

Factors Affecting Water Quality and Sustainability in Dental Practices in Greece

 ,
, 
 ,
,
Abstract
1. Introduction
2. Background of the Study
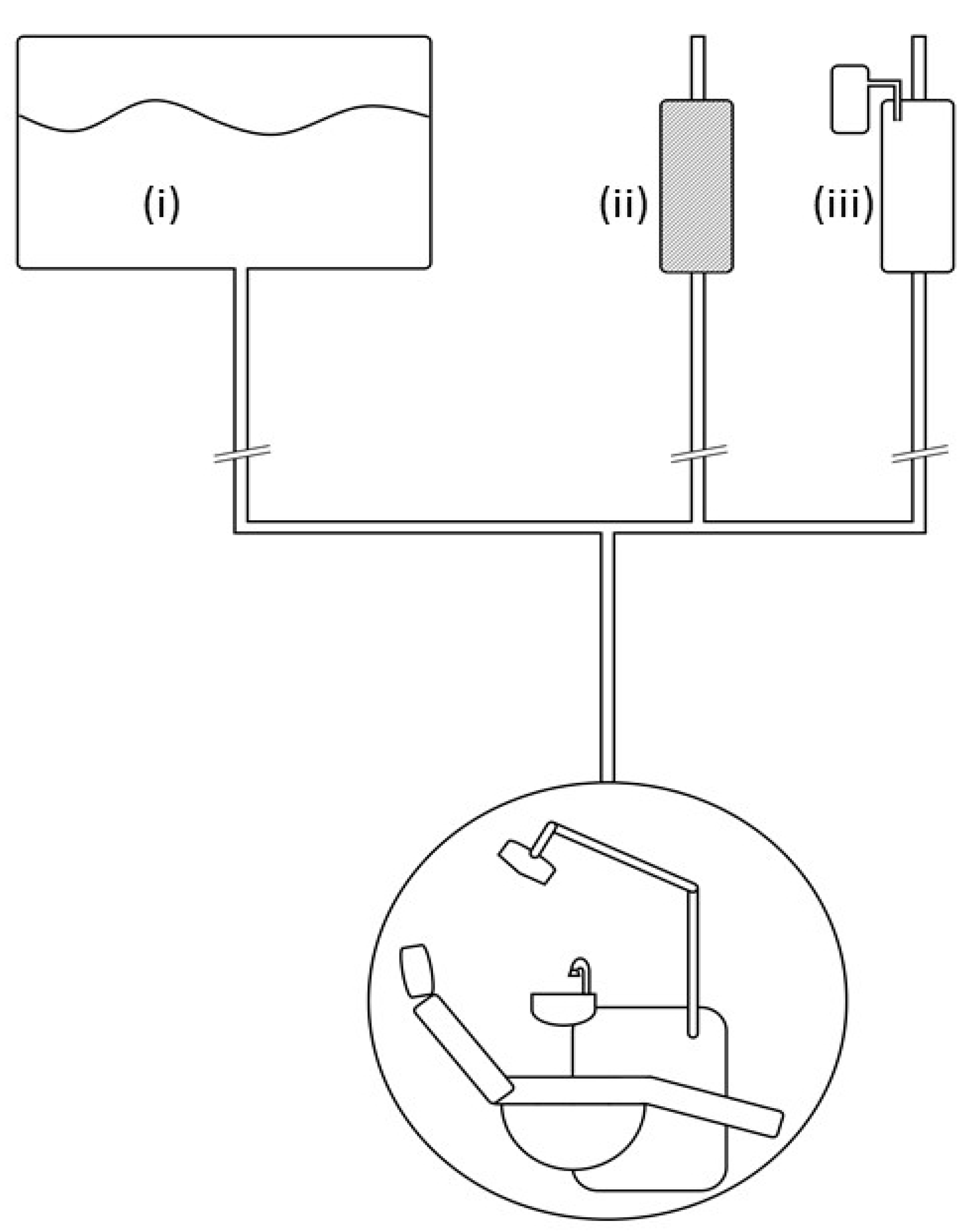
Procedures and Systems for Water Quality Control in the Handpieces and the Dental Unit
3. Research Method
3.1. Design and Validation of the Study Questionnaire
3.2. The Study Sample
3.3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Descriptive Statistics of Dentistry Equipment and Water Quality Practices (n = 206)

{kind=link}
{kind=link}
| n | % | ||
|---|---|---|---|
| Equipment How Old | 0–5 years | 43 | 20.90% |
| 6–10 years | 41 | 19.90% | |
| 11–20 years | 88 | 42.70% | |
| 21 years and older | 34 | 16.50% | |
| Has assistant | No | 109 | 52.90% |
| Yes | 97 | 47.10% | |
| Was informed when acquiring | No | 80 | 38.80% |
| Yes | 126 | 61.20% | |
| Interested in learning more | No | 44 | 21.40% |
| Yes | 162 | 78.60% | |
| Confident about water quality | No | 92 | 44.70% |
| Yes | 114 | 55.30% | |
| Performs microbiological test | No | 161 | 78.20% |
| Yes | 45 | 21.80% | |
| Continuous water supply system dental unit | No | 144 | 69.90% |
| Yes | 62 | 30.10% | |
| Continuous water supply system cutters | No | 137 | 66.50% |
| Yes | 69 | 33.50% | |
| Water supply to the dental unit | Water from public network | 130 | 65.00% |
| Distilled/Deionized water | 15 | 7.50% | |
| Water from a filter device directly connected to the supply | 55 | 27.50% | |
| Water supply to handpieces | Water from public network | 124 | 62.30% |
| Deionized/Distilled water | 22 | 11.10% | |
| Water from a filter device directly connected to the supply | 53 | 26.60% | |
| Supply to ultrasonic scaler | Water from public network | 114 | 58.50% |
| Distilled/Deionized water | 31 | 15.90% | |
| Water from a filter device directly connected to the supply | 50 | 25.60% | |
| Has water filter | No | 91 | 44.20% |
| Yes | 115 | 55.80% | |
| Water filter replaced/cleaned | No filter/Don’t want to answer | 99 | 52.10% |
| every month | 5 | 2.60% | |
| every 6 months | 36 | 18.90% | |
| every 12 months | 21 | 11.10% | |
| every 2 years | 9 | 4.70% | |
| every 5 years + | 4 | 2.10% | |
| whenever there is a problem with the flow | 16 | 8.40% | |
| Knows the active substance of antiseptic Antiseptic to the incisors (auto) | No | 148 | 71.80% |
| Yes | 58 | 28.20% | |
| No | 164 | 90.60% | |
| Antiseptic to the incisors (manually) | Yes | 17 | 9.40% |
| No | 155 | 85.60% | |
| Yes | 26 | 14.40% | |
| Antiseptic reservoir | No | 8 | 3.90% |
| Yes | 198 | 96.10% | |
| Has strong surgical suction | No | 11 | 5.30% |
| Yes | 195 | 94.70% | |
| Small suction | between two patients | 78 | 39.60% |
| every few appointments (3–4) | 37 | 18.80% | |
| per day | 55 | 27.90% | |
| per week | 21 | 10.70% | |
| never before COVID-19 | 4 | 2.00% | |
| never again due to COVID-19 let patients flush | 2 | 1.00% | |
| Surgical suction | between two patients | 18 | 9.00% |
| every few appointments (3–4) | 23 | 11.50% | |
| per day | 89 | 44.50% | |
| per week | 57 | 28.50% | |
| per month | 6 | 3.00% | |
| Never | 7 | 3.50% | |
| Small Suction | between two patients | 90 | 45.50% |
| every few appointments (3–4) | 30 | 15.20% | |
| per day | 53 | 26.80% | |
| per week | 14 | 7.10% | |
| per month | 5 | 2.50% | |
| Never | 6 | 3.00% | |
| Surgical Suction | between two patients | 15 | 7.70% |
| every few appointments (3–4) | 24 | 12.20% | |
| per day | 84 | 42.90% | |
| per week | 58 | 29.60% | |
| per month | 7 | 3.60% | |
| Never | 8 | 4.10% | |
| Dental unit waterline | between two patients | 14 | 7.80% |
| every few appointments (3–4) | 13 | 7.30% | |
| per day | 56 | 31.30% | |
| per week | 54 | 30.20% | |
| per month | 16 | 8.90% | |
| Never | 26 | 14.50% | |
| Disinfecting Surfaces | between two patients | 189 | 92.20% |
| every few appointments (3–4) | 8 | 3.90% | |
| per day | 7 | 3.40% | |
| per week | 1 | 0.50% | |
| Annual maintenance | No | 76 | 38.40% |
| Yes | 122 | 61.60% | |
| Micromotors | 1 | 51 | 24.80% |
| 2 | 69 | 33.50% | |
| 3 | 24 | 11.70% | |
| 4 | 25 | 12.10% | |
| 5+ | 37 | 18.00% | |
| Airotors | 1 | 29 | 14.10% |
| 2 | 63 | 30.60% | |
| 3 | 27 | 13.10% | |
| 4 | 25 | 12.10% | |
| 5+ | 62 | 30.10% | |
| Handpieces Maintenance | Decontamination | 120 | 58.30% |
| Decontamination/Sterilization | 14 | 6.80% | |
| Sterilization | 36 | 17.50% | |
| Surface cleaning | 36 | 17.50% | |
| Has implantology motor | No | 128 | 62.40% |
| Yes | 77 | 37.60% | |
| Via suction vs. central drain | No | 79 | 46.20% |
| Yes | 92 | 53.80% | |
| Has amalgam trap | No | 70 | 35.40% |
| Yes | 128 | 64.60% | |
| Has contract with medical waste collection company | No | 82 | 41.80% |
| Yes | 114 | 58.20% | |
| Has contract for amalgam removal | No | 141 | 73.40% |
| Yes | 51 | 26.60% | |
| Is informed about water quality legislation | No | 167 | 85.60% |
| Yes | 28 | 14.40% | |
| Time spent | no time | 5 | 2.40% |
