
Valuation of a Heatwave Early Warning System for Mitigating Risks Associated with Heat-Related Illness in Central Vietnam

 , , ,
, , ,  ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
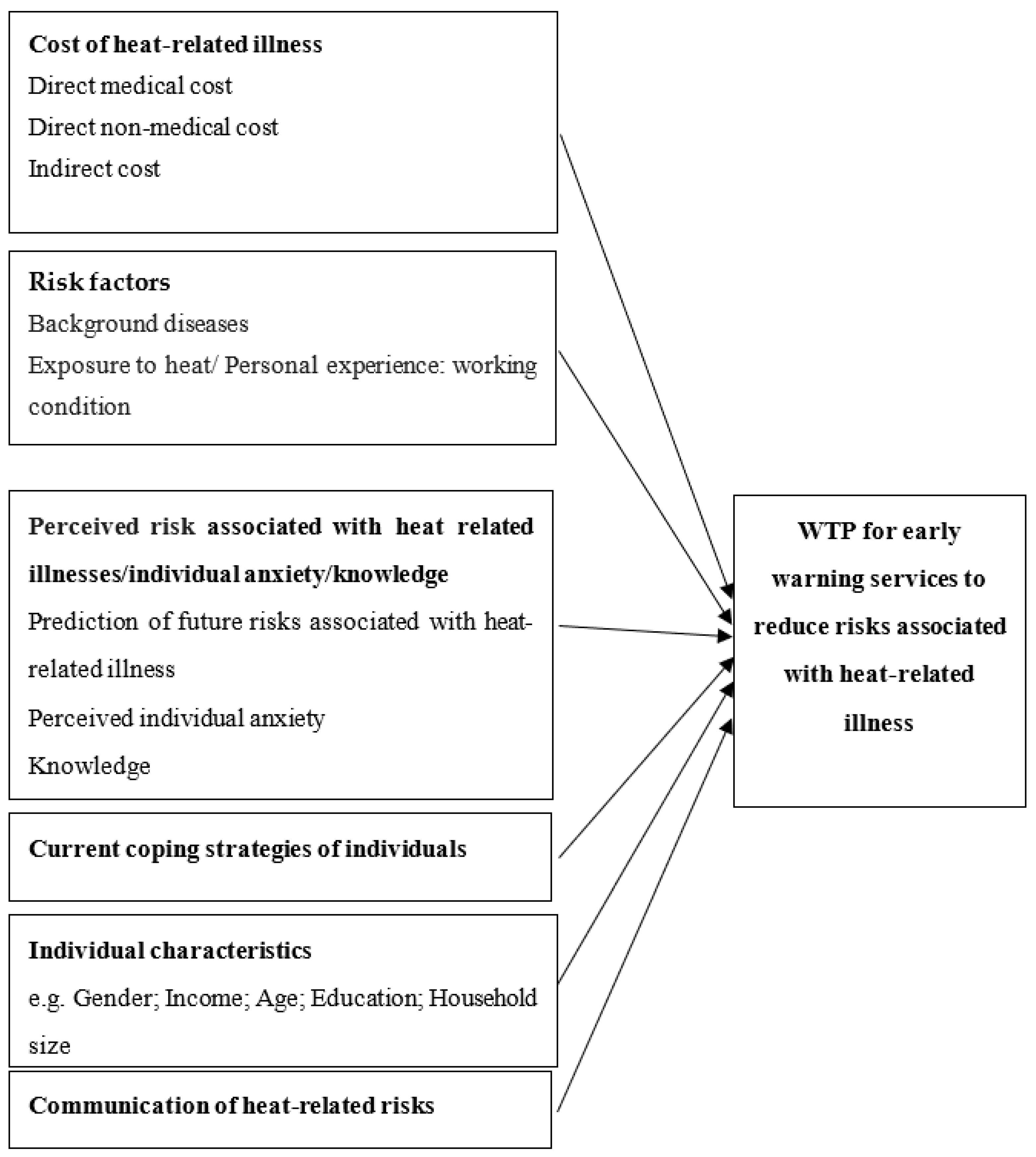
2.1. Research Framework
2.2. Estimation of the WTP for Heatwave Early Warning Services
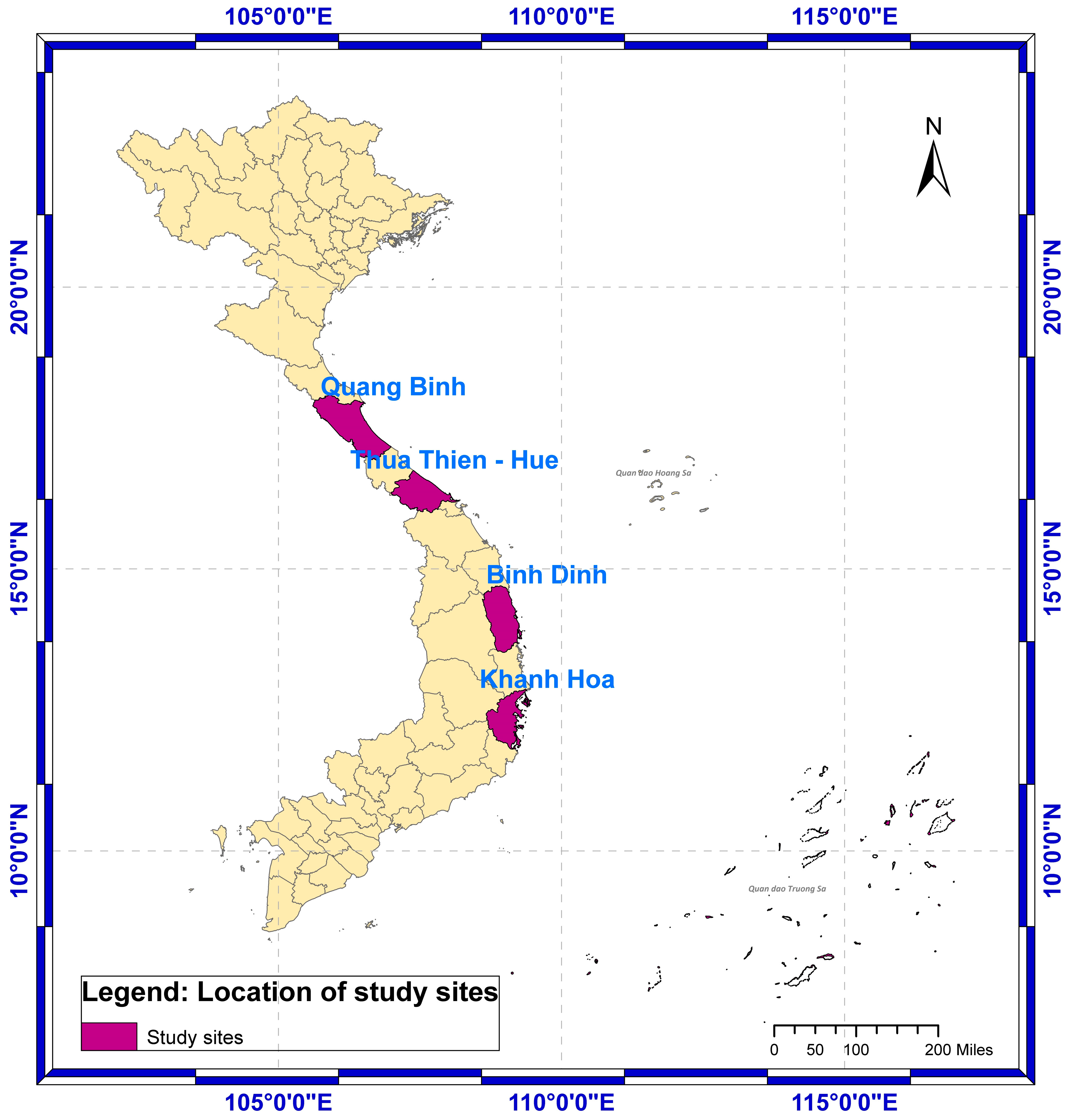
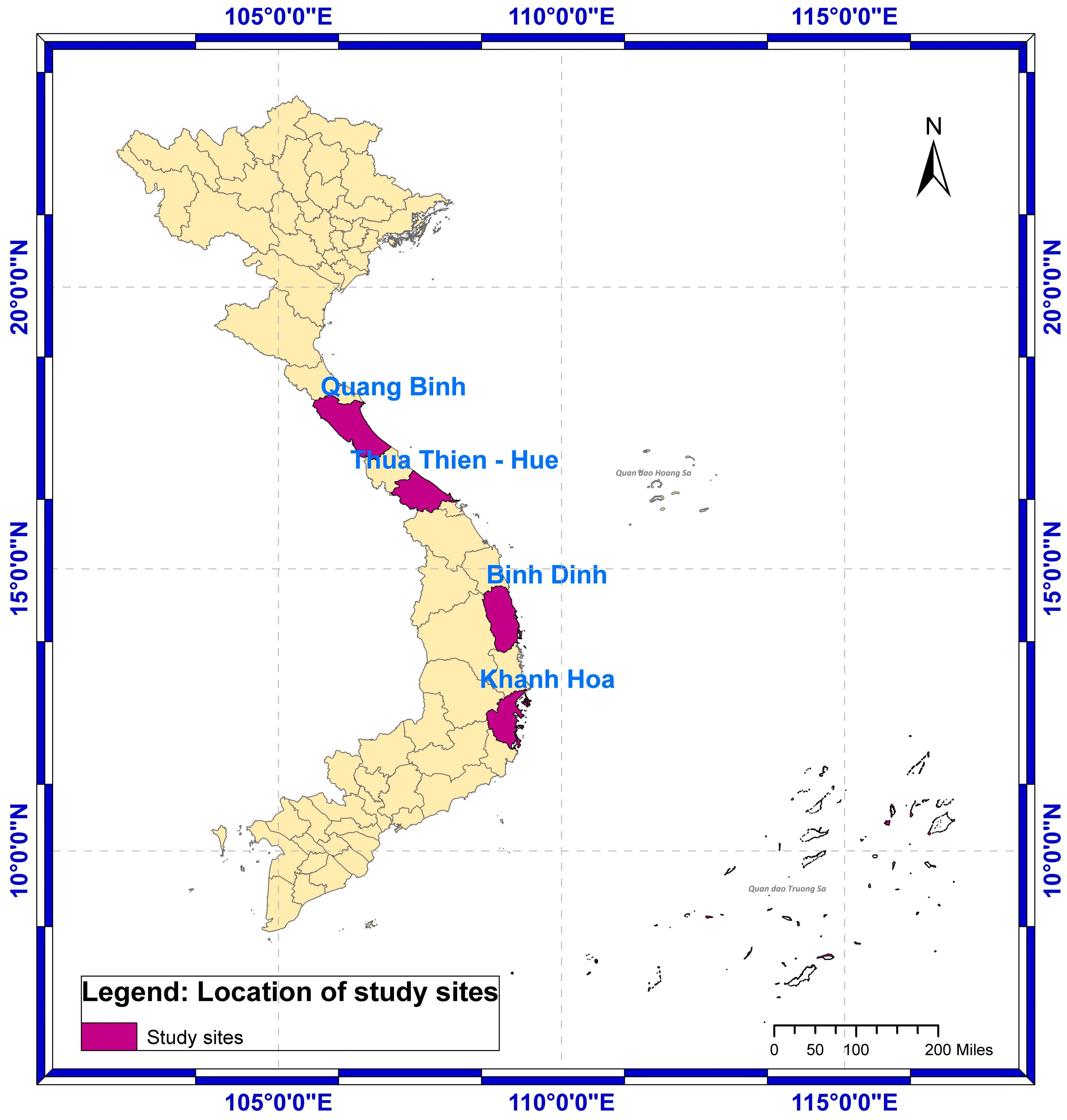
2.3. Study Area
2.4. Data Collection
2.5. Characteristics of the Sample
3. Results
3.1. Cost of Illness
3.2. Participants’ Perception and Experience with Heat-Related Illnesses
3.2.1. Experienced Symptoms with Heat-Related Stress
3.2.2. Exposure to Heat
3.2.3. Coping Strategies for Heatwaves
3.3. WTP Estimates
3.4. Determinants of the WTP
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HEWS | Heatwave Early Warning Systems |
| SMS | Short Message Service |
| WTP | Willingness To Pay |
| VND | Vietnamese Dong |
| EWS | Early Warning Systems |
| CVM | Contingent Valuation Method |
| COI | Cost Of Illness |
Appendix A

{kind=link}
{kind=link}
| Description | Value | Expected Sign | ||
|---|---|---|---|---|
| 1 | Prob(Yes) | Probability of an individual is willing to pay for the SMS-based HEWS to mitigate health risks/illness associated with heatwaves | 1 = Yes; 0 = No | |
| 2 | Bid | Bid levels (annually) (1000 VND) | 5 levels | − |
| Cost of illness | ||||
| 3 | Direct medical cost | Annual direct medical cost related heat illnesses | Continuous | + |
| 4 | Direct non-medical cost | Annual direct non-medical cost related heat illnesses | Continuous | + |
| 5 | Indirect cost | Indirect cost—Annual indirect cost related heat illnesses | Continuous | + |
| Individual relationship with risk | ||||
| 6 | Background diseases | Number of background diseases (Heart disease, Asthma, COPD, Respiratory disease (chronic bronchitis, bronchiectasis), High blood pressure, Diabetes, Other chronic disease) | Numeric | + |
