
Implementing Modern Technology for Vital Sign Monitoring to Enhance Athletic Training and Sports Performance



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Materials and Testing
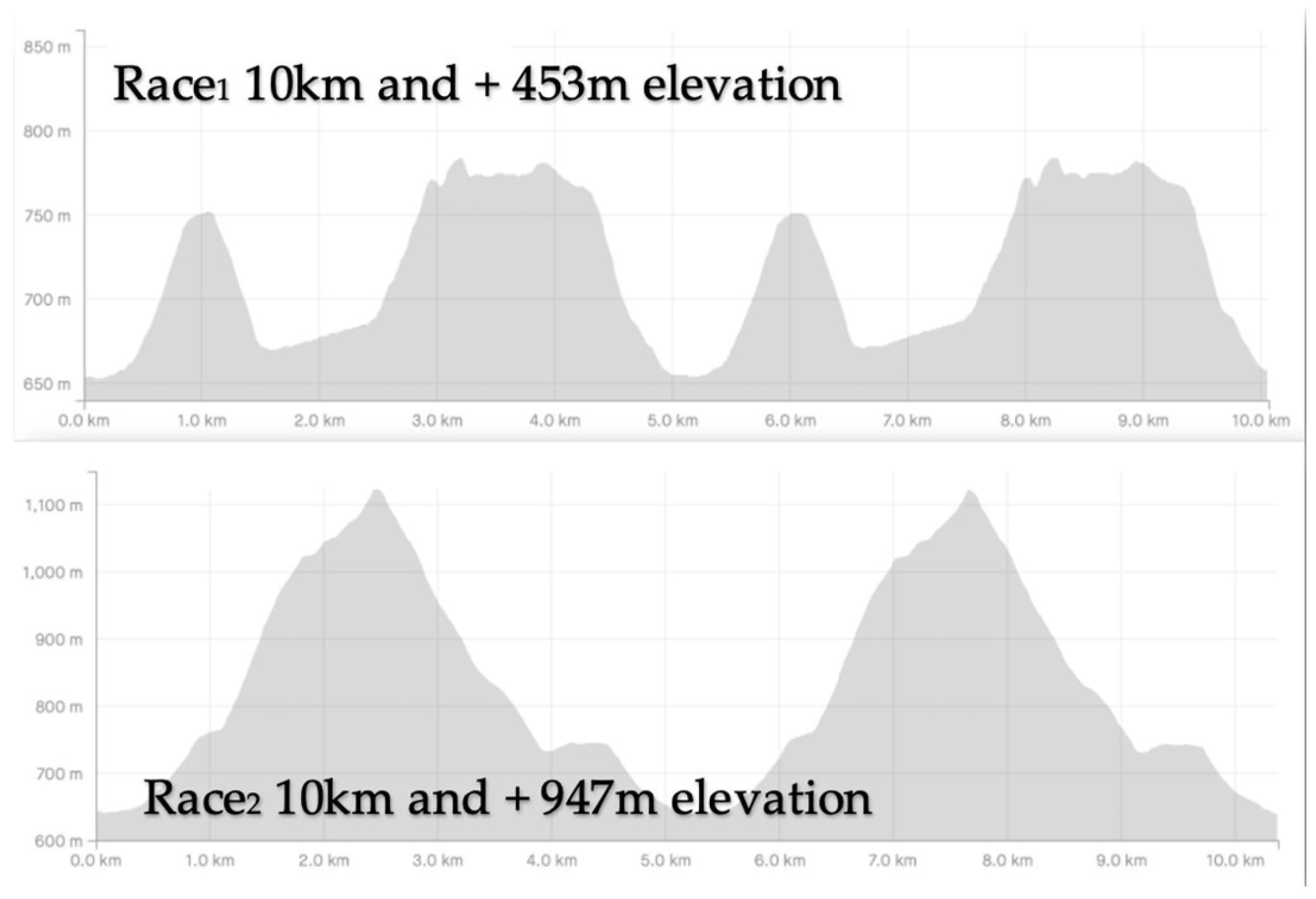
2.3.1. Mountain Running Race, VO2max, Lactate and NeuroTracker Results
2.3.2. EKG Test
2.3.3. MicroAstrup, Biochemical Blood Test and Urine Test
2.3.4. Statistical Analysis
3. Results
3.1. Mountain Running Race, VO2max, Lactate and NeuroTracker Results
3.2. EKG Analysis Results
3.3. Astrup, Biochemical Blood Test and Urine Test Results
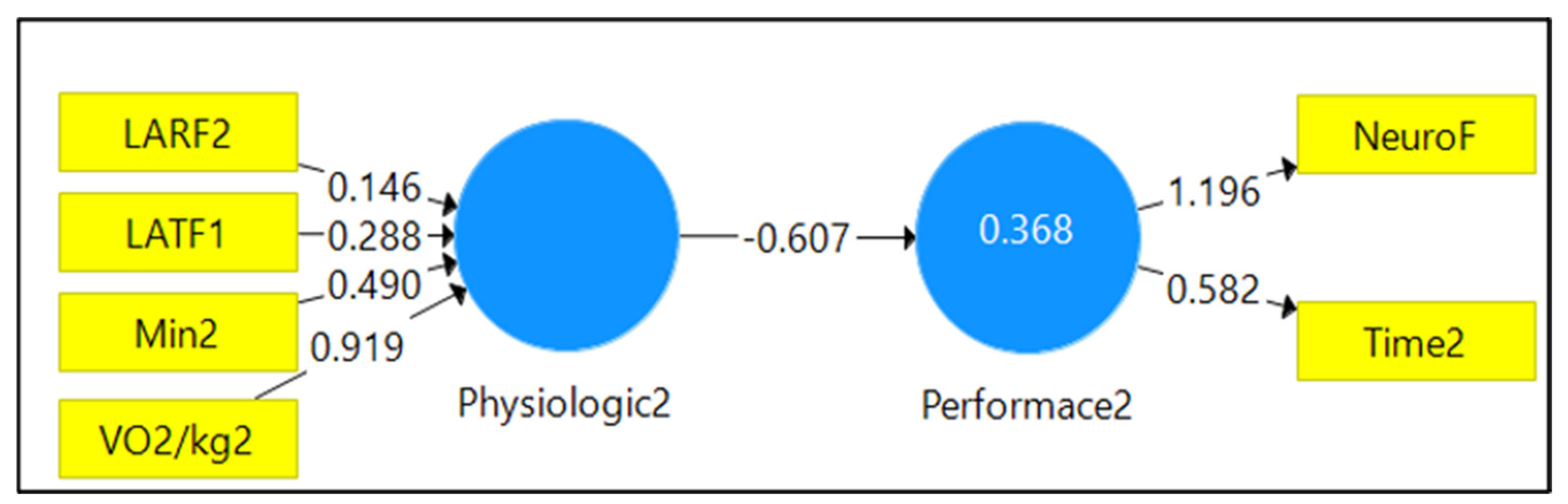
3.4. Factor Analysis Results
Construct Reliability and Validity
3.5. Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations
References
- History wmra.ch. Available online: https://wmra.ch/about-us/history (accessed on 9 December 2021).
- López-García, S.; Muriel-Isidro, J.; Ruibal-Lista, B.; Maneiro, R.; Amatria-Jiménez, M. Review of the Organizational Structures of the Trail Running, Skyrunning and Mountain Running Modalities in Spain. Sustainability 2022, 14, 12401. [Google Scholar] [CrossRef]
- Ketenci, S.; Saraçoğlu, İ.; Duranay, R.; Elgörmüş, Ç.S.; Aynacıoğlu, A.Ş. Retrospective analysis of biochemical markers in COVID-19 intensive care unit patients. Egypt J. Bronchol. 2022, 16, 27. [Google Scholar] [CrossRef]
- Bodys-Pełka, A.; Kusztal, M.; Boszko, M.; Główczyńska, R.; Grabowski, M. Non-Invasive Continuous Measurement of Haemodynamic Parameters—Clinical Utility. J. Clin. Med. 2021, 10, 4929. [Google Scholar] [CrossRef] [PubMed]
- Federatia Romana de Atletism. Available online: https://www.fra.ro/rezultate-2022/ (accessed on 24 October 2022).
