1. Introduction
In recent decades, researchers and psychologists all over the world have paid increased attention to the condition of pathological affective dependence (PAD) as a risk factor in intimate partner violence (IPV). IPV is defined by the UN [
1] as “behavior by an intimate partner or ex-partner that causes physical, sexual, or psychological harm, including physical aggression, sexual coercion, psychological abuse or controlling behaviors” (p. 24). An important addition to this definition is that IPV can occur between those aged 16 or over who have been intimate partners or family members, regardless of gender or sexuality [
2]. Intimate partner violence (IPV) is a global public-health problem: approximately 27% of ever-partnered women of age varying between 15–49 years experienced physical and/or sexual IPV [
3]. IPV heavily influences national economic development, costing an estimated 5% of the world’s gross domestic product (GDP) and nearly 15% of the GDP in Sub-Saharan Africa [
3]. Given this huge economic impact, the United Nations has called for better statistics on the nature, prevalence, causes, and consequences of gender-based violence as a basis for its elimination [
4]. This pressure led, in 2015, to the formulation of Sustainable Development Goal (SDG) 5.2, which urges governments to “eliminate all forms of violence against all women and girls in public and private…”. “Gender equality is not only a fundamental human right but a necessary foundation for a peaceful, prosperous, and sustainable world” (SDG 5). Widespread endorsement of SDG 5.2 compels national governments to measure and report rates of violence against women, including IPV (SDG 5.2.1). Moreover, reducing IPV is part of the sixteenth SDG, aimed at promoting peaceful and inclusive societies, reducing violence (SDG 16.1), and protecting children from abuse (SDG 16.1). IPV can cause or contribute to severe problems (i.e., substance misuse, complex post-traumatic stress disorder, depression, and suicidal ideation, etc.), significant transgenerational trauma transmission, huge economic costs, increased levels of physical morbidity and mortality [
5,
6]. IPV can take place in all types of intimate relationships and can vary in severity (e.g., severe versus less severe), incidence (e.g., regular occurrence versus rare), and goal (e.g., instrumental versus reactive; [
7], p. 588). Several studies and meta-analyses indicate that both men and women can behave as perpetrators and victims of IPV [
8,
9,
10,
11,
12]. This side effect may be an outcome of the normalization processes of violence as a way to face conflict [
13,
14]. IPV is to an increasing extent described in the newspapers. Inthe last years, the still unsolved phenomenon of IPV has been intensified by the COVID-19 pandemic and its control measures (i.e., lockdowns, mobility restrictions, and curfews; [
15]). Although several studies analyzed the risk factors for IPV, there is a lack of studies that investigate the specific pathological cognitive-behavioral determinants (goals, anti-goals, and dysfunctional self-other beliefs) which contribute to IPV. For example, Capaldi et al. [
16] included in their systematic review only risk factors such as contextual characteristics of partners (demographic, neighborhood, community, and school factors), developmental characteristics and behaviors of the partners (e.g., family, peer, psychological/behavioral, and cognitive factors), and relationship influences and interactional patterns. Implementing effective sustainable responses to IPV within healthcare and social systems is a challenge and there is no consensus about the best evidence-based model to apply to this huge social problem [
17]. Until recently, research exploring responses to IPV has tended to apply theoretical perspectives and methodologies which obscure the complexities, arising from interactionsof the antecedents of IPV and IPV itself. Given the range of evidence for the interaction of individual experiences of IPV (directly as a victim, and indirectly as a child) and the subsequent negative impact on the family’swell-being, this article has a primary focus on PAD as one of the main psychological antecedents of IPV [
18,
19,
20,
21]. We believe that understanding the mechanisms underpinning the condition of PAD is useful for guiding future social research and/or clinical practice that seeks to support individuals affected by IPV. The psychological experience of PAD negatively affects people’s ability to work, social relationships, and quality of life: individuals in this condition show a loss of interest in other activities outside the relationship with the partner (e.g., close friends, hobbies, and sports) and display academic or work impairment due to the incapability to focus on other areas of life [
20].
This is surprising that PAD is not yet considered in psychiatric nosology and there is a lack of a clinical model explaining this condition. Pugliese et al. [
19] presented the preliminary results of a pilot study aimed at introducing the main features of a prototypical patient suffering from PAD. Designing effective prevention requires knowing which psychological conditions will increase or decrease the risk of experiencing IPV—also known as risk and protective factors, respectively. Identifying the anatomy of a typical affective dependent (TAD) in terms of cognitive-behavioral determinants (goals, anti-goals, self-other beliefs) represents the first step to understanding the pathogenesis of IPV. This new conceptualization may contribute to preventing and intervening in the case of the IPV social phenomenon, which has its origin in adverse childhood experiences but is maintained by dysfunctional beliefs rooted in our society in terms of stereotypes and prejudices [
22,
23]. For example, cultures that support women’s economic dependence (vs independence), or specific explicit and implicit gender stereotypes play a pivotal role in increasing the occurrence of intimate partner violence against women and their affective dependence on their abusive partner. These aspects are linked to its origin, to the responses to women violence victims, and to the environment where it occurs [
23]. Men, just like women, are limited by stereotypes and misjudged if they act outside their traditional gender roles. A set of studies in 2015 [
24] showed that men who cried at work were perceived as less competent than women who cried. This negative bias can explain the reduced number of men who decide to report the IPV to the police and the tendency at justifying it as a possible incident [
22].