| 7 | Exposure | Exposure to heat: working condition—To what extent is your job exposed to the heat? | Completely contactless (1) Less exposure (2) Moderate exposure (3) Frequent contact (4) Very often in contact (5) | +/− |
| Perceived risk associated with heat related illnesses | ||||
| 8 | Future risk | Prediction of future risks associated with heat related illness—In your opinion, how likely is the probability of prolonged/severe/peak heatwaves in Central Vietnam increase in the future/or in the next 10 years? | 1 = likely and very likely 0 = otherwise | + |
| 9 | Anxiety | Perceived individual anxiety—How worried are you about the effects of heat stroke on yourself? | Extremely concerned/anxious (1) Concern (2) Quite Concern (3) Little Concern (4) No worries at all (5) | + |
| 10 | Knowledge | Knowledge of heat related illnesses | Numeric, Number of correct answers | + |
| 11 | Current adaptation/coping strategies of individual (Cope) | |||
| Coping strategies | Cop1. Buy/use air conditioner Cop2. Buy/use fan/ceiling fan Cop3. Plant trees around the house Cop4. Stay indoors/stay out of the sun Cop5. Shower several times a day Cop6. Use thin clothes Cop7. Work early in the morning or late in the evening Cop8. Swim Cop9. Upgrade/repair house features (e.g., thick walls, high ceilings, insulation) | 1 = Yes; 0 = No | +/− | |
| Individual characteristics | ||||
| 12 | Gender | Gender of the respondents | 1 = Male, 0 = Female | |
| 13 | Age | Age of the respondent in years | Continuous | +/− |
| 14 | Income | Household income level | Numeric | |
| 15 | Education | Education level of the participant | Numeric | |
| 16 | Household size | Number of persons living in the family | Persons | +/− |
| Communication of heat related risks | ||||
| 17 | Channel | Total channels received health related warnings during the last 5 years? | Numeric, from 1 to 8 channels | +/− |
Appendix B. Valuation Scenario
Appendix C
| 5% | 10% | 15% | 20% | 25% | 30% | 35% | 40% | 45% | 50% | |
|---|---|---|---|---|---|---|---|---|---|---|