| up to 2 h per month | 57 | 27.70% | |
| up to 4 h per month | 62 | 30.10% | |
| more than 4 h | 82 | 39.80% | |
| Money spent | EUR 0 per month | 8 | 3.90% |
| less than EUR 25 per month | 44 | 21.40% | |
| EUR 25–50 per month | 89 | 43.20% | |
| EUR 51–75 per month | 38 | 18.40% | |
| more than EUR 75 per month | 27 | 13.10% | |
| Environmentally friendly practices | a little bit | 28 | 15.40% |
| Satisfactorily | 85 | 46.70% | |
| Enough | 50 | 27.50% | |
| very much | 19 | 10.40% | |
| Implementation of disinfection protocol is my responsibility | No | 86 | 41.70% |
| Yes | 120 | 58.30% | |
| Stricter after COVID-19 | No | 99 | 49.30% |
| Yes | 102 | 50.70% |
References
- Department of Health. Environment and Sustainability Health Technical Memorandum 07-04: Water Management and Water Efficiency—Best Practice Advice for the Healthcare Sector. 2013. Available online: http://www.nationalarchives.gov.uk/doc/open-government-licence/ (accessed on 15 March 2023).
- Facciolà, A.; Laganà, P.; Caruso, G. The COVID-19 pandemic and its implications on the environment. Environ. Res. 2021, 201, 111648. [Google Scholar] [CrossRef] [PubMed]
- Lawler, O.K.; Allan, H.L.; Baxter, P.W.J. The COVID-19 pandemic is intricately linked to biodiversity loss and ecosystem health. Lancet Planet. Health 2021, 5, e840–e850. [Google Scholar] [CrossRef] [PubMed]
- Marazziti, D.; Cianconi, P.; Mucci, F.; Foresi, L.; Chiarantini, I.; Della Vecchia, A. Climate change, environment pollution, COVID-19 pandemic and mental health. Sci. Total Environ. 2021, 773, 145182. [Google Scholar] [CrossRef] [PubMed]
- Nandi, S.; Sarkis, J.; Hervani, A.A.; Helms, M.M. Redesigning Supply Chains using Blockchain-Enabled Circular Economy and COVID-19 Experiences. Sustain. Prod. Consum. 2021, 27, 10–22. [Google Scholar] [CrossRef]
- Εuropean Commision. Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee, and the Committee of the Regions. EU Biodiversity Strategy for 2030. Bringing Nature Back into Our Lives. Brussels. 20 May 2020. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=celex%3A52020DC0380 (accessed on 15 March 2023).
- Intergovernmental science-policy Platform for Biodiversity and Ecosystem Services (IPBES). Summary for Policymakers of the Global Assessment Report on Biodiversity and Ecosystem Services of the Intergovernmental Science-Policy Platform on Biodiversity and Ecosystem Services; IPBES: Bonn, Germany, 2019; Volume A.2, p. 12-1. [Google Scholar]
- European Environmental Bureau. EEB Position for a Revised Urban WasteWater Directive. Available online: https://eeb.org/wp-content/uploads/2021/07/EEB-position-for-a-revised-UWWTD.pdf (accessed on 15 April 2023).
- European Parliament. Revision of the Urban Wastewater Treatment Directive. Available online: https://www.europarl.europa.eu/legislative-train/theme-a-european-green-deal/file-revision-of-the-urban-wastewater-treatment-directive-(refit) (accessed on 15 April 2023).
- European Green Deal. Available online: https://www.consilium.europa.eu/en/policies/green-deal/#:~:text=The%20European%20Green%20Deal%20is%20a%20package%20of%20policy%20initiatives,a%20modern%20and%20competitive%20economy (accessed on 15 March 2023).
- CDC. Reduce Risk from Water. Available online: https://www.cdc.gov/hai/prevent/environment/water.html (accessed on 15 April 2023).
- Leach, R. Water Management, and IP Risk. Infect. Cont. Today 2023, 27. Available online: https://www.infectioncontroltoday.com/view/water-management-ip-risk (accessed on 15 April 2023).
- Antoniadou, M.; Tzoutzas, I.; Tzermpos, F.; Panis, V.; Maltezou, H.; Tseroni, M.; Madianos, F. Infection control during COVID-19 outbreak in a university dental school. J. Oral Hyg. Health 2020, 8, 4. [Google Scholar]
- Rezania, S.; Park, J.; Md Din, M.F. Microplastics pollution in different aquatic environments and biota: A review of recent studies. Mar. Pollut. Bull. 2018, 133, 191–208. [Google Scholar] [CrossRef]
- Dulsat-Masvidal, M.; Ciudad, C.; Infante, O.; Mateo, R.; Lacorte, S. Water pollution threats in important bird and biodiversity areas from Spain. J. Hazard Mater. 2023, 448, 130938. [Google Scholar] [CrossRef]
- Szymańska, J.; Sitkowska, J. Bacterial contamination of dental unit waterlines. Environ. Monit. Assess 2013, 185, 3603–3611. [Google Scholar] [CrossRef]
- Yuan, Q.; Zhang, M.; Zhou, J. To Implement A Clear-Water Supply System for Fine-Sediment Experiment in Laboratories. Water 2019, 11, 2476. [Google Scholar] [CrossRef]
- Matys, J.; Grzech-Leśniak, K. Dental Aerosol as a Hazard Risk for Dental Workers. Materials 2020, 13, 5109. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Summary of Infection Prevention Practices in Dental Settings. Basic Expectations for Safe Care. Atlanta, GA: Centers for Disease Control and Prevention, US Dept of Health and Human Services; October 2016. Available online: https://www.cdc.gov/oralhealth/infectioncontrol/pdf/safe-care2.pdf (accessed on 20 March 2023).
