System Dynamics Modeling for Assessing the Impact of COVID-19 on Food Supply Chains: A Case Study of Kenya and Rwanda

 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. General Overview
2.2. Key Assumptions
- The population is homogenous and well mixed, with no significant changes to the total population due to births, deaths, or migration.
- At the initial stage, the disease is assumed to be imported to the country through arriving passengers only.
- Lockdown reduces the mobility of labor, and this directly increases the number of people unemployed.
- The infectiousness of an individual is not uniform between exposure and recovery.
- The infectiousness of asymptomatic individuals is lower than that of symptomatic individuals.
- Weather and climatic conditions play no role in disease infectiousness in the selected region.
- The incubation period is 14 days. This is the time it takes patients infected with COVID-19 to show symptoms [24].
- The recovery rate is represented by a first-order variable, meaning that for a given population of infectious individuals, an exponential decline will occur, while a portion of the population will recover faster than others.
- Asymptomatic individuals may recover without even going to the hospital. Similarly, this recovery mechanism is applied to the portion of the population who received vaccines.
- Every phase of the infection has delays; for example, there is a delay in showing symptoms of COVID-19 (delay of asymptomatic recovery = 11 days).
- The fatality rate is increased by delays in seeking treatment or prior conditions of the patient, such as respiratory diseases.
- The rate of vaccination in Eastern African countries is still low and undetermined.
- The current vaccine reduces the severity of disease but not susceptibility.
- Variants of COVID-19 are not considered. The rate of infection differs among variants.
- Females and males were influenced differently by COVID-19, which in certain situations, contributed to an increase in gender-based violence [20]. However, we did not account for gender differences.
- Nutrition security is viewed as the availability of food to nourish the household.
2.3. Datasets
2.4. Model Implementation and Simulation Experiments
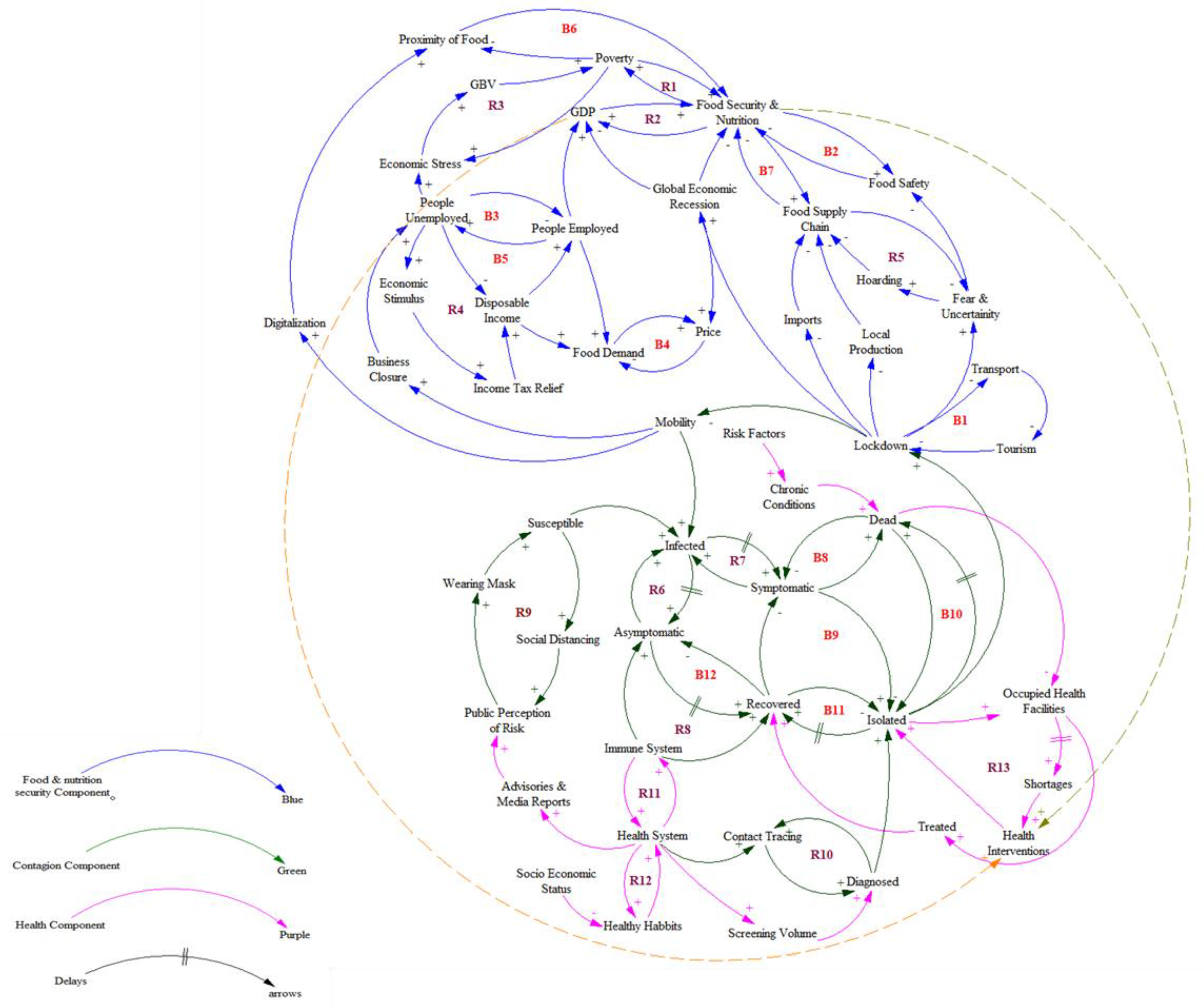
2.5. Causal Loop Diagram (CLD) Elicitation
2.6. Converting the Causal Loop Diagram (CLD) to Stock and Flow Diagrams
2.6.1. The Stock and Flow Diagram for the Contagion Component of the COVID-19 Pandemic
2.6.2. The Stock and Flow Diagram for the Health Component of the COVID-19 Pandemic
2.6.3. The Stock and Flow Diagram for the Food Security and Nutrition Component of the COVID-19 Pandemic
2.7. Case Studies: Kenya and Rwanda
3. Results