| Total population for the study area of 4 provinces (‘000 persons) | 237.10 | 474.21 | 711.31 | 948.42 | 1185.52 | 1422.62 | 1659.73 | 1896.83 | 2133.93 | 2371.04 |
| Total affected population for the study area of 4 provinces (‘000 persons) | 71.13 | 142.26 | 213.39 | 284.52 | 355.66 | 426.79 | 497.92 | 569.05 | 640.18 | 711.31 |
| WTP for the study area of 4 provinces (‘000 VND) | 20,137,933 | 40,275,866 | 60,413,798 | 80,551,731 | 100,689,664 | 120,827,597 | 140,965,530 | 161,103,462 | 181,241,395 | 201,379,328 |
| WTP for the study area of 4 provinces (USD) | 875,562 | 1,751,125 | 2,626,687 | 3,502,249 | 4,377,811 | 5,253,374 | 6,128,936 | 7,004,498 | 7,880,061 | 8,755,623 |
| 5% | 10% | 15% | 20% | 25% | 30% | 35% | 40% | 45% | 50% | |
|---|---|---|---|---|---|---|---|---|---|---|
| Total population for the Central Coast of Vietnam (‘000 persons) | 1009.36 | 2018.73 | 3028.09 | 4037.46 | 5046.82 | 6056.19 | 7065.55 | 8074.92 | 9084.28 | 10,093.65 |
| Total affected population for the Central Coast of Vietnam (‘000 persons) | 302.81 | 605.62 | 908.43 | 1211.24 | 1514.05 | 1816.86 | 2119.67 | 2422.48 | 2725.28 | 3028.09 |
| WTP for the Central Coast of Vietnam (‘000 VND) | 85,728,368 | 171,456,736 | 257,185,103 | 342,913,471 | 428,641,839 | 514,370,207 | 600,098,575 | 685,826,943 | 771,555,310 | 857,283,678 |
| WTP for Central Coast of Vietnam (USD) | 3,727,320 | 7,454,641 | 11,181,961 | 14,909,281 | 18,636,602 | 22,363,922 | 26,091,242 | 29,818,563 | 33,545,883 | 37,273,203 |
References
- Miah, M.R.; Hasan, M.M.; Parisha, J.T.; Shahriar, C.S.; Sayok, A.K.; Chowdhury, S.H. Adverse Global Health Impacts Due to the Proliferation of Man-Made Technological Heatwaves. Resour. Environ. 2022, 12, 67–75. [Google Scholar]
- Tran, D.N.; Doan, V.Q.; Nguyen, V.T.; Khan, A.; Thai, P.K.; Cunrui, H.; Chu, C.; Schak, E.; Phung, D. Spatial patterns of health vulnerability to heatwaves in Vietnam. Int. J. Biometeorol. 2020, 64, 863–872. [Google Scholar] [CrossRef] [PubMed]