- Leoni, E.; Dallolio, L.; Stagni, F.; Sanna, T.; D’Alessandro, G.; Piana, G. Impact of a Risk Management Plan on Legionella Contamination of Dental Unit Water. Int. J. Environ. Res. Public Health 2015, 12, 2344–2358. [Google Scholar] [CrossRef] [PubMed]
- Dallolio, L.; Scuderi, A.; Rini, M.S.; Valente, S.; Farruggia, P.; Bucci Sabattini, M.A.; Leoni, E. Effect of Different Disinfection Protocols on Microbial and Biofilm Contamination of Dental Unit Waterlines in Community Dental Practices. Int. J. Environ. Res. Public Health 2014, 11, 2064–2076. [Google Scholar] [CrossRef] [PubMed]
- Shajahan, I.F.; Kandaswamy, D.; Srikanth, P.; Narayana, L.L.; Selvarajan, R. Dental unit waterlines disinfection using hypochlorous acid-based disinfectant. J. Conserv. Dent. JCD 2016, 19, 347–350. [Google Scholar] [CrossRef]
- Ditommaso, S.; Giacomuzzi, M.; Ricciardi, E.; Zotti, C.M. Efficacy of a Low Dose of Hydrogen Peroxide (Peroxy Ag+) for Continuous Treatment of Dental Unit Water Lines: Challenge Test with Legionella pneumophila Serogroup 1 in a Simulated Dental Unit Waterline. Int. J. Environ. Res. Public Health 2016, 13, 745. [Google Scholar] [CrossRef]
- Lizzadro, J.; Mazzotta, M.; Girolamini, L.; Dormi, A.; Pellati, T.; Cristino, S. Comparison between Two Types of Dental Unit Waterlines: How Evaluation of Microbiological Contamination Can Support Risk Containment. Int. J. Environ. Res. Public Health 2019, 16, 328. [Google Scholar] [CrossRef]
- Cervino, G.; Fiorillo, L.; Laino, L.; Herford, A.S.; Lauritano, F.; Giudice, G.L.; Fama, F.; Santoro, R.; Troiano, G.; Iannello, G. Oral Health Impact Profile in Celiac Patients: Analysis of Recent Findings in a Literature Review. Gastroenterol. Res. Pract. 2018, 2018, 7848735. [Google Scholar] [CrossRef]
- Gawish, S.; Abbass, A.; Abaza, A. Occurrence and biofilm forming ability of Pseudomonas aeruginosa in the water output of dental unit waterlines in a dental center in Alexandria, Egypt. Germs 2019, 9, 71–80. [Google Scholar] [CrossRef]
- Ajami, B.; Ghazvini, K.; Movahhed, T.; Ariaee, N.; Shakeri, M.T.; Makarem, S. Contamination of a Dental Unit Water Line System by Legionella Pneumophila in the Mashhad School of Dentistry in 2009. Iran Red Crescent. Med. J. 2012, 14, 376–378. [Google Scholar]
- Tuvo, B.; Totaro, M.; Cristina, M.L. Prevention and Control of Legionella and Pseudomonas spp. Colonization in Dental Units. Pathogens 2020, 9, 305. [Google Scholar] [CrossRef]
- Pouralibaba, F.; Balaei, E.; Kashefimehr, A. Evaluation of Gram-Negative Bacterial Contamination in Dental Unit Water Supplies in a University Clinic in Tabriz, Iran. J. Dent. Res. Dent. Clin. Dent. Prospect 2011, 5, 94–97. [Google Scholar] [CrossRef]
- Giacomuzzi, M.; Zotti, C.M.; Ditommaso, S. Colonization of Dental Unit Waterlines by Helicobacter pylori: Risk of Exposure in Dental Practices. Int. J. Environ. Res. Public Health 2019, 16, 2981. [Google Scholar] [CrossRef] [PubMed]
- Cicciù, M. Water Contamination Risks at the Dental Clinic. Biology 2020, 9, 43. [Google Scholar] [CrossRef] [PubMed]
- Cárdenas, A.M.; Campos-Bijit, V.; Di Francesco, F.; Schwarz, F.; Cafferata, E.A.; Vernal, R. Electrolyzed water for the microbiologic control in the pandemic dental setting: A systematic review. BMC Oral. Health 2022, 22, 579. [Google Scholar] [CrossRef]
- Hatzenbuehler, L.A.; Tobin-D’Angelo, M.; Drenzek, C.; Peralta, G.; Cranmer, L.C.; Anderson, E.J.; Milla, S.S.; Abramowicz, S.; Yi, J.; Hilinski, J.; et al. Pediatric dental clinic-associated outbreak of Mycobacterium abscessus infection. J. Pediatr. Infect. Dis. Soc. 2017, 6, e116–e122. [Google Scholar] [CrossRef]
- Han, P.; Li, H.; Walsh, L.J.; Ivanovski, S. Splatters and Aerosols Contamination in Dental Aerosol Generating Procedures. Appl. Sci. 2021, 11, 1914. [Google Scholar] [CrossRef]
- Spagnolo, A.M.; Sartini, M.; Cristina, M.L. Microbial Contamination of Dental Unit Waterlines and Potential Risk of Infection: A Narrative Review. Pathogens 2020, 13, 651. [Google Scholar] [CrossRef]
- Fiorillo, L. Conscious Sedation in Dentistry. Medicina 2019, 55, 778. [Google Scholar] [CrossRef]
- Walker, J.T.; Bradshaw, D.J.; Bennett, A.M.; Fulford, M.R.; Martin, M.V.; Marsh, P.D. Microbial Biofilm Formation and Contamination of Dental-Unit Water Systems in General Dental Practice. Appl. Environ. Microbiol. 2000, 66, 3363–3367. [Google Scholar] [CrossRef]
- Walker, J.T.; Bradshaw, D.J.; Fulford, M.R.; Marsh, P.D. Microbiological Evaluation of a Range of Disinfectant Products To Control Mixed-Species Biofilm Contamination in a Laboratory Model of a Dental Unit Water System. Appl. Environ. Microbiol. 2003, 69, 3327–3332. [Google Scholar] [CrossRef]
- Yabune, T.; Imazato, S.; Ebisu, S. Assessment of Inhibitory Effects of Fluoride-Coated Tubes on Biofilm Formation by Using the In Vitro Dental Unit Waterline Biofilm Model. Appl. Environ. Microbiol. 2008, 74, 5958–5964. [Google Scholar] [CrossRef] [PubMed]
- Mills, S.E. The dental unit waterline controversy: Defusing the myths, defining the solutions. J. Am. Dent. Assoc. 2000, 131, 1427–1441. [Google Scholar] [CrossRef]
- EU. Directorate-General for Environment. Proposal for Ecodesign for Sustainable Products Regulation. Annexes—Proposal for a Regulation Establishing a Framework for Setting Ecodesign Requirements for Sustainable Products and Repealing Directive 2009/125/EC. Available online: https://environment.ec.europa.eu/publications/proposal-ecodesign-sustainable-products-regulation_en (accessed on 15 March 2023).