- Cousins, S.; Blencowe, N.S.; Blazeby, J.M. What is an invasive procedure? A definition to inform study design, evidence synthesis and research tracking. BMJ Open 2019, 9, e028576. [Google Scholar] [CrossRef]
- Díaz Martínez, A.E.; Alcaide Martín, M.J.; González-Gross, M. Basal Values of Biochemical and Hematological Parameters in Elite Athletes. Int. J. Environ. Res. Public Health 2022, 19, 3059. [Google Scholar] [CrossRef]
- Lankford, D.E.; Jake, T.B.; Keegan, H.; Lex, G.; Tyler, H.; Yilin, W. Validity of Two High-Incline VO2max Protocols for College-Aged Population. Int. J. Sport. Exerc. Med. 2019, 5. [Google Scholar]
- Pero, R.; Brancaccio, M.; Mennitti, C.; Gentile, L.; Arpino, S.; De Falco, R.; Leggiero, E.; Ranieri, A.; Pagliuca, C.; Colicchio, R.; et al. Urinary Biomarkers: Diagnostic Tools for Monitoring Athletes’ Health Status. Int. J. Environ. Res. Public Health 2020, 17, 6065. [Google Scholar] [CrossRef]
- Burns, L.; Weissensteiner, J.R.; Cohen, M.; Bird, S.R. A survey of elite and pre-elite athletes’ perceptions of key support, lifestyle and performance factors. BMC Sport. Sci. Med. Rehabil. 2022, 14, 2. [Google Scholar] [CrossRef]
- Janssen, S.L.; Berge, K.; Luiken, T.; Aengevaeren, V.L.; Eijsvogels, T.M. Cardiac troponin release in athletes: What do we know and where should we go? Curr. Opin. Physiol. 2023, 31, 100629. [Google Scholar] [CrossRef]
- Wellens, H.J.; Gorgels, A.P.M. How Important Is the Electrocardiogram in Protecting and Guiding the Athlete? Circulation 2011, 124, 669–671. [Google Scholar] [CrossRef]
- Nicogossian, A.; Kloiber, O.; Stabile, B. The Revised World Medical Association’s Declaration of Helsinki 2013: Enhancing the Protection of Human Research Subjects and Empowering Ethics Review Committees. World Med. Health Policy 2014, 6, 1–3. [Google Scholar] [CrossRef]
- NeuroTracker. Available online: https://www.neurotrackerx.com/#sports (accessed on 21 March 2022).
- Cavanaugh, C. Urine Sediment Exam Provides More Diagnostic Information in AKI than Novel Urinary Biomarkers: PRO. Kidney360 2022, 3, 597–599. [Google Scholar] [CrossRef] [PubMed]
- Imenez Silva, P.H.; Mohebbi, N. Kidney metabolism and acid–base control: Back to the basics. Pflug. Arch.—Eur. J. Physiol. 2022, 474, 919–934. [Google Scholar] [CrossRef]
- Quade, B.N.; Parker, M.D.; Occhipinti, R. The therapeutic importance of acid-base balance. Biochem. Pharmacol. 2021, 183, 114278. [Google Scholar] [CrossRef] [PubMed]
- Faulhaber, M.; Gröbner, K.; Rausch, L.; Gatterer, H.; Menz, V. Effects of Acute Hypoxia on Lactate Thresholds and High-Intensity Endurance Performance—A Pilot Study. IJERPH 2021, 18, 7573. [Google Scholar] [CrossRef]
- Hall, J.E.; Hall, M.E. Guyton and Hall Textbook of Medical Physiology, 14th ed.; Elsevier: Jackson, MS, USA, 2020; pp. 383–400. [Google Scholar]
- Krbec, M.; Waldauf, P.; Zadek, F.; Brusatori, S.; Zanella, A.; Duška, F.; Langer, T. Non-carbonic buffer power of whole blood is increased in experimental metabolic acidosis: An in-vitro study. Front. Physiol. 2022, 13, 1009378. [Google Scholar] [CrossRef] [PubMed]
- Sumi, D.; Kojima, C.; Kasai, N.; Goto, K. The effects of endurance exercise in hypoxia on acid-base balance and potassium kinetics: A randomized crossover design in male endurance athletes. Sport. Med. 2018, 4, 1–8. [Google Scholar] [CrossRef]
- Panarelli, M. Understanding Acid-Base Disorders. Clinical Acid-Base Balance. By W. S. T. Thomson, J. F. Adams and R. A. Cowan. Clin. Chem. Lab. Med. 2000, 38, 482. [Google Scholar] [CrossRef]