- Casanueva, A.; Burgstall, A.; Kotlarski, S.; Messeri, A.; Morabito, M.; Flouris, A.D.; Nybo, L.; Spirig, C.; Schwierz, C. Overview of existing heat-health warning systems in Europe. Int. J. Environ. Res. Public Health 2019, 16, 2657. [Google Scholar] [CrossRef] [PubMed]
- Nhung, N.T.T.; Hoang, L.T.; Tuyet Hanh, T.T.; Toan, L.Q.; Thanh, N.D.; Truong, N.X.; Son, N.A.; Van Nhat, H.; Quyen, N.H.; Van Nhu, H. Effects of Heatwaves on Hospital Admissions for Cardiovascular and Respiratory Diseases, in Southern Vietnam, 2010–2018: Time Series Analysis. Int. J. Environ. Res. Public Health 2023, 20, 3908. [Google Scholar] [CrossRef]
- Tan, N.Q.; Dinh, N.C.; Linh, N.H.K.; Hung, P.X.; Kien, N.D.; Phuong, T.T.; Tinh, B.D. Climate change vulnerability and poverty nexus: Evidence from coastal communities in central Vietnam. J. Agric. Environ. Int. Dev. 2023, 117, 61–84. [Google Scholar] [CrossRef]
- Burkart, K.G.; Brauer, M.; Aravkin, A.Y.; Godwin, W.W.; Hay, S.I.; He, J.; Iannucci, V.C.; Larson, S.L.; Lim, S.S.; Liu, J.; et al. Estimating the cause-specific relative risks of non-optimal temperature on daily mortality: A two-part modelling approach applied to the Global Burden of Disease Study. Lancet 2021, 398, 685–697. [Google Scholar] [CrossRef]
- Nguyen, C.V.; Nguyen, M.H.; Nguyen, T.T. The impact of cold waves and heat waves on mortality: Evidence from a lower middle-income country. Health Econ. 2023, 32, 1220–1243. [Google Scholar] [CrossRef]
- Eckstein, D.; Künzel, V.; Schäfer, L.; Winges, M. Global Climate Risk Index 2020; Who Suffers Most from Extreme Weather Events? Weather-Related Loss Events in 2018 and 1999 to 2018; Germanwatch e.V.: Bonn, Germany, 2020; Available online: https://germanwatch.org/sites/germanwatch.org/files/20-2-01e%20Global%20Climate%20Risk%20Index%202020_10.pdf (accessed on 30 April 2023).
- VC (Visual Crossing Weather) Record-Setting Heat Wave Hits Vietnam and Southeast Asia. 2023. Available online: https://www.visualcrossing.com/resources/blog/record-setting-heat-wave-hits-vietnam-and-southeast-asia/ (accessed on 20 May 2023).