3.1. Reported COVID-19 Cases, Hospitalizations, Recoveries, and Deaths
3.2. Impact of COVID-19 on Food and Nutritional Security
3.3. Sensitivity Analysis
4. Discussion
5. Conclusions and Policy Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B
| DELAY PARAMETERS | |
| Latency period, dLP | 3 Days |
| Incubation period, dIP | 5 Days |
| Developing symptoms period, dDP | 2 Days |
| Asymptomatic recovery period, dAP | 11 Days |
| Infectious asymptomatic to become serious / hospitalize, dIH | 5 Days |
| Symptomatic recovery period, dSP | 14 Days |
| Worsening duration, dWD | 5 Days |
| Hospitalized patient recovery period, dHP | 14 Days |
| Period for critical patient to die, dPD | 5 Days |
| Period for critical patients to recover, dPR | 14 Days |
| Quarantine period/Isolate asymptomatic, dQIA | 1 Day |
| Quarantine period/Isolate symptomatic, dQIS | 2.5 Days |
| Quarantine period/Isolate symptomatic to | 1 Day develop symptoms, dQISD |
| Quarantine period/Isolate symptomatic to | 2.5 Days become serious, dQISB |
| Quarantine period/isolate asymptomatic to | 10 Days recover, dQIAR |
| Quarantine period/Isolate symptomatic to | 13 Days become serious/hospitalize, dQISBH |
| SCORES | |
| Food availability score | 41.8% |
| Food access score | 53.2% |
| Food utilization score | 58.6% |
| Food nutritional security (initial) | 49.0% |
References
- Al-Ali, N. Covid-19 and feminism in the Global South: Challenges, initiatives and dilemmas. Eur. J. Women’s Stud. 2020, 27, 333–347. [Google Scholar] [CrossRef]
- Clapp, J.; Moseley, W.G. This food crisis is different: COVID-19 and the fragility of the neoliberal food security order. J. Peasant Stud. 2020, 47, 1393–1417. [Google Scholar] [CrossRef]
- Yazdanpanah, M.; Tajeri Moghadam, M.; Savari, M.; Zobeidi, T.; Sieber, S.; Löhr, K. The Impact of Livelihood Assets on the Food Security of Farmers in Southern Iran during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 5310. [Google Scholar] [CrossRef]
- Chirisa, I.; Mutambisi, T.; Chivenge, M.; Mabaso, E.; Matamanda, A.R.; Ncube, R. The urban penalty of COVID-19 lockdowns across the globe: Manifestations and lessons for Anglophone sub-Saharan Africa. GeoJournal 2022, 87, 815–828. [Google Scholar] [CrossRef] [PubMed]
- Berg, S.v.d.; Patel, L.; Bridgman, G. Food insecurity in South Africa: Evidence from NIDS-CRAM wave 5. Dev. S. Afr. 2022, 39, 722–737. [Google Scholar] [CrossRef]
- Tien, N.H.; Anh, D.B.H.; Thuc, T.D. Global Supply Chain and Logistics Management; Academic Publications: Dehli, India, 2019; Volume 162. [Google Scholar]
- Tukamuhabwa, B.; Stevenson, M.; Busby, J. Supply chain resilience in a developing country context: A case study on the interconnectedness of threats, strategies and outcomes. Supply Chain Manag. 2017, 22, 486–505. [Google Scholar] [CrossRef]