2. Definition of the Pathological Affective Dependence
According to Pugliese, Saliani, and Mancini [
18,
19,
21,
25] PAD is a relational condition. In this type of relationship, one or both partners engage in abusive, controlling, violent or manipulative behaviors. The relationship is a source of pain for at least one of the partners. Nevertheless, they feel unable to end the relationship or accept that one of the partners might choose to separate. In the event of separation/divorce or rejection, they feel extremely anxious and stressed and prevent the occurrence of this scenario with all their strength. They may also feel desperate and/or angry and try to cope with the consequent distress, ruminating all the time on possible solutions to be reconnected with the abusive partner, forcing themselves into submission, or clinging onto a new dysfunctional relationship. Individuals with PAD may experience negative moods and feelings when they are away from their partners. A way to face separation/rejection and the subsequent craving is forcing the closeness with the abusive partner [
26].
Finally, PAD is both a state and trait condition. A study’s result [
19], revealed that PAD is a latent condition that can be triggered by an abusive environment. The authors showed that: when people are hooked on an abusive relationship, they can show dysfunctional behaviors, beliefs, or goals typical of an individual with a personality disorder. These negative traits and malfunctioning aspects seem to disappear when they are completely out of the pathological environment and the separation from the abusive partner has been fully processed. Abusive partners can be considered as a trigger of PAD. Hence, to prevent the negative effect of the social phenomenon of IPV, government interventions should be targeted at both IPV victims and offenders [
27,
28,
29].
However, affective dependence in a couple is not always pathological. First of all, it reflects the prosocial need for attachment [
30] and can be a source of positive outcomes such as sexual excitement, warmth, support, and safety [
31]. Besides PAD, there is a kind of healthy affective dependence in intimate relationships. According to Curtis [
32] in a mature relationship, both partners reciprocally contribute to creating an environment that supports mutual growth. Each individual may feel committed to acquiring additional education, earning more money, and achieving a greater self-consciousness. Healthily depending on each other, with well-defined boundaries, may finally let both partners feel an increased sense of self-esteem and well-being [
33]. Hence, a healthy concept of affective dependency is based on mutuality and the ability to accept and overcome normal relational tensions and conflicts. In the psychological experience of PAD, physiological conflicts are characterized by a game of dominance and submission [
25], and the risk of violent acts is very high. The PAD partners find themselves trapped while they in vain try to fulfill their core relational needs such as safety, self-esteem, and love [
18,
19,
34]. This condition has negative consequences on the quality of life [
35,
36]. The three fundamental relational needs are put aside, and the focus is on the terminal goal of maintaining the relationship regardless of all the deleterious costs to their well-being, mental and physical health, and sense of safety. According to the goal-oriented theories [
37,
38,
39,
40], as shown by Pugliese et al. [
19] and consistent with the clinical observations [
21,
25], a key factor of these relationships is the presence of an internal conflict between the goal of maintaining the relationship (protecting the traumatic and pathological relationship) and the goal of interrupting the relationship (protecting themselves). In the PAD condition, there is a common belief that self-sacrifice and dysregulated altruism are a way to “cure” a problematic partner. Moreover, there is the idea that there will be a recognition of all the efforts done in the future. These two dysfunctional beliefs are a powerful anesthetic that freezes the relationship for a long time. This has huge negative consequences in terms of physical and/or psychological disorders, especially when the relationship degenerates into IPV; or worse, when the PAD partner decides to end the perceived suffering with extreme gestures, such as suicide or murder-suicide.
This paper has four aims: (1) defining the construct of PAD, (2) presenting a cognitive model of PAD, (3) introducing the cognitive determinants (self/other beliefs, goals, and anti-goals) of a prototypical person suffering from this condition, and (4) presenting the resulting specific TADs (typical affective dependent) profiles (Saver, Unworthy, Traumatic, and Mixed). Understanding the pathogenesis of the phenomenon, the IPV’s cycle and stages, and PAD’s profile (who are typical affective dependent people, what do they think about themselves and about others, which goals they are trying to reach or which terrific scenario they want to avoid at all costs) permit to go deeply at the origin of this experience. It may help to build an intervention that will be finally designed on a strong theoretical model, which is currently missing. It is a basis to build a measure of the pathological profiles: it permits the recognition of people who are at risk of losing their life, contributing to the assessment process of each health professional, including psychologists/psychotherapists, and capturing the phenomenon for social psychologists [
41]. This is decisively relevant to figure out educational policies (in schools, universities, anti-violence centers, social services, etc.), in preventing such a violent phenomenon by improving the well-being and mental health of people with PAD (and their relatives). This will help to stop the intergenerational trauma transmission and the huge social costs implied.
At this point, it could be scientifically and clinically relevant to understand what happens in the mind of the TAD, and what drives them to give up their well-being or life to maintain an unsatisfactory relationship. To answer those questions, we refer to the goal-oriented theory and the centrality of goals in explaining the development of PAD psychopathological symptoms.
3. A Cognitive Model of Pathological Affective Dependence
The inability to end the pathological relationship—regardless of the resulting impairment of work, relational and social life—is what defines the peculiarity of PAD. People with PAD may both be or not be aware of the paradoxical condition they are experiencing. Accordingly, this contradictory scenario is structured in three possible internal conflicts between the goal of maintaining the pathological relationship and the goal of ending it. TADs swing between these two goals apparently without any solution. At this point, the war is in their head, not only in their house. The conflict may be absent, alternate, or akrasic [
18,
25,
41].
