
Greener Neighbourhoods Show Resilience to the Spread but Not Severity of COVID-19 Infection in South Africa



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Data Analysis
Rescaling was conducted in Microsoft Excel 2016.
3. Results
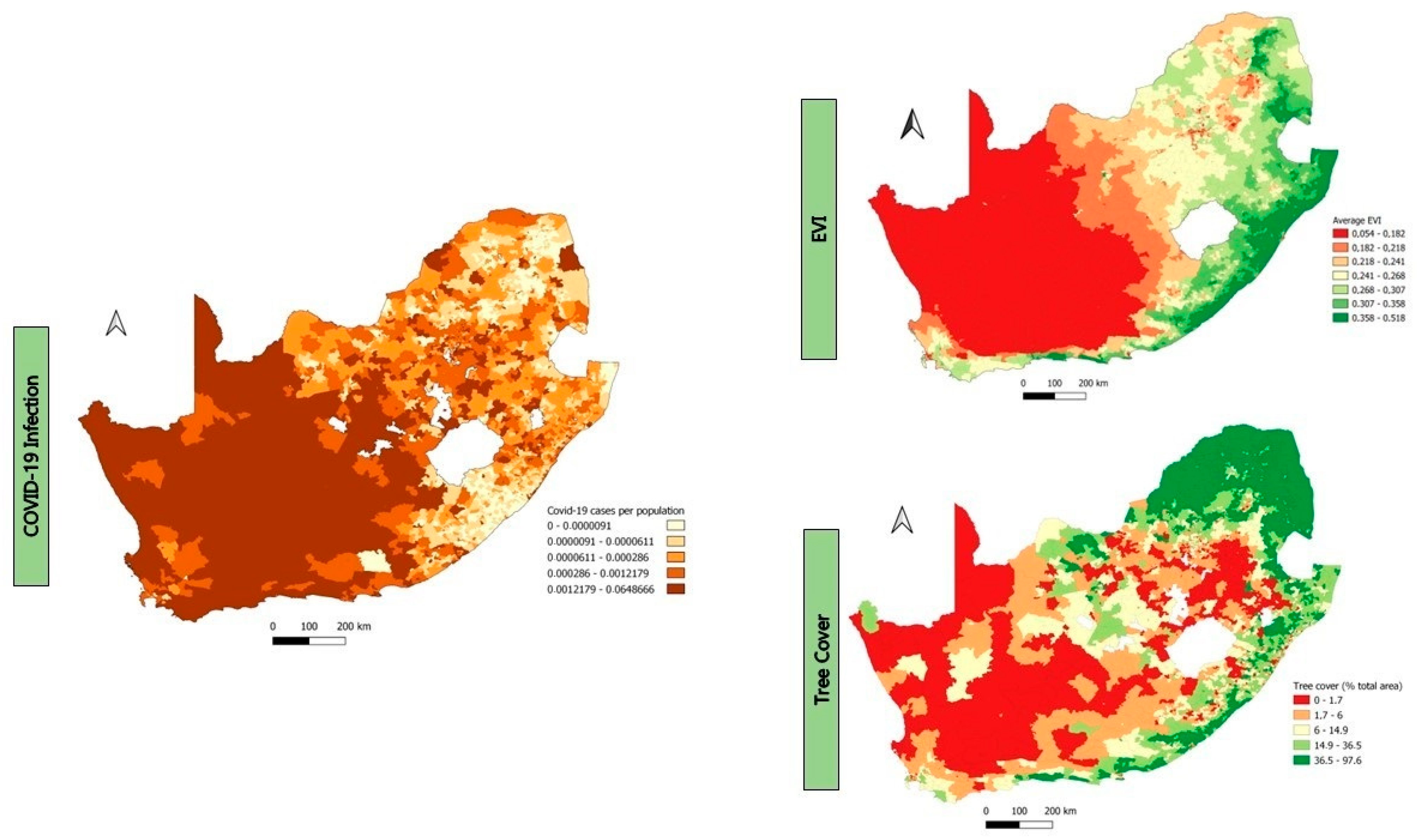
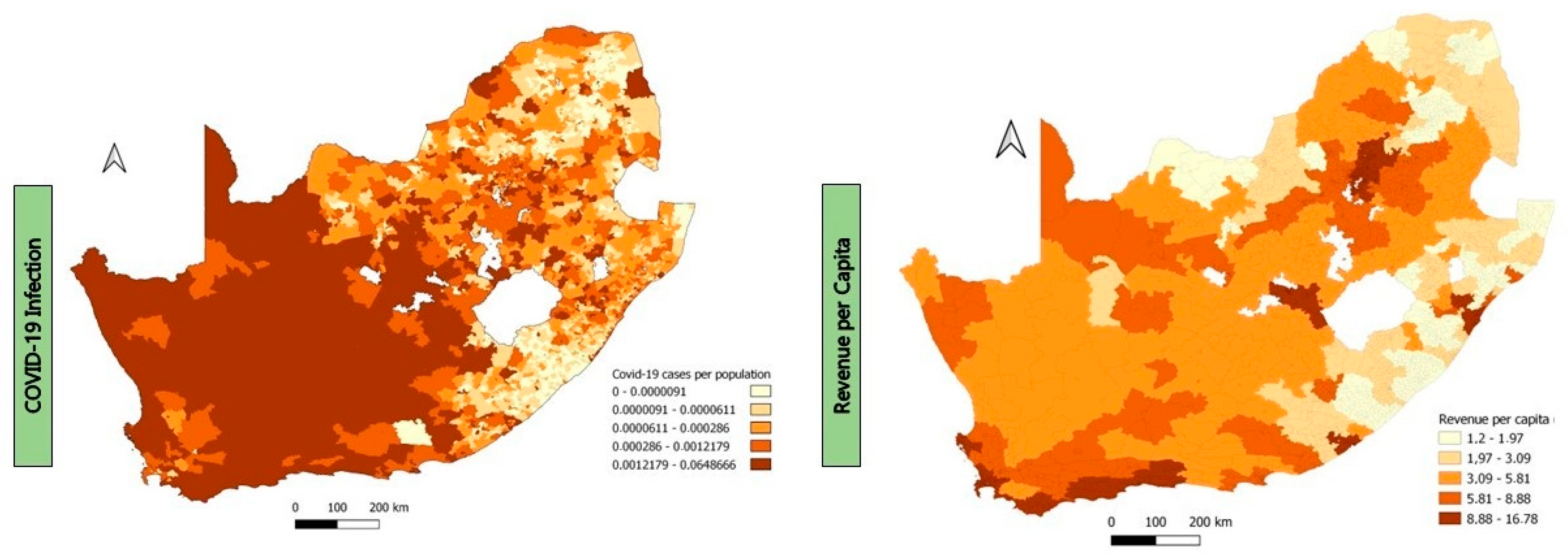
3.1. The Relationship between Greenness and COVID-19 Infection
3.2. The Relationship between Greenness and COVID-19 Severity
4. Discussion
4.1. Greenness versus COVID-19 Infection Rate at Local Municipality Level
4.2. Greenness versus COVID-19 Infection Rate at Ward Level
4.3. Greenness versus COVID-19 Severity
4.4. Revenue Per Capita, Age, Population Density, and Income Levels versus COVID-19 Infection and Severity of COVID-19
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B
References
- WHO (World Health Organisation). Coronavirus Disease 2019 (COVID-19), Situation Report—65. 2020. Available online: https://www.who.int/publications/m/item/situation-report---65 (accessed on 20 February 2023).
- WHO (World Health Organisation). WHO Coronavirus (COVID-19) Dashboard. 2022. Available online: https://covid19.who.int/ (accessed on 27 July 2023).
- DoH (Department of Health). Update on COVID-19 (Saturday 04 June 2022). 2022. Available online: https://sacoronavirus.co.za/2022/06/04/update-on-covid-19-saturday-04-june-2022/ (accessed on 20 February 2023).
