

Spatial Non-Stationarity Effects of Unhealthy Food Environments and Green Spaces for Type-2 Diabetes in Toronto



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Data
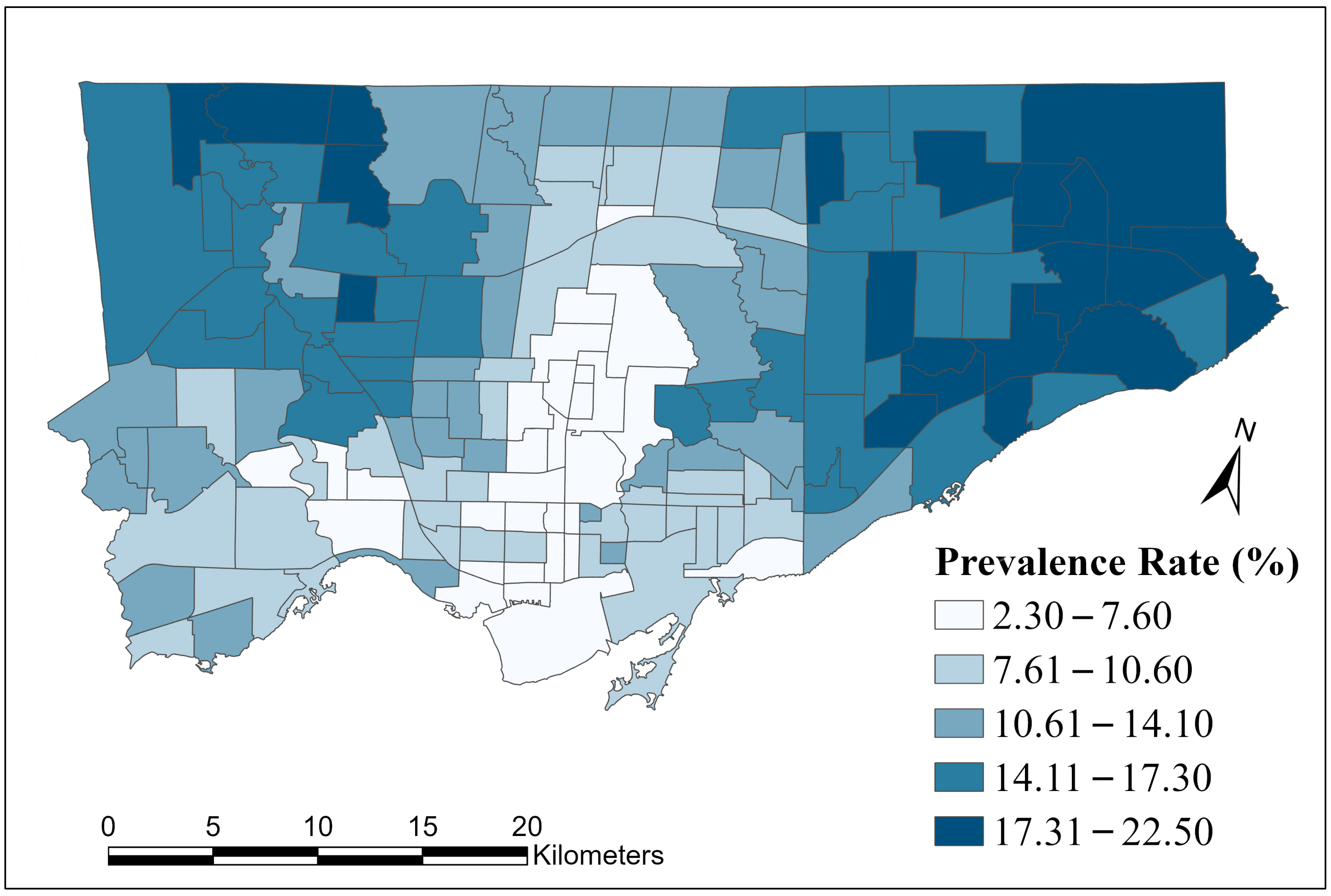
2.2.1. Type-2 Diabetes Mellitus Prevalence Rates
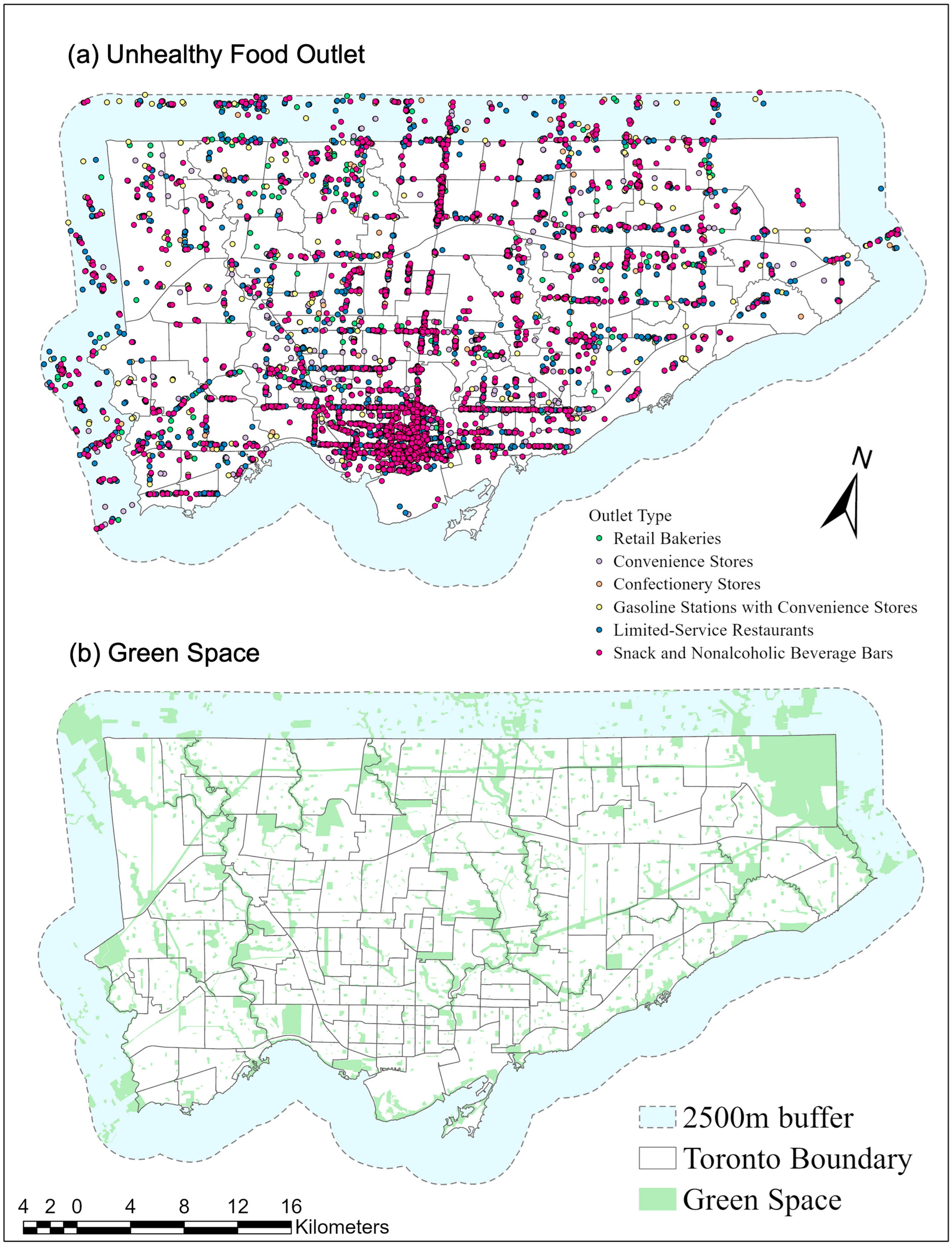
2.2.2. Unhealthy Food Outlets
2.2.3. Green Spaces
2.2.4. Socioeconomic Status
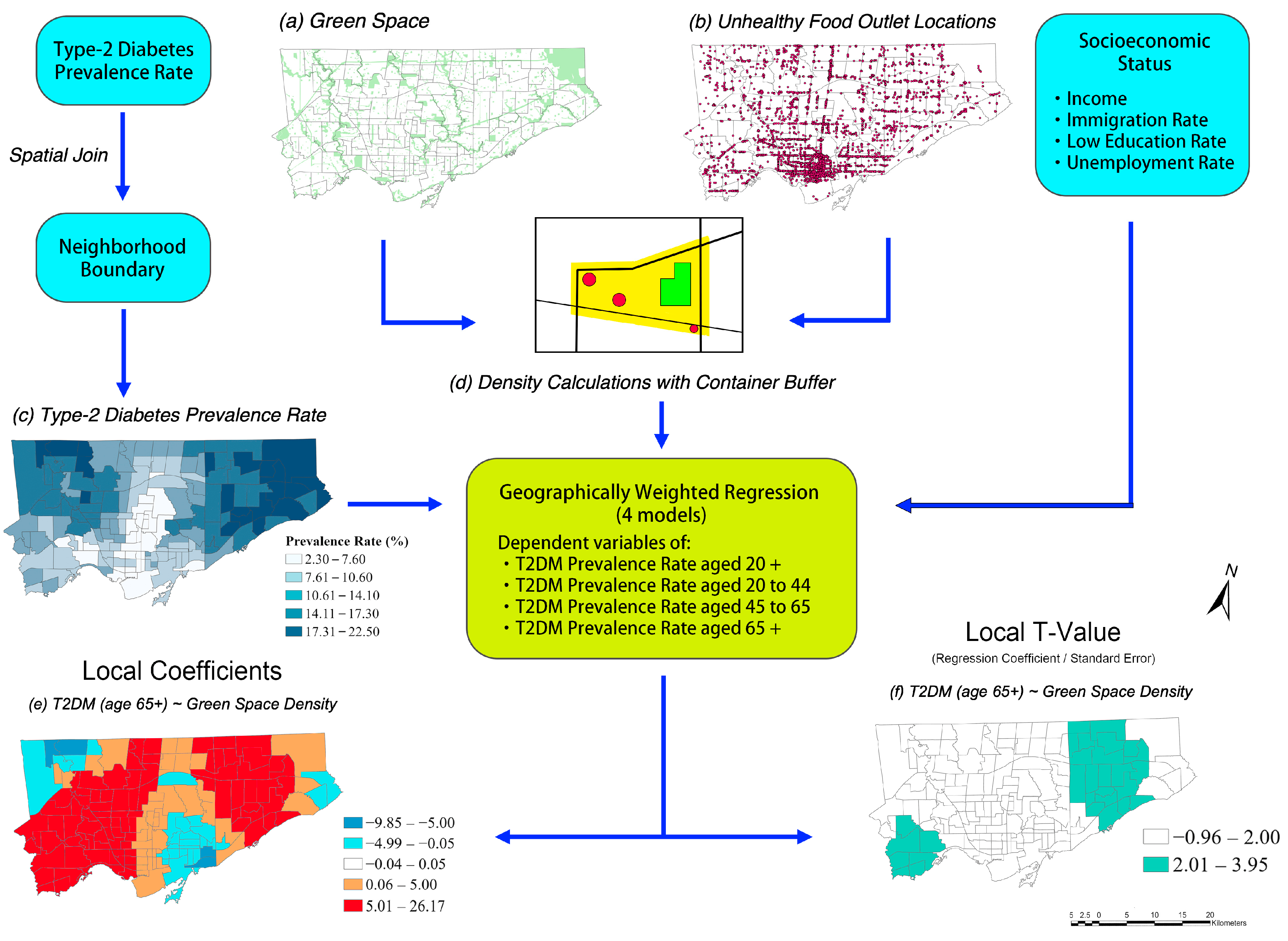