In the first scenario, when the conflict is absent (or Absent), the TAD is not aware of being in a pathological relationship or of the abusive partner’s behaviors. The conflict appears only in others’ eyes. TADs are blind and living their special honeymoon. At the same time, people such as relatives, friends, or the psychotherapist are already aware of the relational malfunction. TADs enter into the conflict between the will of maintaining the relationship and the will to end it as soon as the disadvantages of the pathological relationship appear. At that point, TADs swing among the two poles of the conflict. However, in this first conflict, PAD’s condition is ego-syntonic, and the perceived advantages of staying in the relationship are greater than the costs. TAD chooses to not separate. In the beginning, all pathological relationships are characterized by absent conflict (in the mind of TAD).
The second type of conflict is the alternate current conflict (or Alternate). TADs begin to be aware of relational malfunctions. Specifically, there is a movement between two opposite mental states and goals. Mental states are not yet integrated, and goals are diametrically opposed: for example, the possibility of separating is positively evaluated to improve personal well-being, autonomy, and sense of self-efficacy; and it is negatively evaluated when associated with the desire of creating a family with the partner. Due to the separation of these two mental states, PAD is partially ego-dystonic and ego-syntonic. The TAD might move from one mental state to another one without being aware of the swing: they may decide to end the relationship one week and have a baby the week after. These incoherent patterns are confusing for people around them. At this point, people suffering from PAD can feel misunderstood and could decide to isolate or move on to the following conflict.
The third type of conflict is the akrasic conflict (or Akrasic). This condition occurs immediately after either the absent or the alternate conflict. PAD is fully ego-dystonic, people with PAD are finally aware that they are in a pathological relationship and at the same time unable to end it. TADs ask for help from a friend, family, or professionals. There is an oscillation among two different goals within the same mental state: for example, TADs are aware of swinging between the will of separating and the will of maintaining the relationship at all costs, but they could ignore the reason for this inability to make a final decision. Giacomantonio and Mancini [
42] affirm that the modality of resolution of this conflict can be explained in the light of the Construal Level Theory [
43,
44], to the concept of psychological distance (temporal, spatial, social, and hypothetical) and the phenomenon of temporal discounting [
45]. Concerning the mind of TAD, it happens that they prefer a minor but immediate goal (such as the reduction of separation anxiety, through the reunification with the abusive partner) to a healthier goal, but distant in time (such as the separation and consequent increased mental health and safety perception).
These three conflicts (Absent, Alternate, and Akrasic) play a pivotal role in the four stages of the cognitive model of PAD. Indeed, PAD’s relationships follow a cyclical pattern [
18]. Many discussions of child abuse and domestic, school, or gang violence use the idea of a cycle of violence [
46]. According to Lenore Walker’s theory [
47], there are three phases in all dynamics of an abusive relationship. Walker realized that battered women aren’t attacked at the same time or in the same way. However, the phases remain consistent. Although some phases might last longer or manifest themselves in different ways, they were always evident. According to the Author, there are three different and cyclic phases: tension building phase, acute violence, and reconciliation/honeymoon phase.
In the first phase (tension building phase), there is a gradual intensification of tension. Walker [
46] characterized this by a frequency of continuous conflicts, and psychologically violent acts which involve jealousy, shouting, or small fights. The duration of this phase doesn’t necessarily have a specific time. It can perdure for weeks, months, or years. The second phase (acute violence) is characterized by a lack of control, which usually degenerates into physical, psychological, and/or sexual aggression with increasing severity and frequency. The victim has a traumatic experience and can be isolated as a consequence. He/she may feel anxious and powerless. Due to traumatic reactions, asking for help does not occur often. In the third phase (reconciliation/honeymoon phase), the abusive partner usually asks for forgiveness and promises the victim that he/she will never do it again. Manipulative strategies can be employed to make sure to not end the relationship. In this phase, there is any tension or conflict, and the couple can live on a sort of honeymoon. The victim wants to believe that the abusive partner has changed. The disappeared tension and love bombing behaviors are proof of that. This reconciliation phase ends as soon as small fights begin again. Walker’s model is focused on the timing of the growing violence in the relationship, but it is not considering TAD’s psychological condition. Although it is useful to understand the intimate partner violence trend, this cycle of violence does not deepen the internal mental processes of each phase. The cognitive model of PAD tries to fill this gap focusing on both the cyclic nature of PAD and the TAD’s state of mind.
