
The Role of Fulfilment and Disillusion in the Relationship between Burnout and Career Satisfaction in Italian Healthcare Workers

 , , , ,
, , , ,
Abstract
1. Introduction
1.1. Burnout Syndrome
1.2. Burnout in Healthcare
1.3. Fulfilment, Disillusion, and Burnout in Healthcare
1.4. Satisfaction with a Career in Healthcare
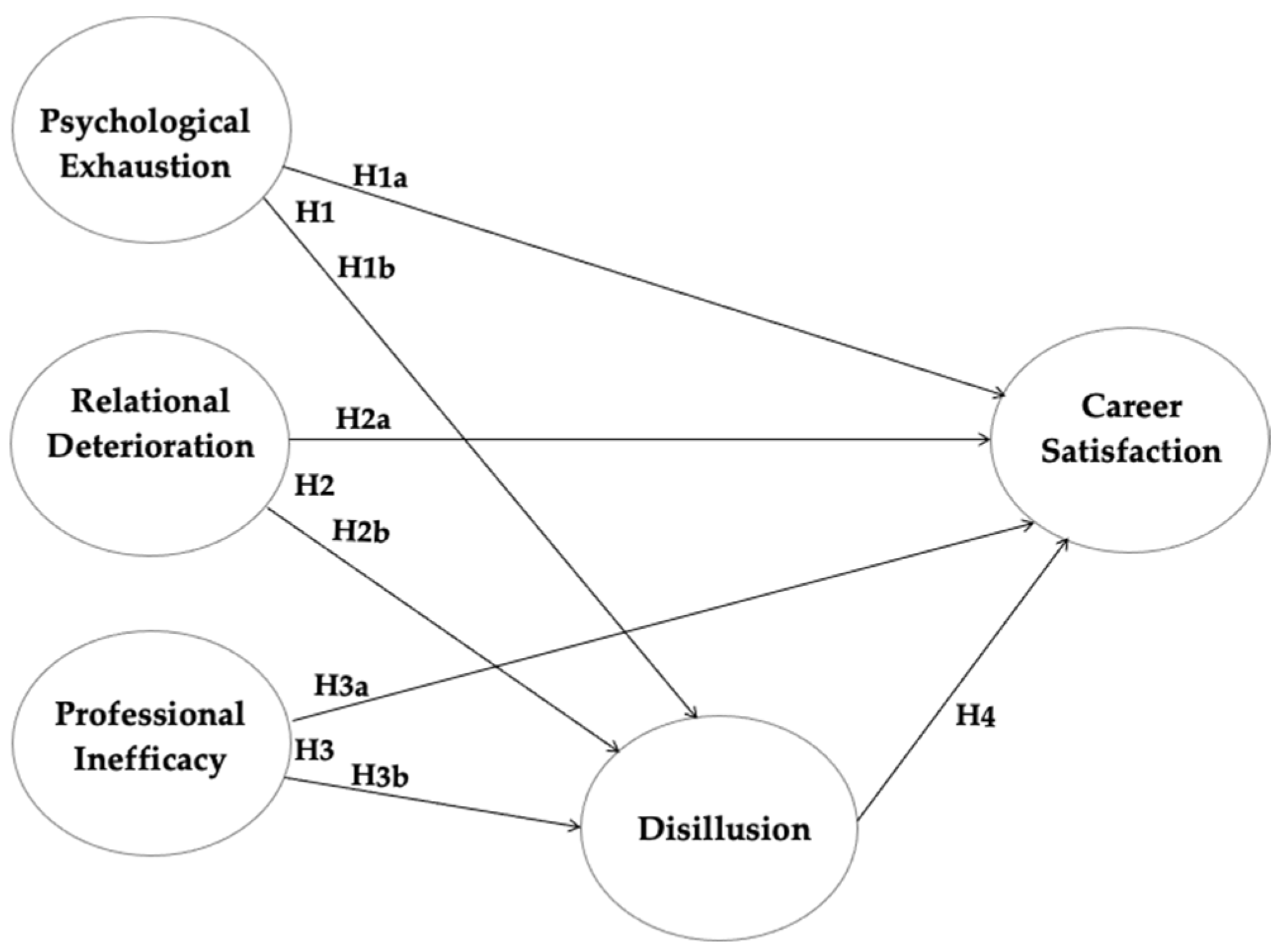
1.5. Aim and Hypotheses
2. Materials and Methods
2.1. Research Design
2.2. Assessment Instruments
2.3. Participants
2.4. Method and Data Analysis
2.5. Ethical Issues
3. Results
3.1. Burnout, Engagement, Satisfaction, Disillusion, and Fulfilment of Healthcare Professionals
3.2. The PLS-SEM Method
3.3. The PLS-SEM Method
4. Discussion
4.1. Practical Implications
4.2. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maslach, C.; Leiter, M.P.; Schaufeli, W.B. Measuring burnout. In The Oxford Handbook of Organizational Well-Being; Cooper, C.L., Cartwright, S., Eds.; Oxford University Press: Oxford, UK, 2009; pp. 86–108. [Google Scholar]
- Schaufeli, W.B. Burnout: A short socio-cultural history. In Burnout, Fatigue, Exhaustion; Neckel, S., Schaffner, A., Wagner, G., Eds.; Palgrave Macmillan: Cham, Switzerland, 2017; pp. 105–127. [Google Scholar]
- Nadon, L.; De Beer, L.T.; Morin, A.J.S. Should Burnout Be Conceptualized as a Mental Disorder? Behav. Sci. 2022, 12, 82. [Google Scholar] [CrossRef] [PubMed]
- Schaufeli, W.B. Burnout: A Critical Overview. In Organizational Stress and Well-Being; Lapierre, L.M., Cooper, C., Eds.; Cambridge University Press: Cambridge, UK, 2023; pp. 214–259. [Google Scholar]
- Schaufeli, W.B. Applying the Job Demands-Resources model: A ‘how to’ guide to measuring and tackling work engagement and burnout. Organ. Dyn. 2017, 46, 120–132. [Google Scholar] [CrossRef]
- Hu, Q.; Schaufeli, W.B.; Taris, T.W. How are changes in exposure to job demands and job resources related to burnout and engagement? A longitudinal study among Chinese nurses and police officers. Stress Health 2017, 33, 631–644. [Google Scholar] [CrossRef] [PubMed]
