.; Alfadhli, Y.; Omachonu, V. Healthcare Waste and Sustainability: Implications for a Circular Economy. Sustainability 2023, 15, 7788. [Google Scholar] [CrossRef]
- Pereno, A.; Eriksson, D. A Multi-Stakeholder Perspective on Sustainable Healthcare: From 2030 Onwards. Futures 2020, 122, 102605. [Google Scholar] [CrossRef]
- Ville, A.; Hunfeld, N.; Bakker, C.; Sene, B.; Diehl, J.C. Towards Circular ICUs: Circular Intubations as a Catalyser for Systemic Change. In Convergence: Breaking down Barriers Between Disciplines; Melles, M., Albayrak, A., Goossens, R.H.M., Eds.; Springer: Cham, Switzerland, 2024; Volume 30, pp. 235–244. [Google Scholar]
- An, Q.; Sandlund, M.; Lundell, S.; Kuenen, C.; Chastin, S.; Helleday, R.; Messiha, K.; Loisel, Q.; Wadell, K. Transition Design: Co-Creating System Solutions for Chronic Obstructive Pulmonary Disease (COPD) Care. Des. Stud. 2025, 98, 101297. [Google Scholar] [CrossRef]
- Bird, M.; McGillion, M.; Chambers, E.M.; Dix, J.; Fajardo, C.J.; Gilmour, M.; Levesque, K.; Lim, A.; Mierdel, S.; Ouellette, C.; et al. A Generative Co-Design Framework for Healthcare Innovation: Development and Application of an End-User Engagement Framework. Res. Involv. Engagem. 2021, 7, 12. [Google Scholar] [CrossRef]
- Adler, L.M.; Ebel, M.; Rathi, D.; Business, A.; Gebauer-Drechsel, H. Design Principles for Product-Service-Software-System Innovation for Healthcare Manufacturers. In Proceedings of the 57th Hawaii International Conference on System Sciences, Hilton, HI, USA, 3–6 January 2024. [Google Scholar]
- Andersen, A.W.; Jørgensen, S.F.; Gunn, W.; Niero, M. Remanufacturing as a Circular Design Strategy in Healthcare: Integrating Socio-Technical and Environmental-Economic Assessments. Proc. Des. Soc. 2024, 4, 1179–1188. [Google Scholar] [CrossRef]
- Bocken, N.; Ritala, P. Six Ways to Build Circular Business Models. J. Bus. Strategy 2022, 43, 184–192. [Google Scholar] [CrossRef]
- Bocken, N.M.P.; De Pauw, I.; Bakker, C.; Van Der Grinten, B. Product Design and Business Model Strategies for a Circular Economy. J. Ind. Prod. Eng. 2016, 33, 308–320. [Google Scholar] [CrossRef]
- Leppälä, K.; Vornanen, L.; Savinen, O. Lifecycle Extension of Single-Use Medical Device Sensors: Case Study of an Engineering Sustainability Transition Program. J. Clean. Prod. 2023, 423, 138518. [Google Scholar] [CrossRef]
- ISO 59004; Circular Economy–Vocabulary, Principles and Guidance for Implementation. ISO: Geneva, Switzerland, 2024.
- Drobetz, N.; Xu, J.; Chang, D.; Hazan, D.; Collins, W.; Drobetz, H. Less Trash, More Treasure. Waste Production and Reduction in Orthopaedic Surgery. ANZ J. Surg. 2025, 95, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Yadav, D.; Garg, R.K.; Ahlawat, A.; Chhabra, D. 3D Printable Biomaterials for Orthopedic Implants: Solution for Sustainable and Circular Economy. Resour. Policy 2020, 68, 101767. [Google Scholar] [CrossRef]
- Mirkouei, A.; Silwal, B.; Ramiscal, L. Enhancing Economic and Environmental Sustainability Benefits Across the Design and Manufacturing of Medical Devices: A Case Study of Ankle Foot Orthosis. In Design for Manufacturing and the Life Cycle Conference; Proceedings of the 11th International Conference on Micro- and Nanosystems; Cleveland, OH, USA, 6–9 August 2017, American Society of Mechanical Engineers: New York, NY, USA, 2017; Volume 4, p. V004T05A005. [Google Scholar]
- Sachin, B.; Rao, C.M.; Kumar, N.K.; Prasad, C.D.; Kumar, A.; Ravikiran; Manjunath, H.N.; Aravind, S.L.; Bavan, S. Design and Fabrication Strategies for Enhancing Patient Comfort and Sustainability through PETG Based 3D-Printed Orthoses. Prog. Addit. Manuf. 2025, 1–20. [Google Scholar] [CrossRef]
- Ahrens, F.; Cherubini, P.; Boulton, J.; Bartholomew, M.; Krumdieck, S. The First Rule of Transition Engineering Is Define the Wicked Problem. In Advances in Transdisciplinary Engineering; Cooper, A., Trigos, F., Stjepandić, J., Curran, R., Lazar, I., Eds.; IOS Press: Amsterdam, The Netherlands, 2024. [Google Scholar]
- Boulton, J.; Krumdieck, S. Transition Engineering Sprint with Oil Industry Experts: Finding the Possibility for Climate-Safe Business Strategies. In Advances in Transdisciplinary Engineering; Cooper, A., Trigos, F., Stjepandić, J., Curran, R., Lazar, I., Eds.; IOS Press: Amsterdam, The Netherlands, 2024. [Google Scholar]
- Cherubini, P.; Ahrens, F.; Andoni, M.; Couraud, B.; Kilgour, J.; Kirli, D.; Iqbal, Z.; Norbu, S.; Papathanasi, A.; Webb, L.; et al. The Challenge of Ending Fuel Poverty: A Transition Engineering Research Sprint. In Advances in Transdisciplinary Engineering; Cooper, A., Trigos, F., Stjepandić, J., Curran, R., Lazar, I., Eds.; IOS Press: Amsterdam, The Netherlands, 2024. [Google Scholar]
- Sein, M.K.; Henfridsson, O.; Purao, S.; Rossi, M.; Lindgren, R. Action Design Research. MIS Q. 2011, 35, 37. [Google Scholar] [CrossRef]
- Smith, P. Orthopädie–Ein Kurioses Feld. Available online: https://www.aerztezeitung.de/Panorama/Orthopaedie-ein-kurioses-Feld-226695.html (accessed on 20 April 2024).