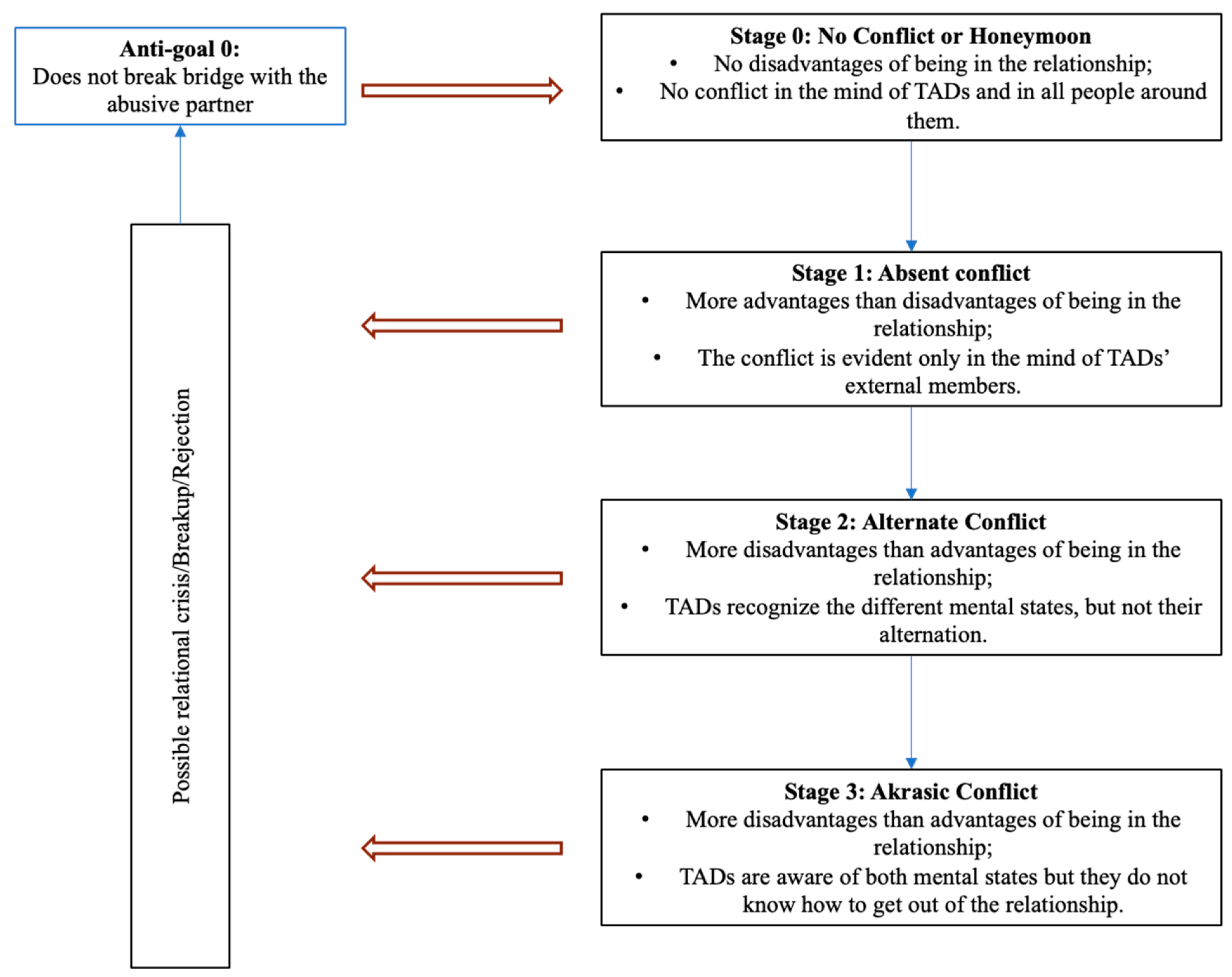
Specifically, in the cognitive model of PAD (see
Figure 1), there is a four-stage cyclic pattern. Except for Stage 0, the other stages are characterized by the three main internal conflicts. All those conflicts are between the goal of maintaining the dysfunctional relationship at all costs and the goal of separating from the abusive partner. The activation of those conflicts is the pathological reason why TADs are frozen in a violent relationship and do not escape from it, even when their life is in danger.
Stage 0. This stage is marked by any type of conflict. Yet, no relational costs have been paid by the TAD. TADs show their best part as well as the abusive partner: despite some signs of an emotionally labile and fleeting partner’s personality—signs necessary to arouse interest in the TAD—the abusive partner is in turn in love, present, generous, eager to share things. This stage is called romantic illusion/honeymoon or Stage 0. In this stage, TADs think that Omnia Vincit Amor, and love magically heals and saves everything. The abusive partner seems perfect, the prince/princess charming, even though he/she has ended up being in a relationship with a frog. Stage 0—also called the honeymoon stage—lasts one week, a month, or a year. It will become the TAD aspirational state of mind: PADs will put all their effort to join it again and again, also when the relationship will degenerate in the later negative following stages.
Stage 1. This stage corresponds to the absent conflict. It is the first negative stage after the love bombing phase. In this stage, there are more advantages than disadvantages being in a relationship. Relational costs (i.e., excessive jealousy, a feeling of living on a roller coaster, devaluation, lack of safety) begin to be evident only in the mind of TAD’s external members such as a friend, family member, or psychotherapist. The conflict is absent in the TAD’s mind. The TADs still think they are fine and happy, that those minor problems can be fixed, and the partner will soon change all the bad behaviors. They got or are trying to get what they want from the relationship, and the self-preservation goals are not yet in place. In this stage, TADs may ask for professional help or have psychological sessions for symptoms not related to the dysfunctional relationship itself (i.e., panic attacks, depression, insomnia, etc.). They could ask to improve their assertiveness even if they do not recognize to be in a perilous relationship with their life at risk [
21]. The psychologist/psychotherapist may feel confused about the relationship’s health. They do not recognize they are in PAD (and the risks associated) and decide to work on other related therapy goals (i.e., depression, insomnia, or burnout) leaving the PAD side work undone. Therefore, it is urgent for all psychologists/psychotherapists to know deeply how a PAD relationship works and to prevent irreversible scenarios such as suicide, and murder-suicide [
21]. Differently from the next stages, in Stage 1, TADs will never end the relationship by themselves. This stage ends with the following scenarios: TADs may have an epiphany and realize they weren’t in a healthy relationship (best case scenario); they can quickly seek a very similar relationship in order not to feel the pain of rejection; the abusive partner may ask to get back together and try again; the abused partner does not end the relationship and stalker them. In all those three last scenarios, TADs will switch in Stage 2.