- Rattrie, L.T.; Kittler, M.G.; Paul, K.I. Culture, burnout, and engagement: A meta-analysis on national cultural values as moderators in JD-R theory. Appl. Psychol. 2020, 69, 176–220. [Google Scholar] [CrossRef]
- Schaufeli, W.B. Work Engagement. What Do We Know and Where Do We Go? Rom. J. Appl. Psychol. 2012, 14, 3–10. [Google Scholar]
- Schaufeli, W.B.; Bakker, A.B. Defining and measuring work engagement: Bringing clarity to the concept. In Work Engagement: A Handbook of Essential Theory and Research; Bakker, A.B., Leiter, M.P., Eds.; Psychology Press: London, UK, 2010; pp. 10–24. [Google Scholar] [CrossRef]
- Hakanen, J.J.; Ropponen, A.; Schaufeli, W.B.; De Witte, H. Who is engaged at work? A large-scale study in 30 European countries. J. Occup. Environ. Med. 2019, 61, 373–381. [Google Scholar] [CrossRef]
- Schaufeli, W.B. Engaging leadership: How to promote work engagement? Front. Psychol. 2021, 12, 754556. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Bakker, A.B.; van Rhenen, W. How changes in job demands and resources predict burnout, work engagement, and sickness absenteeism. J. Organ. Behav. 2009, 30, 893–917. [Google Scholar] [CrossRef]
- Hakanen, J.J.; Schaufeli, W.B. Do burnout and work engagement predict depressive symptoms and life satisfaction? A three-wave seven-year prospective study. J. Affect. Disord. 2012, 141, 415–424. [Google Scholar] [CrossRef]
- Nonnis, M.; Pirrone, M.P.; Cuccu, S.; Agus, M.; Pedditzi, M.L.; Cortese, C.G. Burnout syndrome in reception systems for illegal immigrants in the Mediterranean. A quantitative and qualitative study of Italian practitioners. Sustainability 2020, 12, 5145. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Bakker, A.B. Work Engagement: A Critical Assessment of the Concept and Its Measurement. In Handbook of Positive Psychology Assessment; Tuch, W.R., Bakker, A.B., Tay, L., Gander, F., Eds.; Hogrefe: Göttingen, Germany, 2022; pp. 273–295. [Google Scholar]
- World Health Organization (WHO). International Classification of Diseases (ICD-11). Available online: https://icd.who.int/browse11/l-m/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f129180281 (accessed on 15 September 2023).