- Cicciu, M.; Fiorillo, L.; Herford, A.S.; Crimi, S.; Bianchi, A.; D’Amico, C.; Laino, L.; Cervino, G. Bioactive Titanium Surfaces: Interactions of Eukaryotic and Prokaryotic Cells of Nano Devices Applied to Dental Practice. Biomedicines 2019, 7, 12. [Google Scholar] [CrossRef]
- Cataldi, M.E.; Al Rakayan, S.; Arcuri, C.; Condò, R. Dental unit wastewater, a current environmental problem: A sistematic review. Oral. Implantol. 2017, 10, 354–359. [Google Scholar] [CrossRef]
- Innes, N.; Johnson, I.G.; Al-Yaseen, W.; Harris, R.; Jones, R.; Kc, S.; McGregor, S.; Robertson, M.; Wade, W.G.; Gallagher, J.E. A systematic review of droplet and aerosol generation in dentistry. J. Dent. 2021, 105, 103556. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, J.I.; Imazato, S. Autoclave sterilization of dental handpieces: A literature review. J. Prosthodont. Res. 2020, 64, 239–242. [Google Scholar] [CrossRef]
- Maltezou, H.; Tseroni, Μ.; Vorou, Ρ.; Koutsolioutsou, A.; Antoniadou, Μ.; Tzoutzas, Ι.; Panis, V.; Tzermpos, F.; Madianos, P. Preparing dental schools to refunction safely during the COVID-19 pandemic: An infection prevention and control perspective. J. Infect. Dev. Ctries. 2021, 15, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Senpuku, H.; Fukumoto, M.; Uchiyama, T.; Taguchi, C.; Suzuki, I.; Arikawa, K. Effects of Extraoral Suction on Droplets and Aerosols for Infection Control Practices. Den. J. 2021, 9, 80. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Osman, A.I.; Rooney, D.W.; Oh, W.-D.; Yap, P.-S. Remediation of Heavy Metals in Polluted Water by Immobilized Algae: Current Applications and Future Perspectives. Sustainability 2023, 15, 5128. [Google Scholar] [CrossRef]
- Engsomboon, N.; Pachimsawat, P.; Thanathornwong, B. Comparative Dissemination of Aerosol and Splatter Using Suction Device during Ultrasonic Scaling: A Pilot Study. Dent. J. 2022, 10, 142. [Google Scholar] [CrossRef]
- Li, Y.; Xu, Z.; Ma, H.S.; Hursthouse, A. Removal of Manganese (II) from Acid Mine Wastewater: A Review of the Challenges and Opportunities with Special Emphasis on Mn-Oxidizing Bacteria and Microalgae. Water 2019, 11, 2493. [Google Scholar] [CrossRef]
- Engelmann, C.; Schmidt, L.; Werth, C.J.; Walther, M. Quantification of Uncertainties from Image Processing and Analysis in Laboratory-Scale DNAPL Release Studies Evaluated by Reflective Optical Imaging. Water 2019, 11, 2274. [Google Scholar] [CrossRef]
- Yoon, H.Y.; Lee, S.Y. Susceptibility of bacteria isolated from dental unit waterlines to disinfecting chemical agents. J. Gen. Appl. Microbiol. 2019, 64, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Costa, D.; Girardot, M.; Bertaux, J.; Verdon, J.; Imbert, C. Efficacy of dental unit waterlines disinfectants on a polymicrobial biofilm. Water Res. 2016, 91, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Hoogenkamp, M.A.; Brandt, B.W.; Laheij, A.M.G.A.; de Soet, J.J.; Crielaard, W. The microbiological load and microbiome of the Dutch dental unit; ‘please, hold your breath’. Water Res. 2021, 200, 117205. [Google Scholar] [CrossRef]
- EYDAP Sustainable Development Report. Sustainable Development EYDAP SA. Athens. 2021. Available online: https://www.eydap.gr/userfiles/Presentations/presentations/EYDAP_CSR_2021_21x29-7CM_F13_WEB/index.html#page=1 (accessed on 15 March 2023).
- Gawlik, B.M.; Easton, P.; Koop, S.; Van Leeuwen, K.; Elelman, R. (Eds.) Urban Water Atlas for Europe; European Commission, Publications Office of the European Union: Luxembourg, 2017. [Google Scholar] [CrossRef]
- Putnins, E.E.; Di Giovanni, D.; Bhullar, A.S. Dental unit waterline contamination and its possible implications during periodontal surgery. J. Periodontol. 2001, 72, 393–400. [Google Scholar] [CrossRef]
- Toomarian, L.; Rikhtegaran, S.; Sadighi, M.; Savadi Oskoee, S.; Alizadeh Oskoee, P. Contamination of Dental Unit Water and Air Outlets Following Use of Clean Head System and Conventional Handpieces. J. Dent. Res. Dent. Clin. Dent. Prospect. 2007, 1, 43–47. [Google Scholar] [CrossRef]
- Laino, L.; Cicciù, M.; Fiorillo, L.; Crimi, S.; Bianchi, A.; Amoroso, G.; Monte, I.P.; Herford, A.S.; Cervino, G. Surgical Risk on Patients with Coagulopathies: Guidelines on Hemophiliac Patients for Oro-Maxillofacial Surgery. Int. J. Environ. Res. Public Health 2019, 16, 1386. [Google Scholar] [CrossRef]
- Takenaka, S.; Sotozono, M.; Yashiro, A.; Saito, R.; Kornsombut, N.; Naksagoon, T.; Nagata, R.; Ida, T.; Edanami, N.; Noiri, Y. Efficacy of Combining an Extraoral High-Volume Evacuator with Preprocedural Mouth Rinsing in Reducing Aerosol Contamination Produced by Ultrasonic Scaling. Int. J. Environ. Res. Public Health 2022, 19, 6048. [Google Scholar] [CrossRef]
- Adedoja, O.S.; Hamam, Y.; Khalaf, B.; Sadiku, R. Development of a Contaminant Distribution Model for Water Supply Systems. Water 2019, 11, 1510. [Google Scholar] [CrossRef]
- Acosta-Gio, E.; Bednarsh, H.; Cuny, E.; Eklund, K.; Mills, S.; Risk, D. Sterilization of dental handpieces. Am. J. Infect. Control 2017, 45, 937–938. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.T.; Marsh, P.D. Microbial biofilm formation in DUWS and their control using disinfectants. J. Dent. 2007, 35, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Offner, D.; Fioretti, F.; Musset, A.-M. Contamination of dental unit waterlines: Assessment of three continuous water disinfection systems. BDJ Open 2016, 2, 1–6. [Google Scholar] [CrossRef]
- Pawar, A.; Garg, S.; Mehta, S.; Dang, R. Breaking the Chain of Infection: Dental Unit Water Quality Control. J. Clin. Diagn. Res. 2016, 10, ZC80–ZC84. [Google Scholar] [CrossRef] [PubMed]
- Garg, S.K.; Mittal, S.; Kaur, P. Dental unit waterline management: Historical perspectives and current trends. J. Investig. Clin. Dent. 2012, 3, 247–252. [Google Scholar] [CrossRef]
- Fujita, M.; Mashima, I.; Nakazawa, F. Monitoring the decontamination efficacy of the novel Poseidon-S disinfectant system in dental unit water lines. J. Microbiol. Immunol. Infect. 2017, 50, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Noopan, S.; Unchui, P.; Techotinnakorn, S.; Ampornaramveth, R.S. Plasma Sterilization Effectively Reduces Bacterial Contamination in Dental Unit Waterlines. Int. J. Dent. 2019, 2019, 5720204. [Google Scholar] [CrossRef]
- Pantanella, F.; Schippa, S.; Solimini, A.; Rosa, L.; Bettucci, A.; Berlutti, F. Efficacy of acoustic waves in preventing Streptococcus mutans adhesion on dental unit water line. Ann. Ig. 2019, 31, 109–116. [Google Scholar] [CrossRef]
- Troiano, G.; Laino, L.; Cicciu, M.; Cervino, G.; Fiorillo, L.; D’Amico, C.; Zhurakivska, K.; Lo Muzio, L. Comparison of Two Routes of Administration of Dexamethasone to Reduce the Postoperative Sequelae after Third Molar Surgery: A Systematic Review and Meta-Analysis. Open. Dent. J. 2018, 12, 181–188. [Google Scholar] [CrossRef]
- Kohn, W.G.; Collins, A.S.; Cleveland, J.L.; Harte, J.A.; Eklund, K.J.; Malvitz, D.M. Centers for Disease Control and Prevention (CDC). Guidelines for infection control in dental health-care settings-2003. MMWR Recomm. Rep. 2003, 52, RR-17. [Google Scholar]
- American Dental Association ADA Statement on Dental unit waterlines. J. Am. Dent. Assoc. 1996, 127, 185–186. [CrossRef]
- Alkhulaifi, M.M.; Alotaibi, D.H.; Alajlan, H.; Binshoail, T. Assessment of nosocomial bacterial contamination in dental unit waterlines: Impact of flushing. Saudi Dent. J. 2020, 32, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, L. We Do Not Eat Alone: Formation and Maturation of the Oral Microbiota. Biology 2020, 9, 17. [Google Scholar] [CrossRef]
- Antoniadou, M. Quality of Life and Satisfaction from Career and Work–Life Integration of Greek Dentists before and during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 9865. [Google Scholar] [CrossRef] [PubMed]
- Antoniadou, M.; Chrysochoou, G.; Tzanetopoulos, R.; Riza, E. Green Dental Environmentalism among Students and Dentists in Greece. Sustainability, 2023; under review. [Google Scholar]
- Pasquarella, C.; Veronesi, L.; Napoli, C. Microbial environmental contamination in Italian dental clinics: A multicenter study yielding recommendations for standardized sampling methods and threshold values. Sci. Total. Environ. 2012, 420, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Ping, Y.; Zhou, R.; Wang, J.; Zhang, G. High throughput sequencing-based analysis of microbial diversity in dental unit waterlines supports the importance of providing safe water for clinical use. J. Infect. Public Health 2018, 11, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Water Information System for Europe (WISE). Available online: http://water.europa.eu/ (accessed on 20 March 2023).