- Song, S.; Goh, J.C.; Tan, H.T. Is food security an illusion for cities? A system dynamics approach to assess disturbance in the urban food supply chain during pandemics. Agric. Syst. 2021, 189, 103045. [Google Scholar] [CrossRef]
- Ceballos, F.; Kannan, S.; Kramer, B. Impacts of a national lockdown on smallholder farmers’ income and food security: Empirical evidence from two states in India. World Dev. 2020, 136, 105069. [Google Scholar] [CrossRef]
- Swinnen, J.; McDermott, J. COVID-19 and global food security. EuroChoices 2020, 19, 26–33. [Google Scholar] [CrossRef]
- Béné, C.; Bakker, D.; Chavarro, M.J.; Even, B.; Melo, J.; Sonneveld, A. Global assessment of the impacts of COVID-19 on food security, Glob. Food Secur. 2021, 31, 100575. [Google Scholar] [CrossRef]
- Sánchez, M.V.; Cicowiez, M.; Ortega, A. Prioritizing public investment in agriculture for post-COVID-19 recovery: A sectoral ranking for Mexico. Food Policy 2022, 109, 102251. [Google Scholar] [CrossRef]
- Nechifor, V.; Ramos, M.P.; Ferrari, E.; Laichena, J.; Kihiu, E.; Omanyo, D.; Musamali, R.; Kiriga, B. Food security and welfare changes under COVID-19 in Sub-Saharan Africa: Impacts and responses in Kenya. Glob. Food Secur. 2021, 28, 100514. [Google Scholar] [CrossRef] [PubMed]
- Liguori, J.; Trübswasser, U.; Pradeilles, R.; Le Port, A.; Landais, E.; Talsma, E.F.; Lundy, M.; Bene, C.; Bricas, N.; Laar, A.; et al. How do food safety concerns affect consumer behaviors and diets in low- and middle-income countries? A systematic review. Glob. Food Secur. 2022, 32, 100606. [Google Scholar] [CrossRef]
- Nchanji, E.B.; Lutomia, C.K. Regional impact of COVID-19 on the production and food security of common bean smallholder farmers in Sub-Saharan Africa: Implication for SDG’s. Glob. Food Secur. 2021, 29, 100524. [Google Scholar] [CrossRef] [PubMed]
- Di Vaio, A.; Boccia, F.; Landriani, L.; Palladino, R. Artificial Intelligence in the Agri-Food System: Rethinking Sustainable Business Models in the COVID-19 Scenario. Sustainability 2020, 12, 4851. [Google Scholar] [CrossRef]
- D’Amore, G.; Di Vaio, A.; Balsalobre-Lorente, D.; Boccia, F. Artificial Intelligence in the Water–Energy–Food Model: A Holistic Approach towards Sustainable Development Goals. Sustainability 2022, 14, 867. [Google Scholar] [CrossRef]
- Turner, J.R.; Baker, R.M. Complexity Theory: An Overview with Potential Applications for the Social Sciences. Systems 2019, 7, 4. [Google Scholar] [CrossRef]
- Alexander, F.S.; Yaneer, B.-Y. An introduction to complex systems science and its applications. Complexity 2020, 2020, 6105872. [Google Scholar]