- Goodwin, M.L.; Harris, J.E.; Hernández, A.; Gladden, L.B. Blood Lactate Measurements and Analysis during Exercise: A Guide for Clinicians. J. Diabetes Sci. Technol. 2007, 1, 558–569. [Google Scholar] [CrossRef]
- Hopkins, E.; Sanvictores, T.; Sharma, S. Physiology, Acid Base Balance; StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Lee, E.C.; Fragala, M.S.; Kavouras, S.A.; Queen, R.M.; Pryor, J.L.; Casa, D.J. Biomarkers in Sports and Exercise: Tracking Health, Performance, and Recovery in Athletes. J. Strength Cond. Res. 2017, 31, 2920–2937. [Google Scholar] [CrossRef]
- Neupert, E.; Gupta, L.; Holder, T.; Jobson, S.A. Athlete monitoring practices in elite sport in the United Kingdom. J. Sport. Sci. 2022, 40, 1450–1457. [Google Scholar] [CrossRef] [PubMed]
- Petre, I.M.; Boscoianu, M.; Oancea, B.; Chicomban, M.; Turcu, I.; Simion, G. Analysis of the Physiognomy of Unique Sets in the Maximum Number of Repetitions Strategy—The Case of One-Arm Scott Machine Seated Bicep Curls. Appl. Sci. 2022, 12, 8308. [Google Scholar] [CrossRef]
- Iliadis, A.; Tomovic, M.; Dervas, D.; Psymarnou, M.; Christoulas, K.; Kouidi, E.J.; Deligiannis, A.P. A Novel mHealth Monitoring System during Cycling in Elite Athletes. Int. J. Environ. Res. Public Health 2021, 18, 4788. [Google Scholar] [CrossRef] [PubMed]
- Serhan, M.H.; Yakan, M.; Serhan, C. Sports nutrition knowledge translates to enhanced athletic performance: A cross-sectional study among Lebanese university athletes. Nutr. Food Sci. 2022. [Google Scholar] [CrossRef]
- Simona Nicoleta, C. Utilizarea Tehnologiei de Investigare Biochimică în Dirijarea Efortului la Sportul de Performanţă, 1st ed.; Ministerul Educaţiei, Cercetării, Tineretului şi Sportului: Pitesti, Romania, 2011; pp. 10–17. [Google Scholar]
- Cosmed—K5: Wearable Metabolic System for Both Laboratory and Field Testing. Available online: https://www.cosmed.com/en/products/cardio-pulmonary-exercise-test/k (accessed on 8 November 2021).
- Lactate Pro. Available online: https://www.laktate.com/en/product/lactate-pro-2/ (accessed on 12 November 2021).
- Park, S.Y.; Klotzbier, T.J.; Schott, N. The Effects of the Combination of High-Intensity Interval Training with 3D-Multiple Object Tracking Task on Perceptual-Cognitive Performance: A Randomized Controlled Intervention Trial. Int. J. Env. Res. Public Health 2021, 18, 4862. [Google Scholar] [CrossRef]
- Zimmermann, P.; Schöffl, I.; Schöffl, V.; Zimmermann, L.; Eckstein, M.L.; Moser, O.; Wüstenfeld, J. Physiological Effects of Training in Elite German Winter Sport Athletes: Sport Specific Remodeling Determined Using Echocardiographic Data and CPET Performance Parameters. J. Cardiovasc. Dev. Dis. 2022, 9, 235. [Google Scholar] [CrossRef]
- Thaler, M.S. The Only EKG Book You’ll Ever Need, 8th ed.; Lippincott Williams & Wilkins: Bucuresti, Romania, 2014; pp. 168–290. [Google Scholar]
- Basu, J.; Malhotra, A. Interpreting the Athlete’s ECG: Current State and Future Perspectives. Curr. Treat. Options Cardiovasc. Med. 2018, 20, 1–10. [Google Scholar] [CrossRef]
- Lühker, O.; Berger, M.M.; Pohlmann, A.; Hotz, L.; Gruhlke, T.; Hochreiter, M. Changes in acid–base and ion balance during exercise in normoxia and normobaric hypoxia. Eur. J. Appl. Physiol. 2017, 117, 2251–2261. [Google Scholar] [CrossRef]
- ABL9 blood gas analyzer—Radiometer. Available online: https://www.radiometer.com/en/products/blood-gas-testing/abl9-blood-gas-analyzer (accessed on 15 November 2021).
- Chris, H. Useful Tips to Avoid Preanalytical Errors in Blood Gas Testing. Available online: https://acutecaretesting.org/en/articles/useful-tips-to-avoid-preanalytical-errors-in-blood-gas-testing-ph-pco2-and-po2 (accessed on 15 November 2021).