- European Innovation Partnership on Water. Available online: http://ec.europa.eu/environment/water/innovationpartnership/ (accessed on 15 March 2023).
- Tims, M.; Bakker, A.B.; Derks, D. Development and validation of the job crafting scale. J. Vocational. Behav. 2012, 80, 173–186. [Google Scholar] [CrossRef]
- Bursac, Z.; Gauss, C.H.; Williams, D.K. Purposeful selection of variables in logistic regression. Source Code. Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef] [PubMed]
- Green, H.; Weller, D.; Johnson, S.; Michalenko, E. Microbial Source-Tracking Reveals Origins of Fecal Contamination in a Recovering Watershed. Water 2019, 11, 2162. [Google Scholar] [CrossRef]
- Ayers, K.M.; Thomson, W.M.; Rich, A.M.; Newton, J.T. Gender differences in dentists’ working practices and job satisfaction. J. Dent. 2008, 36, 343–350. [Google Scholar] [CrossRef]
- McKay, J.C.; Ahmad, A.; Shaw, J.L.; Rashid, F.; Clancy, A.; David, C. Gender differences and predictors of work hours in a sample of Ontario dentists. J. Can. Dent. Assoc. 2016, 82, 1488–2159. [Google Scholar]
- Walker, S. Work pattern differences between male and female orthodontists in Canada. J. Can. Dent. Assoc. 2016, 82, g6. [Google Scholar] [PubMed]
- Emrani, R.; Sargeran, K.; Shamshiri, A.R.; Hessari, H. Job satisfaction among dentists according to workplace in Tehran. Front. Dent. 2021, 18, 11. [Google Scholar] [CrossRef] [PubMed]
- Surdu, S.; Mertz, E.; Langelier, M.; Moore, J. Dental workforce trends: A national study of gender diversity and practice patterns. Med. Care. Res. Rev. 2021, 78 (Suppl. 1), 30S–39S. [Google Scholar] [CrossRef] [PubMed]
- Archer, J. The reality and evolutionary significance of human psychological sex differences. Biology 2019, 94, 1381–1415. [Google Scholar] [CrossRef] [PubMed]
- Baptiste, D.; Fecher, A.M.; Dolejs, S.C.; Yoder, J.; Schmidt, C.M.; Couch, M.E. Gender differences in academic surgery, work-life balance, and satisfaction. J. Surg. Res. 2017, 218, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Rich-Edwards, J.W.; Kaiser, U.B.; Chen, G.L.; Manson, J.E.; Goldstein, J.M. Sex and gender differences research design for basic, clinical, and population studies: Essentials for investigators. Endocr. Rev. 2018, 39, 424–439. [Google Scholar] [CrossRef] [PubMed]
- Shannon, G.; Jansen, M.; Williams, K.; Cáceres, C.; Motta, A.; Odhiambo, A. Gender equality in science, medicine, and global health: Where are we at and why does it matter? Lancet 2019, 393, 560–569. [Google Scholar] [CrossRef]
- Nirupama, Y.S.; Boppana, N.K.; Vinnakota, N.R.; Thetakala, R.K.; Kallakuri, P.; Karthik, B.K. Indian women dentists’ perspectives towards balancing professional, personal and social responsibilities. Indian. J. Dent. Res. 2020, 31, 358–362. [Google Scholar] [CrossRef]
- Antoniadou, M. Estimation of Factors Affecting Burnout in Greek Dentists before and during the COVID-19 Pandemic. Dent. J. 2022, 10, 108. [Google Scholar] [CrossRef]
- Dousin, O.; Collins, N.; Kler, B.K. The experience of work-life balance for women doctors and nurses in Malaysia. Asia. Pac. J. Hum. Resour. 2022, 60, 362–380. [Google Scholar] [CrossRef]
- McCarthy, G.M.; MacDonald, J.K. Gender differences in characteristics, infection control practices, knowledge and attitudes related to HIV among Ontario dentists. Commun. Dent. Oral. Epidemiol. 1996, 24, 412–415. [Google Scholar] [CrossRef] [PubMed]
- Reza, E.; Sargeran, K.; Hessari, H.; Masoumeh, E. Differences in the work pattern of male and female dentists in Tehran in 2021. Ital. J. Gend. Specif. Med. 2022, 8, 143–146. [Google Scholar] [CrossRef]
- Li, J.; de Souza, R.; Esfandiari, S.; Feine, J. Have women broken the glass ceiling in North American dental leadership? J. Adv. Dent. Res. 2019, 30, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Shahin, S.Y.; Bugshan, A.S.; Almulhim, K.S.; AlSharief, M.S.; Al-Dulaijan, Y.A.; Siddiqui, I.; Al-Qarni, F.D. Knowledge of dentists, dental auxiliaries, and students regarding the COVID-19 pandemic in Saudi Arabia: A cross-sectional survey. BMC Oral. Health 2020, 20, 363. [Google Scholar] [CrossRef]
- Qabool, H.; Sukhia, R.H.; Fida, M. Knowledge and awareness of dental specialists, general dentists and dental assistants regarding SARS-CoV-2. Dent. Med. Probl. 2021, 58, 285–290. [Google Scholar] [CrossRef]
- Schalli, M.; Kogler, B.; Miorini, T.; Gehrer, M.; Reinthaler, F.F. High-Speed Dental Instruments: An Investigation of Protein-Contaminated Dental Handpieces with the Bicinchoninic Acid Assay in Dental Offices in Styria, Austria. Int. J. Environ. Res. Public Health 2023, 20, 1670. [Google Scholar] [CrossRef]
- Deshpande, A.; Smith, G.W.; Smith, A.J. Biofouling of surgical power tools during routine use. J. Hosp. Infect. 2015, 90, 179–185. [Google Scholar] [CrossRef]
- Rosa, V.; Agarwalla, S.V.; Tan, B.L.; Choo, S.Y.; Sim, Y.F.; Boey, F.Y.C.; Anantharaman, S.; Duggal, M.S.; Tan, K.S. Pandemic Preparedness and Response: A Foldable Tent to Safely Remove Contaminated Dental Aerosols—Clinical Study and Patient Experience. Appl. Sci. 2022, 12, 7409. [Google Scholar] [CrossRef]
- Pinto, F.M.; Bruna, C.Q.; Camargo, T.C.; Marques, M.; Silva, C.B.; Sasagawa, S.M. The practice of disinfection of high-speed handpieces with 70% w/v alcohol: An evaluation. Am. J. Infect. Control 2017, 45, e19–e22. [Google Scholar] [CrossRef]
- Osegueda-Espinosa, A.A.; Sanchez-Perez, L.; Perea-Perez, B.; Labajo-Gonzalez, E.; Acosta-Gio, A.E. Dentists survey adverse events during their clinical training. J. Patient Saf. 2020, 16, e240–e244. [Google Scholar] [CrossRef] [PubMed]
- Hbibi, A.; Kasouati, J.; Charof, R.; Chaouir, S.; El Harti, K. Evaluation of the knowledge and attitudes of dental students toward occupational blood exposure accidents at the end of the dental training program. J Int.Soc. Prev. Commun. Dent. 2018, 8, 77–86. [Google Scholar]
- Agahi, R.H.; Hashemipour, M.A.; Kalantari, M.; Ayatollah-Mosavi, A.; Aghassi, H.; Nassab, A.H.G. Effect of 0.2% chlorhexidine on microbial and fungal contamination of dental unit waterlines. Dent. Res. 2014, 11, 351–356. [Google Scholar]
- Dupont, D.; Adamowicz, W.L.; Krupnick, A. Differences in water consumption choices in Canada: The role of socio-demographics, experiences, and perceptions of health risks. J. Water Health 2010, 8, 671–686. [Google Scholar] [CrossRef] [PubMed]
- Banakar, M.; Bagheri Lankarani, K.; Jafarpour, D. COVID-19 transmission risk and protective protocols in dentistry: A systematic review. BMC. Oral. Health 2020, 20, 275. [Google Scholar] [CrossRef] [PubMed]
- Chate, R.A. An audit improves the quality of water within the dental unit water lines of general dental practices across the East of England. Br. Dent. J. 2010, 209, E11. [Google Scholar] [CrossRef] [PubMed]
- Baudet, A.; Lizon, J.; Martrette, J.M.; Camelot, F.; Florentin, A.; Clément, C. Efficacy of BRS® and Alpron®/Bilpron® Disinfectants for Dental Unit Waterlines: A Six-Year Study. Int. J. Environ. Res. Public Health 2020, 17, 2634. [Google Scholar] [CrossRef]
- Italian Health Ministry. Guidelines for Prevention and Control of Legionellosis. Rome, Italy, 2015. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2362_allegato.pdf (accessed on 15 March 2023).