- Bonaccorsi, G.; Pierri, F.; Cinelli, M.; Flori, A.; Galeazzi, A.; Porcelli, F.; Schmidt, A.L.; Valensise, C.M.; Scala, A.; Quattrociocchi, W.; et al. Economic and social consequences of human mobility restrictions under COVID-19. Proc. Natl. Acad. Sci. USA 2020, 117, 15530–15535. [Google Scholar] [CrossRef]
- Huang, B.; Huang, Z.; Chen, C.; Lin, J.; Tam, T.; Hong, Y.; Pei, S. Social vulnerability amplifies the disparate impact of mobility on COVID-19 transmissibility across the United States. Humanit. Soc. Sci. Commun. 2022, 9, 415. [Google Scholar] [CrossRef]
- Jin, J.; Agarwala, N.; Kundu, P.; Harvey, B.; Zhang, Y.; Wallace, E.; Chatterjee, N. Individual and community-level risk for COVID-19 mortality in the United States. Nat. Med. 2020, 27, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Prem, K.; Liu, Y.; Russell, T.W.; Kucharski, A.J.; Eggo, R.M.; Davies, N.; Jit, M.; Klepac, P.; Flasche, S.; Clifford, S.; et al. The Effect of Control Strategies to Reduce Social Mixing on Outcomes of the COVID-19 Epidemic in Wuhan, China: A Modelling Study. Lancet Public Health 2020, 5, e261–e270. [Google Scholar] [CrossRef]
- Rojas-Rueda, D.; Morales-Zamora, E. Built Environment, Transport, and COVID-19: A Review. Curr. Environ. Health Rep. 2021, 8, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Le, K.; Nguyen, M. The psychological consequences of COVID-19 lockdowns. Int. Rev. Appl. Econ. 2020, 35, 147–163. [Google Scholar] [CrossRef]
- Škare, M.; Soriano, D.R.; Porada-Rochoń, M. Impact of COVID-19 on the travel and tourism industry. Technol. Forecast. Soc. Chang. 2020, 163, 120469. [Google Scholar] [CrossRef] [PubMed]
- Labib, S.; Browning, M.H.; Rigolon, A.; Helbich, M.; James, P. Nature’s contributions in coping with a pandemic in the 21st century: A narrative review of evidence during COVID-19. Sci. Total Environ. 2022, 833, 155095. [Google Scholar] [CrossRef] [PubMed]
- Müller, F.; Röhr, S.; Reininghaus, U.; Riedel-Heller, S.G. Social Isolation and Loneliness during COVID-19 Lockdown: Associations with Depressive Symptoms in the German Old-Age Population. Int. J. Environ. Res. Public Health 2021, 18, 3615. [Google Scholar] [CrossRef] [PubMed]
- Imam, Z.; Odish, F.; Gill, I.; O’Connor, D.; Armstrong, J.; Vanood, A.; Ibironke, O.; Hanna, A.; Ranski, A.; Halalau, A. Older age and comorbidity are independent mortality predictors in a large cohort of 1305 COVID-19 patients in Michigan, United States. J. Intern. Med. 2020, 288, 469–476. [Google Scholar] [CrossRef]
- Hussey, H.; Zinyakatira, N.; Morden, E.; Ismail, M.; Paleker, M.; Bam, J.-L.; London, L.; Boulle, A.; Davies, M.-A. Higher COVID-19 mortality in low-income communities in the City of Cape Town—A descriptive ecological study. Gates Open Res. 2021, 5, 90. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Chen, L.; Liu, X.; Yang, Y.; Sullivan, W.C.; Xu, W.; Webster, C.; Jiang, B. Green spaces mitigate racial disparity of health: A higher ratio of green spaces indicates a lower racial disparity in SARS-CoV-2 infection rates in the USA. Environ. Int. 2021, 152, 106465. [Google Scholar] [CrossRef]
- Spotswood, E.N.; Benjamin, M.; Stoneburner, L.; Wheeler, M.M.; Beller, E.E.; Balk, D.; McPhearson, T.; Kuo, M.; McDonald, R.I. Nature inequity and higher COVID-19 case rates in less-green neighbourhoods in the United States. Nat. Sustain. 2021, 4, 1092–1098. [Google Scholar] [CrossRef]
- Lin, J.; Huang, B.; Kwan, M.-P.; Chen, M.; Wang, Q. COVID-19 infection rate but not severity is associated with availability of greenness in the United States. Landsc. Urban Plan. 2023, 233, 104704. [Google Scholar] [CrossRef]