2.2.5. Derivation of Environmental Variables
2.3. Statistical Analysis
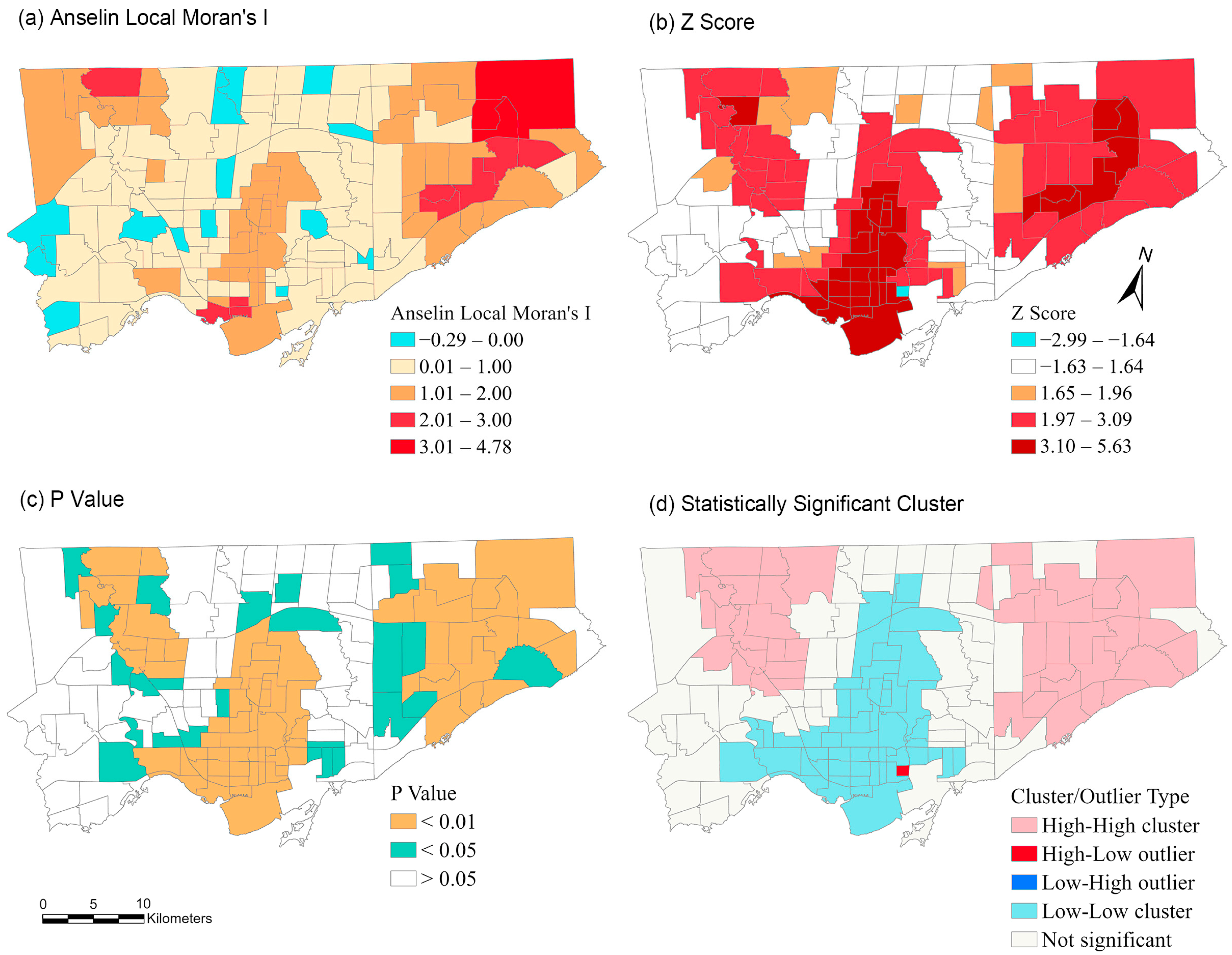
2.3.1. Spatial Autocorrelation
2.3.2. Geographically Weighted Regression (GWR)
2.3.3. Multicollinearity
3. Results
3.1. Descriptive Statistics
3.2. GWR Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed. Available online: www.diabetesatlas.org (accessed on 1 October 2022).