- Petzold, J.; Mose, L. Urban Greening as a Response to Climate-Related Heat Risk: A Social–Geographical Review. Sustainability 2023, 15, 4996. [Google Scholar] [CrossRef]
- Zuo, J.; Pullen, S.; Palmer, J.; Bennetts, H.; Chileshe, N.; Ma, T. Impacts of heat waves and corresponding measures: A review. J. Clean. Prod. 2015, 92, 1–12. [Google Scholar] [CrossRef]
- Himmler, S.; van Exel, J.; Perry-Duxbury, M.; Brouwer, W. Willingness to pay for an early warning system for infectious diseases. Eur. J. Health Econ. 2020, 21, 763. [Google Scholar] [CrossRef]
- Perry-Duxbury, M.; van Exel, J.; Brouwer, W. How to value safety in economic evaluations in health care? A review of applications in different sectors. Eur. J. Health Econ. 2019, 20, 1041–1061. [Google Scholar] [CrossRef] [PubMed]
- Adélaïde, L.; Chanel, O.; Pascal, M. Health effects from heat waves in France: An economic evaluation. Eur. J. Health Econ. 2021, 23, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Toloo, G.; FitzGerald, G.; Aitken, P.; Verrall, K.; Tong, S. Evaluating the effectiveness of heat warning systems: Systematic review of epidemiological evidence. Int. J. Public Health 2013, 58, 667–681. [Google Scholar] [CrossRef]
- Lowe, D.; Ebi, K.L.; Forsberg, B. Heatwave early warning systems and adaptation advice to reduce human health consequences of heatwaves. Int. J. Environ. Res. Public Health 2011, 8, 4623–4648. [Google Scholar] [CrossRef] [PubMed]
- Linares, C.; Martinez, G.S.; Kendrovski, V.; Diaz, J. A new integrative perspective on early warning systems for health in the context of climate change. Environ. Res. 2020, 187, 109623. [Google Scholar] [CrossRef]
- Lan-Huong, T.T.; Van-Anh, D.T.; Dat, T.T.; Truong, D.D.; Tam, D.D. Disaster risk management system in Vietnam: Progress and challenges. Heliyon 2022, 8, e10701. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Hyun, M.-K.; Yoo, S.-H. Households’ Willingness to Pay for Interactive Charging Stations for Vehicle to Grid System in South Korea. Sustainability 2023, 15, 11563. [Google Scholar] [CrossRef]
- Alberini, A.; Hunt, A.; Markandya, A. Willingness to pay to reduce mortality risks: Evidence from a three-country contingent valuation study. Environ. Resour. Econ. 2006, 33, 251–264. [Google Scholar] [CrossRef]
- Corso, P.S.; Ingels, J.B.; Roldos, M.I. A comparison of willingness to pay to prevent child maltreatment deaths in Ecuador and the United States. Int. J. Environ. Res. Public Health 2013, 10, 1342–1355. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, C.H.E.N.; Jie, B.A.N.; Zhao, J.H.; Xu, D.D.; Zhu, P.F.; Li, T.T. Willingness to Pay for Measures of Managing the Health Effects of Heat Wave in Beijing, China: A Cross-sectional Survey. Biomed. Environ. Sci. 2016, 29, 628–638. [Google Scholar] [CrossRef]
- Oloukoi, G.; Bob, U.; Jaggernath, J. Perception and trends of associated health risks with seasonal climate variation in Oke-Ogun region, Nigeria. Health Place 2014, 25, 47–55. [Google Scholar] [CrossRef] [PubMed]
- WHO (World Health Organization). WHO Guide to Identifying the Economic Consequences of Disease and Injury. 2009. Available online: https://apps.who.int/iris/bitstream/handle/10665/137037/9789241598293_eng.pdf (accessed on 20 January 2023).