Stage 2. It corresponds to the alternate conflict. This second internal conflict occurs when both the disadvantages are more than the advantages and PADs begin to be more aware of the related costs. Although TADs are always more conscious about the disadvantages of being in a couple, the commitment in the relationship is still very high. In this stage (as in the following stages), the conflict is between the goal of maintaining the relationship and the goal of ending it. The specialty of this stage is that one of the two goals is alternately salient, and it makes the other one disappear. TADs will recognize the moments of relational malaise and well-being, but they do not recognize their alternation. They oscillate between moments of great well-being and great malaise, but they do not integrate the two different states of mind. At this stage, there are different scenarios: the costs for TADs may increase progressively, a huge new cost appears (for example, a humiliation in public), the small advantages temporarily disappear, or a TAD’s friend (family member or psychotherapist) starts to point them out, self-protection purposes are momentarily activated, relational ego-dystonia appears and therefore the first forms of protest/rebellion to the partner behaviors appear. There is an alternation between states of tension towards the goal of maintaining the relationship and moments of anger/protest without a conscious and lasting integration of the implications of the two states of mind. When TADs are in a negative state of mind (the relationship costs increased), they can decide to end the relationship. In this stage, TADs can also make first contact with a psychologist/psychiatrist and ask for help. According to the specific functioning of this stage and the type of conflict, there is a lack of integration of the two goals. Due to this condition, TADs can suddenly change their idea about ending the relationship when the other goal (saving the relationship at all costs) becomes salient. Most of the time, people around the TAD are confused about their continuous contradictory choices and they may decide to distance themselves from them. This can contribute to isolating TADs but at the same time can be a stimulus to increase their self-reflection and switch to Stage 3.
Stage 3. In Stage 3, TADs enter into an akrasic conflict. Compared to the alternate conflict, in the akrasia condition, TADs integrate the two contradictory goals (save or end the relationship). Therefore, they are fully aware that staying in that type of relationship hurts them, but that they would save the relationship in any case. Although, they would and could end the relationship, either they do not want to, or they think they are not able to separate from the abusive partner. The amount of TAD’s distress is high, the relational costs can negatively affect their social life, work, and friendships. In the worst-case scenario, TAD’s life is in danger. The distress arises not only because of the maladaptive relationship itself but also because of the simultaneous presence of two opposite goals: save and end the relationship. TADs feel trapped in that relationship. Moreover, they negatively judge themselves, because of their inability to end the relationship despite the obvious costs. Most of the time, those secondary thoughts arise from their first disastrous attempt to end the relationship during stage 2. At best, in those stages (2 and 3 stages), TADs consult someone to address the painful situation (a friend or a psychologist/psychotherapist/psychiatrist). At worst, TADs feel no way out, or deserving of mistreatment. In the latter case, they may decide to get back into the relationship, starting a new PAD cycle. Or they may start a new PAD relationship with another abusive partner. This cyclical pattern can last indefinitely and in the worst-case scenario, physical and/or psychological abuses lead to death. For all these reasons, ending a relationship with an abusive partner is particularly difficult. The consequences of PAD relationships are devastating not only for the direct victims but for all the people around them, such as family members, friends, and children [
48]. These relations also have a negative impact not only on TADs’ mental health but also on the physical health of all people involved [
48,
49,
50,
51,
52,
53]. Below, in
Figure 1, we present a cognitive model of PAD. Those four stages allow us to have a definitive vision of the cyclic state of mind of a person with PAD and therefore it may guarantee a targeted intervention.
4. The Prototypical Profile of a Pathological Affective Dependent
The last two aims of this article are to describe the prototypical characteristics of a pathological affective dependent (in terms of goals, anti-goals, and dysfunctional self-other beliefs) based on goal-oriented theories, and the resulting specific TADs profiles (Saver, Unworthy, Traumatic, and Mixed). Deeply knowing the cognitive components of TAD can help to intervene early in case of IPV. Moreover, it can be a useful instrument to understand the mind of those who are facing this horrible condition. Consequently, Pugliese et al. [
19] tried to describe the internal profile of a typical affective dependent (TAD). This profile is based on clinical observations and the results of a first pilot study [
19]. This profile has been built referring to the theory of goal-oriented behaviors [
37,
38,
39,
40]. According to this theory, goals have a pivotal role in explaining psychopathology. Moreover, the preliminary results study [
19] showed that TADs’ goals would help to understand why they keep maintaining pathological relations despite the malaise experienced, or they often run after the wrong partner. Specifically, TAD’s instrumental goal (Goal 0) is to be loved by a problematic/abusive or not available partner. The worst-case scenario is ending the PAD relationship (Anti-goal 0). Three terminal goals are necessary to pursue Goal 0. TADs ’terminal goal is to be important/seen or valuable for their partner (Deontological goal or Goal 1), save/heal their partner (Altruistic goal or Goal 2), and safety and attachment (Safety goal or Goal 3). These goals are not specific to a pathological relationship. They are relational goals of all healthy and happy relationships. In PAD these goals are not reached because of an abusive/problematic and/or not available partner. In this specific relationship, they are expressed as anti-goals (for example, “I do not want to lose my dignity ending the relationship”, or “I can’t leave my partner alone because I can’t bear his/her suffering”). Those partners will never pay back TADs for all their efforts. But TADs develop towards them a huge obsession. On the contrary, caring partners oppress TADs: they prefer distancing partners or not available ones. Partners who love them or who take care of their needs are often described as “boring” or not interesting at all. According to Pugliese et al. [
19], the pathological anti-goals’ activation by these specific partners permits distinguishing PAD from Dependent Personality Disorder [
54,
55]. If the main TADs goal were to obtain excessive care as in dependent personality disorder, they would not avoid partners who carefully fill their needs, as they usually do.