- Bommer, C.; Heesemann, E.; Sagalova, V.; Manne-Goehler, J.; Atun, R.; Bärnighausen, T.; Vollmer, S. The Global Economic Burden of Diabetes in Adults Aged 20–79 Years: A Cost-of-Illness Study. Lancet Diabetes Endocrinol. 2017, 5, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Khunti, K.; Davies, M.J. Type 2 Diabetes. Lancet 2017, 389, 2239–2251. [Google Scholar] [CrossRef] [PubMed]
- Dendup, T.; Feng, X.; Clingan, S.; Astell-Burt, T. Environmental Risk Factors for Developing Type 2 Diabetes Mellitus: A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 78. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation Type 2 Diabetes. Available online: https://idf.org/aboutdiabetes/type-2-diabetes.html (accessed on 8 March 2022).
- Toronto Public Health. Health Surveillance Indicators: Diabetes. Available online: https://www.toronto.ca/wp-content/uploads/2017/12/8c72-tph-hsi-diabetes-july18f.pdf (accessed on 21 August 2022).
- Astell-Burt, T.; Feng, X.; Kolt, G.S. Is Neighborhood Green Space Associated with a Lower Risk of Type 2 Diabetes? Evidence from 267,072 Australians. Diabetes Care 2014, 37, 197–201. [Google Scholar] [CrossRef]
- Bodicoat, D.H.; O’Donovan, G.; Dalton, A.M.; Gray, L.J.; Yates, T.; Edwardson, C.; Hill, S.; Webb, D.R.; Khunti, K.; Davies, M.J. The Association between Neighbourhood Greenspace and Type 2 Diabetes in a Large Cross-Sectional Study. BMJ Open 2014, 4, e006076. [Google Scholar] [CrossRef] [PubMed]
- Ulmer, J.M.; Wolf, K.L.; Backman, D.R.; Tretheway, R.L.; Blain, C.J.A.; O’Neil-Dunne, J.P.M.; Frank, L.D. Multiple Health Benefits of Urban Tree Canopy: The Mounting Evidence for a Green Prescription. Health Place 2016, 42, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Paquet, C.; Coffee, N.T.; Haren, M.T.; Howard, N.J.; Adams, R.J.; Taylor, A.W.; Daniel, M. Food Environment, Walkability, and Public Open Spaces Are Associated with Incident Development of Cardio-Metabolic Risk Factors in a Biomedical Cohort. Health Place 2014, 28, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Mezuk, B.; Li, X.; Cederin, K.; Rice, K.; Sundquist, J.; Sundquist, K. Beyond Access: Characteristics of the Food Environment and Risk of Diabetes. Am. J. Epidemiol. 2016, 183, 1129–1137. [Google Scholar] [CrossRef] [PubMed]
- Ahern, M.; Brown, C.; Dukas, S. A National Study of the Association between Food Environments and County-level Health Outcomes. J. Rural. Health 2011, 27, 367–379. [Google Scholar] [CrossRef]
- Gebreab, S.Y.; Hickson, D.M.A.; Sims, M.; Wyatt, S.B.; Davis, S.K.; Correa, A.; Diez-Roux, A.V. Neighborhood Social and Physical Environments and Type 2 Diabetes Mellitus in African Americans: The Jackson Heart Study. Health Place 2017, 43, 128–137. [Google Scholar] [CrossRef]
- Sundquist, K.; Eriksson, U.; Mezuk, B.; Ohlsson, H. Neighborhood Walkability, Deprivation and Incidence of Type 2 Diabetes: A Population-Based Study on 512,061 Swedish Adults. Health Place 2015, 31, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Creatore, M.I.; Glazier, R.H.; Moineddin, R.; Fazli, G.S.; Johns, A.; Gozdyra, P.; Matheson, F.I.; Kaufman-Shriqui, V.; Rosella, L.C.; Manuel, D.G. Association of Neighborhood Walkability with Change in Overweight, Obesity, and Diabetes. JAMA 2016, 315, 2211–2220. [Google Scholar] [CrossRef] [PubMed]
- Glazier, R.H.; Creatore, M.I.; Weyman, J.T.; Fazli, G.; Matheson, F.I.; Gozdyra, P.; Moineddin, R.; Shriqui, V.K.; Booth, G.L. Density, Destinations or Both? A Comparison of Measures of Walkability in Relation to Transportation Behaviors, Obesity and Diabetes in Toronto, Canada. PLoS ONE 2014, 9, e85295. [Google Scholar] [CrossRef] [PubMed]
- Booth, G.L.; Creatore, M.I.; Moineddin, R.; Gozdyra, P.; Weyman, J.T.; Matheson, F.I.; Glazier, R.H. Unwalkable Neighborhoods, Poverty, and the Risk of Diabetes among Recent Immigrants to Canada Compared with Long-Term Residents. Diabetes Care 2013, 36, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.; Bai, L.; Oiamo, T.H.; Burnett, R.T.; Weichenthal, S.; Jerrett, M.; Kwong, J.C.; Goldberg, M.S.; Copes, R.; Kopp, A.; et al. Association between Road Traffic Noise and Incidence of Diabetes Mellitus and Hypertension in Toronto, Canada: A Population-Based Cohort Study. J. Am. Heart Assoc. 2020, 9, e013021. [Google Scholar] [CrossRef]
- Müller-Riemenschneider, F.; Pereira, G.; Villanueva, K.; Christian, H.; Knuiman, M.; Giles-Corti, B.; Bull, F.C. Neighborhood Walkability and Cardiometabolic Risk Factors in Australian Adults: An Observational Study. BMC Public Health 2013, 13, 1–9. [Google Scholar] [CrossRef]
- Requia, W.J.; Adams, M.D.; Koutrakis, P. Association of PM2.5 with Diabetes, Asthma, and High Blood Pressure Incidence in Canada: A Spatiotemporal Analysis of the Impacts of the Energy Generation and Fuel Sales. Sci. Total Environ. 2017, 584–585, 1077–1083. [Google Scholar] [CrossRef]
- Heidemann, C.; Niemann, H.; Paprott, R.; Du, Y.; Rathmann, W.; Scheidt-Nave, C. Residential Traffic and Incidence of Type 2 Diabetes: The German Health Interview and Examination Surveys. Diabet. Med. 2014, 31, 1269–1276. [Google Scholar] [CrossRef]
- Bodicoat, D.H.; Carter, P.; Comber, A.; Edwardson, C.; Gray, L.J.; Hill, S.; Webb, D.; Yates, T.; Davies, M.J.; Khunti, K. Is the Number of Fast-Food Outlets in the Neighbourhood Related to Screen-Detected Type 2 Diabetes Mellitus and Associated Risk Factors? Public Health Nutr. 2015, 18, 1698–1705. [Google Scholar] [CrossRef]
- Ntarladima, A.M.; Karssenberg, D.; Poelman, M.; Grobbee, D.E.; Lu, M.; Schmitz, O.; Strak, M.; Janssen, N.; Hoek, G.; Vaartjes, I. Associations between the Fast-Food Environment and Diabetes Prevalence in the Netherlands: A Cross-Sectional Study. Lancet Planet Health 2022, 6, e29–e39. [Google Scholar] [CrossRef]
- Li, R.; Chen, G.; Jiao, A.; Lu, Y.; Guo, Y.; Li, S.; Wang, C.; Xiang, H. Residential Green and Blue Spaces and Type 2 Diabetes Mellitus: A Population-Based Health Study in China. Toxics 2021, 9, 11. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Rehm, C.D.; Moudon, A.V.; Arterburn, D. The Geography of Diabetes by Census Tract in a Large Sample of Insured Adults in King County, Washington, 2005–2006. Prev. Chronic Dis. 2014, 11, E125. [Google Scholar] [CrossRef]