- Phogole, B.; Yessoufou, K. A global meta-analysis of effects of green infrastructure on COVID-19 infection and mortality rates. medRxiv 2023. [Google Scholar] [CrossRef]
- Bratman, G.N.; Anderson, C.B.; Berman, M.G.; Cochran, B.; de Vries, S.; Flanders, J.; Folke, C.; Frumkin, H.; Gross, J.J.; Hartig, T.; et al. Nature and mental health: An ecosystem service perspective. Sci. Adv. 2019, 5, eaax0903. [Google Scholar] [CrossRef] [PubMed]
- Frumkin, H.; Gregory, N.; Bratman, G.N.; Breslow, S.J.; Cochran, B.; Kahn, P.H., Jr.; Lawler, J.J.; Levin, P.S.; Tandon, P.S.; Varanasi, U.; et al. Nature Contact and Human Health: A Research Agenda. Environ. Health Perspect. 2017, 125, 075001. [Google Scholar] [CrossRef]
- Li, Q. Effect of forest bathing trips on human immune function. Environ. Health Prev. Med. 2010, 15, 9–17. [Google Scholar] [CrossRef]
- Jiang, B.; Yang, Y.; Chen, L.; Liu, X.; Wu, X.; Chen, B.; Webster, C.; Sullivan, W.C.; Larsen, L.; Wang, J.; et al. Green spaces, especially nearby forest, may reduce the SARS-CoV-2 infection rate: A nationwide study in the United States. Landsc. Urban Plan. 2022, 228, 104583. [Google Scholar] [CrossRef]
- Klompmaker, J.O.; Hart, J.E.; Holland, I.; Sabath, M.; Wu, X.; Laden, F.; Dominici, F.; James, P. County-level exposures to greenness and associations with COVID-19 incidence and mortality in the United States. Environ. Res. 2021, 199, 111331. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Kim, H.; Choi, H.M.; Heo, S.; Fong, K.C.; Yang, J.; Park, C.; Kim, H.; Bell, M.L. Urban environments and COVID-19 in three Eastern states of the United States. Sci. Total Environ. 2021, 779, 146334. [Google Scholar] [CrossRef]
- Russette, H.; Graham, J.; Holden, Z.; Semmens, E.O.; Williams, E.; Landguth, E.L. Greenspace exposure and COVID-19 mortality in the United States: January–July 2020. Environ. Res. 2021, 198, 111195. [Google Scholar] [CrossRef] [PubMed]
- Parveen, N.; Siddiqui, L.; Sarif, N.; Islam, S.; Khanam, N.; Mohibul, S. Industries in Delhi: Air pollution versus respiratory morbidities. Process. Saf. Environ. Prot. 2021, 152, 495–512. [Google Scholar] [CrossRef]
- Yazdi, M.D.; Wei, Y.; Di, Q.; Requia, W.J.; Shi, L.; Sabath, M.B.; Dominici, F.; Schwartz, J. The effect of long-term exposure to air pollution and seasonal temperature on hospital admissions with cardiovascular and respiratory disease in the United States: A difference-in-differences analysis. Sci. Total Environ. 2022, 843, 156855. [Google Scholar] [CrossRef]
- Diener, A.; Mudu, P. How can vegetation protect us from air pollution? A critical review on green spaces’ mitigation abilities for air-borne particles from a public health perspective—With implications for urban planning. Sci. Total Environ. 2021, 796, 148605. [Google Scholar] [CrossRef]
- Kuo, M. How might contact with nature promote human health? Promising mechanisms and a possible central pathway. Front. Psychol. 2015, 6, 1093. [Google Scholar] [CrossRef]
- Nguyen, Q.C.; Huang, Y.; Kumar, A.; Duan, H.; Keralis, J.M.; Dwivedi, P.; Meng, H.-W.; Brunisholz, K.D.; Jay, J.; Javanmardi, M.; et al. Using 164 Million Google Street View Images to Derive Built Environment Predictors of COVID-19 Cases. Int. J. Environ. Res. Public Health 2020, 17, 6359. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Dai, F.; Diehl, J.A.; Chen, M.; Bai, J. Exploring the spatial pattern of community urban green spaces and COVID-19 risk in Wuhan based on a random forest model. Heliyon 2023, 9, e19773. [Google Scholar] [CrossRef]