- Rožman, M.; Grinkevich, A.; Tominc, P. Occupational stress, symptoms of burnout in the workplace and work satisfaction of the age-diverse employees. Organizacija 2019, 52, 46–59. [Google Scholar] [CrossRef]
- Quiceno, J.M.; Alpi, S.V. Burnout: “Syndrome of burning oneself out at work (SBW)”. Acta Colomb. De Psicol. 2007, 10, 117–125. [Google Scholar]
- Trigo, T.R.; Teng, C.T.; Hallak, J.E.C. Burnout syndrome and psychiatric disorders. Arch. Clin. Psychiatry 2007, 34, 223–233. [Google Scholar] [CrossRef]
- Balan, S.A.; Bubenek-Turconi, Ş.I.; Droc, G.; Marinescu, E.; Nita, E.; Popa, M.C.; Popescu-Spineni, D.; Tomescu, D. Burnout syndrome in the Anaesthesia and Intensive Care Unit. Rom. J. Anaesth. Intensive Care 2019, 26, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Jarosz, K.; Zborowska, A.; Młynarska, A. Rationing Care, Job Satisfaction, Fatigue and the Level of Professional Burnout of Nurses in Urology Departments. Int. J. Environ. Res. Public Health 2022, 19, 8625. [Google Scholar] [CrossRef]
- Witczak-Błoszyk, K.; Krysińska, K.; Andriessen, K.; Stańdo, J.; Czabański, A. Work-Related Suicide Exposure, Occupational Burnout, and Coping in Emergency Medical Services Personnel in Poland. Int. J. Environ. Res. Public Health 2022, 19, 1156. [Google Scholar] [CrossRef]
- van Mol, M.M.C.; Nijkamp, M.D.; Bakker, A.B.; Schaufeli, W.B.; Kompanje, E.J.O. Counterbalancing work-related stress? Work engagement among intensive care professionals. Austr. Crit. Care 2018, 31, 234–241. [Google Scholar] [CrossRef]
- Poelmann, F.B.; Koëter, T.; Steinkamp, P.J.; Vriens, M.R.; Verhoeven, B.; Kruijff, S. The immediate impact of the coronavirus disease 2019 (COVID-19) pandemic on burn-out, work-engagement, and surgical training in The Netherlands. Surgery 2021, 170, 719–726. [Google Scholar] [CrossRef]
- Liu, D.; Chen, Y.; Li, N. Tackling the negative impact of COVID-19 on work engagement and taking charge: A multi-study investigation of frontline health workers. J. Appl. Psychol. 2021, 106, 185–198. [Google Scholar] [CrossRef]
- Alanazy, A.R.M.; Alruwaili, A. The Global Prevalence and Associated Factors of Burnout among Emergency Department Healthcare Workers and the Impact of the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Healthcare 2023, 11, 2220. [Google Scholar] [CrossRef]
- Salari, N.; Khazaie, H.; Hosseinian-Far, A.; Khaledi-Paveh, B.; Kazeminia, M.; Mohammadi, M.; Shohaimi, S.; Daneshkhah, A.; Eskandari, S. The prevalence of stress, anxiety and depression within front-line healthcare workers caring for COVID-19 patients: A systematic review and meta-regression. Hum. Resour. Health 2020, 18, 100. [Google Scholar] [CrossRef] [PubMed]
- Shiu, C.; Chen, W.T.; Hung, C.C.; Huang, E.P.C.; Lee, T.S.H. COVID-19 stigma associates with burnout among healthcare providers: Evidence from Taiwanese physicians and nurses. J. Formos. Med. Assoc. 2022, 121, 1384–1391. [Google Scholar] [CrossRef] [PubMed]