Why does the TAD fail to get out of the relationship, despite being aware of the negative consequences? Why does he/she get stuck in the conflict? As stressed by the pilot study [
19], during the clinical sessions, all TADs confirm that they are more terrified of a break-up with the problematic partner than attracted to a stable relationship. Moreover, they were more attracted to problematic partners than safe and caring ones. They explained this inconsistent pattern as the result of their terrifying fear of making his/her partner suffer, deserving nothing better, and feeling lonely/lost when they are alone.
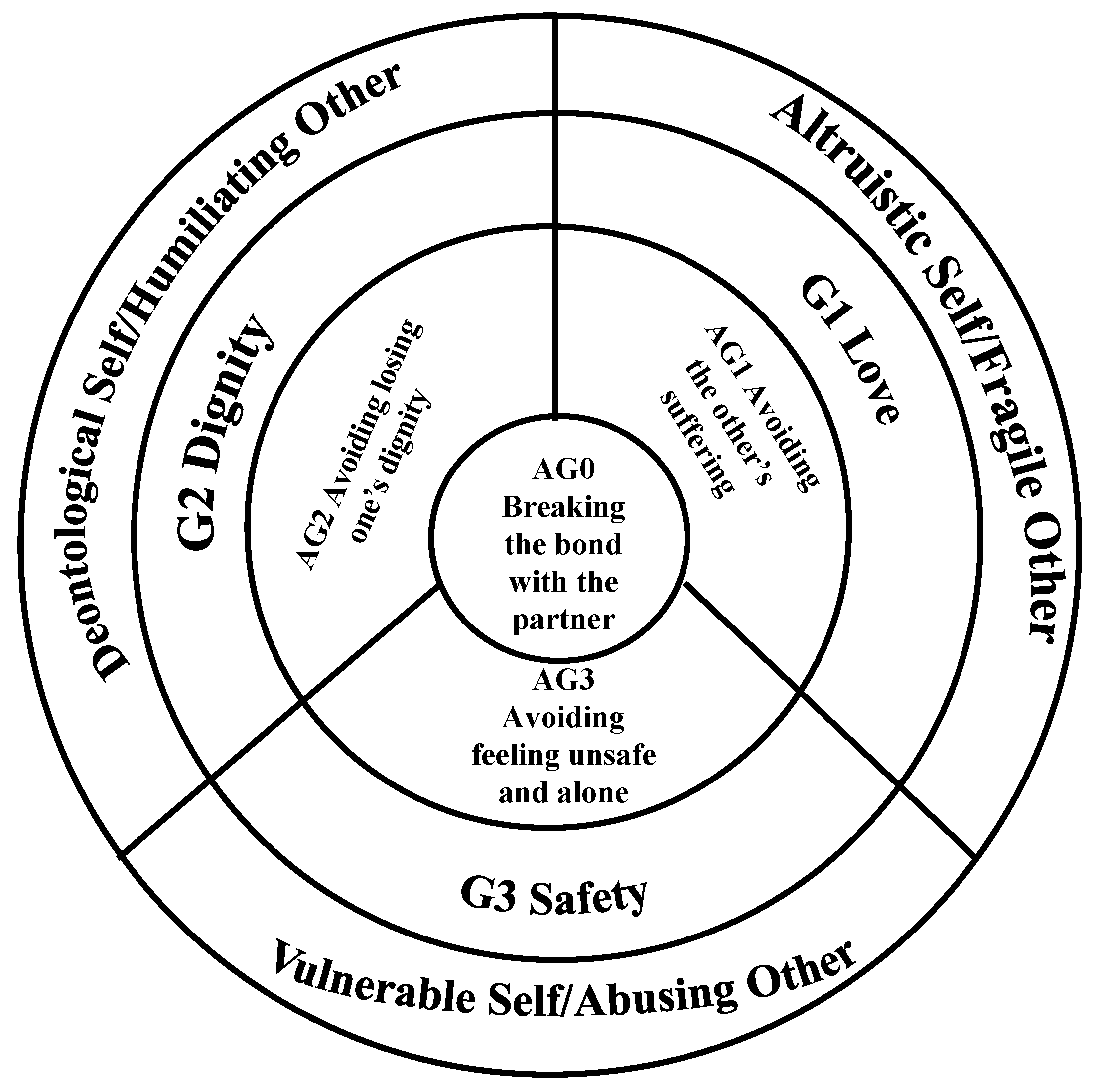
Accordingly, in this first theoretical proposal, we assume that TAD cannot interrupt the dysfunctional relationship for these three specific reasons. As represented in
Figure 2, the worst-case scenario for the TAD is ending the relationship (Anti-goal 0 or AG0). The TAD will therefore uphold the AG0 as much as possible. Their main goal is maintaining the dysfunctional relationship at all costs or to be loved in the way they dream of forever (Goal 0 or G0). This goal is supported by three main worries named terminal anti-goals. Each anti-goal (the TAD’s worst-case scenario) refers to a specific relational goal (the goal they would reach through the relationship and/or partner) and self/other beliefs (self/partner pictures built in their early childhood experiences). Anti-goal 1 (AG1): avoiding the other’s suffering. The goal is to change/save someone emotionally fragile, violent, and unattainable and feel finally loved (Goal 1: Love); Anti-goal 2 (AG2): avoiding the loss of own dignity. The goal is to feel worthy/seen or to retrieve one’s value, lost during a dysfunctional relationship with a denigrating, humiliating, and insulting partner (Goal 2: Dignity); Anti-goal 3 (AG3): avoiding feeling unsafe and alone. The goal is safety and attachment. They need to feel safe and protected or retrieve their sense of safety lost during the relationship with an abusive, physically, and sexually abusive partner (Goal 3: Safety).