- Gomez-Cabrera, M.C.; Carretero, A.; Millan-Domingo, F.; Garcia-Dominguez, E.; Correas, A.G.; Olaso-Gonzalez, G.; Viña, J. Redox-related biomarkers in physical exercise. Redox Biol. 2021, 42, 101956. [Google Scholar] [CrossRef]
- Forsal, I.; Bodelsson, M.; Wieslander, A.; Nilsson, A.; Pouchoulin, D.; Broman, M. Analysis of acid–base disorders in an ICU cohort using a computer script. Intensive Care Med. Exp. 2022, 10, 1. [Google Scholar] [CrossRef]
- Pedlar, C.R.; Newell, J.; Lewis, N.A. Blood Biomarker Profiling and Monitoring for High-Performance Physiology and Nutrition: Current Perspectives, Limitations and Recommendations. Sport. Med. 2019, 49, 185–198. [Google Scholar] [CrossRef] [PubMed]
- CDS Medonic M-Series Hematology Analyzer. Available online: https://www.medline.com/product/CDS-Medonic-M-Series-Hematology-Analyzer/Hematology-Analyzers/Z05-PF54418?question=medonic&index=P2&indexCount=2#mrkMore (accessed on 10 November 2021).
- Leard Statistics. Available online: https://statistics.laerd.com/premium/spss/pstt/paired-samples-t-test-in-spss-17.php (accessed on 21 December 2022).
- Ferretti, G.; Fagoni, N.; Taboni, A.; Vinetti, G.; di Prampero, P.E. A century of exercise physiology: Key concepts on coupling respiratory oxygen flow to muscle energy demand during exercise. Eur. J. Appl. Physiol. 2022, 122, 1317–1365. [Google Scholar] [CrossRef] [PubMed]
- Knechtle, B.; Nikolaidis, P.T.; Zingg, M.A.; Rosemann, T.; Rüst, C.A. Differences in Age of Peak Marathon Performance between Mountain and City Marathon Running—The “Jungfrau Marathon” in Switzerland. Chin. J. Physiol. 2017, 60, 11–22. [Google Scholar] [CrossRef]
- Liu, R.; Krüger, K.; Pilat, C.; Fan, W.; Xiao, Y.; Seimetz, M.; Ringseis, R.; Baumgart-Vogt, E.; Eder, K.; Weissmann, N.; et al. Excessive Accumulation of Intracellular Ca2+ After Acute Exercise Potentiated Impairment of T-cell Function. Front. Physiol. 2021, 12, 728625. [Google Scholar] [CrossRef] [PubMed]
- Alves, M.D.D.J.; Silva, D.D.S.; Pereira, E.V.M.; Pereira, D.D.; de Sousa Fernandes, M.S.; Santos, D.F.C.; Oliveira, D.P.M.; Vieira-Souza, L.M.; Aidar, F.J.; de Souza, R.F. Changes in Cytokines Concentration Following Long-Distance Running: A Systematic Review and Meta-Analysis. Front. Physiol. 2022, 13, 838069.1. [Google Scholar] [CrossRef]
- Guyton, H. Tratat de Fiziologie a Omului, 11th ed.; Editura Medicala Callisto: Bucuresti, Romania, 2007; 1152p. [Google Scholar]
- Dakduk, S.; González, Á.; Portalanza, A. Learn About Structural Equation Modeling in SmartPLS With Data from the Customer Behavior in Electronic Commerce Study in Ecuador (2017); SAGE Publications: Thousand Oaks, CA, USA, 2019; pp. 2–19. [Google Scholar]
- Hair, J.F.; Risher, J.J.; Sarstedt, M.; Ringle, C.M. When to use and how to report the results of PLS-SEM. Eur. Bus. Rev. 2019, 31, 2–24. [Google Scholar] [CrossRef]
- Hair, F.M.J., Jr.; Hult, G.T.M.; Ringle, C.; Sarstedt, M. Investigation of mobile banking usage with partial least squares structural equation modeling. Gazi J. Econ. Bus. 2021, 7. [Google Scholar]
- Henseler, J.; Dijkstra, T.K.; Sarstedt, M.; Ringle, C.M.; Diamantopoulos, A.; Straub, D.W.; Ketchen, D.J., Jr.; Hair, J.F.; Hult, G.T.M.; Calantone, R.J. Common Beliefs and Reality about PLS. Organ. Res. Methods 2014, 17, 182–209. [Google Scholar] [CrossRef]