- Prasad, K.; McLoughlin, C.; Stillman, M.; Poplau, S.; Goelz, E.; Taylor, S.; Nankivil, N.; Brown, R.; Linzer, M.; Cappelucci, K.; et al. Prevalence and correlates of stress and burnout among U.S. healthcare workers during the COVID-19 pandemic: A national cross-sectional survey study. eClinicalMedicine 2021, 35, 100879. [Google Scholar] [CrossRef]
- Bafei, S.E.C.; Chen, J.; Qian, Y.; Yuan, L.; Zhou, Y.; Sambou, M.L.; Walker, A.N.; Li, W.; Liu, S. The Association between Burnout, Social Support, and Psychological Capital among Primary Care Providers in Togo: A Cross-Sectional Study. Medicina 2023, 59, 175. [Google Scholar] [CrossRef] [PubMed]
- Luthans, F.; Youssef-Morgan, C.M. Psychological Capital: An Evidence-Based Positive Approach. Annu. Rev. Organ. Psychol. Organ. Behav. 2017, 4, 339–366. [Google Scholar] [CrossRef]
- Barello, S.; Palamenghi, L.; Graffigna, G. Burnout and somatic symptoms among frontline healthcare professionals at the peak of the Italian COVID-19 pandemic. Psychiatry Res. 2020, 290, 113129. [Google Scholar] [CrossRef] [PubMed]
- Santinello, M.; Negrisolo, A. Quando Ogni Passione è Spenta. La Sindrome del Burnout nelle Professioni Sanitarie; Mc Graw Hill: Milan, Italy, 2009; pp. 5–34. [Google Scholar]
- Borgogni, L.; Consiglio, C.; Alessandri, G.; Schaufeli, W.B. “Don’t throw the baby out with the bathwater!” Interpersonal strain at work and burnout. Eur. J. Work Organ. Psychol. 2012, 21, 875–898. [Google Scholar] [CrossRef]
- Nonnis, M.; Massidda, D.; Cuccu, S.; Cortese, C.G. The impact of workaholism on nurses’ burnout and disillusion. Open Psychol. J. 2018, 11, 77–88. [Google Scholar] [CrossRef]
- Edelwich, J.; Brodsky, A. Burnout: Stages of Disillusionment in the Helping Professions; Human Sciences Press: New York, NY, USA, 1981. [Google Scholar]
- Pines, A.; Aronson, E.; Kafry, D. Burnout: From Tedium to personal Growth; The free Press: New York, NY, USA, 1981. [Google Scholar]
- Pedditzi, M.L.; Nonnis, M. Psycho-social sources of stress and burnout in schools: Research on a sample of Italian teachers. Med. Lav. 2014, 105, 48–62. [Google Scholar]
- Nonnis, M.; Agus, M.; Frau, G.; Urban, A.; Cortese, C.G. Job Seekers’ Burnout and Engagement: A Qualitative Study of Long-Term Unemployment in Italy. Int. J. Environ. Res. Public Health 2023, 20, 5968. [Google Scholar] [CrossRef]
- Nonnis, M.; Frau, G.; Agus, M.; Urban, A.; Cortese, C.G. Burnout without a job: An explorative study on a sample of Italian unemployed jobseekers. J. Public Health Res. 2023, 12, 22799036221149260. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.; Gunderman, R.B. Enhancing the Professional Fulfillment of Physicians. Acad. Med. 2006, 81, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Simons, G.; Baldwin, D.S. A critical review of the definition of ‘wellbeing’ for doctors and their patients in a post COVID-19 era. Int. J. Soc. Psychiatry 2021, 67, 984–991. [Google Scholar] [CrossRef] [PubMed]