- Siringi, E.M. Analysis of Economic Effect of COVID-19 Pandemic on the Kenyan Economy. Afr. Rev. 2020, 49, 38–53. [Google Scholar] [CrossRef]
- Kansiime, M.K.; Tambo, J.A.; Mugambi, I.; Bundi, M.; Kara, A.; Owuor, C. COVID-19 implications on household income and food security in Kenya and Uganda: Findings from a rapid assessment. World Dev. 2021, 137, 104903. [Google Scholar] [CrossRef]
- Sutcliffe, S.; Lau, J.; Barnes, M.L.; Mbaru, E.; Wade, E.; Hungito, W.; Muly, I.; Wanyonyi, S.; Muthiga, N.A.; Cohen, P.J.; et al. COVID-19 impacts on food systems in fisheries-dependent island communities. Ecol. Soc. 2023, 28, 1. [Google Scholar] [CrossRef]
- Picchioni, F.; Goulao, L.F.; Roberfroid, D. The impact of COVID-19 on diet quality, food security and nutrition in low- and middle-income countries: A systematic review of the evidence. Clin. Nutr. 2022, 41, 2955–2964. [Google Scholar] [CrossRef]
- Venkateswaran, J.; Damani, O. Effectiveness of testing, tracing, social distancing and hygiene in tackling COVID-19 in India: A system dynamics model. arXiv 2020, arXiv:2004.08859. [Google Scholar] [CrossRef]
- Kazancoglu, Y.; Ozbiltekin-Pala, M.; Sezer, M.D.; Ekren, B.Y.; Kumar, V. Assessing the Impact of COVID-19 on Sustainable Food Supply Chains. Sustainability 2022, 14, 143. [Google Scholar] [CrossRef]
- Li, S.; Ma, S.; Zhang, J. Building a system dynamics model to analyze scenarios of COVID-19 policymaking in tourism-dependent developing countries: A case study of Cambodia. Tour. Econ. 2022, 29, 13548166211059080. [Google Scholar] [CrossRef]
- Kozlovskyi, S.; Bilenko, D.; Kuzheliev, M.; Lavrov, R.; Kozlovskyi, V.; Mazur, H.; Taranych, A. The system dynamic model of the labor migryant policy in economic growth affected by COVID-19. Glob. J. Environ. Sci. Manag. 2020, 6, 95–106. [Google Scholar]
- Marzouk, M.; Azab, S.; Elshaboury, N.; Megahed, A.; Metawie, M.; El Hawary, M.; Ghaith, D.; Bayoumi, A. Modeling COVID-19 effects on SDGs using system dynamics in Egypt. Environ. Sci. Pollut. Res. 2022, 29, 59235–59246. [Google Scholar] [CrossRef]
- Jia, S.; Li, Y.; Fang, T. System dynamics analysis of COVID-19 prevention and control strategies. Environ. Sci. Pollut. Res. 2022, 29, 3944–3957. [Google Scholar] [CrossRef]
- Shukla, A.; Tomer, N.; Singh, P. System Dynamics Modeling to Understand the Impact of Covid-19 on Indian Economy. Manag. Dyn. 2021, 21, 2. [Google Scholar] [CrossRef]
- Tonnang, H.; Greenfield, J.; Mazzaferro, G.; Austin, C.C.; WG, R. COVID-19 Emergency public health and economic measures causal loops: A computable framework. SSRN 2020. [Google Scholar] [CrossRef]
- Health Policy and Systems Research: A Methodology Reader. Available online: https://apps.who.int/iris/handle/10665/44803 (accessed on 23 July 2021).