- McManus, K.R.; Fan, P.L. Purchasing, installing and operating dental amalgam separators: Practical issues. J. Am. Dent. Assoc. 2003, 134, 1054–1065. [Google Scholar] [CrossRef]
- Spaveras, A.; Antoniadou, M. Awareness of Students and Dentists on Sustainability Issues, Safety of Use and Disposal of Dental Amalgam. Dent. J. 2023, 11, 21. [Google Scholar] [CrossRef]
- Oosthuysen, J.; Potgieter, E.; Fossey, A. Compliance with infection prevention and control in oral health-care facilities: A global perspective. Int. Dent. J. 2014, 64, 297–311. [Google Scholar] [CrossRef]
- Carraro, E.; Bonetta, S.; Bonetta, S. Hospital Wastewater: Existing Regulations and Current Trends in Management. In Hospital Wastewaters. The Handbook of Environmental Chemistry; Verlicchi, P., Ed.; Springer: Cham, Switzerland, 2017; Volume 60. [Google Scholar] [CrossRef]


| n | % | ||
|---|---|---|---|
| Gender | Men | 117 | 56.8% |
| Women | 88 | 42.7% | |
| Other | 1 | 0.5% | |
| Family Status | Unmarried | 48 | 23.3% |
| Married | 139 | 67.5% | |
| Other | 19 | 9.2% | |
| Age | up to 30 years | 15 | 7.3% |
| 31–40 | 29 | 14.1% | |
| 41–50 | 64 | 31.1% | |
| 51–60 | 60 | 29.1% | |
| 60+ | 38 | 18.4% | |
| Workplace | Athens or urban center | 190 | 92.2% |
| Province | 16 | 7.8% | |
| Experience | 0–10 years | 32 | 15.5% |
| 11–20 years | 59 | 28.6% | |
| 21–30 years | 57 | 27.7% | |
| 30+ | 58 | 28.2% | |
| Family Income | up to EUR 25,000 | 69 | 33.5% |
| EUR 25,001–50,000 | 90 | 43.7% | |
| 50,001 and above | 39 | 18.9% | |
| I don’t want to answer | 8 | 3.9% | |
| Education | Basic dental education in Greece | 89 | 43.2% |
| Basic dental education abroad | 38 | 18.4% | |
| Postgraduate education | 103 | 50.0% | |
| Recognized specialty | 21 | 10.2% | |
| Clinical activity | General dentistry | 156 | 75.7% |
| other activities | 50 | 24.3% | |
| Dental practice | private dental practice | 136 | 66.0% |
| dental clinic | 57 | 27.7% | |
| Other | 13 | 6.3% | |
| Female | Male | χ2(p) | ||||
|---|---|---|---|---|---|---|
| n | % | N | % | |||
| Interested in learning more | 77 | 87.50% | 84 | 71.80% | 7.35 (0.006) | |
| Continuous water supply system cutters | 22 | 25.00% | 47 | 40.20% | 5.17 (0.023) | |
| Water supply to the dental unit | Water from public network | 62 | 73.80% | 67 | 58.30% | 8.90 (0.012) |
| Distilled/Deionized water | 8 | 9.50% | 7 | 6.10% | ||
| Water from a filter device directly connected to the supply | 14 | 16.70% | 41 | 35.70% | ||
| Water supply to the handpieces | Water from public network | 58 | 70.70% | 66 | 56.90% | 6.72 (0.035) |
| Deionized/Distilled water | 10 | 12.20% | 11 | 9.50% | ||
| Water from a filter device directly connected to the supply | 14 | 17.10% | 39 | 33.60% | ||
| Supply to ultrasonic scaler | Water from public network | 55 | 68.80% | 59 | 51.80% | 10.31 (0.006) |
| Distilled/Deionized water | 14 | 17.50% | 16 | 14.00% | ||
| Water from a filter device directly connected to the supply | 11 | 13.80% | 39 | 34.20% | ||
| Disinf. Surfaces | between two patients | 85 | 97.70% | 103 | 88.00% | 12.54 (0.028) |
| every few appointments | 0 | 0.00% | 8 | 6.80% | ||
| per day | 1 | 1.10% | 6 | 5.10% | ||
| per week | 1 | 1.10% | 0 | 0.00% | ||
| Annual maintenance | 55 | 66.30% | 66 | 57.90% | 10.10 (0.018) | |
| Has implantology motor | 24 | 27.60% | 52 | 44.40% | 6.07 (0.014) | |
| Experience | χ2(p) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 0–10 Years | 11–20 Years | 21–30 Years | 31 Years and Over | |||||||
| n | % | n | % | n | % | N | % | |||
| Water supply to the dental unit | Water from public network | 25 | 89.30% | 36 | 63.20% | 37 | 64.90% | 32 | 55.20% | 13.70 (0.033) |
| Distilled/Deionized water | 1 | 3.60% | 7 | 12.30% | 4 | 7.00% | 3 | 5.20% | ||
| Water from filter | 2 | 7.10% | 14 | 24.60% | 16 | 28.10% | 23 | 39.70% | ||
| Water supply to the handpieces | Water from public network | 24 | 92.30% | 37 | 62.70% | 34 | 60.70% | 29 | 50.00% | 16.69 (0.010) |
| Deionized/Distilled water | 1 | 3.80% | 9 | 15.30% | 6 | 10.70% | 6 | 10.30% | ||
| Water from filter | 1 | 3.80% | 13 | 22.00% | 16 | 28.60% | 23 | 39.70% | ||
| Supply to ultrasonic scaler | Water from public network | 21 | 80.80% | 38 | 64.40% | 32 | 58.20% | 23 | 41.80% | 13.63 (0.034) |
| Distilled/Deionized water | 3 | 11.50% | 8 | 13.60% | 7 | 12.70% | 13 | 23.60% | ||
| Water from filter | 2 | 7.70% | 13 | 22.00% | 16 | 29.10% | 19 | 34.50% | ||
| Large amount of water through surgical suction to the dental unit | between two patients | 5 | 17.20% | 0 | 0.00% | 2 | 3.60% | 8 | 15.10% | 31.12 (0.008) |
| every few appointments (3–4) | 2 | 6.90% | 5 | 8.60% | 10 | 17.90% | 7 | 13.20% | ||
| per day | 9 | 31.00% | 28 | 48.30% | 22 | 39.30% | 25 | 47.20% | ||
| per week or more | 13 | 44.80% | 25 | 43.10% | 22 | 39.40% | 13 | 24.60% | ||
| Large amount of water to the dental unit | between two patients | 4 | 16.00% | 2 | 3.80% | 4 | 8.30% | 4 | 7.40% | 27.69 (0.024) |
| every few appointments (3–4) | 1 | 4.00% | 3 | 5.80% | 2 | 4.20% | 7 | 13.00% | ||
| per day | 10 | 40.00% | 11 | 21.20% | 13 | 27.10% | 22 | 40.70% | ||
| per week or more | 10 | 40.00% | 36 | 69.30% | 29 | 60.40% | 21 | 39.00% | ||
| Micromotors | 1 | 15 | 46.90% | 18 | 30.50% | 12 | 21.10% | 6 | 10.30% | 25.92 (0.011) |