- Geyer, R.; Jambeck, J.R.; Law, K.L. Production, Use, and Fate of All Plastics Ever Made. Sci. Adv. 2017, 3, e1700782. [Google Scholar] [CrossRef]
- Bringezu, S. Possible Target Corridor for Sustainable Use of Global Material Resources. Resources 2015, 4, 25–54. [Google Scholar] [CrossRef]
- Calverley, D.; Anderson, K. Phaseout Pathways for Fossil Fuel Production Within Paris-Compliant Carbon Budgets; IISD: Winnipeg, MB, Canada, 2022. [Google Scholar]
- Ofgem What Is a Regulatory Sandbox? 2018. Available online: https://www.ofgem.gov.uk/sites/default/files/docs/2018/09/what_is_a_regulatory_sandbox.pdf (accessed on 13 May 2025).
- Robinson, J.B. Futures under Glass. Futures 1990, 22, 820–842. [Google Scholar] [CrossRef]
- Max-Neef, M. Development and Human Needs. In Development Ethics, 1st ed.; Routledge: London, UK, 1992; ISBN 9780754628385. [Google Scholar]
- Veropalumbo, R.; Oreto, C.; Viscione, N.; Pirozzi, F.; Pontoni, L.; Trancone, G.; Race, M.; Russo, F. Exploring the Effect on the Environment of Encapsulated Micro- and Nano-Plastics into Asphalt Mastics for Road Pavement. Environ. Res. 2023, 216, 114466. [Google Scholar] [CrossRef] [PubMed]
- Creutzig, F. Limits to Liberalism: Considerations for the Anthropocene. Ecol. Econ. 2020, 177, 106763. [Google Scholar] [CrossRef]
- Göpel, M. The Great Mindshift. In The Anthropocene: Politik—Economics—Society—Science; Springer: Cham, Switzerland, 2016; Volume 2, ISBN 978-3-319-43765-1. [Google Scholar]
- Weimann, L.; Weimann, E. On the Road to Net Zero Health Care Systems: Governance for Sustainable Health Care in the United Kingdom and Germany. Int. J. Environ. Res. Public Health 2022, 19, 12167. [Google Scholar] [CrossRef]
- Ward, M.E.; Daly, A.; McNamara, M.; Garvey, S.; Teeling, S.P. A Case Study of a Whole System Approach to Improvement in an Acute Hospital Setting. Int. J. Environ. Res. Public Health 2022, 19, 1246. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healthcare Stakeholders | Calls and Commitments |
|---|---|
| Plastic industry associations | Commitments to eco-friendly product design, circular economy policies, and sustainable plastic sources [3,4] |
| Healthcare bodies | Commitments from the British National Health Services in England, Scotland, and Wales to net zero energy and circular resource use in the coming decades [5,6,7]; the commitments are now part of statuary guidance by UK law [8] |
| International Hospital Federation | Guidelines for waste reduction, sustainable supply chains, and procurement and sustainable hospital food [9] |
| Research | Calls for more recycling, sustainable product design, bio-based plastic, and biodegradable plastic [10] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahrens, F.; Nettlenbusch, L.-M.; Krumdieck, S.; Hasse, A. Sustainable Healthcare Plastic Products: Application of the Transition Engineering Design Approach Yields a Novel Concept for Circularity and Sustainability. Sustainability 2025, 17, 4672. https://doi.org/10.3390/su17104672
Ahrens F, Nettlenbusch L-M, Krumdieck S, Hasse A. Sustainable Healthcare Plastic Products: Application of the Transition Engineering Design Approach Yields a Novel Concept for Circularity and Sustainability. Sustainability. 2025; 17(10):4672. https://doi.org/10.3390/su17104672
Chicago/Turabian StyleAhrens, Florian, Lisa-Marie Nettlenbusch, Susan Krumdieck, and Alexander Hasse. 2025. "Sustainable Healthcare Plastic Products: Application of the Transition Engineering Design Approach Yields a Novel Concept for Circularity and Sustainability" Sustainability 17, no. 10: 4672. https://doi.org/10.3390/su17104672
APA StyleAhrens, F., Nettlenbusch, L.-M., Krumdieck, S., & Hasse, A. (2025). Sustainable Healthcare Plastic Products: Application of the Transition Engineering Design Approach Yields a Novel Concept for Circularity and Sustainability. Sustainability, 17(10), 4672. https://doi.org/10.3390/su17104672