- Khan, N.I.; Brouwer, R.; Yang, H. Household’s willingness to pay for arsenic safe drinking water in Bangladesh. J. Environ. Manag. 2014, 143, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Georgiou, S.; Langford, I.H.; Bateman, I.J.; Turner, R.K. Determinants of individuals’ willingness to pay for perceived reductions in environmental health risks: A case study of bathing water quality. Environ. Plan. A 1998, 30, 577–594. [Google Scholar] [CrossRef]
- Gerking, S.; De Haan, M.; Schulze, W. The marginal value of job safety: A contingent valuation study. J. Risk Uncertain. 1988, 1, 185–199. [Google Scholar] [CrossRef]
- Hunter, P.D.; Hanley, N.; Czajkowski, M.; Mearns, K.; Tyler, A.N.; Carvalho, L.; Codd, G.A. The effect of risk perception on public preferences and willingness to pay for reductions in the health risks posed by toxic cyanobacterial blooms. Sci. Total Environ. 2012, 426, 32–44. [Google Scholar] [CrossRef]
- Gyrd-Hansen, D.; Halvorsen, P.A.; Kristiansen, I.S. Willingness-to-pay for a statistical life in the times of a pandemic. Health Econ. 2008, 17, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Pham, K.H.; Le Thi, Q.X.; Petrie, D.J.; Adams, J.; Doran, C.M. Households’ willingness to pay for a motorcycle helmet in Hanoi, Vietnam. Appl. Health Econ. Health Policy 2008, 6, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Akompab, D.A.; Peng, B.; Susan, W.; Grant, J.; Walker, I.A.; Augoustinos, M. Heat Waves and Climate Change: Applying the Health Belief Model to Identify Predictors of Risk Perception and Adaptive Behaviours in Adelaide, Australia. Int. J. Environ. Res. Public Health 2013, 10, 2164–2184. [Google Scholar] [CrossRef]
- Carlsson, F.; Johansson-Stenman, O.; Martinsson, P. Is transport safety more valuable in the air? J. Risk Uncertain. 2004, 28, 147–163. Available online: http://www.jstor.org/stable/41761136 (accessed on 10 July 2023). [CrossRef]
- Mofadal, A.I.; Kanitpong, K.; Jiwattanakulpaisarn, P. Analysis of pedestrian accident costs in Sudan using the willingness-to-pay method. Accid. Anal. Prev. 2015, 78, 201–211. [Google Scholar] [CrossRef]
- Halvorsen, B. Ordering effects in contingent valuation surveys. Environ Resour. Econ. 1996, 8, 485–499. [Google Scholar] [CrossRef]
- Henson, S. Consumer willingness to pay for reductions in the risk of food poisoning in the UK. J. Agric. Econ. 1996, 47, 403–420. [Google Scholar] [CrossRef]
- My, N.H.D.; Kien, N.D.; Hung, P.X.; Anh, L.T.Q. Does the value of water-related ecosystem services capture water scarcity? Application to rice farming in the Mekong Delta of Vietnam? Water Econ. Policy 2023, 2350006. [Google Scholar] [CrossRef]
- Agyekum, T.P.; Antwi-Agyei, P.; Dougill, A.J. The contribution of weather forecast information to agriculture, water, and energy sectors in East and West Africa: A systematic review. Front. Environ. Sci. 2022, 10, 935696. [Google Scholar] [CrossRef]
- Nkiaka, E.; Taylor, A.; Dougill, A.J.; Antwi-Agyei, P.; Fournier, N.; Bosire, E.N.; Konte, O.; Lawal, K.A.; Mutai, B.; Mwangi, E. Identifying user needs for weather and climate services to enhance resilience to climate shocks in sub-Saharan Africa. Environ. Res. Lett. 2019, 14, 123003. [Google Scholar] [CrossRef]
- Awolala, D.; Mutemi, J.; Adefisan, E.; Antwi-Agyei, P.; Taylor, A.; Muita, R.; Bosire, E.; Mutai, B.; Nkiaka, E. Economic Value and Latent Demand for Agricultural Drought Forecast: Emerging Market for Weather and Climate Information in Central-Southern Nigeria. Clim. Risk Manag. 2023, 39, 100478. [Google Scholar] [CrossRef]
- Abdeta, D.; Ayana, A.N.; Bekele, Y. Willingness to pay for forest conservation: Evidence from a contingent valuation survey analysis in Southwest Ethiopia. Glob. Ecol. Conserv. 2023, 46, e02551. [Google Scholar] [CrossRef]
- Krinsky, I.; Robb, A.L. On approximating the statistical properties of elasticities. Rev. Econ. Stat. 1986, 68, 715–719. [Google Scholar] [CrossRef]
- General Statistics Office of Vietnam (GSO). 2023. Available online: https://www.gso.gov.vn/ (accessed on 10 July 2023).
- Dang, T.A.T.; Wraith, D.; Bambrick, H.; Dung, N.; Truc, T.T.; Tong, S.; Naish, S.; Dunne, M.P. Short-term effects of temperature on hospital admissions for acute myocardial infarction: A comparison between two neighboring climate zones in Vietnam. Environ. Res. 2019, 175, 167–177. [Google Scholar] [CrossRef]
- Phung, D.; Nguyen, H.X.; Nguyen, H.L.T.; Luong, A.M.; Do, C.M.; Tran, Q.D.; Chu, C. The effects of socioecological factors on variation of communicable diseases: A multiple-disease study at the national scale of Vietnam. PLoS ONE 2018, 13, e0193246. [Google Scholar] [CrossRef]
- Ngo-Duc, T. Climate Change in the Coastal Regions of Vietnam. In Coastal Disasters and Climate Change in Vietnam; Thao, N.D., Takagi, H., Esteban, M., Eds.; Elsevier: Oxford, UK, 2014; pp. 175–198. [Google Scholar]
- Hodgson, T.A.; Meiners, M.R. Cost-of-illness methodology: A guide to current practices and procedures. The Milbank Memorial Fund Quarterly. Health Soc. 1982, 60, 429–462. [Google Scholar] [CrossRef]
- Rice, D.P. Cost of illness studies: What is good about them? Inj. Prev. 2000, 6, 177–179. [Google Scholar] [CrossRef] [PubMed]
- Penn, J.; Hu, W. Cheap talk efficacy under potential and actual Hypothetical Bias: A meta-analysis. J. Environ. Econ. Manag. 2019, 96, 22–35. [Google Scholar] [CrossRef]
- Sajise, A.J.; Samson, J.N.; Quiao, L.; Sibal, J.; Raitzer, D.A.; Harder, D. Contingent Valuation of Nonmarket Benefits in Project Economic Analysis: A Guide to Good Practice; Asian Development Bank: Mandaluyong, Philippines, 2021; Available online: https://www.adb.org/publications/valuation-nonmarket-benefits-project-economic-analysis-guide (accessed on 5 July 2023).
