Abstract
This study examined the phenomenon of “food deserts” in Las Palmeras, a vulnerable neighborhood in Córdoba, Spain, a medium-sized city known for its agricultural traditions and Mediterranean diet. Through a mixed-methods approach, including spatial analysis, and quantitative and qualitative assessments, we compared dietary habits and food accessibility in Las Palmeras to other Córdoba neighborhoods. We found that Las Palmeras residents reported significantly lower fruit and vegetable consumption and expressed greater difficulty accessing healthy foods despite having a relatively short commute time to the nearest grocery store. Moreover, people in Las Palmeras reported spending more time preparing meals than people in other parts of the city. In contrast, El Brillante, a high-income neighborhood, reported consistent healthy food consumption, even with longer commutes to supermarkets and less time spent preparing meals. This disparity suggests that economic barriers and education levels play a critical role in food choices, emphasizing that food deserts are multidimensional and encompass more than just geographical accessibility to nutritious food. Utilizing the Sustainable Development Goals (SDGs) as a holistic approach, our study amplifies the discussion of sustainable urban development, examining the complex interplay of geographic proximity, socio-economic status, educational levels, generational changes, and the variety of food options in determining access to healthy food. This research offers valuable insights into food accessibility in Spain and contributes to the European dialogue on food deserts and food security, informing strategies for enhancing urban food security, particularly in vulnerable neighborhoods.
1. Introduction
The concept of “food deserts”—urban areas where residents face barriers to accessing affordable and nutritious food—is a subject of significant attention in public health, urban planning, and even socio-economic circles [1,2]. These zones, heavily researched in the US and UK, are emblematic of broader socio-economic disparities, where factors like income, spatial distribution, variety of food options, culture, and education converge to shape food accessibility [3,4,5]. Geographical barriers to accessing nutritious food may predispose individuals to rely on proximate retail outlets, such as fast food establishments and convenience stores [6,7]. These venues often proffer low-price food items characterized by diminished nutrient profiles and elevated caloric densities [8]. Disparities beyond just availability and distance to food stores encompass economic constraints, cultural food preferences, education levels about nutritious diets, and time constraints that limit home cooking opportunities [9,10,11].
Spain, renowned for its rich agricultural production and the world-acclaimed Mediterranean diet recognized by UNESCO as immaterial world heritage, is not immune to this phenomenon [12,13]. Despite its global food and gastronomy reputation, rapid urbanization coupled with economic vulnerabilities and rapid inflation indicate emerging food accessibility challenges [14,15]. This is especially evident in medium-sized cities, which are frequently overshadowed in mainstream research, where one can discern stark contrasts in urban structures, economic status, and community health [16,17].
The existence of food deserts stands in direct opposition to several of the United Nations’ Sustainable Development Goals (SDGs) [18,19,20], notably Goals 2, 3, and 11. SDG 2 aims to “End hunger, achieve food security and improved nutrition, and promote sustainable agriculture” [21]. Food deserts, characterized by limited access to nutritious and affordable food, directly contravene this goal by perpetuating hunger and nutritional deficiencies among urban populations [2]. Furthermore, the lack of access to healthy food choices in these areas contributes to diet-related diseases, thereby impeding progress toward SDG 3 [20], which seeks to “Ensure healthy lives and promote well-being for all at all ages” [21]. Populations in food deserts often have limited access to fresh fruits and vegetables, leading to diets high in (ultra)-processed and energy-dense foods [2]. This dietary pattern is strongly associated with increased risks of obesity, a finding that is consistently reported in public health [22,23,24]. Obesity, in turn, is a known risk factor for various metabolic disorders, including type 2 diabetes, as established in epidemiological studies [25,26,27]. The limited availability of nutrient-rich foods in these areas exacerbates the risk of cardiovascular diseases [28], with some studies highlighting a connection between food deserts and the increased prevalence of hypertension [29] and heart disease [30,31].
Moreover, the psychological impact of living in food-insecure environments, a common characteristic of food deserts, is evidenced by the increased rates of mental health disorders, including depression and anxiety [2,32,33]. The impact is particularly pronounced in children and adolescents, where inadequate nutrition can affect cognitive development and academic performance [34,35]. Additionally, SDG 11 targets to “Make cities and human settlements inclusive, safe, resilient, and sustainable” [21]. The existence of food deserts typically reflects broader socio-economic and spatial inequalities within urban areas, thereby undermining the inclusivity and sustainability of these communities [36]. As highlighted in [37], the quality of life in urban areas, encompassing health and well-being, is a crucial aspect not only of the Sustainable Development Goals (SDGs) but also of the European Green Deal.
The majority of the existing literature on food deserts has been predominantly centered on larger urban areas in the UK and US [2,38], offering comprehensive insights into the socio-economic and health-related impacts of limited access to nutritious and affordable food in these regions [39]. However, this leaves a substantial research gap regarding how food deserts manifest and influence communities in smaller urban and suburban settings across other European nations. These areas, often characterized by distinct socio-economic dynamics, cultural practices, and urban planning models, may exhibit unique patterns [40,41] and consequences of food scarcity that are not adequately captured by the existing research predominantly based on Anglo–American contexts. This void signifies a pressing need for focused studies on food deserts in diverse European settings [39], especially in Mediterranean countries with their praised diet and in smaller cities to develop a more nuanced understanding of this complex issue and to inform targeted policy interventions suited to varied European contexts. This research aims to address this gap by focusing on a medium-sized Spanish city, offering insights into the unique challenges and dynamics of food deserts in such contexts.
In their recent publication, ref. [42] introduced a novel index for assessing food insecurity within a European urban context, integrating economic, geographic, and cultural dimensions. Building upon this foundation, our study extends the analysis by incorporating additional dimensions aligned with the Sustainable Development Goals, specifically focusing on educational and generational factors to provide a more comprehensive understanding of food insecurity. This holistic approach allows us to transcend beyond the biased view of food deserts as mere localized issues. Instead, we align our investigation with broader themes encompassed within the SDGs [43]—not only the direct SDGs previously mentioned, but the promotion of quality education (SDG 4) [21] and the pursuit of responsible consumption and production patterns (SDG 12) [21]. To our knowledge, there is no current research in the literature assessing food desert issues with this boarder holistic approach. This integrative methodology positions the unique challenges of food accessibility within Las Palmeras in relation to wider socio-economic and environmental considerations [44]. By adopting this SDG-centric perspective, our study not only seeks to delineate the characteristics of food deserts but also aims to contribute to a more comprehensive understanding of their role in the sustainable evolution of urban habitats [43]. Such an approach ensures that our findings and subsequent recommendations resonate with the broader objectives of sustainable urban development, addressing the immediate concerns of food scarcity while simultaneously contributing to the overarching goals of the 2030 Agenda for Sustainable Development [43].
This study scrutinizes food accessibility and food choices in a low-income neighborhood—Las Palmeras—of a medium-sized Spanish city—Córdoba. By adopting a comprehensive approach through qualitative and quantitative means, including interviews, population surveys, and spatial analysis, we seek to unravel the patterns of fruit and vegetable consumption, assess the multifaceted accessibility to nutritious foods, delve into the reasons governing dietary selections, and understand the connection between socio-economic status, education, time availability for cooking, and the distribution of food outlets. The primary objective of this paper is to explore in-depth the phenomenon of food deserts, particularly focusing on understanding the interplay between geographical accessibility, socio-economic factors, educational attainment, generational changes, and variety of food choices in determining access to healthy food options. This paper aims to analyze how these elements collectively impact dietary choices and nutritional quality, especially in urban settings or economically disadvantaged neighborhoods. This investigation seeks to include a comparative analysis of different neighborhoods to highlight how varying levels of income, education, and food store diversity influence residents’ food purchasing behaviors and overall diet quality. Hence, this research endeavors to provide a detailed analysis of how context affects the food diet decisions of vulnerable populations in Mediterranean small- and medium-sized cities. The findings derived will not only shed light on Spain’s unique challenges but will also elevate the pan-European conversation on food deserts, empowering stakeholders to formulate comprehensive approaches to boost food accessibility.
2. Materials and Methods
2.1. Hypothesis of the Study
In urban neighborhoods characterized by socio-economic disadvantages, such as Las Palmeras in Córdoba, Spain, several factors influence the dietary patterns of the residents, leading to reduced consumption of healthy foods. This scenario contributes to the manifestation of “food deserts” and is expected to be more pronounced in these areas compared to more affluent areas.
This hypothesis aims to explore the multifaceted impact of geographical accessibility, socio-economic status, and educational attainment on food choices and dietary habits in urban settings, particularly in neighborhoods facing economic challenges. The study posits that these combined factors lead to the emergence of food deserts, adversely affecting the nutritional quality of diets among residents in economically disadvantaged areas.
2.2. Study Area
The efficacy of social interventions is critically dependent on the process of cultural adaptation, which necessitates an in-depth understanding of the target territory. This research is conducted as part of the IN-HABIT initiative, financed by the EU Horizon 2020 program (ref. number 869227). IN-HABIT’s mission is to improve inclusive health and well-being in small to medium-sized cities by implementing different types of strategies. In Córdoba, Spain, the project specifically focused on the Las Palmeras neighborhood. Córdoba, a mid-sized city in the heart of Andalusia with a population of 326,039 inhabitants [45], is notable for its unique historical and cultural heritage [46,47], evidenced by its four UNESCO World Heritage Sites. Despite this rich cultural backdrop, the city faces significant socio-economic challenges, including a high unemployment rate (28.46%) [45] and the presence of several marginalized neighborhoods, among which Las Palmeras is prominent.