- Nabhan, D. Preventive Medicine in Elite Sport: The Role of the Periodic Health Evalutation. Ph.D. Thesis, Norwegian School of Sport Science, Oslo, Norway, 2022. [Google Scholar]
- Callegari, G.A.; Novaes, J.S.; Neto, G.R.; Dias, I.; Garrido, N.D.; Dani, C. Creatine Kinase and Lactate Dehydrogenase Responses after Different Resistance and Aerobic Exercise Protocols. J. Hum. Kinet. 2017, 58, 65–72. [Google Scholar] [CrossRef]
- Alesi, M.; Gómez-López, M.; Borrego, C.C. Editorial: Psychological Factors in Physical Education and Sport. Front. Psychol. 2022, 12, 826291. [Google Scholar] [CrossRef]
- Pardo Albiach, J.; Mir-Jimenez, M.; Hueso Moreno, V.; Nácher Moltó, I.; Martínez-Gramage, J. The Relationship between VO2max, Power Management, and Increased Running Speed: Towards Gait Pattern Recognition through Clustering Analysis. Sensors 2021, 21, 2422. [Google Scholar] [CrossRef] [PubMed]
- Foster, C. V O2 max and training indices as determinants of competitive running performance. J. Sport. Sci. 1983, 1, 13–22. [Google Scholar] [CrossRef]
- Navalta, J.W.; Beck, V.D.Y.; Diaz, T.M.; Ollano, V.E. Effects of nutritional and hydration strategies during ultramarathon events between finishers and non-finishers: A systematic review protocol. PLoS ONE 2022, 17, e0272668. [Google Scholar] [CrossRef] [PubMed]
- Katharina, W.; Mohamad, M.; Derrick, T.; Martina, G.; Gerold, W.; Claus, L.; Lee, H.; Thomas, R.; Beat, K. Supplement intake in half-marathon, (ultra-)marathon and 10-km runners—Results from the NURMI study (Step 2). J. Int. Soc. Sport. Nutr. 2021, 18, 64. [Google Scholar] [CrossRef]
- Spaner, C.R.; Musteata, S.; Kenny, R.A.; Gawryluk, J.R.; Hofer, S.; Christie, B.R. 3-Dimensional Multiple Object Tracking Training Can Enhance Selective Attention, Psychomotor Speed, and Cognitive Flexibility in Healthy Older Adults. Ageing Sci. Ment. Health Stud. 2019, 3, 1–12. [Google Scholar]
- Komarudin, K.; Hidayat, Y.; Novian, G. Neurotracker Training to Improve Shooting Performance of Archery Athletes. Int. J. Hum. Mov. Sport. Sci. 2021, 9, 66–70. [Google Scholar] [CrossRef]
- Komarudin, K.; Mulyana, M.; Berliana, B.; Purnamasari, I. NeuroTracker Three-Dimensional Multiple Object Tracking (3D-MOT): A Tool to Improve Concentration and Game Performance among Basketball Athletes. Ann. Appl. Sport Sci. 2021, 9, 0-0. [Google Scholar] [CrossRef]
- Phillips, J.; Andre, T. Visual tracking speed threshold in NCAA Division I women’s soccer predicting match performance: A preliminary study. Sci. J. Sport Perform. 2022, 2, 94–104. [Google Scholar] [CrossRef]
- Kennedy, M.; Comer, F.; Young, J.A.; Valasek, A.E. Increasing Primary Care Follow-up after Preparticipation Physical Evaluations. Pediatr. Qual. Saf. 2020, 5, e358. [Google Scholar] [CrossRef]
- Sato, S.; Dyar, K.A.; Treebak, J.T.; Jepsen, S.L.; Ehrlich, A.M.; Ashcroft, S.P.; Trost, K.; Kunzke, T.; Prade, V.M.; Small, L.; et al. Atlas of exercise metabolism reveals time-dependent signatures of metabolic homeostasis. Cell Metab. 2022, 34, 329–345.e8. [Google Scholar] [CrossRef]