- Gunatilake, H.; Yang, J.C.; Pattanayak, S.; Choe, K.A. Good Practices for Estimating Reliable Willingness-to-Pay Values in the Water Supply and Sanitation Sector; Asian Development Bank: Mandaluyong, Philippines, 2007; ISSN 1655-5236. Available online: https://www.adb.org/publications/good-practices-estimating-reliable-willingness-pay-values-water-supply-sector (accessed on 5 July 2023).
- Beckmann, S.K.; Hiete, M.; Schneider, M.; Beck, C. Heat adaptation measures in private households: An application and adaptation of the protective action decision model. Humanit. Soc. Sci. Commun. 2021, 8, 227. [Google Scholar] [CrossRef]
- Williams, S.; Hanson-Easey, S.; Nitschke, M.; Howell, S.; Nairn, J.; Beattie, C.; Wynwood, G.; Bi, P. Heat-health warnings in regional Australia: Examining public perceptions and responses. Environ. Hazards 2019, 18, 287–310. [Google Scholar] [CrossRef]
- Climate Analytics. Decarbonising South & South East Asia-Country Profile-Vietnam. 2019. Available online: https://climateanalytics.org/media/decarbonisingasia2019-profile-vietnam-climateanalytics.pdf (accessed on 20 June 2023).
- Tuan, T.H.; My, N.H.D.; Anh, L.T.Q.; Van Toan, N. Using contingent valuation method to estimate the WTP for mangrove restoration under the context of climate change: A case study of Thi Nai lagoon, Quy Nhon city, Vietnam. Ocean Coast. Manag. 2014, 95, 198–212. [Google Scholar] [CrossRef]
- Anaman, K.A.; Quaye, R.; Amankwah, E. Evaluation of public weather services by users in the formal services sector in Accra. Ghana. Mod. Econ. 2017, 8, 921–945. [Google Scholar] [CrossRef]
- Parker, D.J.; Blyth, A.M.; Woolnough, S.J.; Dougill, A.J.; Bain, C.L.; de Coning, E.; Diop-Kane, M.; Foamouhoue, A.K.; Lamptey, B.; Ndiaye, O.; et al. The African SWIFT project: Growing science capability to bring about a revolution in weather prediction. Bull. Am. Meteorological Soc. 2021, 103, E349–E369. [Google Scholar] [CrossRef]
- Harvey, B.; Huang, Y.-S.; Araujo, J.; Vincent, K.; Roux, J.-P.; Rouhaud, E.; Visman, E. Mobilizing climate information for decision-making in Africa: Contrasting user-centered and knowledge-centered approaches. Front. Clim. 2021, 2, 589282. [Google Scholar] [CrossRef]
- OECD (Organization for Economic Co-Operation and Development). The Economic Appraisal of Environmental Projects and Policies: A Practical Guide; OECD: Paris, France, 1995. [Google Scholar]

| Items | % | Items | % |
|---|---|---|---|
| Gender | Household income (million VND/month) | ||
| Male | 54.8 | Less than 3 | 9.5 |
| Female | 45.2 | 3 to less than 5 | 10.8 |
| Age (year) | 65.5 a (14.9) b | 5 to less than 10 | 35.5 |
| Education | 10 and higher | 44.2 | |
| Primary school and lower | 26.0 | ||
| Secondary school | 25.3 | ||
| High school | 19.5 | ||
| Colleges | 17.3 | ||
| University and higher | 12.0 | ||
| Cost Items | 1000 VND | % |
|---|---|---|
| Direct costs | 23,801.3 | 79.80 |
| 14,230.9 | 59.79 |
| 9570.3 | 40.21 |
| Indirect costs | 6025.6 | 20.20 |
| Total | 29,858.6 | 100.00 |
| Heat-Related Illnesses | Strongly Disagree (1) | Disagree (2) | Neutral (3) | Agree (4) | Strongly Agree (5) |
|---|---|---|---|---|---|
| Cramps due to heatstroke | 2.0 | 24.3 | 26.3 | 44.0 | 3.5 |
| Heat stroke | 1.3 | 5.5 | 13.8 | 58.5 | 21.0 |
| Heat exhaustion/fatigue due to heat | 1.0 | 11.0 | 19.0 | 54.0 | 15.0 |
| Feeling constrained/unable to do activities that I enjoy | 0.8 | 12.0 | 18.8 | 57.8 | 10.8 |
| Headache | 1.0 | 5.8 | 10.8 | 63.0 | 19.5 |
| Sleepless | 0.8 | 6.0 | 12.0 | 61.0 | 20.3 |
| Disorientation/unable to function normally/unable to concentrate on work | 1.3 | 12.5 | 25.3 | 51.7 | 9.3 |
| Mentally exhausting/draining | 0.5 | 4.3 | 9.8 | 66.4 | 19.0 |
| Coping Strategies | %Yes |
|---|---|
| 1. Buy/use air conditioner | 54.5 |
| 2. Buy/use fan/ceiling fan | 94.5 |
| 3. Plant trees around the house | 83.5 |