- Peng, W.; Dong, Y.; Tian, M.; Yuan, J.; Kan, H.; Jia, X.; Wang, W. City-level greenness exposure is associated with COVID-19 incidence in China. Environ. Res. 2022, 209, 112871. [Google Scholar] [CrossRef]
- Lee, K.-S.; Min, H.S.; Jeon, J.-H.; Choi, Y.-J.; Bang, J.H.; Sung, H.K. The association between greenness exposure and COVID-19 incidence in South Korea: An ecological study. Sci. Total Environ. 2022, 832, 154981. [Google Scholar] [CrossRef]
- You, Y.; Pan, S. Urban Vegetation Slows Down the Spread of Coronavirus Disease (COVID-19) in the United States. Geophys. Res. Lett. 2020, 47, e2020GL089286. [Google Scholar] [CrossRef]
- Liu, C.; Liu, Z.; Guan, C. The impacts of the built environment on the incidence rate of COVID-19: A case study of King County, Washington. Sustain. Cities Soc. 2021, 74, 103144. [Google Scholar] [CrossRef] [PubMed]
- Ciupa, T.; Suligowski, R. Green-Blue Spaces and Population Density versus COVID-19 Cases and Deaths in Poland. Int. J. Environ. Res. Public Health 2020, 18, 6636. [Google Scholar] [CrossRef]
- Lata, K.; Thapa, K.; Rajput, A.S. Liveability of Indian Cities and Spread of COVID-19—Case of Tier-1 Cities. Indian J. Public Adm. 2021, 67, 365–382. [Google Scholar] [CrossRef]
- Huang, J.; Kwan, M.-P.; Kan, Z.; Wong, M.S.; Kwok, C.Y.T.; Yu, X. Investigating the Relationship between the Built Environment and Relative Risk of COVID-19 in Hong Kong. ISPRS Int. J. Geo-Inf. 2020, 9, 624. [Google Scholar] [CrossRef]
- You, H.; Wu, X.; Guo, X. Distribution of COVID-19 Morbidity Rate in Association with Social and Economic Factors in Wuhan, China: Implications for Urban Development. Int. J. Environ. Res. Public Health 2020, 17, 3417. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chen, N.; Du, W.; Li, Y.; Zheng, X. Multi-source sensor based urban habitat and resident health sensing: A case study of Wuhan, China. J. Affect. Disord. 2021, 198, 107883. [Google Scholar] [CrossRef]
- Johnson, T.F.; Hordley, L.A.; Greenwell, M.P.; Evans, L.C. Associations between COVID-19 transmission rates, park use, and landscape structure. Sci. Total Environ. 2021, 789, 148123. [Google Scholar] [CrossRef]
- Pan, J.; Bardhan, R.; Jin, Y. Spatial distributive effects of public green space and COVID-19 infection in London. Urban For. Urban Green. 2021, 62, 127182. [Google Scholar] [CrossRef]
- Zhang, L.; Tan, P.Y. Associations between Urban Green Spaces and Health are Dependent on the Analytical Scale and How Urban Green Spaces are Measured. Int. J. Environ. Res. Public Health 2019, 16, 578. [Google Scholar] [CrossRef]
- Stats SA (Statistics South Africa). 60,6 Million People in South Africa. 2022. Available online: https://www.statssa.gov.za/?p=15601 (accessed on 17 April 2022).
- Stats SA (Statistics South Africa). Mid-Year Population Estimates. 2021. Available online: http://www.statssa.gov.za/publications/P0302/P03022021.pdf (accessed on 17 April 2022).
- Rouget, M.; Reyers, B.; Jonas, Z.; Desmet, P.; Driver, A.; Maze, K.; Egoh, B.; Cowling, R.M. National Spatial Biodiversity Assessment 2004, Technical Report Volume 1: Terrestrial Component; South African National Biodiversity Institute: Pretoria, South Africa, 2004. [Google Scholar]
- SANBI. National Biodiversity Monitoring & Reporting Framework; SANBI: Silverton, South Africa, 2007. [Google Scholar]
- Mamathaba, M.P.; Yessoufou, K.; Moteetee, A. What Does It Take to Further Our Knowledge of Plant Diversity in the Megadiverse South Africa? Diversity 2022, 14, 748. [Google Scholar] [CrossRef]
- De Beers, J. Natural Capita1: Land and Terrestrial Ecosystem Accounts, 1990 to 2014. 2020. Available online: https://www.statssa.gov.za/publications/D04011/D040111990to2014.pdf (accessed on 17 April 2022).