These anti-goals have been developed as a result of the long-term frustration of basic needs (attachment and moral) and/or parental behavioral models learned in early relationships. These conditions have developed different and separate parts (or images) of the self (and a relative image of the partner), each with a specific purpose [
34]. Getting stuck in a relationship despite the malaise experienced originates in the unconscious desire to redeem the traumas experienced during childhood: emotional deprivation, abuse, depreciation, lack of care, etc. [
56]. The TAD adults may have been children who they could not choose to separate from their parents even if they were mistreated. They could escape from that condition because of their need to survive. They may have been a child identified with the parent with the mission of love and sacrifice towards the other problematic partner (because of long-term psychological or physical disease, or a child devoted to loving and saving the problematic parent, despised, and neglected by the other partner). In other words, the role played by the other parent seems decisive in the dynamics of the psychological development of the future TAD.
On the contrary, the need of being important to another one, to care for him/her regularly, and to feel safe and secure with the partner can be considered normal and healthy needs of a healthy relationship [
57]. Dysregulation of these needs in a positive or negative direction can be considered a sign of PAD.
As can be seen in
Figure 1 and in line with the clinical observations and study results, the main goal (G0) and three terminal goals (G1, G2, and G3) refer to the following self/other beliefs:
Romantic self-/idealized other (Goal 0)
Altruistic self/problematic-fragile other (Goal 1)
Deontological self/humiliating other (Goal 2)
Vulnerable-Traumatic- Emotionally unavailable self/abusing other (Goal 3)
In line with the cognitive model of PAD, already in part presented by Pugliese et al. [
18,
19,
21,
25] we can hypothesize that there are four main factors, which can describe the psychological condition of TAD. These specific TAD factors are labeled: Altruistic, Deontological, Vulnerable, and Conflict.
The first three factors refer to the above-mentioned four main anti-goals, goals and self, and other beliefs. They can be all present simultaneously with the same weights or with different weights. Moreover, TADs may be aware of them according to the stage of the relationship and the type of conflict taking place. For example, in alternate conflict conditions, TAD cannot be aware of having a relationship with a psychologically abusive partner while he/she could be aware of his/her behaviors the following week. This is because mental states are not integrated into TAD’s mind. Accordingly, the conflict factor could be considered transversal to all the first three conditions. Hence, it will be present in all three conditions, except for the altruistic self-problematic/fragile other one. In this condition, when TAD is helping/saving the problematic partner, the PAD is ego-syntonic, the goal is reached, and there are not any internal conflicts in TAD’s mind (alternate and akrasic conflict). The conflict starts when the partners start to reject the TAD’s help, mistreating or abusing them verbally, psychologically, or physically.
The first three factors can be described using the specific TAD internal conflict. Specifically:
Anti-Goal 1: to avoid the other’s suffering
Goal 1 or Love: to change/save someone emotionally fragile, violent, and not emotionally available
Self: altruistic self
Other: problematic/fragile partner
- 2.
Deontological Factor (2)
Anti-Goal 2: to avoid losing one’s dignity
Goal 2 or Dignity: to feel worthy or to retrieve one’s value lost during the dysfunctional relationship with a denigrating, humiliating, and insulting partner
Self: deontological self
Other: humiliating partner
- 3.
Vulnerable Factor (3)
Anti-Goal 3: to avoid feeling unsafe and alone
Goal 3 or Safety: to feel safe and cared for, or retrieve one’s sense of safety lost during the relationship with an abusive, physically and sexually abusive partner.
Self: vulnerable/traumatic self
Other: emotionally unavailable/abusive partner
- 4.
Conflicts Factor (4)
In conclusion, we hypothesize that there are more types of TADs. Of course, all TADs share the common fear of ending the relationship, and the three conflicts (which are the cognitive factors in maintaining the suffering). Moreover, TADs could not end the relationship because of three other specific fears: some TADs do not want to end the relationship because they could feel unworthy and disgusting, other TADs because they could feel alone and helpless, others because they could feel bad when they do not (excessively) take care of and “save” the poor, fragile partner, still others for all the three reasons or a couple of them. In summary, we could hypothesize four prototypical profiles, consistently with the hyper-invested anti-goal: Saver (Anti-goal 1), Unworthy (Anti-goal 2), Traumatic (Anti-goal 3), and Mixed (all anti-goals or two of them). The latter are the most problematic and chaotic. Finally, we would like to point out that, in all PADs, the responsibility for the final decision about the relationship destiny must play a crucial role (probably due to some form of anticipated self-criticism). In fact, the problem of the PAD is not the abandonment or rejection itself (even if they fear them). Rather they suffer for not ending the relationship despite having understood that it would be the healthiest and best choice for them or not doing enough to prevent abandonment.