- Kolpak, P.; Wang, L. Exploring the Social and Neighbourhood Predictors of Diabetes: A Comparison between Toronto and Chicago. Prim. Health Care Res. Dev. 2017, 18, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Christine, P.J.; Auchincloss, A.H.; Bertoni, A.G.; Carnethon, M.R.; Sánchez, B.N.; Moore, K.; Adar, S.D.; Horwich, T.B.; Watson, K.E.; Roux, A.V.D. Longitudinal Associations between Neighborhood Physical and Social Environments and Incident Type 2 Diabetes Mellitus: The Multi-Ethnic Study of Atherosclerosis (MESA). JAMA Intern. Med. 2015, 175, 1311–1320. [Google Scholar] [CrossRef] [PubMed]
- Frankenfeld, C.L.; Leslie, T.F.; Makara, M.A. Diabetes, Obesity, and Recommended Fruit and Vegetable Consumption in Relation to Food Environment Sub-Types: A Cross-Sectional Analysis of Behavioral Risk Factor Surveillance System, United States Census, and Food Establishment Data. BMC Public Health 2015, 15, 1–9. [Google Scholar] [CrossRef]
- Piccolo, R.S.; Duncan, D.T.; Pearce, N.; McKinlay, J.B. The Role of Neighborhood Characteristics in Racial/Ethnic Disparities in Type 2 Diabetes: Results from the Boston Area Community Health (BACH) Survey. Soc. Sci. Med. 2015, 130, 79–90. [Google Scholar] [CrossRef]
- Chowdhury, M.A.B.; Uddin, M.J.; Khan, H.M.R.; Haque, M.R. Type 2 Diabetes and Its Correlates among Adults in Bangladesh: A Population Based Study. BMC Public Health 2015, 15, 1070. [Google Scholar] [CrossRef]
- Wu, H.; Meng, X.; Wild, S.H.; Gasevic, D.; Jackson, C.A. Socioeconomic Status and Prevalence of Type 2 Diabetes in Mainland China, Hong Kong and Taiwan: A Systematic Review. J. Glob. Health 2017, 7, 011103. [Google Scholar] [CrossRef] [PubMed]
- Wang, F. Why Public Health Needs GIS: A Methodological Overview. Ann. GIS 2019, 26, 1–12. [Google Scholar] [CrossRef]
- Kwan, M.P. The Uncertain Geographic Context Problem. Environ. Health 2012, 102, 958–968. [Google Scholar] [CrossRef]
- Buzzelli, M. Modifiable Areal Unit Problem. Int. Encycl. Hum. Geogr. 2020, 169. [Google Scholar] [CrossRef]
- Kwan, M.-P. The Stationarity Bias in Research on the Environmental Determinants of Health. Health Place 2021, 70, 102609. [Google Scholar] [CrossRef]
- Wang, J.; Lee, K.; Kwan, M.-P. Environmental Influences on Leisure-Time Physical Inactivity in the US: An Exploration of Spatial Non-Stationarity. ISPRS Int. J. Geoinf. 2018, 7, 143. [Google Scholar] [CrossRef]
- Siordia, C.; Saenz, J.; Tom, S.E. An Introduction to Macro- Level Spatial Nonstationarity: A Geographically Weighted Regression Analysis of Diabetes and Poverty. Hum. Geogr. 2012, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Hipp, J.A.; Chalise, N. Peer Reviewed: Spatial Analysis and Correlates of County-Level Diabetes Prevalence, 2009–2010. Prev. Chronic Dis. 2015, 12, 140404. [Google Scholar] [CrossRef] [PubMed]
- Margolis, D.J.; Hoffstad, O.; Nafash, J.; Leonard, C.E.; Freeman, C.P.; Hennessy, S.; Wiebe, D.J. Location, Location, Location: Geographic Clustering of Lower-Extremity Amputation Among Medicare Beneficiaries with Diabetes. Diabetes Care 2011, 34, 2363–2367. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada 2016 Census of Population—Data Products. Available online: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/index-eng.cfm (accessed on 16 October 2022).
- City of Toronto. Population Demographics of Toronto. Available online: https://www.toronto.ca/wp-content/uploads/2019/11/99b4-TOHealthCheck_2019Chapter1.pdf (accessed on 14 October 2022).
- Toronto Open Data Portal. Neighbourhoods—City of Toronto Open Data Portal. Available online: https://open.toronto.ca/dataset/neighbourhoods/ (accessed on 16 January 2023).
- Ontario Community Health Profiles Partnership. Available online: http://www.ontariohealthprofiles.ca/dataTablesON.php?varTab=HPDtbl&select1=7 (accessed on 8 March 2022).
- ICES. Available online: https://www.ices.on.ca (accessed on 11 September 2022).
- SafeGraph. Available online: https://www.safegraph.com/ (accessed on 14 October 2022).
- Chang, S.; Pierson, E.; Koh, P.W.; Gerardin, J.; Redbird, B.; Grusky, D.; Leskovec, J. Mobility Network Models of COVID-19 Explain Inequities and Inform Reopening. Nature 2020, 589, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Kupfer, J.A.; Li, Z.; Ning, H.; Huang, X. Using Mobile Device Data to Track the Effects of the COVID-19 Pandemic on Spatiotemporal Patterns of National Park Visitation. Sustainability 2021, 13, 9366. [Google Scholar] [CrossRef]
- Zhou, H.; Kim, G.; Wang, J.; Wilson, K. Investigating the Association between the Socioeconomic Environment of the Service Area and Fast Food Visitation: A Context-Based Crystal Growth Approach. Health Place 2022, 76, 102855. [Google Scholar] [CrossRef]
- Polsky, J.Y.; Moineddin, R.; Glazier, R.H.; Dunn, J.R.; Booth, G.L. Foodscapes of Southern Ontario: Neighbourhood Deprivation and Access to Healthy and Unhealthy Food Retail. Can. J. Public Health 2014, 105, e369–e375. [Google Scholar] [CrossRef] [PubMed]
- Mahendra, A.; Polsky, J.Y.; Robitaille, É.; Lefebvre, M.; McBrien, T.; Minaker, L.M. Geographic Retail Food Environment Measures for Use in public Health. Health Promot. Chronic Dis. Prev. Can. 2017, 37, 357. [Google Scholar] [CrossRef] [PubMed]
- Powell, L.M.; Han, E.; Zenk, S.N.; Khan, T.; Quinn, C.M.; Gibbs, K.P.; Pugach, O.; Barker, D.C.; Resnick, E.A.; Myllyluoma, J.; et al. Field Validation of Secondary Commercial Data Sources on the Retail Food Outlet Environment in the U.S. Health Place 2011, 17, 1122–1131. [Google Scholar] [CrossRef] [PubMed]
- De la Fuente, F.; Saldías, M.A.; Cubillos, C.; Mery, G.; Carvajal, D.; Bowen, M.; Bertoglia, M.P. Green Space Exposure Association with Type 2 Diabetes Mellitus, Physical Activity, and Obesity: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 18, 97. [Google Scholar] [CrossRef] [PubMed]
- Hayes, C.; Kriska, A. Role of Physical Activity in Diabetes Management and Prevention. J. Am. Diet. Assoc. 2008, 108, S19–S23. [Google Scholar] [CrossRef] [PubMed]
- Richardson, E.A.; Pearce, J.; Mitchell, R.; Kingham, S. Role of Physical Activity in the Relationship between Urban Green Space and Health. Public Health 2013, 127, 318–324. [Google Scholar] [CrossRef]
- DMTI Spatial Inc. Park Sports Field Region—2019. Available online: https://geo.scholarsportal.info/#r/details/_uri@=11120733$DMTI_2019_CMCS_ParksSportsFieldRegion (accessed on 15 October 2022).