- Situation Analysis of Children and Women in Kenya 2017. Available online: https://www.unicef.org/kenya/reports/situation-analysis-children-and-women-kenya-2017 (accessed on 21 July 2021).
- Sokame, B.M.; Tonnang, H.E.Z.; Subramanian, S.; Bruce, A.Y.; Dubois, T.; Ekesi, S.; Calatayud, P.-A. A system dynamics model for pests and natural enemies interactions. Sci. Rep. 2021, 11, 1401. [Google Scholar] [CrossRef]
- Turner, C.; Aggarwal, A.; Walls, H.; Herforth, A.; Drewnowski, A.; Coates, J.; Kalamatianou, S.; Kadiyala, S. Concepts and critical perspectives for food environment research: A global framework with implications for action in low- and middle-income countries. Glob. Food Secur. 2018, 18, 93–101. [Google Scholar] [CrossRef]
- Hannah, S.; Carlos, G.-P.; Nico, S.; Wolfgang, C. QtAC: An R-package for analyzing complex systems development in the framework of the adaptive cycle metaphor. Ecol. Model. 2022, 466, 109860. [Google Scholar] [CrossRef]
- Whegang, Y.S.; Tonnang, Z.E.H.; Choukem, S.P. Modelling and projections of the COVID-19 epidemic and the potential impact of social distancing in Cameroon. J. Public Health Afr. 2022, 12, 1479. [Google Scholar] [CrossRef]
- Impacts of COVID-19 on Food Security and Nutrition: Developing Effective Policy Responses to Address the Hunger and Malnutrition Pandemic. Available online: https://www.researchgate.net/publication/344863122_Impacts_of_COVID-19_on_food_security_and_nutrition_developing_effective_policy_responses_to_address_the_hunger_and_malnutrition_pandemic (accessed on 27 December 2022).
- Arndt, C.; Davies, R.; Gabriel, S.; Harris, L.; Makrelov, K.; Robinson, S.; Levy, S.; Simbanegavi, W.; van Seventer, D.; Anderson, L. Covid-19 lockdowns, income distribution, and food security: An analysis for South Africa. Glob. Food Secur. 2020, 26, 100410. [Google Scholar] [CrossRef]
- The Impact of COVID-19 Control Measures on Social Contacts and Transmission in Kenyan Informal Settlements. Available online: https://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-020-01779-4 (accessed on 12 January 2023).