- Bellieni, C.V.; Righetti, P.; Ciampa, R.; Iacoponi, F.; Coviello, C.; Buonocore, G. Assessing burnout among neonatologists. J. Matern. Fetal Neonatal Med. 2012, 25, 2130–2134. [Google Scholar] [CrossRef] [PubMed]
- Ruggieri, V.; Zeppegno, P.; Gramaglia, C.; Gili, S.; Deantonio, L.; Krengli, M. A survey of Italian radiation oncologists: Job satisfaction and burnout. Tumori 2014, 100, 307–314. [Google Scholar] [CrossRef] [PubMed]
- While, A.; Blackman, C. Reflections on nursing as a career choice. J. Nurs. Manag. 1998, 6, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Rognstad, M.K.; Aasland, O. Change in career aspirations and job values from study time to working life. J. Nurs. Manag. 2007, 15, 424–432. [Google Scholar] [CrossRef]
- Newton, J.M.; Kelly, C.M.; Kremser, A.K.; Jolly, B.; Billett, S. The motivations to nurse: An exploration of factors amongst undergraduate students, registered nurses and nurse managers. J. Nurs. Manag. 2009, 17, 392–400. [Google Scholar] [CrossRef]
- Schrijver, I.; Brady, K.J.; Trockel, M. An exploration of key issues and potential solutions that impact physician wellbeing and professional fulfillment at an academic center. PeerJ 2016, 4, e1783. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Bakker, A.B.; van der Heijden, F.M.M.A.; Prins, J.T. Workaholism, burnout and well-being among junior doctors: The mediating role of role conflict. Work Stress 2009, 23, 155–172. [Google Scholar] [CrossRef]
- Martínez-López, J.A.; Lázaro-Pérez, C.; Gómez-Galán, J. Burnout among Direct-Care Workers in Nursing Homes during the COVID-19 Pandemic in Spain: A Preventive and Educational Focus for Sustainable Workplaces. Sustainability 2021, 13, 2782. [Google Scholar] [CrossRef]
- Jung, F.U.; Bodendieck, E.; Bleckwenn, M.; Hussenoeder, F.S.; Luppa, M.; Riedel-Heller, S.G. Burnout, work engagement and work hours—how physicians’ decision to work less is associated with work-related factors. BMC Health Serv. Res. 2023, 23, 157. [Google Scholar] [CrossRef]
- Lyubarova, R.; Salman, L.; Rittenberg, E. Gender Differences in Physician Burnout: Driving Factors and Potential Solutions. Perm. J. 2023, 27, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Spector, P.E. Job Satisfaction: Application, Assessment, Causes, and Consequences; SAGE Publications Inc.: Thousand Oaks, CA, USA, 1997. [Google Scholar]
- Arifin, J.; Raharjo, T.J. Analysis of the Organizational Climate Factors on the Service Quality and Work Satisfaction towards Lecturer’s Work Commitments in the Specialist’s Medical Education Program at Universitas Diponegoro Semarang. In Proceedings of the 6th International Conference on Science, Education and Technology (ISET 2020), Semarang, Indonesia, 9 September 2020; Atlantis Press: Amsterdam, The Netherlands, 2021; pp. 545–548. [Google Scholar] [CrossRef]