- Cheng, Y.J.; Kanaya, A.M.; Araneta, M.R.G.; Saydah, S.H.; Kahn, H.S.; Gregg, E.W.; Fujimoto, W.Y.; Imperatore, G. Prevalence of Diabetes by Race and Ethnicity in the United States, 2011–2016. JAMA 2019, 322, 2389–2398. [Google Scholar] [CrossRef]
- Ledford, C.J.W.; Seehusen, D.A.; Crawford, P.F. Geographic and Race/Ethnicity Differences in Patient Perceptions of Diabetes. J. Prim. Care Community Health 2019, 10, 2150132719845819. [Google Scholar] [CrossRef]
- Tenkorang, E.Y. Early Onset of Type 2 Diabetes among Visible Minority and Immigrant Populations in Canada. Ethn. Health 2016, 22, 266–284. [Google Scholar] [CrossRef]
- Esri Inc. ArcGIS Pro 3.0. Available online: https://www.esri.com/en-us/arcgis/products/arcgis-pro/overview (accessed on 16 January 2023).
- Chen, X. Take the Edge off: A Hybrid Geographic Food Access Measure. Appl. Geogr. 2017, 87, 149–159. [Google Scholar] [CrossRef]
- Chen, X.; Ye, X.; Widener, M.J.; Delmelle, E.; Kwan, M.-P.; Shannon, J.; Racine, E.F.; Adams, A.; Liang, L.; Jia, P. A Systematic Review of the Modifiable Areal Unit Problem (MAUP) in Community Food Environmental Research. Urban Inform. 2022, 1, 1–11. [Google Scholar] [CrossRef]
- Needham, C.; Sacks, G.; Orellana, L.; Robinson, E.; Allender, S.; Strugnell, C. A Systematic Review of the Australian Food Retail Environment: Characteristics, Variation by Geographic Area, Socioeconomic Position and Associations with Diet and Obesity. Obes. Rev. 2020, 21, e12941. [Google Scholar] [CrossRef] [PubMed]
- Leung, Y.; Mei, C.L.; Zhang, W.X. Statistical Tests for Spatial Nonstationarity Based on the Geographically Weighted Regression Model. Environ. Plan. A Econ. Space 2016, 32, 9–32. [Google Scholar] [CrossRef]
- Wheeler, D.; Tiefelsdorf, M. Multicollinearity and Correlation among Local Regression Coefficients in Geographically Weighted Regression. J. Geogr. Syst. 2005, 7, 161–187. [Google Scholar] [CrossRef]
- Brunsdon, C.; Fotheringham, A.S.; Charlton, M.E. Geographically Weighted Regression: A Method for Exploring Spatial Nonstationarity. Geogr. Anal. 1996, 28, 281–298. [Google Scholar] [CrossRef]
- Powers, S.L.; Matthews, S.A.; Mowen, A.J. Does the Relationship between Racial, Ethnic, and Income Diversity and Social Capital Vary across the United States? A County-Level Analysis Using Geographically Weighted Regression. Appl. Geogr. 2021, 130, 102446. [Google Scholar] [CrossRef]
- Gebreab, S.Y.; Diez Roux, A.V. Exploring Racial Disparities in CHD Mortality between Blacks and Whites across the United States: A Geographically Weighted Regression Approach. Health Place 2012, 18, 1006–1014. [Google Scholar] [CrossRef]
- John Fox, S.W. Car: Companion to Applied Regression. Available online: https://cran.r-project.org/package=car (accessed on 16 October 2022).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.r-project.org/ (accessed on 17 October 2022).
- Garson, G.D. Testing Statistical Assumptions; Statistical Associates Publishing: Asheboro, NC, USA, 2012. [Google Scholar]