- Mindrescu, V.; Enoiu, R.S. Deconstructing the Parent–Child Relationship during the COVID-19 Pandemic through Tech-Wise Outlets Such as the Internet and Media Consumption. Sustainability 2022, 14, 13138. [Google Scholar] [CrossRef]
- van der Wall, E.E. Long-distance running: Running for a long life? Neth. Heart J. 2014, 22, 89–90. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Athlete | Height (cm) | Weight (kg) | Age (2021) (Years) | BMI (kg/m2) |
|---|---|---|---|---|
| A1 | 176 | 67 | 26 | 21.63 |
| A2 | 173 | 65 | 32 | 21.72 |
| A3 | 175 | 67 | 34 | 21.88 |
| A4 | 178 | 58 | 38 | 18.31 |
| A5 | 176 | 70 | 28 | 22.6 |
| A6 | 175 | 50 | 22 | 16.33 |
| A7 | 170 | 62 | 20 | 21.45 |
| Protocol Respected | Duration (min) | |
|---|---|---|
| Mountain Running Race | Warming up Cool-down | 30 20 |
| EKG | Performed in rest conditions | 10 |
| Effort test | Individual gymnastics | 15 |
| Easy running on the stadium | 15 | |
| Easy running on the treadmill | 8 | |
| Bruce protocol to measure VO2max | 18–20 | |
| Cool down (running and stretching) | 30 (15-15) | |
| Lactate analysis | Blood samples were performed at the end of the running on the treadmill and 15 min later | 16 |
| Biochemical blood test | No breakfast before Samples were performed before exercise | 5 |
| Astrup method | No breakfast before Samples were performed before exercise | 5 |
| Urine summary | No breakfast before Specific protocol to avoid contamination of the sample | 5 |
| NeuroTracker | Specific NeuroTracker protocol | According to the protocol |
| Level | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| Speed (km/h) | 2.7 | 4 | 5.4 | 6.7 | 8 | 8.8 | 9.6 |
| Elevation (%) | 10 | 12 | 14 | 16 | 18 | 20 | 22 |
| Athlete | Time1 | Time2 | Rank 1 | Rank 2 | Min1 | VO2 /kg1 | HR max1 | Min2 | VO2 /kg2 | HR max2 | LATI1 | LARI1 | LATF2 | LARF2 | NeuroI | NeuroF |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A1 | 2481 | 3685 | 1 | 4 | 19.03 | 70.4 | 195 | 19.35 | 71.2 | 199 | 12.2 | 6.1 | 11.2 | 5.6 | 1.88 | 2.12 |
| A2 | 2500 | 3570 | 2 | 1 | 18.25 | 70.1 | 188 | 19.2 | 70.6 | 188 | 15.8 | 7.5 | 12.5 | 7.1 | 1.17 | 1.86 |
| A3 | 2513 | 3749 | 3 | 6 | 18.47 | 65.1 | 197 | 19.18 | 68.1 | 197 | 13.5 | 6.9 | 12.8 | 6.5 | 1.05 | 1.76 |
| A4 | 2559 | 3608 | 6 | 2 | 19.11 | 63.2 | 201 | 19.8 | 64.2 | 201 | 12.8 | 6.5 | 11.9 | 6.1 | 1.41 | 1.88 |
| A5 | 2564 | 3669 | 7 | 3 | 18.1 | 52.8 | 205 | 19.15 | 54.6 | 210 | 12.1 | 7.1 | 11.7 | 6.8 | 1.86 | 2.09 |
| A6 | 2692 | 4028 | 12 | 8 | 18.51 | 43.5 | 198 | 19.1 | 48.7 | 198 | 14.7 | 10.8 | 12.8 | 9.9 | 2 | 2.52 |
| A7 | 2908 | 4409 | 16 | 9 | 19.17 | 64.4 | 200 | 19.23 | 65.1 | 200 | 12.1 | 5.9 | 12 | 5.5 | 1.67 | 2.31 |
| Athlete | Initial Test Modifications | Clinical Significance | Final Test Modifications | Clinical Significance |
|---|---|---|---|---|
| A1 | Bradycardic rhythm | Increased effort tolerance | PR > 0.2 s | Atrioventricular block type 1 |
| A2 | Bradycardic rhythm | Increased effort tolerance | Bradycardic rhythm | Increased effort tolerance |
| A3 | Increasing the amplitude of the R wave in aVL > 11mm | Left ventricular hypertrophy | ST elevation from V2–V5 | Anterior stroke |
| A4 | PR > 0.2 s | Atrioventricular block type 1 | PR > 0.2 s | Atrioventricular block type 1 |