- Dayaram, A.; Harris, L.R.; Grobler, B.A.; Van der Merwe, S.; Rebelo, A.G.; Ward Powrie, L.; Rebelo, A.G.; Powrie, L.W. Vegetation Map of South Africa, Lesotho and Swaziland 2018: A description of changes since 2006. Bothalia 2019, 49, a2452. [Google Scholar] [CrossRef]
- Cox, R.L.; Underwood, E.C. The Importance of Conserving Biodiversity Outside of Protected Areas in Mediterranean Ecosystems. PLoS ONE 2011, 6, e14508. [Google Scholar] [CrossRef]
- Clark, A.; Jit, M.; Warren-Gash, C.; Guthrie, B.; Wang, H.H.X.; Mercer, S.W.; Sanderson, C.; McKee, M.; Troeger, C.; Ong, K.L.; et al. Global, regional, and national estimates of the population at increased risk of severe COVID-19 due to underlying health conditions in 2020: A modelling study. Lancet Glob. Health 2020, 8, e1003–e1017. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 17 April 2022).
- Dean, A.; Voss, D.; Draguljić, D. Design and Analysis of Experiments, 2nd ed.; Springer International Publishing AG: Berlin, Germany, 2017. [Google Scholar]
- Brooks, M.E.; Kristensen, K.; van Benthem, K.J.; Magnusson, A.; Berg, C.W.; Nielsen, A.; Skaug, H.J.; Maechler, M.; Bolker, B.M. glmmTMB Balances Speed and Flexibility Among Packages for Zero-inflated Generalized Linear Mixed Modeling. R J. 2017, 9, 378–400. [Google Scholar] [CrossRef]
- O’Hara, R.B.; Kotze, D.J. Do not log-transform count data. Methods Ecol. Evol. 2010, 1, 118–122. [Google Scholar] [CrossRef]
- Ferrari, S.; Cribari-Neto, F. Beta Regression for Modelling Rates and Proportions. J. Appl. Stat. 2004, 31, 799–815. [Google Scholar] [CrossRef]
- Sy, K.T.L.; White, L.F.; Nichols, B.E. Population density and basic reproductive number of COVID-19 across United States counties. PLoS ONE 2021, 16, e0249271. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, V.; Gadi, N.; Spihlman, A.P.; Wu, S.C.; Choi, C.H.; Moulton, V.R. Aging, Immunity, and COVID-19: How Age Influences the Host Immune Response to Coronavirus Infections? Front. Physiol. 2021, 11, 571416. [Google Scholar] [CrossRef]
- Kim, S.Y.; Yoo, D.M.; Min, C.; Choi, H.G. The Effects of Income Level on Susceptibility to COVID-19 and COVID-19 Morbidity/Mortality: A Nationwide Cohort Study in South Korea. J. Clin. Med. 2021, 10, 4733. [Google Scholar] [CrossRef]
- Lin, J.; Kroll, C.N.; Nowak, D.J.; Greenfield, E.J. A review of urban forest modeling: Implications for management and future research. Urban For. Urban Green. 2019, 43, 126366. [Google Scholar] [CrossRef]
- Chen, Q.X.; Huang, C.L.; Yuan, Y.; Tan, H.P. Influence of COVID-19 event on air quality and their association in mainland China. Aerosol Air Qual. Res. 2020, 20, 1541–1551. [Google Scholar] [CrossRef]
- Reid, C.E.; Clougherty, J.E.; Shmool, J.L.; Kubzansky, L.D. Is All Urban Green Space the Same? A Comparison of the Health Benefits of Trees and Grass in New York City. Int. J. Environ. Res. Public Health 2017, 14, 1411. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Zhou, Y.; Wang, R.; Qian, Z.; Knibbs, L.D.; Jalaludin, B.; Schootman, M.; McMillin, S.E.; Howard, S.W.; Lin, L.-Z.; et al. Associations between trees and grass presence with childhood asthma prevalence using deep learning image segmentation and a novel green view index. Environ. Pollut. 2021, 286, 117582. [Google Scholar] [CrossRef]