- Bennett, G.G.; McNeill, L.H.; Wolin, K.Y.; Duncan, D.T.; Puleo, E.; Emmons, K.M. Safe to Walk? Neighborhood Safety and Physical Activity among Public Housing Residents. PLoS Med. 2007, 4, e306. [Google Scholar] [CrossRef]
- Salois, M.J. Obesity and Diabetes, the Built Environment, and the ‘Local’Food Economy in the United States, 2007. Econ. Hum. Biol. 2012, 10, 35–42. [Google Scholar] [CrossRef]
- Kwan, M.P.; Wang, J.; Tyburski, M.; Epstein, D.H.; Kowalczyk, W.J.; Preston, K.L. Uncertainties in the Geographic Context of Health Behaviors: A Study of Substance Users’ Exposure to Psychosocial Stress Using GPS Data. Int. J. Geogr. Inf. Sci. 2019, 33, 1176–1195. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | Minimum | Maximum | Mean | Median | Standard Deviation | Total |
|---|---|---|---|---|---|---|
| All ages 20+ | 5360 | 29,457 | 15,167 | 14,392 | 5419 | 2,396,337 |
| Age 20 to 44 | 2318 | 19,463 | 7241 | 6738 | 3064 | 1,144,070 |
| Age 45 to 64 | 1845 | 9726 | 4966 | 4634 | 1837 | 784,704 |
| Age 65 and above | 679 | 7628 | 2959 | 2756 | 1340 | 467,563 |
| Variable | Description | Year | Source |
|---|---|---|---|
| Dependent Variable | |||
| Type-2 Diabetes Mellitus Prevalence Rates | Total cases of diabetes by population in neighborhood | 2019 | Ontario Community Health Profiles Partnership |
| Independent Variable | |||
| Unhealthy Food Outlet Density (Count per km2) | Number of locations of limited-service (fast food) restaurants, confectionery retailers, bakeries, and convenience stores by neighborhood area | 2019 | SafeGraph |
| Green Space Density (% km2) | Area of parks and recreation spaces by neighborhood area | 2019 | DMTI Spatial Inc. |
| Medium Total Income | Median total income among recipients ($) | 2015 | 2016 Canadian Census |
| Unemployment Rate | Percentage of residents who are unemployed | 2016 | |
| Low-Education Rate | Percentage of residents who have not obtained any certificates, diplomas, or degrees | 2016 | |
| Immigration Rate | Percentage of the residents who are, or who have ever been, landed immigrants and permanent residents | 2016 | |
| Variables | Minimum | Maximum | Mean | Median | Standard Deviation |
|---|---|---|---|---|---|
| T2DM Prevalence Rate Age 20+ (%) | 2.30 | 22.50 | 12.20 | 12.00 | 4.40 |
| T2DM Prevalence Rate Age 20–44 (%) | 0.90 | 5.50 | 2.60 | 2.30 | 1.14 |
| T2DM Prevalence Rate Age 45–64 (%) | 4.70 | 31.00 | 14.60 | 13.70 | 5.81 |
| T2DM Prevalence Rate Age 65+ (%) | 14.70 | 50.00 | 31.60 | 30.90 | 7.80 |
| Green Space Density (% km2) | 7.70 | 64.00 | 19.00 | 20.30 | 8.60 |
| Unhealthy Food Outlet Density (Count per km2) | 1.66 | 52.0 | 7.6 | 12.6 | 12.4 |
| Immigration Rate (% Population) | 20.7334 | 70.2330 | 44.9463 | 45.8499 | 12.4900 |
| Low-Education Rate (% Population) | 2.4690 | 30.4626 | 13.2855 | 13.1108 | 6.1950 |
| Medium Annual Income ($) | 19,797 | 65,639 | 34,701 | 32,387 | 10,360 |
| Unemployment Rate (% Population) | 4.5272 | 12.2839 | 7.9010 | 7.4982 | 1.5618 |