The neighborhood, situated on the outskirts of Córdoba, spans approximately 114,000 m2 and is home to 2212 residents [48] (Appendix A). It is characterized by social segregation, a high dependency on social subsidies, and a range of vulnerabilities, including family disintegration, educational failures, and health disparities. The residents of Las Palmeras contend with various barriers to well-being, such as limited employment opportunities, substandard housing quality, insufficient green spaces, and low educational attainment. Residency in Las Palmeras often carries a stigma, influencing inhabitants’ social identity and aspirations. Health concerns in the area include poor diets, high obesity rates, early substance use, and unwanted pregnancies.
2.3. Survey Design and Recruitment
The University of Reading’s ethics committee granted ethical approval (2021-085-RM) for this study. We ensured that all data collection and handling processes aligned with European data protection standards [49]. Each participant provided written informed consent before participating in the study.
We distributed our survey through social media, associations, NGOs, local government channels, and direct in-person interactions at various times and locations. We primarily focused on residents of the Las Palmeras neighborhood but included participants from other Córdoba areas for a broader comparison. Our diverse distribution methods made it challenging to calculate a definitive response rate [50]. In total, 457 individuals participated, with 234 from Las Palmeras and 223 from other city parts. We conducted the data collection in November 2021. The questionnaire was conducted in Spanish and was not gender based; it collected socio-demographic data (age, gender, employment status, and educational attainment) and assessed eating habits and access to healthy foods using Likert scales. Key questions included the following: “How much time do you typically spend preparing your meals at home each day?”; “How many portions of fruit and vegetables do you eat on a typical day?”; “How easy and simple is it for you and your household to eat healthy food in a typical week?”; “How easy is it to find healthy food in your neighborhood or living area?”.
2.4. Qualitative Methods: Interviews and Focus Groups
We organized a focus group to explore generational differences in dietary patterns and potential factors contributing to food deserts in Las Palmeras. Over three years, the IN-HABIT project conducted various workshops in the Las Palmeras neighborhood. We leveraged one of these workshops to host our focus group, recruiting participants through local advertising. Considering the neighborhood’s cultural context, where women mainly manage domestic responsibilities, including food purchasing and preparation, we specifically targeted female participants using a purposeful sampling method; hence, the focus groups were gender based and only women participated. This approach aligns with qualitative research methodologies that select specific population segments to provide rich, relevant, and diverse perspectives [51]. All women in the focus group also participated in the subsequent survey, ensuring a comprehensive understanding of their experiences.
We conducted the focus group session on 8 November 2023. We deliberately made concerted efforts to ensure representation across various age brackets and different sectors of the neighborhood, resulting in the participation of 11 women, aged between 20 and 67 years. This diversity aimed to capture a broad range of experiences and viewpoints [52].
We adhered to the European Union’s ethical standards and data handling protocols for research involving human subjects. We thoroughly briefed all participants about their rights and the research procedures before obtaining their informed consent.
A social worker, experienced in moderating focus groups and familiar with the participants, facilitated the focus group. This familiarity helped create a trusting environment, reducing potential response bias. Following best practices in focus group facilitation ensured candid and unbiased participation [53,54]. The lead researcher attended the session to address all relevant research questions comprehensively. We conducted the session in Spanish and provided transcriptions in Spanish and English, enhancing accessibility and interpretive accuracy for a wider audience.
2.5. Data Analysis
We first evaluated the association between neighborhoods and responses on the Likert scale using a chi-square test. Subsequently, models were constructed to discern dietary habit differences between Las Palmeras and other Córdoba neighborhoods, adjusting for age, gender, and highest educational level achieved.
To assess if the presence or absence of supermarkets and grocery stores and the variety of options were associated with healthy eating, we identified all supermarkets and grocery chains in Córdoba. We identified supermarkets as food providers that present a broad range of healthful options [55]. These supermarkets were characterized as the typical grocery outlets from prominent chains active in Córdoba, such as Lidl and Mercadona. We excluded convenience stores as these tend to have few options for healthy food, if any [55,56]. We identified each supermarket inside the city using their web page addresses. Then we used official Spanish neighborhood demarcations available publicly as land registry records [48] to calculate the area of the different neighborhoods. Once we had the demarcations by neighborhood, we used governmental data from 2020 to classify neighborhoods by average income per capita [45]. Key neighborhoods selected for deeper analysis included the highest-income area (El Brillante/Naranjo), the area with the densest supermarket concentration (Historic center), Las Palmeras (our target neighborhood), and Poligono del Guadalquivir—another neighborhood with socio-demographic characteristics that mirror Las Palmeras.
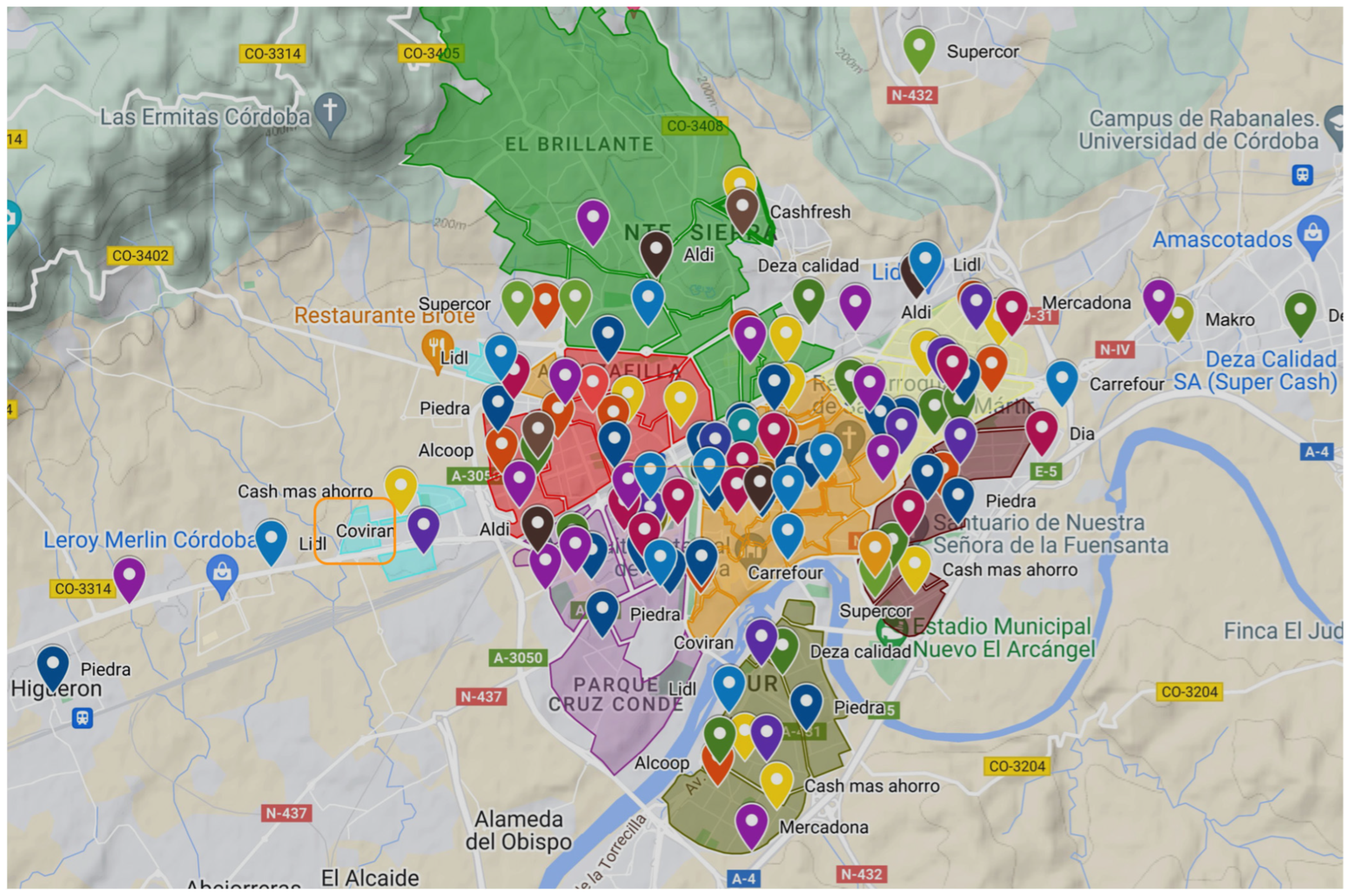
To assess variety, we identified the number of supermarkets or grocery stores in each neighborhood and the number of brands (Figure 1). To assess supermarket density, we computed the number of supermarkets by area in km2. To assess accessibility to healthy supermarkets, we used the ChatGPT AI software (version 4 arquitecture) [57] to randomly identify 30 coordinates in each neighborhood to simulate random addresses; we double checked the integrity of each geographic point using QGIS (version 3.34.2) [58]. Then, we estimated the proximity to the nearest grocery store or supermarket and used Google Maps [59] to calculate the walking and driving times to travel there. Finally, we compared the distances between neighborhoods using ANOVAs. Analyses were conducted using OpenStreetMap [60], R software (version 4.3.2) [61], QGIS [58], ChatGPT [57], and Google Maps [59].