- Yessoufou, K.; Sithole, M.; Elansary, H.O. Effects of urban green spaces on human perceived health improvements: Provision of green spaces is not enough but how people use them matters. PLoS ONE 2020, 15, e0239314. [Google Scholar] [CrossRef]
- Vivier, E.; Tomasello, E.; Baratin, M.; Walzer, T.; Ugolini, S. Functions of natural killer cells. Nat. Immunol. 2008, 9, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Cilliers, E.J. Reflecting on Green Infrastructure and Spatial Planning in Africa: The Complexities, Perceptions, and Way Forward. Sustainability 2019, 11, 455. [Google Scholar] [CrossRef]
- Wong, D.W.S.; Li, Y. Spreading of COVID-19: Density matters. PLoS ONE 2020, 15, e0242398. [Google Scholar] [CrossRef]
- Baena-Díez, J.M.; Barroso, M.; Cordeiro-Coelho, S.I.; Díaz, J.L.; Grau, M. Impact of COVID-19 outbreak by income: Hitting hardest the most deprived. J. Public Health 2020, 42, 698–703. [Google Scholar] [CrossRef]
- Finch, W.H.; Finch, M.E.H. Poverty and COVID-19: Rates of Incidence and Deaths in the United States During the First 10 Weeks of the Pandemic. Front. Sociol. 2020, 5, 47. [Google Scholar] [CrossRef]
- Weill, J.A.; Stigler, M.; Deschenes, O.; Springborn, M.R. Social distancing responses to COVID-19 emergency declarations strongly differentiated by income. Proc. Natl Acad. Sci. USA 2020, 117, 19658–19660. [Google Scholar] [CrossRef]
- Chen, J.T.S.; Krieger, N. Revealing the Unequal Burden of COVID-19 by Income, Race/Ethnicity, and Household Crowding: US County Versus Zip Code Analyses. J. Public Health Manag. Pract. 2020, 27, S43–S56. [Google Scholar] [CrossRef] [PubMed]
- McPhearson, T.; Grabowski, Z.; Herreros-Cantis, P.; Mustafa, A.; Ortiz, L.; Kennedy, C.; Tomateo, C.; Lopez, B.; Olivotto, V.; Vantu, A. Pandemic Injustice: Spatial and Social Distributions of COVID-19 in the US Epicenter. J. Extrem. Events 2020, 7, 2150007. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Feng, X.; Mavoa, S.; Badland, H.M.; Giles-Corti, B. Do low-income neighbourhoods have the least green space? A cross-sectional study of Australia’s most populous cities. BMC Public Health 2014, 14, 292. [Google Scholar] [CrossRef] [PubMed]
- Wüstemann, H.; Kalisch, D.; Kolbe, J. Access to urban green space and environmental inequalities in Germany. Landsc. Urban Plan. 2017, 164, 124–131. [Google Scholar] [CrossRef]
- Watkins, S.L.; Gerrish, E. The relationship between urban forests and race: A meta-analysis. J. Environ. Manag. 2018, 209, 152–168. [Google Scholar] [CrossRef]
- Nwosu, E.; Fismen, A.-S.; Helleve, A.; Hongoro, C.; Sewpaul, R.; Reddy, P.; Alaba, O.; Harbron, J. Trends in prevalence of overweight and obesity among South African and European adolescents: A comparative outlook. BMC Public Health 2022, 22, 2287. [Google Scholar] [CrossRef]
- Rideout, A.; Murray, C.; Isles, C. Regional variation in COVID-19 positive hospitalisation across Scotland during the first wave of the pandemic and its relation to population density: A cross-sectional observation study. PLoS ONE 2021, 16, e0253636. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.; Chang, X.; He, Y.; Tan, K.J.K. The determinants of COVID-19 morbidity and mortality across countries. Sci. Rep. 2022, 12, 5888. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.; Hergens, M.-P.; Fors, S.; Tynelius, P.; de Leon, A.P.; Lager, A. Individual and neighborhood risk factors of hospital admission and death during the COVID-19 pandemic: A population-based cohort study. BMC Med. 2023, 21, 1–9. [Google Scholar] [CrossRef]