- Meilianti, S.; Matuluko, A.; Ibrahim, N.; Uzman, N.; Bates, I. A global study on job and career satisfaction of early-career pharmacists and pharmaceutical scientists. Explor. Res. Clin. Soc. Pharm. 2022, 5, 100110. [Google Scholar] [CrossRef] [PubMed]
- De Simone, S.; Vargas, M.; Servillo, G. Organizational strategies to reduce physician burnout: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2019, 33, 883–894. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Misra, R.; Madan, R. The Saviors Are Also Humans’: Understanding the Role of Quality of Work Life on Job Burnout and Job Satisfaction Relationship of Indian Doctors. J. Health Manag. 2019, 21, 210–229. [Google Scholar] [CrossRef]
- Keller, E.; Widestrom, M.; Gould, J.; Fang, R.; Davis, K.G.; Gillespie, G.L. Examining the Impact of Stressors during COVID-19 on Emergency Department Healthcare Workers: An International Perspective. Int. J. Environ. Res. Public Health 2022, 19, 3730. [Google Scholar] [CrossRef]
- Selič-Zupančič, P.; Klemenc-Ketiš, Z.; Onuk Tement, S. The Impact of Psychological Interventions with Elements of Mindfulness on Burnout and Well-Being in Healthcare Professionals: A Systematic Review. J. Multidiscip. Healthc. 2023, 16, 1821–1831. [Google Scholar] [CrossRef]
- Kuhn, G.; Goldberg, R.; Compton, S. Tolerance for uncertainty, burnout, and satisfaction with the career of emergency medicine. Ann. Emerg. Med. 2009, 54, 106–113. [Google Scholar] [CrossRef]
- Santinello, M. Link Burnout Questionnaire—LBQ; Giunti O.S. Organizzazioni Speciali: Firenze, Italia, 2007. [Google Scholar]
- Sirigatti, S.; Stefanile, C. OSI: Occupational Stress Indicator; Giunti O.S. Organizzazioni Speciali: Firenze, Italia, 2002. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; Guilford Publications: New York, NY, USA, 2023. [Google Scholar]
- Hair, J.; Tatham, R.L.; Anderson, R.E.; Black, W. Multivariate Data Analysis; Pearson Prentice Hall: Upper Saddle River, NJ, USA, 2006; Volume 6. [Google Scholar]
- Hair, J.F.; Risher, J.J.; Sarstedt, M.; Ringle, C.M. When to use and how to report the results of PLS-SEM. Eur. Bus. Rev. 2019, 31, 2–24. [Google Scholar] [CrossRef]
- Sarstedt, M.; Ringle, C.; Hair, J. Partial Least Squares Structural Equation Modeling; Springer Nature Switzerland: Cham, Switzerland, 2021; pp. 1–47. [Google Scholar] [CrossRef]
- Esposito Vinzi, V.; Chin, W.W.; Henseler, J.; Wang, H. Handbook of Partial Least Squares: Concepts, Methods and Applications; Springer Handbooks of Computational Statistics; Springer: Berlin/Heidelberg, Germany, 2010. [Google Scholar] [CrossRef]
- Hair, J.F., Jr.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M.; Danks, N.P.; Ray, S. Evaluation of Reflective Measurement Models. Partial Least Squares Structural Equation Modeling (PLS-SEM) Using R: A Workbook; Springer: Berlin/Heidelberg, Germany, 2021; pp. 75–90. [Google Scholar]