| 2 | 5 | 15.60% | 22 | 37.30% | 19 | 33.30% | 23 | 39.70% | ||
| 3 | 3 | 9.40% | 5 | 8.50% | 9 | 15.80% | 7 | 12.10% | ||
| 4 | 3 | 9.40% | 8 | 13.60% | 3 | 5.30% | 11 | 19.00% | ||
| 5+ | 6 | 18.80% | 6 | 10.20% | 14 | 24.60% | 11 | 19.00% | ||
| Airotors | 1 | 11 | 34.40% | 8 | 13.60% | 5 | 8.80% | 5 | 8.60% | 29.17 (0.004) |
| 2 | 10 | 31.30% | 20 | 33.90% | 17 | 29.80% | 16 | 27.60% | ||
| 3 | 1 | 3.10% | 14 | 23.70% | 5 | 8.80% | 7 | 12.10% | ||
| 4 | 3 | 9.40% | 5 | 8.50% | 11 | 19.30% | 6 | 10.30% | ||
| 5+ | 7 | 21.90% | 12 | 20.30% | 19 | 33.30% | 24 | 41.40% | ||
| Is informed about water quality legislation | 8 | 27.60% | 3 | 5.40% | 7 | 13.20% | 10 | 17.50% | 8.34 (0.039) | |
| Time Spent | no time | 4 | 12.50% | 0 | 0.00% | 1 | 1.80% | 0 | 0.00% | 26.21 (0.002) |
| up to 2 h per month | 13 | 40.60% | 13 | 22.00% | 15 | 26.30% | 16 | 27.60% | ||
| up to 4 h per month | 10 | 31.30% | 22 | 37.30% | 14 | 24.60% | 16 | 27.60% | ||
| more than 4 h | 5 | 15.60% | 24 | 40.70% | 27 | 47.40% | 26 | 44.80% | ||
| Education Abroad | χ2(p) | Postgraduate Education | χ2(p) | Recognized Specialty | χ2(p) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No | Yes | No | Yes | No | Yes | |||||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |||||
| Has assistant | 83 | 49.40% | 14 | 36.80% | ns | 41 | 35.70% | 56 | 61.50% | 13.66 (<0.001) | 82 | 44.30% | 15 | 71.40% | 5.56 (0.018) | |
| Knows the active substance of antiseptic | 45 | 31.70% | 13 | 39.40% | ns | 25 | 25.50% | 33 | 42.90% | 5.86 (0.016) | 55 | 35.00% | 3 | 16.70% | ns | |
| Antiseptic to the handpieces (auto) | 15 | 9.90% | 2 | 6.70% | ns | 5 | 4.90% | 12 | 15.20% | 5.54 (0.019) | 15 | 9.20% | 2 | 11.10% | ns | |
| Antiseptic to the handpieces (manually) | 17 | 11.30% | 9 | 30.00% | 7.15 (0.008) | 18 | 17.60% | 8 | 10.10% | ns | 25 | 15.30% | 1 | 5.60% | ns | |
| Small Suction | between two patients | 80 | 50.00% | 10 | 26.30% | 13.26 (0.021) | 44 | 40.70% | 46 | 51.10% | 13.04 (0.023) | 85 | 47.80% | 5 | 25.00% | ns |
| every few appointments | 25 | 15.60% | 5 | 13.20% | 13 | 12.00% | 17 | 18.90% | 28 | 15.70% | 2 | 10.00% | ||||
| per day | 36 | 22.50% | 17 | 44.70% | 38 | 35.20% | 15 | 16.70% | 45 | 25.30% | 8 | 40.00% | ||||
| per week or more | 19 | 11.80% | 6 | 15.8% | 13 | 12.00% | 12 | 13.40% | 20 | 11.20% | 5 | 25.00% | ||||
| Annual maintenance | 103 | 64.00% | 19 | 51.40% | ns | 58 | 53.20% | 64 | 71.90% | 7.24 (0.007) | 114 | 64.00% | 8 | 40.00% | 4.40 (0.036) | |
| Micromotors | 1 | 38 | 22.60% | 13 | 34.20% | ns | 34 | 29.60% | 17 | 18.70% | 12.72 (0.013) | 43 | 23.20% | 8 | 38.10% | ns |
| 2 | 55 | 32.70% | 14 | 36.80% | 41 | 35.70% | 28 | 30.80% | 63 | 34.10% | 6 | 28.60% | ||||
| 3 | 20 | 11.90% | 4 | 10.50% | 8 | 7.00% | 16 | 17.60% | 22 | 11.90% | 2 | 9.50% | ||||
| 4 | 22 | 13.10% | 3 | 7.90% | 17 | 14.80% | 8 | 8.80% | 24 | 13.00% | 1 | 4.80% | ||||
| 5+ | 33 | 19.60% | 4 | 10.50% | 15 | 13.00% | 22 | 24.20% | 33 | 17.80% | 4 | 19.00% | ||||
| Airotors | 1 | 21 | 12.50% | 8 | 21.10% | ns | 21 | 18.30% | 8 | 8.80% | 8.94 (0.063) | 20 | 10.80% | 9 | 42.90% | 22.76 (<0.001) |
| 2 | 49 | 29.20% | 14 | 36.80% | 36 | 31.30% | 27 | 29.70% | 54 | 29.20% | 9 | 42.90% | ||||
| 3 | 21 | 12.50% | 6 | 15.80% | 16 | 13.90% | 11 | 12.10% | 27 | 14.60% | 0 | 0.00% | ||||
| 4 | 21 | 12.50% | 4 | 10.50% | 16 | 13.90% | 9 | 9.90% | 25 | 13.50% | 0 | 0.00% | ||||
| 5+ | 56 | 33.30% | 6 | 15.80% | 26 | 22.60% | 36 | 39.60% | 59 | 31.90% | 3 | 14.30% | ||||
| Has amalgam trap | 106 | 65.80% | 22 | 59.50% | ns | 70 | 63.60% | 58 | 65.90% | ns | 121 | 68.00% | 7 | 35.00% | 8.56 (0.003) | |
| Has contract for amalgam removal | 42 | 27.30% | 9 | 23.70% | ns | 22 | 20.60% | 29 | 34.10% | 4.46 (0.035) | 48 | 28.10% | 3 | 14.30% | ns | |
| Environment-friendly practices | A little | 26 | 17.20% | 2 | 6.50% | 10.93 (0.012) | 18 | 17.10% | 10 | 13.00% | ns | 28 | 17.10% | 0 | 0.00% | ns |
| Satisfactory | 73 | 48.30% | 12 | 38.70% | 48 | 45.70% | 37 | 48.10% | 76 | 46.30% | 9 | 50.00% | ||||
| Enough | 41 | 27.20% | 9 | 29.00% | 30 | 28.60% | 20 | 26.00% | 43 | 26.20% | 7 | 38.90% | ||||
| Very much | 11 | 7.30% | 8 | 25.80% | 9 | 8.60% | 10 | 13.00% | 17 | 10.40% | 2 | 11.10% | ||||
| Implementation of disinfection protocol is my responsibility | 99 | 58.90% | 21 | 55.30% | ns | 76 | 66.10% | 44 | 48.40% | 6.57(0.010) | 111 | 60.00% | 9 | 42.90% | ns | |
| General Dentistry | χ2(p) | Clinic vs. Private Practice | χ2(p) | Family Income | χ2(p) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No | Yes | No | Yes | EUR < 25.000 | 25.001–50.000 € | EUR > 50.000 | ||||||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | |||||
| Equipment age | 0–5 years | 12 | 24.00% | 31 | 19.90% | ns | 30 | 19.90% | 13 | 23.60% | 16.12 (0.001) | 19 | 27.50% | 11 | 12.20% | 10 | 57.50% | ns |
| 6–10 years | 13 | 26.00% | 28 | 17.90% | 21 | 13.90% | 20 | 36.40% | 12 | 17.40% | 17 | 18.90% | 11 | 30.30% | ||||
| 11–20 years | 17 | 34.00% | 71 | 45.50% | 70 | 46.40% | 18 | 32.70% | 30 | 43.50% | 44 | 48.90% | 11 | 30.30% | ||||
| 21 and above | 8 | 16.00% | 26 | 16.70% | 30 | 19.90% | 4 | 7.30% | 8 | 11.60% | 18 | 20.00% | 7 | 15.20% | ||||
| Has assistant | 39 | 78.00% | 58 | 37.20% | 25.32 (<0.001) | 50 | 33.10% | 47 | 85.50% | 44.26 (<0.001) | 22 | 31.90% | 45 | 50.00% | 27 | 66.70% | 14.36 (<0.001) | |