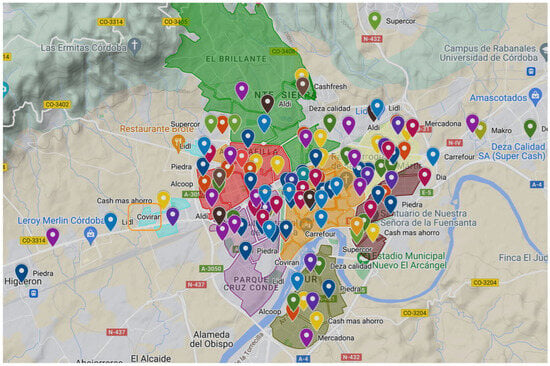
Figure 1.
Map of Córdoba highlighting supermarkets and neighborhood boundaries. This map illustrates the city of Córdoba, with clear demarcations of its various neighborhoods and the locations of supermarkets. Each supermarket is indicated with a specific marker, allowing for an easy visual assessment of their distribution across the city. Las Palmeras neighborhood is identified with an orange square.
3. Results
3.1. Socio-Demographic and Descriptive Statistics
The analysis included a total of four hundred and fifty-seven completed surveys; two hundred and thirty-four participants were from Las Palmeras and two hundred and twelve were from other neighborhoods in Córdoba. The socio-demographic characteristics of the participants are presented in Table 1. The sample was primarily composed of women (60%), the average age was 39 years, and the level of education varied significantly between Las Palmeras and the other neighborhoods. A total of 49% of participants from Las Palmeras had “no studies”, or their highest level of education was “primary or secondary education”, while in the rest of the neighborhoods in Córdoba, only 10% of participants reported having either “no studies” or that their highest level of education was “primary or secondary education”.

Table 1.
Characteristics of participants by neighborhood (Las Palmeras vs. other). This table presents a breakdown of the socio-demographic profiles of the study participants, categorized by their respective neighborhoods. It includes demographic variables such as age, gender, employment status, and educational attainment, with variable names emphasized in bold and italics. Each neighborhood is represented in a separate column, facilitating a direct comparison across different areas.
3.2. Eating Behaviours
A total of 18% of participants in Las Palmeras reported not eating fruits and vegetables at all during the day, while only 6.3% of people in the other neighborhoods reported not consuming fruits and vegetables (Table 2). In Las Palmeras, 35% of participants reported some kind of difficulty eating healthy foods, while in other neighborhoods, the value was closer to 21%. None of the participants from the neighborhoods of Córdoba reported to have difficulties buying healthy food, while in Las Palmeras, 12% of the participants reported having issues buying healthy foods in their area (Table 2). Finally, almost 20% of participants from Las Palmeras reported spending more than two hours a day preparing meals, while only 8% reported cooking for more than two hours in other neighborhoods (Table 2). The chi-square tests show differences between Las Palmeras and the other neighborhoods for fruit and vegetable intake (p-value = 0.003), the easiness of eating healthy food (p-value < 0.001), easiness to buy healthy food in the neighborhood (p-value < 0.001), and time spent preparing meals (p-value < 0.001). Once we fitted the models and corrected them for demographic factors, only the easiness of eating healthy food (p-value = 0.02, b = 0.27, 95% CI = 0.04, 0.50) and the easiness of buying healthy food in the neighborhood (p-value < 0.001, b = 1.09, 95% CI = 0.69, 1.50) remained significant (Table 3); however, the models, overall, fitted regularly.
Table 2.
Eating habits by neighborhood (Las Palmeras vs. other neighborhoods). This table presents a comparative analysis of key eating habits between residents of Las Palmeras and those from other neighborhoods. The table is divided into distinct sections, each representing a different aspect of dietary behavior, with names and chi-square results emphasized in bold and italics: (1) fruit and vegetable intake, (2) weekly intake of healthy foods, (3) ease of access to healthy food in the neighborhood, and (4) time spent preparing meals. For each category, data are split by neighborhood, with one column for Las Palmeras and another for other neighborhoods. The survey was not gender based and both men and women participated.
Table 3.
General linear models of eating habits by neighborhood, adjusted for socio-demographic factors. This table displays the results of general linear models analyzing various eating habits, including fruit and vegetable intake, ease of access to healthy food in the neighborhood, weekly intake of healthy foods, and time spent preparing meals. The analysis is stratified by neighborhood (Las Palmeras vs. other) and adjusted for key socio-demographic variables such as age, gender, and highest educational level. The table provides coefficients, 95% CI, R2, and p-value, indicating the relationship between each eating habit and the neighborhood, while controlling for socio-demographic factors.
3.3. Geospatial Analysis
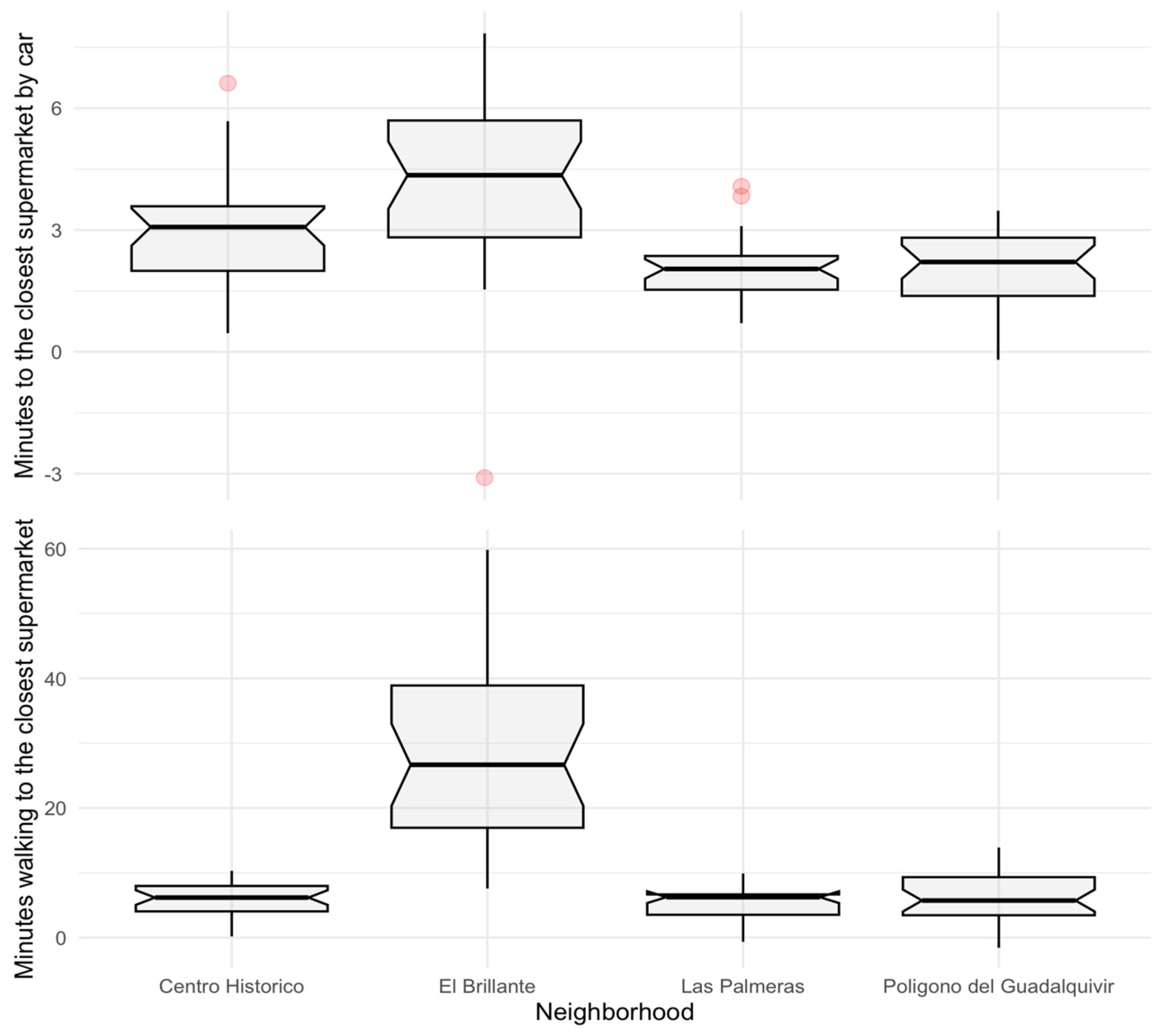
We found that the neighborhood of Las Palmeras has no supermarket or grocery store within its boundaries. The closest grocery store was located in the next neighborhood of Miralbaida. The closest big supermarket was 5 min away by car or a 29-minute walk. The average number of supermarkets in other neighborhoods of the city was between 3 and 5, and the city center had as many as 17 stores. Once we corrected by the area of the neighborhood, the city center had on average 7.2 stores per km2; El Brillante/Naranjo, the neighborhood with the highest income on average, had 0.39 supermarkets per km2 in its area. Supermarket accessibility was best in the inner district of the city center, which has high supermarket density and variety. Poligono del Guadalquivir, the other neighborhood with demographic factors similar to Las Palmeras, had 4.41 supermarkets per km2 (Appendix B) and two supermarket varieties. Finally, we found differences among neighborhoods in the time to go to the closest supermarket, either by foot or by car. However, the ANOVA tests show that the neighborhoods with the highest income per capita (El Brillante) reported having the longest commute time to go to the supermarket via both methods of transport (Figure 2).