| 4. Stay indoors/stay out of the sun | 86.8 |
| 5. Shower several times a day | 52.0 |
| 6. Use thin clothes | 94.3 |
| 7. Work early in the morning or late in the evening | 66.3 |
| 8. Swim in pool | 29.3 |
| 9. Upgrade/repair house features (e.g., thick walls, high ceilings, insulation) | 36.3 |
| Items | VND/Year/Person |
|---|---|
| Mean/median | 283,110 |
| Krinsky and Robb (95%) C.I. | |
| Lower bound | 233,720 |
| Upper bound | 335,720 |
| Coef. | Robust S.E. | z | p-Value | |
|---|---|---|---|---|
| Constant | −5.831 | 4.308 | −1.35 | 0.176 |
| Bid | −0.003 | 0.0002 | −15.66 | 0.000 |
| Cost of heat related illness | ||||
| Direct medical cost | 0.198 | 0.057 | 3.46 | 0.001 |
| Direct non-medical cost | 0.241 | 0.102 | 2.36 | 0.018 |
| Indirect cost | −0.103 | 0.180 | −0.57 | 0.566 |
| Individual relationship with risk | ||||
| Background diseases | ||||
| 1 | 0.979 | 0.015 | 65.05 | 0.000 |
| 2 | 0.787 | 0.044 | 17.84 | 0.000 |
| 3 | 1.235 | 0.150 | 8.23 | 0.000 |
| 4 or more | 1.016 | 0.310 | 3.27 | 0.001 |
| Exposure to heat: working condition: base = 1 | ||||
| 2 | 0.323 | 0.066 | 4.92 | 0.000 |
| 3 | 0.640 | 0.082 | 7.79 | 0.000 |
| 4 | 0.887 | 0.283 | 3.13 | 0.002 |
| 5 | 1.213 | 0.818 | 1.48 | 0.138 |
| Perceived risk associated with heat related illnesses | ||||
| Knowledge | −0.011 | 0.084 | −1.25 | 0.212 |
| Anxiety | 0.088 | 0.323 | 0.27 | 0.787 |
| Future risk | 0.076 | 0.111 | 0.69 | 0.493 |
| Coping strategies (Cop) | ||||
| Cop1 | 0.314 | 0.185 | 1.70 | 0.090 |
| Cop2 | 0.469 | 0.192 | 2.45 | 0.014 |
| Cop3 | −0.040 | 0.122 | −0.33 | 0.745 |
| Cop4 | 0.392 | 0.210 | 1.87 | 0.062 |
| Cop5 | −0.273 | 0.172 | −1.59 | 0.112 |
| Cop6 | −1.091 | 0.208 | −5.25 | 0.000 |
| Cop7 | 0.093 | 0.121 | 0.77 | 0.441 |
| Cop8 | 0.250 | 0.025 | 10.08 | 0.000 |
| Cop9 | −0.387 | 0.080 | −4.82 | 0.000 |
| Individual characteristics | ||||
| Gender (base = Female) | −0.062 | 0.303 | −0.21 | 0.837 |
| Age | −0.004 | 0.006 | −0.67 | 0.502 |
| Income: base = 1 | ||||
| 2 | 0.434 | 0.303 | 1.44 | 0.151 |
| 3 | 0.406 | 0.194 | 2.09 | 0.037 |
| 4 | 0.814 | 0.116 | 6.99 | 0.000 |
| 5 | 0.490 | 0.144 | 3.39 | 0.001 |
| Education | 0.207 | 0.073 | 2.85 | 0.004 |
| Household size | 0.092 | 0.007 | 12.67 | 0.000 |
| Communication of heat related risks | ||||
| Channel | 0.069 | 0.032 | 2.14 | 0.032 |
| Number of observations | 368 | |||
| Log Pseudolikelihood | −153.897 | |||
| Pseudo R2 | 0.3962 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kien, N.D.; My, N.H.D.; Thu, D.T.A.; Tri, T.T.C.; Son, N.H.; Phong, T.K.; Tin, H.C.; Lan, N.H.; Thang, T.B.; The, B.D.; et al. Valuation of a Heatwave Early Warning System for Mitigating Risks Associated with Heat-Related Illness in Central Vietnam. Sustainability 2023, 15, 15342. https://doi.org/10.3390/su152115342
Kien ND, My NHD, Thu DTA, Tri TTC, Son NH, Phong TK, Tin HC, Lan NH, Thang TB, The BD, et al. Valuation of a Heatwave Early Warning System for Mitigating Risks Associated with Heat-Related Illness in Central Vietnam. Sustainability. 2023; 15(21):15342. https://doi.org/10.3390/su152115342
Chicago/Turabian StyleKien, Nguyen Duc, Nguyen H. D. My, Dang Thi Anh Thu, Ton That Canh Tri, Nghiem Hong Son, Thai Khanh Phong, Hoang Cong Tin, Nguyen Hoang Lan, Tran Binh Thang, Bui Dung The, and et al. 2023. "Valuation of a Heatwave Early Warning System for Mitigating Risks Associated with Heat-Related Illness in Central Vietnam" Sustainability 15, no. 21: 15342. https://doi.org/10.3390/su152115342
APA StyleKien, N. D., My, N. H. D., Thu, D. T. A., Tri, T. T. C., Son, N. H., Phong, T. K., Tin, H. C., Lan, N. H., Thang, T. B., The, B. D., & Dung, P. T. (2023). Valuation of a Heatwave Early Warning System for Mitigating Risks Associated with Heat-Related Illness in Central Vietnam. Sustainability, 15(21), 15342. https://doi.org/10.3390/su152115342