- The Jamovi Project, Version 2.3; Jamovi: Sydney, Australia, 2023. Available online: https://www.jamovi.org (accessed on 2 November 2023).
- Ringle, C.M.; Wende, S.; Becker, J.M. SmartPLS 4, Version 4; SmartPLS: Oststeinbek, Germany, 2022. Available online: https://www.smartpls.com (accessed on 2 November 2023).
- Hair, J.F.; Sarstedt, M.; Pieper, T.M.; Ringle, C.M. The Use of Partial Least Squares Structural Equation Modeling in Strategic Management Research: A Review of Past Practices and Recommendations for Future Applications. Long. Range Plann. 2012, 45, 320–340. [Google Scholar] [CrossRef]
- Hair, J.F., Jr.; Sarstedt, M.; Ringle, C.M.; Gudergan, S.P. Advanced Issues in Partial Least Squares Structural Equation Modeling; SAGE Publications Inc.: New York, NY, USA, 2023. [Google Scholar]

{kind=link}
{kind=link}
| Latent Construct | Variable Loadings | Dijkstra-Henseler’s Rho A | Cronbach’s Alpha | Average Variance Extracted (AVE) | Adjusted R2 |
|---|---|---|---|---|---|
| Psychophysical exhaustion | From 0.755 to 0.832 | 0.894 | 0.891 | 0.647 | |
| Relational deterioration | From 0.308 to 0.774 | 0.761 | 0.703 | 0.417 | |
| Professional inefficacy | From 0.528 to 0.767 | 0.773 | 0.761 | 0.459 | |
| Disillusion | From 0.544 to 0.888 | 0.903 | 0.844 | 0.645 | 0.738 |
| Career satisfaction | From 0.637 to 0.887 | 0.882 | 0.872 | 0.619 | 0.564 |
| HTMT Coefficient | |
|---|---|
| Psychophysical exhaustion <-> Career satisfaction | 0.790 |
| Psychophysical exhaustion <-> Disillusion | 0.936 |
| Psychophysical exhaustion <-> Relational deterioration | 0.726 |
| Psychophysical exhaustion <-> Professional inefficacy | 0.806 |
| Relational deterioration <-> Professional inefficacy | 0.720 |
| Relational deterioration <-> Career satisfaction | 0.676 |
| Relational deterioration <-> Disillusion | 0.781 |
| Professional inefficacy <-> Career satisfaction | 0.647 |
| Professional inefficacy <-> Disillusion | 0.798 |
| Career satisfaction <-> Disillusion | 0.836 |
| VIF | |
|---|---|
| Psychophysical exhaustion -> Disillusion | 2.097 |
| Psychophysical exhaustion -> Career satisfaction | 3.801 |
| Relational deterioration -> Disillusion | 1.670 |
| Relational deterioration -> Career satisfaction | 1.804 |
| Professional inefficacy -> Disillusion | 1.965 |
| Professional inefficacy -> Career satisfaction | 2.001 |
| Disillusion -> Career satisfaction | 3.857 |
| Relationship | F-Square |
|---|---|
| Psychophysical exhaustion -> Disillusion | 0.812 |
| Psychophysical exhaustion -> Career satisfaction | 0.036 |
| Relational deterioration -> Career satisfaction | 0.013 |
| Relational deterioration -> Disillusion | 0.080 |
| Professional inefficacy -> Disillusion | 0.018 |
| Professional inefficacy -> Career satisfaction | 0.000 |