- COVID-19 Forecasting Team. Variation in the COVID-19 infection–fatality ratio by age, time, and geography during the pre-vaccine era: A systematic analysis. Lancet 2022, 399, 1469–1488. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Estimate (β) | Std. Error (±) | Z Values | PR (>|Z|) | |
|---|---|---|---|---|
| EVI | −0.32 | 0.06461 | −4.95 | <0.001 *** |
| Population density | −0.028 | 0.03497 | −0.81 | 0.419 |
| Revenue per capita | 0.528 | 0.04549 | 11.60 | <0.001 *** |
| Tree cover | −0.287 | 0.06532 | −4.40 | <0.001 *** |
| Population density | −0.036 | 0.03643 | −0.99 | 0.322 |
| Revenue per capita | 0.504 | 0.04529 | 11.12 | <0.001 *** |
| Grass cover | −0.012 | 0.04988 | −0.239 | 0.811 |
| Population density | −0.029 | 0.03938 | −0.740 | 0.459 |
| Revenue per capita | 0.451 | 0.04599 | 9.795 | <0.001 *** |
| Estimate (β) | Std. Error (±) | Z Values | PR (>|Z|) | |
|---|---|---|---|---|
| EVI | −0.219 | 0.05761 | −3.797 | <0.001 *** |
| Age | −0.277 | 0.17975 | −1.543 | 0.123 |
| Population density | −0.561 | 0.42749 | −1.312 | 0.189 |
| Revenue per capita | −1.449 | 0.11653 | −12.436 | <0.001 *** |
| Tree cover | −0.1 | 0.04653 | −2.146 | 0.032 * |
| Age | −0.077 | 0.18387 | −0.419 | 0.675 |
| Population density | −0.27 | 0.39398 | −0.685 | 0.494 |
| Revenue per capita | −1.22 | 0.10575 | −11.534 | <0.001 *** |
| Grass cover | −0.447 | 0.058825 | −7.603 | <0.001 *** |
| Age | −0.005 | 0.190021 | −0.024 | 0.981 |
| Population density | −1.246 | 0.549421 | −2.268 | 0.023 * |
| Revenue per capita | −1.125 | 0.105906 | −10.623 | <0.001 *** |
| Estimate (β) | Std. Error (±) | Z Values | PR (>|Z|) | |
|---|---|---|---|---|
| EVI | −0.123 | 0.09355 | −1.32 | 0.188 |
| Age | −0.461 | 0.18636 | −2.47 | 0.013 * |
| Population density | 0.267 | 0.15066 | 1.77 | 0.077 |
| Revenue per capita | 0.352 | 0.15757 | 2.23 | 0.026 * |
| Tree cover | −0.172 | 0.1080 | −1.59 | 0.111 |
| Age | −0.429 | 0.2069 | −2.08 | 0.038 * |
| Population density | 0.258 | 0.1480 | 1.74 | 0.081 |
| Revenue per capita | 0.322 | 0.1832 | 1.76 | 0.078 |
| Grass cover | 0.103 | 0.1098 | 0.94 | 0.349 |
| Age | −0.433 | 0.2067 | −2.09 | 0.036 * |
| Population density | 0.344 | 0.1655 | 2.08 | 0.038 * |
| Revenue per capita | 0.273 | 0.1520 | 1.79 | 0.073 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phogole, B.; Yessoufou, K. Greener Neighbourhoods Show Resilience to the Spread but Not Severity of COVID-19 Infection in South Africa. Sustainability 2023, 15, 14508. https://doi.org/10.3390/su151914508
Phogole B, Yessoufou K. Greener Neighbourhoods Show Resilience to the Spread but Not Severity of COVID-19 Infection in South Africa. Sustainability. 2023; 15(19):14508. https://doi.org/10.3390/su151914508
Chicago/Turabian StylePhogole, Bopaki, and Kowiyou Yessoufou. 2023. "Greener Neighbourhoods Show Resilience to the Spread but Not Severity of COVID-19 Infection in South Africa" Sustainability 15, no. 19: 14508. https://doi.org/10.3390/su151914508
APA StylePhogole, B., & Yessoufou, K. (2023). Greener Neighbourhoods Show Resilience to the Spread but Not Severity of COVID-19 Infection in South Africa. Sustainability, 15(19), 14508. https://doi.org/10.3390/su151914508