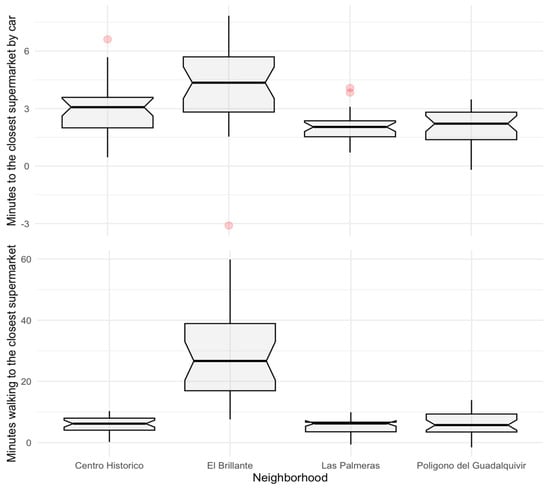
Figure 2.
Commute time to closest supermarket by neighborhood. This figure presents two boxplots comparing the commute time to the closest supermarket among different neighborhoods, differentiated by mode of transportation. The upper boxplot displays the time taken to reach the nearest supermarket by car, while the lower boxplot shows the time taken to walk to the nearest supermarket. Each boxplot includes data for various neighborhoods, including Las Palmeras, El Brillante, the city center, and Poligono del Guadalquivir.
3.4. Focus Group
In the conducted focus group, none of the women participants were familiar with the term “food desert”. All reported being primarily responsible for food purchasing and preparation within their households, except for one participant who did not cook. The household compositions varied; one participant cohabitated with her boyfriend, a younger participant resided with her parents, one was a widow living alone, another older participant took care of her parents, and one lived with her husband while also caring for her parents. Most other participants lived with their spouses and children, with the largest household comprising five individuals. Among the participants, the two younger women (under 30 years) were childless, and one older participant was single without children. The majority had grown children and grandchildren.
Throughout the discussions, it became apparent that the gender dynamics within households significantly influenced food-related responsibilities. Women participants consistently described themselves as the primary decision-makers and actors in food shopping and meal preparation activities. This dominant role of women in managing household nutrition was a recurring theme, reflecting traditional gender norms around food and family care in the community.
Participants reported planning meals in advance, with most grocery shopping undertaken in supermarkets outside the neighborhood due to the limited local options. Everyday items were purchased at neighborhood stores, but longer shopping trips required a bus journey of approximately one and a half to two hours (e.g, woman 2: “I have to go to Mercadona to buy food”). While some stews were made with items from local stores, major shopping trips for items like fish or lean protein were less frequent, ranging from weekly to monthly. The focus group also touched upon the changing dynamics of gender roles, particularly how the increasing employment of women has impacted meal preparation habits. Participants noted that with both men and women now often engaged in full-time work, there was less time available for traditional cooking practices. This shift was seen as contributing to the younger generation’s increased reliance on convenient food options, including ready-to-eat meals and processed foods, as opposed to home-cooked meals.
Fruit and vegetable consumption varied among participants. While some ate vegetables daily, often fried or in stews, fruit intake was generally lower, with most consuming it only a few times a week. Red meats and processed meats like pork cuts were widely consumed (e.g, woman 3: “Yesterday I had French fries, peppers and eggs, and I had a ham sandwich at night. At noon, I made tripe for my husband, but I don’t like them, so “flamenquín” balls (fried steak/ham with breadcrumbs) and French fries.”). Despite being aware of healthier food choices, many participants admitted insufficient intake of fish, fruits, and vegetables and excessive coffee consumption. None of the participants talked about other diet-related issues that are associated with obesity, like food portions, excess fried food intake, or the type of protein consumed. All acknowledged the impact of their diets on their health.
Price emerged as the primary factor influencing food purchases, with only two participants not constrained by budget. Preferences of husbands and children, particularly aversions to vegetables, also played a role in food choices. Some avoided fish due to taste preferences or perceived poor quality. Distance and cost were cited as barriers to accessing a wider variety of food. The two young participants highlighted a lack of time as a major constraint to eating healthy foods.
Regarding dietary habits, participants noted that their cooking styles closely mirrored those of their parents, with traditional dishes like “potaje” (hearty legume stew) and “guisados” (meat or other proteins with potatoes and sauce) being common. The youngest participant mentioned cooking at home, while another younger participant preferred quicker, ready-made supermarket options. Participants observed a generational shift in eating habits, perceiving past diets as healthier and more natural compared to current trends of processed and chemically enhanced foods (e.g, woman 2: “The Young ones only eat burgers”). The convenience of ready-to-eat meals was seen as contributing to a decline in cooking among younger generations. Older participants expressed a desire to pass down traditional cooking skills to younger family members, noting a general lack of time or interest in cooking among the youth. This shift was exemplified by one young participant’s preference for pizza and another’s reliance on quick options like macaroni or French fries, highlighting a move away from traditional culinary practices.
4. Discussion
This research aimed to elucidate the potential existence of a food desert in the Las Palmeras neighborhood of Córdoba, Spain, by assessing residents’ dietary habits and accessibility to fresh and healthy foods compared to other neighborhoods in the city. This comprehensive analysis presents a multifaceted view of the concept of food deserts, emphasizing the interplay between geographical proximity, socio-economic factors, educational attainment, and the variety of food options. While our findings indicate a correlation between socio-economic constraints, limited educational opportunities, and the challenges in accessing healthy foods in Las Palmeras, it is essential to clarify that these factors may not directly cause the existence of food deserts but rather contribute to the vulnerability of the residents in this area. Socio-economic status and education levels are integral components of the broader social determinants of health that influence a range of life outcomes, including access to nutritious food. In this context, they act as contributing factors that exacerbate the challenges faced by residents of Las Palmeras in accessing healthy food options rather than being direct variables causing the food desert condition. Therefore, it is crucial to view these socio-economic and educational factors as part of a complex web of determinants that collectively impact the food environment in Las Palmeras. Our findings revealed that food choices in Las Palmeras are not the result of one specific factor but rather the combination of economic, cultural, educational, geographical, and generational issues that intertwined, creating a unique environment that makes access to healthy foods difficult. Key points are that the social exclusion experienced in these neighborhoods can lead to a sense of disenfranchisement and disconnection from broader societal networks or even nearby neighborhoods and that the lower levels of education limit access to social capital that could otherwise facilitate better opportunities for making healthy food choices, hence improving health outcomes. Similar studies on food insecurity have highlighted its multidimensional nature and the complex interplay of factors influencing access to healthy food options [62].
Several noteworthy factors underscore the complex issue of food accessibility in Las Palmeras. First of all, contrary to expectations based on the literature [63,64,65], Las Palmeras did not exhibit the longest distance to a supermarket. However, Las Palmeras inhabitants reported significantly reduced fruit and vegetable consumption, while simultaneously expressing heightened difficulty in obtaining such items locally. From a logistic standpoint, 30 designated points in Las Palmeras suggest an average commute of about two minutes by car and approximately four and a half minutes on foot to the closest supermarket. El Brillante, Córdoba’s highest per-capita income neighborhood, has the lowest supermarket density and the longest commutes. Yet, survey data indicate its residents report consistent high fruit and vegetable consumption without expressing accessibility challenges. Our results go in hand with those of [66], which showed that participants from food deserts in Pennsylvania were willing to travel to supermarkets to shop for food and found no association between distance to the closest supermarket and diet. This trend has been found with other health measures such as those of [67], which found no association between proximity to the nearest supermarket and fruit and vegetable consumption, and those of [68], which measured supermarket distance and obesity rates and found no correlation between distance and obesity.
Other factors, such as education, quality, size and diversity of supply chains, or even access to cars, could be playing a more significant role than the distance in this scenario [69,70,71]. El Brillante had six supermarkets in its area from different brands, three of which were among the city’s largest supermarkets. On the other hand, the store near Las Palmeras was small with limited food variety and, according to the focus groups, had low-quality foods. This trend highlights the importance of a dimension to assess food deserts other than the distance to a supermarket; this additional dimension is the variety of supermarkets. In affluent areas like El Brillante, a diverse array of food options is readily available, reflecting the socio-economic privileges that enable access to a wider range of healthy foods. A neighborhood with similar demographic factors to Las Palmeras, El Poligono del Guadalquivir, scored a bit higher in fruit and vegetable intake, access to healthy food in the kitchen, and the easiness of eating healthy food at home. Unlike Las Palmeras, this neighborhood had four supermarkets in its area, all from different brands. The comparison of these two neighborhoods showed that although it may be geographically close, a singular supermarket near the neighborhood is not enough to guarantee access to healthy food, due to a lack of variety and offerings.