| Variables | GWR Model 1 Response Variable: T2DM Prevalence Rate (Age 20 and Above) (R2 = 0.9173; Adjusted R2 = 0.8982; AIC = 581.1; Distance Band = 13.3870 km) | |||||||
|---|---|---|---|---|---|---|---|---|
| Positive Coefficient Estimates (%) | Significant Positive Coefficient Estimates (%) † | Negative Coefficient Estimates (%) | Significant Negative Coefficient Estimates (%) †† | Minimum Coefficient Estimate | Median Coefficient Estimate | Mean Coefficient Estimate | Maximum Coefficient Estimate | |
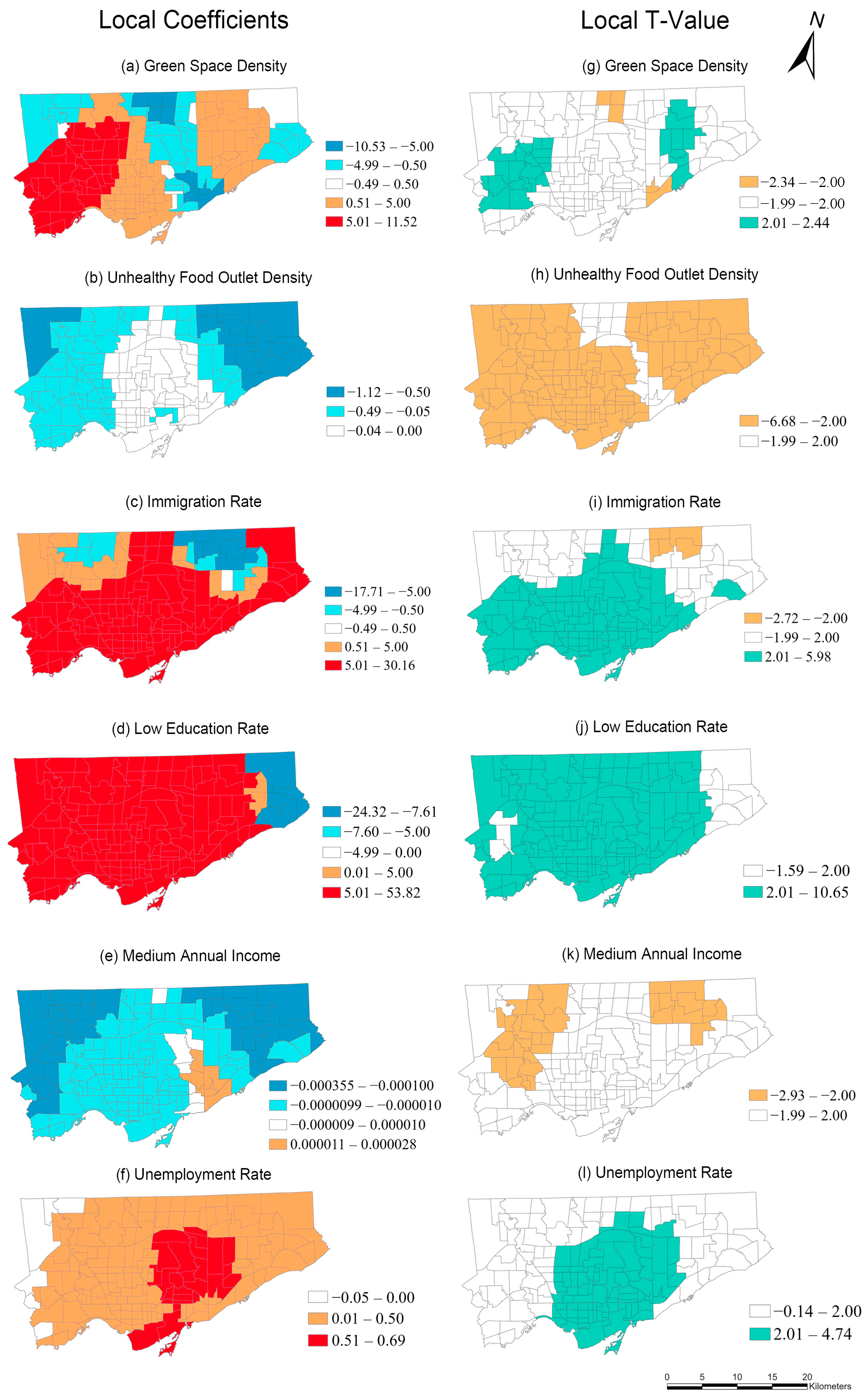
| Green Space Density (β1) | 72 | 18 | 28 | 3 | −10.5258 | 2.4558 | 11.5205 | 11.5205 |
| Unhealthy Food Outlet Density (β2) | 0 | 0 | 100 | 87 | −1.1155 | −0.0547 | −0.1761 | −0.0251 |
| Immigration Rate (β3) | 89 | 70 | 11 | 3 | −17.7147 | 8.3376 | 7.4683 | 30.153 |
| Low-Education Rate (β4) | 97 | 92 | 3 | 0 | −24.3151 | 25.9015 | 26.9508 | 53.8229 |
| Medium Annual Income (β5) | 8 | 0 | 92 | 20 | −0.000355 | −0.000042 | −0.000067 | 0.000029 |
| Unemployment Rate (β6) | 96 | 50 | 4 | 0 | −0.0475 | 0.3733 | 0.3475 | 0.6921 |
| Mean | Median | Standard Deviation | Minimum | Maximum | ||||
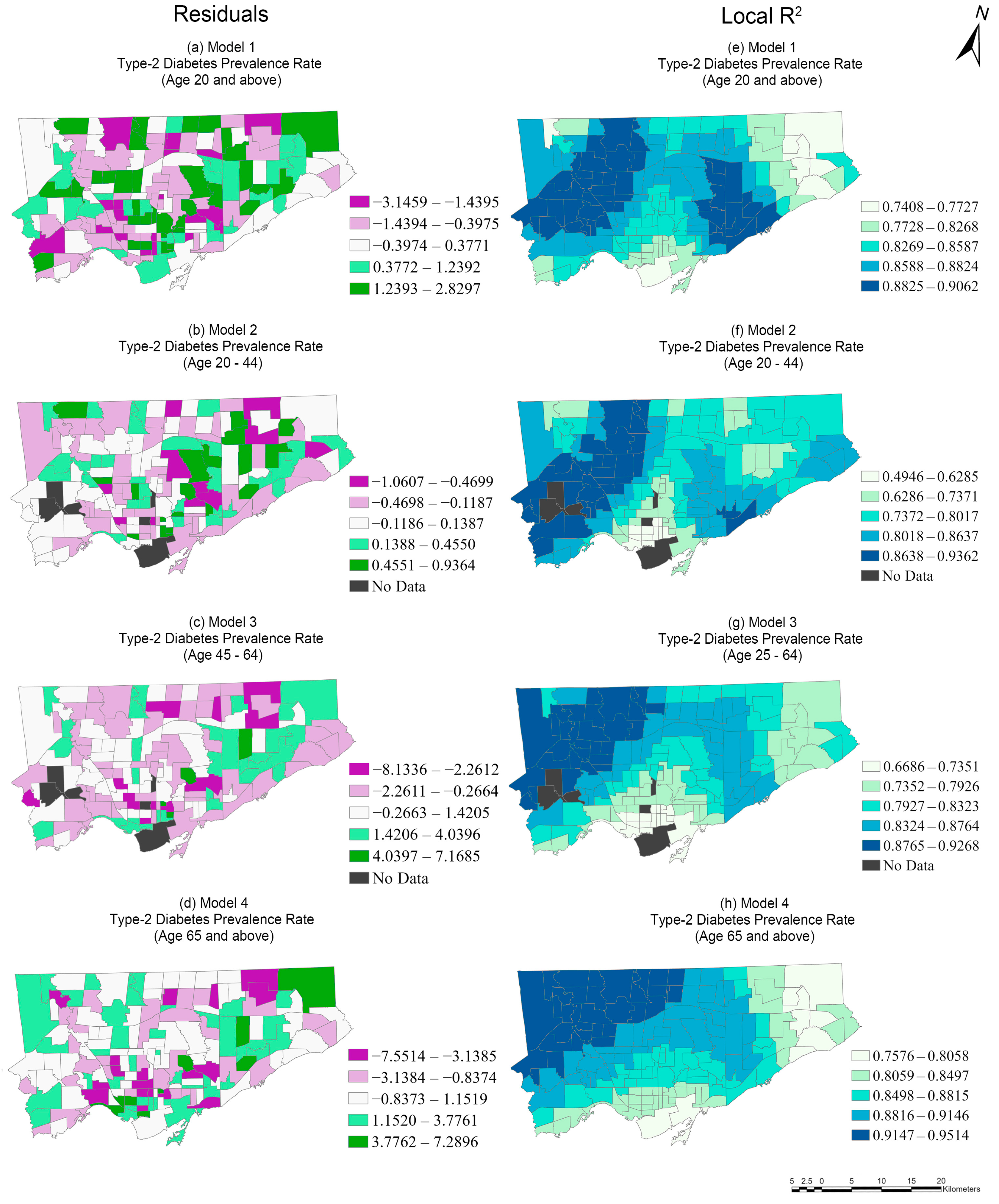
| Local R2 | 0.8565 | 0.8648 | 0.03751 | 0.7408 | 0.9063 | |||
| Residual | 0.0425 | 0.0256 | 1.2647 | −3.1460 | 2.830 | |||
| Variables | GWR Model 2 Response Variable: T2DM Prevalence Rate (Age 20 to 44) (R2 = 0.9018; Adjusted R2 = 0.8568; AIC = 223.89; Distance Band = 9.61 km) | |||||||
|---|---|---|---|---|---|---|---|---|
| Positive Coefficient Estimates (%) | Significant Positive Coefficient Estimates (%) † | Negative Coefficient Estimates (%) | Significant Negative Coefficient Estimates (%) †† | Minimum Coefficient Estimate | Median Coefficient Estimate | Mean Coefficient Estimate | Maximum Coefficient Estimate | |
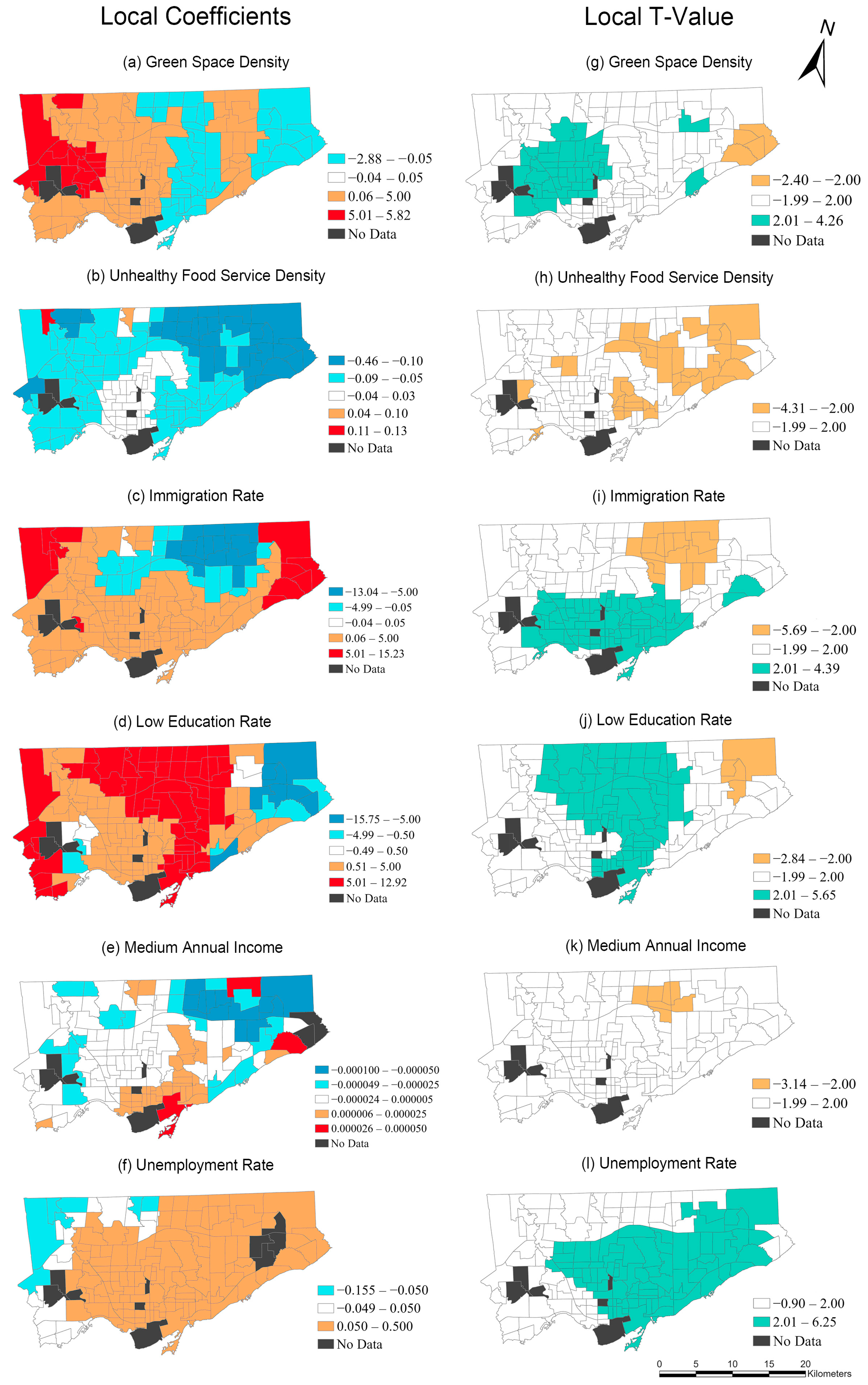
| Green Space Density (β1) | 71 | 29 | 28 | 3 | −2.8841 | 2.1885 | 1.7834 | 5.8218 |
| Unhealthy Food Outlet Density (β2) | 1 | 0 | 99 | 26 | −0.4595 | −0.0171 | 0.0588 | 0.1266 |
| Immigration Rate (β3) | 78 | 45 | 22 | 11 | −13.0359 | 2.9434 | 1.6437 | 15.2293 |
| Low-Education Rate (β4) | 88 | 45 | 11 | 3 | −15.7521 | 4.3253 | 3.9859 | 12.9259 |
| Medium Annual Income (β5) | 43 | 0 | 57 | 5 | −0.0001 | −0.000005 | −0.00001 | 0.000059 |
| Unemployment Rate (β6) | 89 | 55 | 11 | 0 | −0.1551 | 0.1621 | 0.1920 | 0.5348 |
| Mean | Median | Standard Deviation | Minimum | Maximum | ||||
| Local R2 | 0.7894 | 0.7974 | 0.0920 | 0.4946 | 0.9362 | |||
| Residual | 0.0289 | −0.0128 | 0.9730 | −3.1591 | 2.3771 | |||
| Variables | GWR Model 3 Response Variable: T2DM Prevalence Rate (Age 45 to 64) (R2 = 0.8769; Adjusted R2 = 0.8479; AIC = 705.04; Distance Band = 13.5573 km) | |||||||
|---|---|---|---|---|---|---|---|---|
| Positive Coefficient Estimates (%) | Significant Positive Coefficient Estimates (%) † | Negative Coefficient Estimates (%) | Significant Negative Coefficient Estimates (%) †† | Minimum Coefficient Estimate | Median Coefficient Estimate | Mean Coefficient Estimate | Maximum Coefficient Estimate | |