5. Conclusions
PAD and IPV are complex and multidimensional problems whose consequences harm victims, their families, and society as a whole [
58].
Empirical research confirms that partners and children exposed to IPV have serious negative consequences on both physical and mental health [
48,
49,
50,
51,
52,
53]. These results highlight the need to identify risk factors for the intergenerational transmission of IPV [
56]. Both IPV and intergenerational transmission of relational trauma can be considered a limitation on the achievement of the fifth and the sixteenth SDGs, which are respectively reducing the violence against women, promoting a peaceful and inclusive society, eliminating violence, and protecting children from abuse.
Current evidence indicates that several factors increase the vulnerability of being involved in IPV as either victims or perpetrators. For example, psychosocial factors such as exposure to multiple adversities, where children are exposed to violence, maltreatment, low self-esteem, and socioeconomic disadvantage [
10,
12,
16,
59] have all been found to be linked to IPV. It is thus beneficial to consider such psychosocial factors when investigating IPV. Although there is an urgent need for targeted interventions that are based on a clear conceptualization of IPV antecedents, international literature misses a psychological risk factor as PAD clinical functioning. To understand, therefore, how to intervene with people experiencing similar suffering, it is essential to understand TAD’s mind, and why there is a freeze in such unsatisfactory and dangerous relationships. Although PAD has attracted considerable attention across disciplines, many health professionals ignore how to intervene in the case of PAD and IPV due to a lack of a model for its maladaptive functioning.
The general aim of this paper has been to fill this gap, helping professionals to recognize the prototypical profile of people with PAD, meant as an IPV risk factor, and intervene before the cycle of violence is activated [
21,
46]. Hence, the objectives of the paper were mainly four: define the PAD construct, present a cognitive model of PAD based on goal-oriented theories [
37,
38,
39,
40], identify the prototypal characteristics of TADs (such as goals, anti-goals, and dysfunctional self-other beliefs), and specific TAD’s profiles (Saver, Unworthy, Traumatic and Mixed). We believe that PAD is a fundamental psychological antecedent and a contributing cause of IPV. PAD is meant as both a trait and a state condition [
19]. This means that PAD is a latent condition activated by a dysfunctional environment such as a pathological partner or/and a culture that justifies gender-based violence. These results stress the importance of a socio-psychological intervention for both victims and perpetrators. Concerning the victims of IPV, it seems fundamental to understand that the main characteristic of the PAD is the development of an internal conflict between maintaining the dysfunctional relationship and escaping from it. TADs swing in those two opposite goals. Most TADs are aware of being in a violent relationship. But this awareness is not a sufficient condition for its resolution. If TADs rationally understand the dysfunctionality of their relationship, they fail to unlock it emotionally. The internal conflict looks like an unsolvable quiz and without adequate interventions, it could last for a long time and lead to extreme gestures such as suicide or murder-suicide or persecutory acts such as stalking. In fact, in terms of health intervention, the psychologist/psychotherapist’s ability to recognize that they are facing a cycle of PAD allows them to prevent therapeutic errors in the case formalization, and the following therapeutic work [
21].
Moreover, if until now PAD has been treated as a simple declination of dependent personality disorder or one of the forms of addiction (alcohol, drugs, sex, and gambling), it follows that the treatments used fail to consider the multiplicity of PAD. The use of the four factors (Altruistic, Deontological, Vulnerable, and Conflict) and the four TAD profiles (Saver, Unworthy, Traumatic, and Mixed) in understanding TAD mental functioning and types would likely lead to targeted intervention in the field of social and clinical psychology. This is fundamental to prevent and intervene in time and break the cycle of IPV. It follows the need and urgency of a therapy protocol that can intervene on PAD as an antecedent of IPV. This clinical intervention must consider the dynamics of internal conflict based on the various stages of the relationship. This has also several implications in terms of social interventions, such as community education programs in schools and Universities, in social centers of aggregation, with a focus on PAD prevention (i.e., how to quickly recognize an abusive partner, characteristics of healthy intimate relationships, human rights in intimate relationships, etc.). This work aims to become the starting point of a broader project aimed at filling this gap by creating a cognitive-behavioral protocol and sustainable social interventions capable of reducing the negative health and societal outcomes of the PAD condition. A sustainable healthcare response to IPV relies on the interaction between the complex world in which PADs live and the complex healthcare system that face their situation [
17]. An effective and sustainable healthcare response to IPV and its antecedents emerges when the interaction between the two complex systems (the PAD and the healthcare setting) favors the mutual adaptation in ways that generate positive outcomes for both victims and perpetrators (e.g., reduced violence) and the health professionals (e.g., increased capability in responding). Sustainable interventions occur when there are mutual understanding, adaptation, and solutions between the involved characters and an increased likelihood of positive outcomes. Since the coronavirus outbreak exacerbated existing inequalities for women and girls across every sphere—from health and the economy to security and social protection, it is urgent to propose a complex model connecting antecedents and consequences of IPV. The pandemic has also led to a worrying increase in violence against women and girls. With lockdown measures many women were trapped at home with their abusers, struggling to access healthcare services that were dramatically reduced. Emerging data showed that, since the outbreak of the pandemic, violence against women and girls, and particularly domestic violence—has intensified [
4]. Hence, the time to answer can’t be postponed anymore.

 ,
, 

{kind=link}
{kind=link}