| A5 | Increasing the amplitude of the R wave in DI > 13 mm | Left ventricular hypertrophy | Increasing the amplitude of the wave R in DI > 13 mm | Left ventricular hypertrophy |
| A6 | Bradycardic rhythm | Increased effort tolerance | Increasing the amplitude of the R wave in aVL > 11 mm | Left ventricular hypertrophy |
| A7 | Bradycardic rhythm | Increased exercise tolerance | Bradycardic rhythm | Increased exercise tolerance |
| pO2 | pCO2 | SO2 | Ca++ | Cl− | LDH | CPK | P |
|---|---|---|---|---|---|---|---|
| 75–100 | 35–45 | 95–100 | 4.61–5.33 | 98–106 | 230–460 | 50–250 | +/- |
| mmHg | mmHg | % | mg/dL | mmol/dL | UI/L | UI/L |
| Athlete | pO21 | pO22 | pCO21 | pCO22 | SO21 | SO22 | Ca++1 | Ca++2 | Cl−1 | Cl−2 | LDH1 | LDH2 | CPK1 | CPK2 | P1 | P2 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A1 | 66.6↓ | 72↓ | 37.5↔ | 35.9↔ | 93.2↓ | 94.3↓ | 4.2↓ | 4.28↓ | 111↑ | 108↑ | 518↑ | 318↔ | 215 ↔ | 166↔ | + | - |
| A2 | 62.1↓ | 69↓ | 34.5↓ | 37.5↔ | 92.6↓ | 93.7↓ | 4.2↓ | 4.69↔ | 110↑ | 105↔ | 448↑ | 301↔ | 439↑ | 236↔ | - | - |
| A3 | 54.7↓ | 60↓ | 37↔ | 39,6↔ | 87↓ | 90.2↓ | 3.7↓ | 4.1↓ | - | - | 325↔ | 289↔ | 182↔ | 143↔ | - | - |
| A4 | 66.1↓ | 66.4↓ | 47.1↑ | 34.3↓ | 92.2↓ | 93.2↓ | 4.1↓ | 4.1↓ | - | - | 503↑ | 470↑ | 210↔ | 205↔ | - | - |
| A5 | 71.7↓ | 82↔ | 34.8↓ | 42↔ | 93.8↓ | 94,2↓ | 4.27↓ | 4↓ | - | - | 637↑ | 348↔ | 649↑ | 329↑ | + | - |
| A6 | 60↓ | 74↓ | 48.7↑ | 46↑ | 89.7↓ | 91.8↓ | 4.47↓ | 4.23↓ | 110↑ | 108↑ | 367↔ | 325↔ | 254↑ | 251↑ | - | - |
| A7 | 54.5↓ | 68↓ | 44.1↔ | 41.6↔ | 86.9↓ | 93.1↓ | 4.6↓ | 4.25↓ | - | - | 362↔ | 294↔ | 468↑ | 385↑ | + | - |
| Variable | CA | rho_A | CR | AVE |
|---|---|---|---|---|
| Physiologic2 | >0.7 | >0.7 | >0.7 | >0.5 |
| 1 | ||||
| Sensory activity | 0.821 | 1.142 | 0.932 | 0.884 |
| Variable | LARF2 | LATF2 | Min2 | NeuroF | Time2 | VO2max |
|---|---|---|---|---|---|---|
| VIF | 4.488 | 2128 | 1.271 | 1.941 | 1.941 | 2.793 |
| Pair of Variables | 95% CID | t-Value | p-Value | Result |
|---|---|---|---|---|
| Rank1-Rank2 | (−1.54,5.54) | 1.38 | 0.005 | RNH |
| VO2max1-VO2max2 | (−1.12,0.89) | −4.47 | 0.004 | RNH |
| NTi-NTf | (−0.5,0.2) | −6.59 | 0.004 | RNH |
| pO21-pO22 | (−12.5,−3.39) | −4.2 | 0.005 | RNH |
| SO21-SO22 | (−2.1,2) | −2.84 | 0.029 | RNH |
| LDH1-LDH2 | (116.4,99.17) | 3.1 | 0.021 | RNH |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Enoiu, R.-S.; Găinariu, I.; Mîndrescu, V. Implementing Modern Technology for Vital Sign Monitoring to Enhance Athletic Training and Sports Performance. Sustainability 2023, 15, 2520. https://doi.org/10.3390/su15032520
Enoiu R-S, Găinariu I, Mîndrescu V. Implementing Modern Technology for Vital Sign Monitoring to Enhance Athletic Training and Sports Performance. Sustainability. 2023; 15(3):2520. https://doi.org/10.3390/su15032520
Chicago/Turabian StyleEnoiu, Răzvan-Sandu, Iulia Găinariu, and Veronica Mîndrescu. 2023. "Implementing Modern Technology for Vital Sign Monitoring to Enhance Athletic Training and Sports Performance" Sustainability 15, no. 3: 2520. https://doi.org/10.3390/su15032520
APA StyleEnoiu, R.-S., Găinariu, I., & Mîndrescu, V. (2023). Implementing Modern Technology for Vital Sign Monitoring to Enhance Athletic Training and Sports Performance. Sustainability, 15(3), 2520. https://doi.org/10.3390/su15032520