Our results also showed that socio-economic barriers also compromise access to healthy foods [72,73]. Las Palmeras stands as one of Spain’s economically disadvantaged neighborhoods, hinting at the potential financial constraints its residents face in accessing nutritious foods [73]. The higher cost of healthful food, combined with market dynamics that might curtail product availability based on consumer purchasing power, could further hinder access [74,75]. For instance, costly nutritious items, such as nuts, might be unaffordable to Las Palmeras residents, and, consequentially, local stores might not even stock such products. This finding aligns with existing literature emphasizing that individuals from economically disadvantaged areas often spend a larger fraction of their income on food, albeit cheaper and less nutritious food [76,77]. Furthermore, there is a need to recognize the predominant demographics of the neighborhood, which include mothers with multiple children (often derived from early pregnancy) or elderly women, possibly experiencing mobility challenges and difficult access to independent modes of transport [78,79]; in contrast, in El Brillante/Naranjo, most people have private cars. The combination of these socio-economic factors might affect access to supermarkets more than mere distance.
Over the past few generations, there has been a significant shift in eating behaviors, reflecting broader societal changes [80,81], as highlighted by the women in the focus group. In earlier times, meals were predominantly prepared at home, often from scratch, using fresh ingredients [82]. Cooking skills were passed down through generations, and meals were a central aspect of family life [80,82]. However, with the advent of industrialization and the rise in dual-income households, these traditions began to wane. Today’s generations are increasingly reliant on ready-to-eat meals and processed foods, driven by convenience and time constraints [83,84]. The proliferation of fast-food outlets, the availability of microwaveable meals, and the ease of ordering food online have further fueled this trend [84]. While these changes have brought about unprecedented convenience, they have also raised concerns about nutritional quality. Processed foods often contain higher levels of sugar, salt, and unhealthy fats, contributing to rising rates of obesity and related health issues [85,86]. The lack of nutritional knowledge, combined with the lack of time to cook meals and the easiness of accessing processed food, makes younger generations in neighborhoods like Las Palmeras more vulnerable to adopting and perpetuating unhealthy eating habits.
Educational disparities play a critical role in this complex web. Lower educational attainment in these communities often results in reduced employment opportunities and perpetuates a cycle of poverty. This lack of education also hinders the acquisition of knowledge about health-promoting behaviors, thereby exacerbating health disparities [87]. In Las Palmeras, the lower educational levels may contribute to limited nutritional awareness and poorer diet quality, as seen in other studies [88]. Furthermore, educational attainment appears to be a pivotal factor in food choice. Lower educational levels may impact their comprehensive food literacy, affecting dietary habits [89]. Those with more advanced educational backgrounds tend to opt for healthier nutritional patterns, as shown by [90], who found that higher education correlates with healthier food choices due to increased nutritional knowledge.
The interplay of factors contributing to neighborhoods at risk of social exclusion is intricate and multifaceted, often leading to self-perpetuating cycles that exacerbate issues related to health and well-being [91,92,93]. These neighborhoods, typically characterized by higher levels of poverty, unemployment, and lower educational attainment, face a network of interrelated challenges that reinforce one another [92]. For instance, limited economic resources not only restrict access to quality healthcare and nutritious food but also lead to substandard living conditions, which in turn can exacerbate health problems [94]. While from an exclusively geographical perspective, access to food might not be the primary concern in Las Palmeras, a combination of economic constraints and limited awareness due to educational levels possibly plays a pivotal role in shaping the dietary patterns of its residents [77]. The recognition of the complex dimensions of food security underscores the necessity of innovative governance models, which rely on collaborative efforts between civil society, the private sector, and local government entities [95]. Therefore, although policies aimed at redistributing food, such as food banks, might assist in addressing food insecurity in these areas, more comprehensive strategies are necessary. As highlighted by [96] in a recent publication, relying solely on food banks may not suffice to effectively tackle the complex issue of food insecurity.
This holistic or multidimensional perception of urban phenomena, as adopted in our research, serves as a microcosm of the global challenges outlined in the Sustainable Development Goals (SDGs), aligning with our initial proposal of using the SDGs as a comprehensive approach [43]. This interconnected nature of the SDGs is vividly illustrated by the challenges encountered in Las Palmeras. By addressing food accessibility issues in this neighborhood, our study contributes directly to the aims of SDG 11 (Sustainable Cities and Communities) while also impacting SDG 3 (Good Health and Well-being) through the potential for improved public health outcomes. Furthermore, the educational component of our findings, emphasizing the need for enhanced nutritional literacy, aligns seamlessly with SDG 4 (Quality Education). The observed disparities in food accessibility between El Brillante and Las Palmeras highlight the need for a more heterogeneous food landscape, illustrating how urban planning and public health strategies must converge to foster sustainable consumption patterns as envisaged by SDG 12. This interplay of various SDGs within a localized context not only reflects broader discussions in the literature but also underscores our study’s alignment with a larger narrative. Our research, therefore, transcends the exploration of an isolated urban issue, instead situating it within the expansive discourse of sustainable urban development. Through this approach, we demonstrate that local actions and research endeavors are integral to advancing global objectives for sustainable development, thereby contributing meaningfully to the broader conversation on creating resilient and sustainable urban environments.
5. Conclusions
Our study in the Las Palmeras neighborhood of Córdoba, Spain offers an analysis of the interplay between geographical accessibility, socio-economic factors, educational attainment, generational changes, and food variety in determining access to healthy food options. Despite being geographically close to supermarkets, Las Palmeras residents encounter significant challenges in accessing nutritious foods, primarily influenced by socio-economic constraints and limited educational opportunities. This situation contrasts with that in more affluent areas like El Brillante, where residents have access to a wider variety of food options.
The differences in food accessibility between Las Palmeras and El Brillante highlight the influence of socio-economic and educational factors. El Brillante, with its higher economic status, presents a greater variety of food retailers, facilitated by the residents’ purchasing power, which enhances their access to diverse and healthy food options. On the other hand, Las Palmeras, which is affected by economic limitations, exhibits a narrower range of food options. The impact of these economic challenges is further compounded by educational factors, which potentially influence the residents’ ability to make informed dietary choices. Therefore, the variety of food in Las Palmeras is limited, reflecting the neighborhood’s socio-economic context.
Our findings indicate that the concept of food deserts is shaped by more than just physical distance to food sources; economic status and educational background also play significant roles. These factors contribute to barriers that extend beyond physical access, influencing the ability to purchase and utilize healthier food options. These insights are not only relevant to the specific context of Las Palmeras but also contribute to global efforts to achieve the United Nations Sustainable Development Goals. By addressing the identified challenges in food accessibility, our research contributes to efforts toward achieving several SDGs. These include SDG 2 through improving food security, SDG 3 by promoting healthier diets, and SDG 11 by highlighting the need for inclusive urban development strategies. Moreover, the educational aspects of our findings support SDG 4, emphasizing the importance of nutritional education in making informed food choices. Moreover, the educational aspects of our findings support SDG 4, emphasizing the importance of nutritional education in making informed food choices. Addressing these issues requires an approach that goes beyond improving physical access to healthy foods. It necessitates policies and interventions that also consider economic and educational disparities. Thus, our localized study offers valuable contributions to these global goals, demonstrating how targeted interventions in specific communities can resonate with broader sustainable development efforts. Such a comprehensive strategy is essential for bridging the gap in food accessibility and contributing to the overall health and sustainability of urban communities.
6. Limitations
This study represents an initial exploration into the concept of food deserts within the Spanish context, particularly focusing on the Las Palmeras neighborhood in Córdoba. Despite its comprehensive approach, combining various methodologies and considering a range of factors, the research is subject to limitations that merit consideration. One key limitation is the underrepresentation of ethnic minorities in the sample, constituting only 2% of respondents. This limited representation restricts the depth of analysis regarding ethnicity’s role in accessing nutritious food. Additionally, the study did not account for other socio-demographic variables, such as unemployment rates, that might influence access to healthy food.
The reliance on the 2020 Spanish census data presents another constraint. Although these is the latest available data, the socio-economic landscape may have shifted post-pandemic, potentially affecting some indicators. Furthermore, the cross-sectional design of this study restricts its ability to capture the evolving nature of food deserts over time, whereas a longitudinal approach could provide more dynamic insights.
Moreover, the study’s findings may have limited applicability beyond the specific context of Córdoba. The distinct socio-economic, cultural, and urban characteristics of the Las Palmeras neighborhood may not be directly comparable to other cities, countries, or regions. The study’s focus and methodology, deeply rooted in the local context, potentially limit the generalizability of the findings to areas with different economic structures, cultural backgrounds, or dietary habits. The observed dynamics in a medium-sized city like Córdoba may also differ from those in larger urban centers or rural areas. Consequently, while this study offers insights into food accessibility in Las Palmeras, extrapolating these findings to different geographical contexts requires caution. Future research should consider comparative analyses across varied locations to enhance our understanding of food deserts in diverse settings and inform appropriate interventions in public health and urban planning.
Author Contributions
C.C.-P.: conceptualization, methodology, software, formal analysis, writing—original draft, writing—review and editing, visualization, data curation. F.-J.M.-C.: conceptualization, qualitative methodology, writing—review and editing. M.M.D.-S.: conceptualization, supervision, writing—review and editing, funding acquisition. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded under the IN-HABIT project (Inclusive Health and Wellbeing in Medium and Small Size Cities—https://www.inhabit-h2020.eu) as part of the Horizon 2020 Program (Grant Agreement No.: 869227). The content of this document does not reflect the official opinion of the European Union. Responsibility for the information and views expressed therein lies entirely with the authors.