- Janssens, W.; Pradhan, M.; de Groot, R.; Sidze, E.; Donfouet, H.P.P.; Abajobir, A. The short-term economic effects of COVID-19 on low-income households in rural Kenya: An analysis using weekly financial household data. World Dev. 2021, 138, 105280. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LOOP DESCRIPTION | IMPLICATION | |
| FOOD SECURITY AND NUTRTION COMPONENT | ||
| B1 | Lockdown–transport–tourism–lockdown | Lockdown impacts transport, which reduces tourism |
| B2 | Food security and nutrition–food safety–food security and nutrition | Low rate of food safety reduces food security and nutrition |
| B3 | People employed–people unemployed–people employed | Employment rate reduces unemployment and vice versa |
| B4 | Price–food demand–price | High food demand escalates prices and vice versa |
| B5 | People employed–people unemployed–disposable income–people employed | Disposable income is negatively affected by unemployment |
| B6 | Food security and nutrition–poverty–proximity of food–food security and nutrition | Positive proximity of food results in high food security and nutrition |
| B7 | Food security and nutrition–food supply chain–food security and nutrition | Disrupted food supply chain reduces food security and nutrition and vice versa |
| R1 | Food security and nutrition–poverty–food security and nutrition | Poverty negatively impacts food security and nutrition |
| R2 | Food security and nutrition–GDP–food security and nutrition | High GDP increases food security and nutrition and vice versa |
| R3 | Economic stress–GBV–poverty–economic stress | GBV increases poverty, which impacts economic stress |
| R4 | People unemployed–economic stimulus–income tax relief–disposable income–people employed–people–unemployed | Unemployment induces tax relief, thus increasing disposable income |
| R5 | Food supply chain–fear and uncertainty–hoarding–food supply chain | Fear and uncertainty give rise to hoarding behavior, hurting the food supply chain |
| CONTAGION COMPONENT | ||
| R6 | Asymptomatic–infected–asymptotic | Exponential growth of infected individuals in the population |
| R7 | Infected–symptomatic–infected | Upsurge in number of deceased and isolated individuals |
| R8 | Immune system–asymptomatic–recovered–immune system | Strong immune system increases the number of asymptomatic individuals |
| R9 | Susceptible–social distance–public perception–wearing mask–susceptible | Wearing masks and social distancing increase the number of susceptible individuals |
| R10 | Contact tracing–di agnosed–contact tracing | Contact tracing increases the number of diagnosed individuals |
| B8 | Symptomatic–deceased–symptomatic | Symptomatic individuals after a time delay could die |
| B9 | Recovered–symptomatic–isolated–recovered | Recovered individuals reduce the number of symptomatic individuals |
| B10 | Isolated–deceased–isolated | After delay, a group of isolated individuals died, contributing to increase the number of deceased individuals |
| B11 | Recovered–isolated–recovered | After delay, a group of isolated individuals recovered |
| B12 | Asymptomatic–recovered–asymptomatic | After delay, a group of asymptomatic individuals recovered |
| HEALTH COMPONENT | ||
| R11 | Immune system–health system–immune system | Decent health system enhances immune system |
| R12 | Healthy habits–health system–healthy habits | Healthy habits increase the number of individuals with a strong immune system |
| R13 | Health intervention–isolated–occupied health facilities–shortage–health interventions | More health interventions increase the number of isolated individuals and occupied health facilities, contributing to shortages |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tonnang, H.E.Z.; Sokame, B.M.; Wamalwa, M.; Niassy, S.; Muriithi, B.W. System Dynamics Modeling for Assessing the Impact of COVID-19 on Food Supply Chains: A Case Study of Kenya and Rwanda. Sustainability 2023, 15, 4717. https://doi.org/10.3390/su15064717
Tonnang HEZ, Sokame BM, Wamalwa M, Niassy S, Muriithi BW. System Dynamics Modeling for Assessing the Impact of COVID-19 on Food Supply Chains: A Case Study of Kenya and Rwanda. Sustainability. 2023; 15(6):4717. https://doi.org/10.3390/su15064717
Chicago/Turabian StyleTonnang, Henri E. Z., Bonoukpoè Mawuko Sokame, Mark Wamalwa, Saliou Niassy, and Beatrice Wambui Muriithi. 2023. "System Dynamics Modeling for Assessing the Impact of COVID-19 on Food Supply Chains: A Case Study of Kenya and Rwanda" Sustainability 15, no. 6: 4717. https://doi.org/10.3390/su15064717
APA StyleTonnang, H. E. Z., Sokame, B. M., Wamalwa, M., Niassy, S., & Muriithi, B. W. (2023). System Dynamics Modeling for Assessing the Impact of COVID-19 on Food Supply Chains: A Case Study of Kenya and Rwanda. Sustainability, 15(6), 4717. https://doi.org/10.3390/su15064717