| Performs microbiological test | 13 | 26.00% | 32 | 20.50% | ns | 33 | 21.90% | 12 | 21.80% | ns | 17 | 24.60% | 13 | 14.40% | 14 | 56.10% | 7.60 (0.022) | |
| Continuous water supply system to dental unit | 15 | 30.00% | 47 | 30.10% | ns | 41 | 27.20% | 21 | 38.20% | ns | 16 | 23.20% | 26 | 28.90% | 18 | 48.50% | 6.38 (0.041) | |
| Antiseptic to the handpieces (auto) | 6 | 13.60% | 11 | 8.00% | ns | 8 | 6.10% | 9 | 18.40% | 6.36 (0.012) | 8 | 14.00% | 3 | 3.80% | 6 | 16.10% | 6.21 (0.045) | |
| Antiseptic to the handpieces (manually) | 2 | 4.50% | 24 | 17.50% | 4.56 (0.033) | 19 | 14.40% | 7 | 14.30% | ns | 9 | 15.80% | 10 | 12.50% | 6 | 16.10% | ns | |
| Clean suctiotion Large Small | between two patients | 21 | 45.70% | 69 | 45.40% | ns | 63 | 44.10% | 27 | 49.10% | ns | 27 | 40.30% | 39 | 46.40% | 0 | 45.50% | 23.24 (0.010) |
| every few appointments | 3 | 6.50% | 27 | 17.80% | 24 | 16.80% | 6 | 10.90% | 13 | 19.40% | 9 | 10.70% | 1 | 18.20% | ||||
| per day | 13 | 28.30% | 40 | 26.30% | 38 | 26.60% | 15 | 27.30% | 13 | 19.40% | 30 | 35.70% | 5 | 15.20% | ||||
| per week or more | 9 | 19.5% | 16 | 10.6% | 18 | 12.6% | 7 | 12.7% | 14 | 20.9% | 6 | 7.2% | 6 | 12.1% | ||||
| between two patients | 4 | 8.50% | 11 | 7.40% | 11.64 (0.040) | 8 | 5.60% | 7 | 13.00% | ns | 6 | 9.10% | 3 | 3.60% | 8 | 6.10% | ns | |
| every few appointments | 3 | 6.40% | 21 | 14.10% | 14 | 9.90% | 10 | 18.50% | 9 | 13.60% | 12 | 14.30% | 1 | 9.10% | ||||
| per day | 24 | 51.10% | 60 | 40.30% | 61 | 43.00% | 23 | 42.60% | 20 | 30.30% | 38 | 45.20% | 0 | 63.60% | ||||
| per week or more | 16 | 34.00% | 57 | 38.30% | 59 | 41.50% | 14 | 25.90% | 31 | 47.00% | 31 | 37.00% | 8 | 38.00% | ||||
| Micromotors | 1 | 9 | 18.00% | 42 | 26.90% | ns | 46 | 30.50% | 5 | 9.10% | 31.40 (<0.001) | 23 | 33.30% | 20 | 22.20% | 15 | 18.20% | 24.39 (0.002) |
| 2 | 19 | 38.00% | 50 | 32.10% | 58 | 38.40% | 11 | 20.00% | 20 | 29.00% | 39 | 43.30% | 3 | 24.20% | ||||
| 3 | 5 | 10.00% | 19 | 12.20% | 16 | 10.60% | 8 | 14.50% | 9 | 13.00% | 12 | 13.30% | 11 | 9.10% | ||||
| 4 | 4 | 8.00% | 21 | 13.50% | 15 | 9.90% | 10 | 18.20% | 8 | 11.60% | 8 | 8.90% | 4 | 15.20% | ||||
| 5+ | 13 | 26.00% | 24 | 15.40% | 16 | 10.60% | 21 | 38.20% | 9 | 13.00% | 11 | 12.20% | 0 | 33.30% | ||||
| Airotors | 1 | 10 | 20.00% | 19 | 12.20% | ns | 24 | 15.90% | 5 | 9.10% | 22.04 (<0.001) | 13 | 18.80% | 13 | 14.40% | 2 | 6.10% | ns |
| 2 | 16 | 32.00% | 47 | 30.10% | 53 | 35.10% | 10 | 18.20% | 23 | 33.30% | 28 | 31.10% | 1 | 30.30% | ||||
| 3 | 6 | 12.00% | 21 | 13.50% | 23 | 15.20% | 4 | 7.30% | 9 | 13.00% | 15 | 16.70% | 14 | 3.00% | ||||
| 4 | 5 | 10.00% | 20 | 12.80% | 19 | 12.60% | 6 | 10.90% | 9 | 13.00% | 10 | 11.10% | 6 | 15.20% | ||||
| 5+ | 13 | 26.00% | 49 | 31.40% | 32 | 21.20% | 30 | 54.50% | 15 | 21.70% | 24 | 26.70% | 6 | 45.50% | ||||
| Has implantology motor | 17 | 34.70% | 60 | 38.50% | ns | 48 | 32.00% | 29 | 52.70% | 7.37 (0.007) | 28 | 41.20% | 28 | 31.10% | 0 | 45.50% | ns | |
| Has amalgam trap | 25 | 52.10% | 103 | 68.70% | 4.38 (0.038) | 90 | 62.50% | 38 | 70.40% | ns | 46 | 71.90% | 54 | 61.40% | 38 | 62.50% | ns | |
| Has contract for amalgam removal | 10 | 21.70% | 41 | 28.10% | ns | 32 | 22.70% | 19 | 37.30% | 4.07 (0.044) | 16 | 27.10% | 21 | 23.90% | 20 | 34.40% | ns | |
| Money Spent | <25 EUR/month | 11 | 22.00% | 33 | 21.20% | 37 | 24.50% | 7 | 12.70% | 21 | 30.40% | 18 | 20.00% | 5 | 12.10% | |||
| 25–50 EUR/month | 18 | 36.00% | 71 | 45.50% | 73 | 48.30% | 16 | 29.10% | 30 | 43.50% | 42 | 46.70% | 8 | 30.30% | ||||
| 50–75 EUR/month | 9 | 18.00% | 29 | 18.60% | 24 | 15.90% | 14 | 25.50% | 10 | 14.50% | 14 | 15.60% | 3 | 36.40% | ||||
| >75 EUR/month | 9 | 18.00% | 18 | 11.50% | 12 | 7.90% | 15 | 27.30% | 6 | 8.70% | 12 | 13.30% | 1 | 18.20% | ||||
| Implementation of disinfection protocol is my responsibility | 19 | 38.00% | 101 | 64.70% | 11.14 (<0.001) | 104 | 68.90% | 16 | 29.10% | 26.24 (<0.001) | 49 | 71.00% | 47 | 52.20% | 0 | 54.50% | 6.26 (0.044) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antoniadou, M.; Intzes, A.; Kladouchas, C.; Christou, I.; Chatzigeorgiou, S.; Plexida, M.; Stefanidakis, V.; Tzoutzas, I. Factors Affecting Water Quality and Sustainability in Dental Practices in Greece. Sustainability 2023, 15, 9115. https://doi.org/10.3390/su15119115
Antoniadou M, Intzes A, Kladouchas C, Christou I, Chatzigeorgiou S, Plexida M, Stefanidakis V, Tzoutzas I. Factors Affecting Water Quality and Sustainability in Dental Practices in Greece. Sustainability. 2023; 15(11):9115. https://doi.org/10.3390/su15119115
Chicago/Turabian StyleAntoniadou, Maria, Anestis Intzes, Christos Kladouchas, Iliana Christou, Stavroula Chatzigeorgiou, Martha Plexida, Valantis Stefanidakis, and Ioannis Tzoutzas. 2023. "Factors Affecting Water Quality and Sustainability in Dental Practices in Greece" Sustainability 15, no. 11: 9115. https://doi.org/10.3390/su15119115
APA StyleAntoniadou, M., Intzes, A., Kladouchas, C., Christou, I., Chatzigeorgiou, S., Plexida, M., Stefanidakis, V., & Tzoutzas, I. (2023). Factors Affecting Water Quality and Sustainability in Dental Practices in Greece. Sustainability, 15(11), 9115. https://doi.org/10.3390/su15119115