Institutional Review Board Statement
The survey for data collection (2021-085-RM) has been granted approval by the ethics committee of the University of Reading. Participants were informed about the purpose of the research, data collection and management, and the anonymity of the survey, and then they signed an informed consent. Data are treated respecting the anonymity of the participants.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data of the participants’ survey will be available in Zenodo upon acceptance of the study (DOI will be provided). The data will only be available from the authors upon request.
Acknowledgments
The authors are very thankful to the researchers who designed the survey and helped with the dissemination and collection of data: Isotta Mac Fadden (USAL), Roberta Cocchioni (ISIM), Giacomo Arrighini (ISIM), Paola Di Lazzaro (ISIM), Cristiana Russo (ISIM), Sveva Batani (ISIM), Monica D’Arcangelis (ISIM), Maria Dentale (ISIM), Rachel Mc Cloy (UREAD), Shannon Wake (UREAD), and the ladies of Las Palmeras who participated in the focus group.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
Geographic overview of the study area. This map provides a comprehensive view of the study location. At the national level, it indicates the position of Córdoba within Spain (inset), highlighting the city’s geographical context within the country. The main section of the map zooms into the city of Córdoba, delineating its boundaries and urban layout. Within this urban setting, the Las Palmeras neighborhood is distinctly marked, showcasing its specific location relative to the broader cityscape.
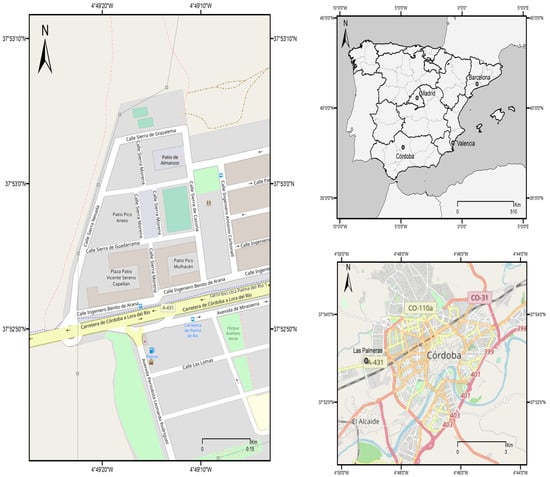
Figure A1.
Map of Córdoba and “Las Palmera”.
Figure A1.
Map of Córdoba and “Las Palmera”.

Appendix B
Supermarkets and economic overview by neighborhood in Córdoba. This table provides a detailed comparison of each neighborhood in Córdoba, showcasing key data points: the average GDP per capita, the total number of supermarkets, and the density of supermarkets per square kilometer. The neighborhoods are listed in one column, with corresponding data on supermarket count, supermarket density, and economic indicators in subsequent columns.
Table A1.
Summary of supermarket distribution and density in relation to neighborhood GDP.
Table A1.
Summary of supermarket distribution and density in relation to neighborhood GDP.
| Neighborhood | Annual GDP Per Capita (Euros) | Number of Supermarkets | Density of Supermarkets Per km2 |
|---|---|---|---|
| Tejares, Molinos Alta, San Cayetano | 17,715 | 2 | 5.56 |
| El Brillante, Naranjo | 17,340 | 3 | 0.32 |
| Huerta de la Marquesa | 16,029 | 0 | 0 |
| Cercadilla, Olivos Borrachos | 15,728 | 1 | 1.85 |
| Vista Alegre, Vallellano, Parque Cruz Conde | 15,468 | 2 | 0.45 |
| Arruzafilla | 14,283 | 2 | 2.25 |
| Santa Rosa, Camping | 14,215 | 2 | 1.92 |
| Casco histórico | 14,043 | 18 | 7.2 |
| Santa Isabel | 13,214 | 2 | 1.9 |
| Ciudad Jardínn | 1306 | 12 | 7.8 |
| Margaritas, Colonia de la Paz | 11,597 | 5 | 2.02 |
| Cañero, Fidiana | 11,244 | 1 | 1.2 |
| Valdeolleros, Chinales | 10,543 | 1 | 0.86 |
| Levante, Zumbacón | 10,466 | 5 | 4.38 |
| Figueroa | 10,393 | 5 | 4.55 |
| Viñuela, Rescatado, Cerro de la Golondrina | 10,115 | 5 | 3.36 |
| Miralbaida, Electromecánicas | 10,017 | 1 | 1.27 |
| El Arcángel | 9764 | 2 | 1.89 |
| Fátima | 9704 | 2 | 1.26 |
| Campo de la Verdad, Fray Albino | 9284 | 2 | 1.8 |
| Fuensanta, Santuario | 9102 | 3 | 2.95 |
| El Higuerón, Alameda del Ovispo | 8772 | 3 | 2.12 |
| Las Moreras, Huerta de la Reina | 8706 | 0 | 0 |
| Sector Sur | 8181 | 5 | 1.81 |
| Polígono del Guadalquivir | 7488 | 2 | 0.41 |
| Las Palmeras, Parque Azahara | 7482 | 0 | 0 |
References
- Cummins, S.; Macintyre, S. “Food deserts”—Evidence and assumption in health policy making. Br. Med. J. 2002, 325, 436–438. [Google Scholar] [CrossRef]
- Walker, R.E.; Keane, C.R.; Burke, J.G. Disparities and access to healthy food in the United States: A review of food deserts literature. Health Place 2010, 16, 876–884. [Google Scholar] [CrossRef]
- Chavis, C.; Bhuyan, I.A. Data-driven food desert metric to understand access to grocery stores using chi-square automatic interaction detector decision tree analysis. Transp. Res. Rec. 2022, 2676, 571–589. [Google Scholar] [CrossRef]
- Schafft, K.A.; Jensen, E.B.; Hinrichs, C.C. Food deserts and overweight schoolchildren: Evidence from Pennsylvania. Rural Sociol. 2009, 74, 153–177. [Google Scholar] [CrossRef]
- Howerton, G.; Trauger, A. “Oh honey, don’t you know?” The Social Construction of Food Access in a Food Desert. ACME Int. J. Crit. Geogr. 2017, 16, 740–760. [Google Scholar]
- Evans, A.; Banks, K.; Jennings, R.; Nehme, E.; Nemec, C.; Sharma, S.; Hussaini, A.; Yaroch, A. Increasing access to healthful foods: A qualitative study with residents of low-income communities. Int. J. Behav. Nutr. Phys. Act. 2015, 12, S5. [Google Scholar] [CrossRef] [PubMed]
- Vandevijvere, S.; Sushil, Z.; Exeter, D.J.; Swinburn, B. Obesogenic retail food environments around New Zealand schools: A national study. Am. J. Prev. Med. 2016, 51, e57–e66. [Google Scholar] [CrossRef] [PubMed]
- Laska, M.N.; Hearst, M.O.; Forsyth, A.; Pasch, K.E.; Lytle, L. Neighbourhood food environments: Are they associated with adolescent dietary intake, food purchases and weight status? Public Health Nutr. 2010, 13, 1757–1763. [Google Scholar] [CrossRef] [PubMed]
- Morland, K.B.; Evenson, K.R. Obesity prevalence and the local food environment. Health Place 2009, 15, 491–495. [Google Scholar] [CrossRef] [PubMed]
- Larson, N.I.; Story, M.T.; Nelson, M.C. Neighborhood environments: Disparities in access to healthy foods in the US. Am. J. Prev. Med. 2009, 36, 74–81. [Google Scholar] [CrossRef]
- D’iez, J.; Cebrecos, A.; Rapela, A.; Borrell, L.N.; Bilal, U.; Franco, M. Socioeconomic inequalities in the retail food environment around schools in a Southern European context. Nutrients 2019, 11, 1511. [Google Scholar] [CrossRef] [PubMed]
- Blas, A.; Garrido, A.; Unver, O.; Willaarts, B. A comparison of the Mediterranean diet and current food consumption patterns in Spain from a nutritional and water perspective. Sci. Total Environ. 2019, 664, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- Mariscal-Arcas, M.; Rivas, A.; Velasco, J.; Ortega, M.; Caballero, A.M.; Olea-Serrano, F. Evaluation of the Mediterranean Diet Quality Index (KIDMED) in children and adolescents in Southern Spain. Public Health Nutr. 2009, 12, 1408–1412. [Google Scholar] [CrossRef] [PubMed]
- Gracia-Arnaiz, M. Eating in a time of ‘crisis’: New health and dietary contexts in Spain. In Envisioning a Future without Food Waste and Food Poverty: Societal Challenges; Wageningen Academic Publishers: Wageningen, The Netherlands, 2015; pp. 1–38. [Google Scholar]
- Gracia Arnaiz, M.; Garc’ia Oliva, M.; Demonte, F.C. The problem of hunger in Spain: Analysis of digital media from 2008–2018. 2022, 4, 3–17. [Google Scholar] [CrossRef]
- Kunzmann, K.R. Medium-sized towns, strategic planning and creative governance. In Making Strategies in Spatial Planning: Knowledge and Values; Springer: Dordrecht, The Netherlands, 2010; pp. 27–45. [Google Scholar]
- Borrell, C.; Pons-Vigués, M.; Morrison, J.; D’iez, È. Factors and processes influencing health inequalities in urban areas. J. Epidemiol. Community Health 2013, 67, 389–391. [Google Scholar] [CrossRef] [PubMed]
- Plum, A.; Kaljee, L. Achieving sustainable, community-based health in Detroit through adaptation of the UNSDGs. Ann. Glob. Health 2016, 82, 981–990. [Google Scholar] [CrossRef]