| Disillusion -> Career satisfaction | 0.129 |
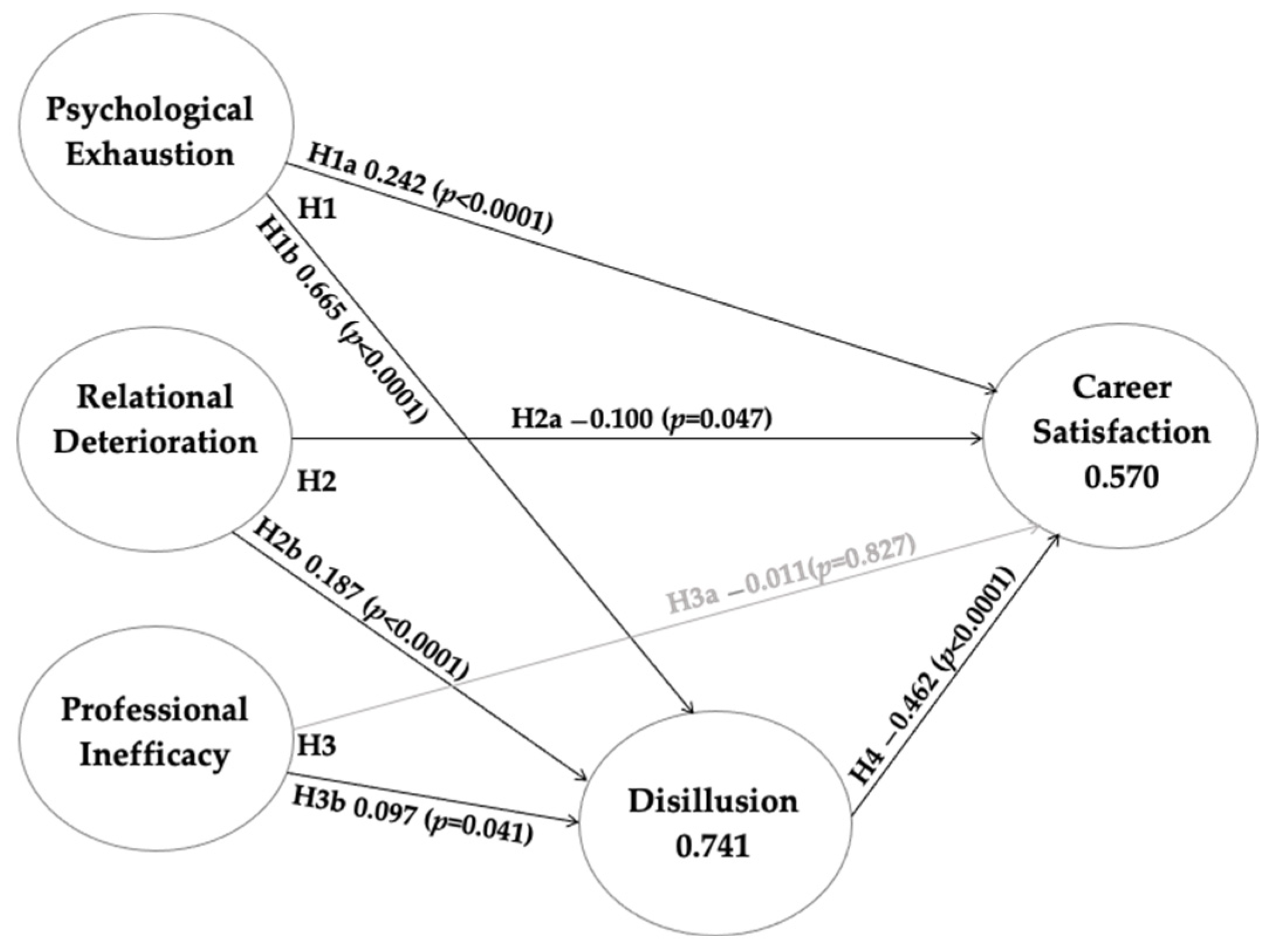
| Hypothesis | Relationship | Standardized Beta | Standard Deviation | T-Value | p-Value | Decision |
|---|---|---|---|---|---|---|
| Direct paths | ||||||
| H1a | Psychophysical exhaustion -> Career satisfaction | −0.242 | 0.080 | 3.011 | 0.003 | Supported |
| H1b | Psychophysical exhaustion -> Disillusion | 0.665 | 0.042 | 15.855 | <0.001 | Supported |
| H2a | Relational deterioration -> Career satisfaction | −0.100 | 0.050 | 1.991 | 0.047 | Supported |
| H2b | Relational deterioration -> Disillusion | 0.187 | 0.044 | 4.284 | <0.001 | Supported |
| H3a | Professional inefficacy -> Career satisfaction | −0.011 | 0.052 | 0.219 | 0.827 | NOT supported |
| H3b | Professional inefficacy -> Disillusion | 0.097 | 0.047 | 2.048 | 0.041 | Supported |
| H4 | Disillusion -> Career satisfaction | −0.462 | 0.078 | 5.889 | <0.001 | Supported |
| Specific indirect effects | ||||||
| H1 | Psychophysical exhaustion -> Disillusion -> Career satisfaction | −0.307 | 0.056 | 5.492 | <0.001 | Supported |
| H2 | Relational deterioration -> Disillusion -> Career satisfaction | −0.086 | 0.024 | 3.583 | <0.001 | Supported |
| H3 | Professional inefficacy -> Disillusion -> Career satisfaction | −0.045 | 0.024 | 1.896 | 0.058 | NOT supported |
| Total effects | ||||||
| H1 | Psychophysical exhaustion -> Career satisfaction | −0.549 | 0.055 | 9.937 | <0.001 | Supported |
| H2 | Relational deterioration -> Career satisfaction | −0.187 | 0.051 | 3.639 | <0.001 | Supported |
| H3 | Professional inefficacy -> Career satisfaction | −0.056 | 0.057 | 0.984 | 0.325 | NOT supported |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nonnis, M.; Agus, M.; Corona, F.; Aru, N.; Urban, A.; Cortese, C.G. The Role of Fulfilment and Disillusion in the Relationship between Burnout and Career Satisfaction in Italian Healthcare Workers. Sustainability 2024, 16, 893. https://doi.org/10.3390/su16020893
Nonnis M, Agus M, Corona F, Aru N, Urban A, Cortese CG. The Role of Fulfilment and Disillusion in the Relationship between Burnout and Career Satisfaction in Italian Healthcare Workers. Sustainability. 2024; 16(2):893. https://doi.org/10.3390/su16020893
Chicago/Turabian StyleNonnis, Marcello, Mirian Agus, Francesca Corona, Nicola Aru, Antonio Urban, and Claudio Giovanni Cortese. 2024. "The Role of Fulfilment and Disillusion in the Relationship between Burnout and Career Satisfaction in Italian Healthcare Workers" Sustainability 16, no. 2: 893. https://doi.org/10.3390/su16020893
APA StyleNonnis, M., Agus, M., Corona, F., Aru, N., Urban, A., & Cortese, C. G. (2024). The Role of Fulfilment and Disillusion in the Relationship between Burnout and Career Satisfaction in Italian Healthcare Workers. Sustainability, 16(2), 893. https://doi.org/10.3390/su16020893