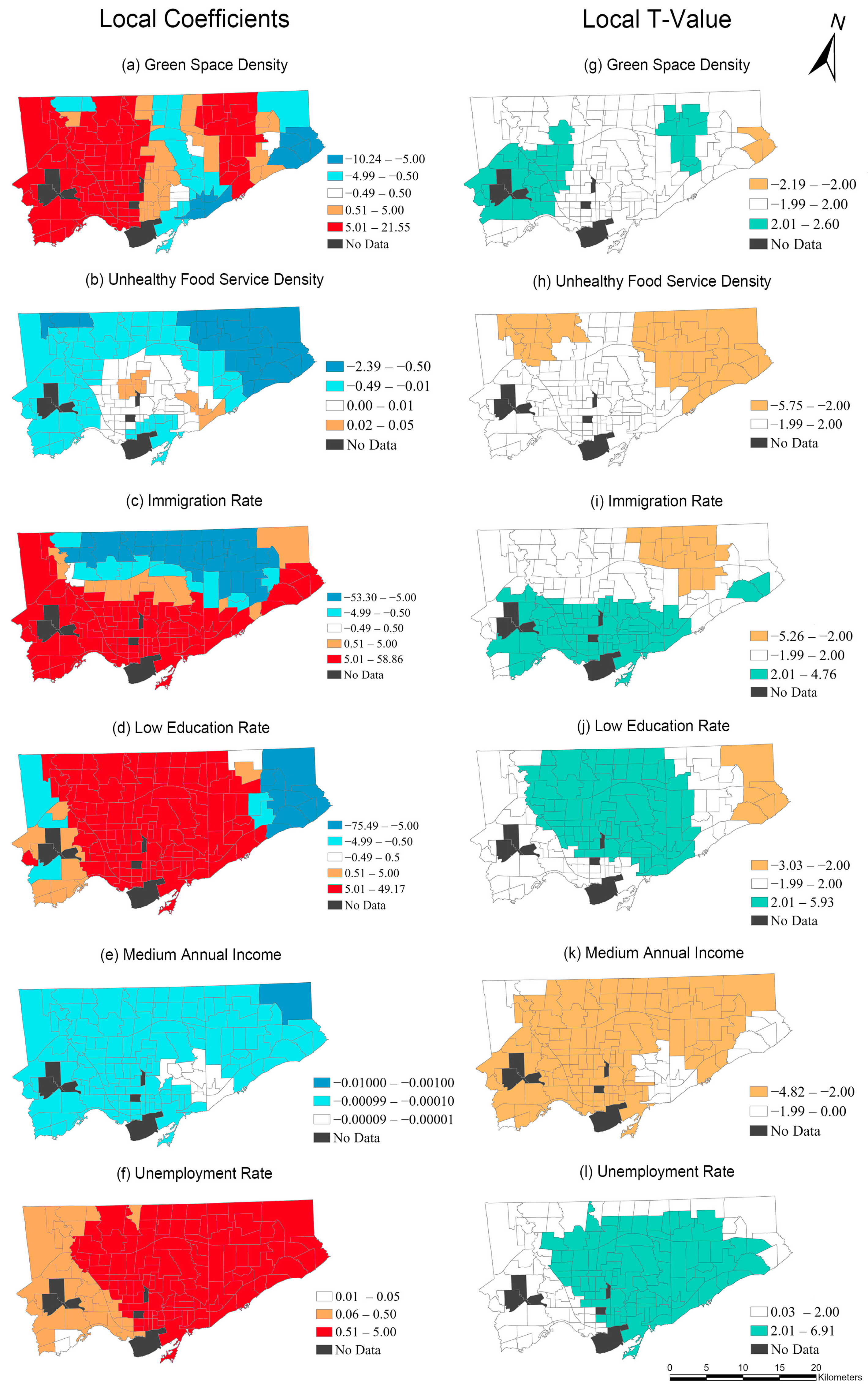
| Green Space Density (β1) | 82 | 24 | 18 | 1 | −10.2352 | 5.7940 | 6.0480 | 21.5513 |
| Unhealthy Food Outlet Density (β2) | 21 | 0 | 79 | 28 | −2.389 | −0.0204 | −0.2308 | 0.2108 |
| Immigration Rate (β3) | 71 | 49 | 29 | 11 | −59.2993 | 9.6930 | 6.3398 | 58.8553 |
| Low-Education Rate (β4) | 90 | 55 | 9 | 3 | −75.4935 | 18.1957 | 15.5273 | 49.1686 |
| Medium Annual Income (β5) | 0 | 0 | 100 | 85 | −0.001003 | −0.000164 | −0.000222 | 0.000067 |
| Unemployment Rate (β6) | 100 | 63 | 0 | 0 | 0.0134 | 0.8120 | 0.8313 | 1.8059 |
| Mean | Median | Standard Deviation | Minimum | Maximum | ||||
| Local R2 | 0.8175 | 0.8219 | 0.0607 | 0.6686 | 0.9268 | |||
| Residual | 0.1286 | −0.0097 | 2.0344 | −8.1336 | 7.1685 | |||
| Variables | GWR Model 4 Response Variable: T2DM Prevalence Rate (Age 65 and above) (R2 = 0.9012; Adjusted R2 = 0.8813; AIC = 784.66; Distance Band = 14.55 km) | |||||||
|---|---|---|---|---|---|---|---|---|
| Positive Coefficient Estimates (%) | Significant Positive Coefficient Estimates (%) † | Negative Coefficient Estimates (%) | Significant Negative Coefficient Estimates (%) †† | Minimum Coefficient Estimate | Median Coefficient Estimate | Mean Coefficient Estimate | Maximum Coefficient Estimate | |
| Green Space Density (β1) | 81 | 18 | 19 | 0 | −9.8495 | 5.6945 | 5.6301 | 26.1653 |
| Unhealthy Food Outlet Density (β2) | 62 | 3 | 38 | 17 | −2.0939 | 0.0264 | −0.1292 | 0.1017 |
| Immigration Rate (β3) | 67 | 30 | 33 | 11 | −43.7693 | 5.5009 | 2.9680 | 57.6589 |
| Low-Education Rate (β4) | 94 | 92 | 6 | 3 | −82.5982 | 48.9387 | 44.3856 | 72.6199 |
| Medium Annual Income (β5) | 0 | 0 | 100 | 99 | −0.00125 | −0.000373 | −0.000419 | −0.000261 |
| Unemployment Rate (β6) | 57 | 14 | 43 | 10 | −1.1561 | 0.1496 | 0.1120 | 1.2070 |
| Mean | Median | Standard Deviation | Minimum | Maximum | ||||
| Local R2 | 0.8759 | 0.8782 | 0.0428 | 0.7576 | 0.9514 | |||
| Residual | 0.1220 | 0.0991 | 2.4626 | −7.5515 | 7.2896 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ge, H.; Wang, J. Spatial Non-Stationarity Effects of Unhealthy Food Environments and Green Spaces for Type-2 Diabetes in Toronto. Sustainability 2023, 15, 1762. https://doi.org/10.3390/su15031762
Ge H, Wang J. Spatial Non-Stationarity Effects of Unhealthy Food Environments and Green Spaces for Type-2 Diabetes in Toronto. Sustainability. 2023; 15(3):1762. https://doi.org/10.3390/su15031762
Chicago/Turabian StyleGe, Haoxuan, and Jue Wang. 2023. "Spatial Non-Stationarity Effects of Unhealthy Food Environments and Green Spaces for Type-2 Diabetes in Toronto" Sustainability 15, no. 3: 1762. https://doi.org/10.3390/su15031762
APA StyleGe, H., & Wang, J. (2023). Spatial Non-Stationarity Effects of Unhealthy Food Environments and Green Spaces for Type-2 Diabetes in Toronto. Sustainability, 15(3), 1762. https://doi.org/10.3390/su15031762