- Mohiuddin, Z.A.; Begum, R.; Iqbal, H. Significance of Gender Equality in accomplishment of Sustainable Development Goals. Significance 2018, 41, 26–33. [Google Scholar]
- Spencer, G.; Corbin, J.H.; Miedema, E. Sustainable development goals for health promotion: A critical frame analysis. Health Promot. Int. 2019, 34, 847–858. [Google Scholar] [CrossRef]
- United Nations. United Nations Global Sustainable Development Report 2015; United Nations: San Francisco, CA, USA, 2015. [Google Scholar]
- Fong, A.J.; Lafaro, K.; Fong, Y. ASO Author Reflections: Access to Healthcare Does Not Mean Access to Health: Food Deserts in the Land of Plenty. Ann. Surg. Oncol. 2021, 28, 2508–2509. [Google Scholar] [CrossRef] [PubMed]
- Reed, M.; Dancy, B.; Holm, K.; Wilbur, J.; Fogg, L. Eating behaviors among early adolescent African American girls and their mothers. J. Sch. Nurs. 2013, 29, 452–463. [Google Scholar] [CrossRef] [PubMed]
- Buscemi, J.; O’Donnell, A.; Takgbajouah, M.; Patano, P. A Spatial Analysis of Food Insecurity and Body Mass Index with Income and Grocery Store Density in a Diverse Sample of Adolescents and Young Adults. Nutrients 2023, 15, 1435. [Google Scholar] [CrossRef] [PubMed]
- Moulana, M.; Lima, R.; Reckelhoff, J.F. Metabolic syndrome, androgens, and hypertension. Curr. Hypertens. Rep. 2011, 13, 158–162. [Google Scholar] [CrossRef]
- Jung, U.J.; Choi, M.-S. Obesity and its metabolic complications: The role of adipokines and the relationship between obesity, inflammation, insulin resistance, dyslipidemia and nonalcoholic fatty liver disease. Int. J. Mol. Sci. 2014, 15, 6184–6223. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, Y.; Kihara, S.; Funahashi, T.; Matsuzawa, Y.; Libby, P. Adiponectin: A key adipocytokine in metabolic syndrome. Clin. Sci. 2006, 110, 267–278. [Google Scholar] [CrossRef]
- Kelli, H.M.; Hammadah, M.; Ahmed, H.; Ko, Y.-A.; Topel, M.; Samman-Tahhan, A.; Awad, M.; Patel, K.; Mohammed, K.; Sperling, L.S.; et al. Association between living in food deserts and cardiovascular risk. Circ. Cardiovasc. Qual. Outcomes 2017, 10, e003532. [Google Scholar] [CrossRef]
- Hardin-Fanning, F. Adherence to a Mediterranean diet in a rural Appalachian food desert. Rural Remote Health 2013, 13, 215–224. [Google Scholar] [CrossRef]
- Kelli, H.M.; Kim, J.H.; Samman Tahhan, A.; Liu, C.; Ko, Y.-A.; Hammadah, M.; Sullivan, S.; Sandesara, P.; Alkhoder, A.A.; Choudhary, F.K.; et al. Living in food deserts and adverse cardiovascular outcomes in patients with cardiovascular disease. J. Am. Heart Assoc. 2019, 8, e010694. [Google Scholar] [CrossRef] [PubMed]
- Testa, A.; Jackson, D.B.; Semenza, D.C.; Vaughn, M.G. Food deserts and cardiovascular health among young adults. Public Health Nutr. 2021, 24, 117–124. [Google Scholar] [CrossRef]
- Walsan, R.; Pai, N.B.; Rajan, B. Food deserts and its impact on mental health. Indian J. Soc. Psychiatry 2016, 32, 435. [Google Scholar]
- Crowe, J.; Lacy, C.; Columbus, Y. Barriers to food security and community stress in an urban food desert. Urban Sci. 2018, 2, 46. [Google Scholar] [CrossRef]
- Pizzol, D.; Tudor, F.; Racalbuto, V.; Bertoldo, A.; Veronese, N.; Smith, L. Systematic review and meta-analysis found that malnutrition was associated with poor cognitive development. Acta Paediatr. 2021, 110, 2704–2710. [Google Scholar] [CrossRef]
- Akubuilo, U.C.; Iloh, K.K.; Onu, J.U.; Iloh, O.N.; Ubesie, A.C.; Ikefuna, A.N. Nutritional status of primary school children: Association with intelligence quotient and academic performance. Clin. Nutr. ESPEN 2020, 40, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Tozer, L.; Hörschelmann, K.; Anguelovski, I.; Bulkeley, H.; Lazova, Y. Whose city? Whose nature? Towards inclusive nature-based solution governance. Cities 2020, 107, 102892. [Google Scholar] [CrossRef]
- Voukkali, I.; Zorpas, A.A. Evaluation of urban metabolism assessment methods through SWOT analysis and analytical hierocracy process. Sci. Total Environ. 2022, 807, 150700. [Google Scholar] [CrossRef] [PubMed]
- Wagner, J.; Hinton, L.; McCordic, C.; Owuor, S.; Capron, G.; Arellano, S. Do Urban Food Deserts Exist in the Global South? An Analysis of Nairobi and Mexico City. Sustainability 2019, 11, 1963. [Google Scholar] [CrossRef]
- Cerovečki, I.; Grünhagen, M. “Food Deserts” in Urban Districts. J. Macromark. 2016, 36, 337–353. [Google Scholar] [CrossRef]
- Anheier, H.K.; Hoelscher, M. Cultural sustainability in small and medium-sized cities. In Culture and Sustainability in European Cities: Imagining Europolis; Routledge: London, UK, 2015; p. 17. [Google Scholar]
- Wagner, M.; Growe, A. Research on small and medium-sized towns: Framing a new field of inquiry. World 2021, 2, 105–126. [Google Scholar] [CrossRef]
- Bernaschi, D.; Marino, D.; Cimini, A.; Mazzocchi, G. The Social Exclusion Perspective of Food Insecurity: The Case of Blacked-Out Food Areas. Sustainability 2023, 15, 2974. [Google Scholar] [CrossRef]
- Ali, S.M.; Appolloni, A.; Cavallaro, F.; D’Adamo, I.; Di Vaio, A.; Ferella, F.; Gastaldi, M.; Ikram, M.; Kumar, N.M.; Martin, M.A.; et al. Development Goals towards Sustainability. Sustainability 2023, 15, 9443. [Google Scholar] [CrossRef]
- Bernaschi, D.; Leonardi, L. Food insecurity and changes in social citizenship. A comparative study of Rome, Barcelona and Athens. Eur. Soc. 2023, 25, 413–443. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística pablación Córdoba 2022. Available online: https://ine.es/nomen2/index.do?accion=busquedaRapida&subaccion=&numPag=0&ordenAnios=ASC&nombrePoblacion=cordoba&botonBusquedaRapida=Consult+selection (accessed on 3 August 2023).
- Garcia, L.G.; Muñoz Fernandez, G.A.; Lopez-Guzman, T. Cultural tourism and flamenco in the city of Cordoba (Spain). J. Qual. Assur. Hosp. Tour. 2019, 20, 581–598. [Google Scholar] [CrossRef]
- Lopez-Guzman, T.; Gonzalez Santa-Cruz, F. International tourism and the UNESCO category of intangible cultural heritage. Int. J. Cult. Tour. Hosp. Res. 2016, 10, 310–322. [Google Scholar] [CrossRef]
- Ayuntamiento de Córdoba Población barrios 2020. Available online: https://www.cordoba.es/la-ciudad/cifras-estadisticas/estadisticas-de-poblacion/estadisticas-2020 (accessed on 16 August 2023).
- General Data Protection Regulation (GDPR) 2018. Available online: https://eur-lex.europa.eu/eli/reg/2016/679/oj (accessed on 15 October 2022).
- Bethlehem, J. Selection bias in web surveys. Int. Stat. Rev. 2010, 78, 161–188. [Google Scholar] [CrossRef]
- Patton, M.Q. Qualitative Research & Evaluation Methods: Integrating Theory and Practice; Sage Publications: London, UK, 2014. [Google Scholar]
- Krueger, R.A.; Casey, M.A. Focus Group Interviewing. In Handbook of Practical Program Evaluation; Jossey-Bass: Hoboken, NJ, USA, 2015; pp. 506–534. [Google Scholar]
- Bayne-Smith, M.; Mizrahi, T.; García, M. Interdisciplinary Community Collaboration: Perspectives of Community Practitioners on Successful Strategies. J. Community Pract. 2008, 16, 249–269. [Google Scholar] [CrossRef]
- Williams, S.; Parang, E. Using focus groups to match user expectations with library constraints. Ser. Libr. 1997, 31, 335–339. [Google Scholar] [CrossRef]
- Jang, M.J.; Kim, S.A.; Chung, S.; Joung, H. Accessibility and Availability of Food Store in Urban Area of Korea. FASEB J. 2017, 31, lb446. [Google Scholar] [CrossRef]
- De Weese, R.S.; Ohri-Vachaspati, P. Disparities in Healthy Food Access: Are We Improving? FASEB J. 2017, 31, 45–47. [Google Scholar]
- OpenAI ChatGPT: Optimizing Language Models for Dialogue 2023. Available online: https://openai.com/chatgpt (accessed on 15 October 2022).
- QGIS Development Team QGIS Geographic Information System; Open Source Geospatial Foundation Project; Open Source Geospatial Foundation: Beaverton, ON, USA, 2016.
- Google LLC. Google Maps 2023; Google: Mountain View, CA, USA, 2023. [Google Scholar]
- OpenStreetMap. Contributors OpenStreetMap 2023; OpenStreetMap: Washington, DC, USA, 2023. [Google Scholar]
- R Core Team R: A Language and Environment for Statistical Computing. Vienna, Austria, 2023; Available online: https://www.r-project.org/ (accessed on 15 October 2022).
- Grimaccia, E.; Naccarato, A. Food insecurity in Europe: A gender perspective. Soc. Indic. Res. 2022, 161, 649–667. [Google Scholar] [CrossRef]
- Bodor, J.N.; Rice, J.C.; Farley, T.A.; Swalm, C.M.; Rose, D. The association between obesity and urban food environments. J. Urban Health 2010, 87, 771–781. [Google Scholar] [CrossRef]
- Morland, K.; Wing, S.; Roux, A.D. The contextual effect of the local food environment on residents’ diets: The atherosclerosis risk in communities study. Am. J. Public Health 2002, 92, 1761–1768. [Google Scholar] [CrossRef]
- Laraia, B.A.; Siega-Riz, A.M.; Kaufman, J.S.; Jones, S.J. Proximity of supermarkets is positively associated with diet quality index for pregnancy. Prev. Med. 2004, 39, 869–875. [Google Scholar] [CrossRef]
- Dubowitz, T.; Zenk, S.N.; Ghosh-Dastidar, B.; Cohen, D.A.; Beckman, R.; Hunter, G.; Steiner, E.D.; Collins, R.L. Healthy food access for urban food desert residents: Examination of the food environment, food purchasing practices, diet and BMI. Public Health Nutr. 2015, 18, 2220–2230. [Google Scholar] [CrossRef]
- Aggarwal, A.; Cook, A.J.; Jiao, J.; Seguin, R.A.; Vernez Moudon, A.; Hurvitz, P.M.; Drewnowski, A. Access to supermarkets and fruit and vegetable consumption. Am. J. Public Health 2014, 104, 917–923. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A. The economics of food choice behavior: Why poverty and obesity are linked. In Obesity Treatment and Prevention: New Directions; Karger Publishers: Basel, Switzerland, 2012; Volume 73, pp. 95–112. [Google Scholar]
- Krukowski, R.A.; West, D.S.; Harvey-Berino, J.; Prewitt, T.E. Neighborhood Impact on Healthy Food Availability and Pricing in Food Stores. J. Community Health 2010, 35, 315–320. [Google Scholar] [CrossRef]
- Vogel, C.; Ntani, G.; Inskip, H.; Barker, M.; Cummins, S.; Cooper, C.; Moon, G.; Baird, J. Education and the Relationship Between Supermarket Environment and Diet. Am. J. Prev. Med. 2016, 51, e27–e34. [Google Scholar] [CrossRef] [PubMed]
- Minaker, L.M.; Olstad, D.L.; Thompson, M.E.; Raine, K.D.; Fisher, P.; Frank, L.D. Associations between frequency of food shopping at different store types and diet and weight outcomes: Findings from the NEWPATH study. Public Health Nutr. 2016, 19, 2268–2277. [Google Scholar] [CrossRef]
- Gustin, L.; Gray, V. A Sustainable Cooking Show Intervention to Address Barriers Contributing to Suboptimal Diets. J. Nutr. Food Sci. 2018, 8, 2. [Google Scholar] [CrossRef]
- Wolfson, J.A.; Ramsing, R.; Richardson, C.R.; Palmer, A. Barriers to healthy food access: Associations with household income and cooking behavior. Prev. Med. Rep. 2019, 13, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A. Obesity, diets, and social inequalities. Nutr. Rev. 2009, 67, S36–S39. [Google Scholar] [CrossRef]
- Dai, D.; Wang, F. Geographic disparities in accessibility to food stores in southwest Mississippi. Environ. Plan. B Plan. Des. 2011, 38, 659–677. [Google Scholar] [CrossRef]
- Ward, P.R.; Verity, F.; Carter, P.; Tsourtos, G.; Coveney, J.; Wong, K.C. Food stress in Adelaide: The relationship between low income and the affordability of healthy food. J. Environ. Public Health 2013, 2013, 968078. [Google Scholar] [CrossRef] [PubMed]
- Hallum, S.; Hughey, S.; Wende, M.; Stowe, E.; Kaczynski, A. Healthy and unhealthy food environments are linked with neighbourhood socio-economic disadvantage: An innovative geospatial approach to understanding food access inequities. Public Health Nutr. 2020, 23, 3190–3196. [Google Scholar] [CrossRef] [PubMed]
- Major, E.; Delmelle, E.C.; Delmelle, E. SNAPScapes: Using geodemographic segmentation to classify the food access landscape. Urban Sci. 2018, 2, 71. [Google Scholar] [CrossRef]
- Mayfield, K.E.; Carolan, M.; Weatherspoon, L.; Chung, K.R.; Hoerr, S.M. African American Women’s Perceptions on Access to Food and Water in Flint, Michigan. J. Nutr. Educ. Behav. 2017, 49, 519–524.e1. [Google Scholar] [CrossRef] [PubMed]
- Espinoza-Ortega, A. Nostalgia in food consumption: Exploratory study among generations in Mexico. Int. J. Gastron. Food Sci. 2021, 25, 100399. [Google Scholar] [CrossRef]
- Kime, N. Children’s eating behaviours: The importance of the family setting. Area 2008, 40, 315–322. [Google Scholar] [CrossRef]
- Ogden, J.; Dalkou, M.; Kousantoni, M.; Ventura, S.S.; Reynolds, R. Body weight, the home environment, and eating behaviour across three generations of women: A Quasi-longitudinal study in four Mediterranean and non-Mediterranean countries. Aust. Psychol. 2017, 52, 442–452. [Google Scholar] [CrossRef]
- Slater, J. Is cooking dead? The state of Home Economics Food and Nutrition education in a Canadian province. Int. J. Consum. Stud. 2013, 37, 617–624. [Google Scholar] [CrossRef]
- Muhamad, I.I.; Abdul Karim, N. Trends, convenience, and safety issues of ready meals. In Minimally Processed Foods: Technologies for Safety, Quality, and Convenience; Springer International Publishing: Cham, Switzerland, 2014; pp. 105–123. [Google Scholar]
- Fuhrman, J. The hidden dangers of fast and processed food. Am. J. Lifestyle Med. 2018, 12, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Weaver, C.M.; Dwyer, J.; Fulgoni III, V.L.; King, J.C.; Leveille, G.A.; MacDonald, R.S.; Ordovas, J.; Schnakenberg, D. Processed foods: Contributions to nutrition. Am. J. Clin. Nutr. 2014, 99, 1525–1542. [Google Scholar] [CrossRef]
- Cutler, D.M.; Lleras-Muney, A. Understanding differences in health behaviors by education. J. Health Econ. 2010, 29, 1–28. [Google Scholar] [CrossRef]
- Cutler, D.M.; Glaeser, E.L.; Shapiro, J.M. Why have Americans become more obese? J. Econ. Perspect. 2003, 17, 93–118. [Google Scholar] [CrossRef]
- Vidgen, H.A.; Gallegos, D. Defining food literacy and its components. Appetite 2014, 76, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef] [PubMed]
- Cattell, V. Poor people, poor places, and poor health: The mediating role of social networks and social capital. Soc. Sci. Med. 2001, 52, 1501–1516. [Google Scholar] [CrossRef] [PubMed]
- Roux, A.V.D.; Mair, C. Neighborhoods and health. Ann. N. Y. Acad. Sci. 2010, 1186, 125–145. [Google Scholar] [CrossRef]
- Kamp, I.; van Loon, J.; Droomers, M.; Hollander, A. den Residential Environment and Health: A Review of Methodological and Conceptual Issues. Rev. Environ. Health 2004, 19, 381–401. [Google Scholar] [CrossRef] [PubMed]
- Poulsen, M.N.; Hulland, K.R.S.; Gulas, C.A.; Pham, H.; Dalglish, S.L.; Wilkinson, R.K.; Winch, P.J. Growing an urban oasis: A qualitative study of the perceived benefits of community gardening in baltimore, maryland. Cult. Agric. Food Environ. 2014, 36, 69–82. [Google Scholar] [CrossRef]
- Zerbian, T.; de Luis Romero, E. The role of cities in good governance for food security: Lessons from Madrid’s urban food strategy. Territ. Polit. Gov. 2023, 11, 794–812. [Google Scholar] [CrossRef]
- Warshawsky, D.N. Food insecurity and the COVID pandemic: Uneven impacts for food bank systems in Europe. Agric. Hum. Values 2023, 40, 725–743. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).