

The Robust Emergency Medical Facilities Location-Allocation Models under Uncertain Environment: A Hybrid Approach



Abstract
1. Introduction
2. The Framework and Preliminaries
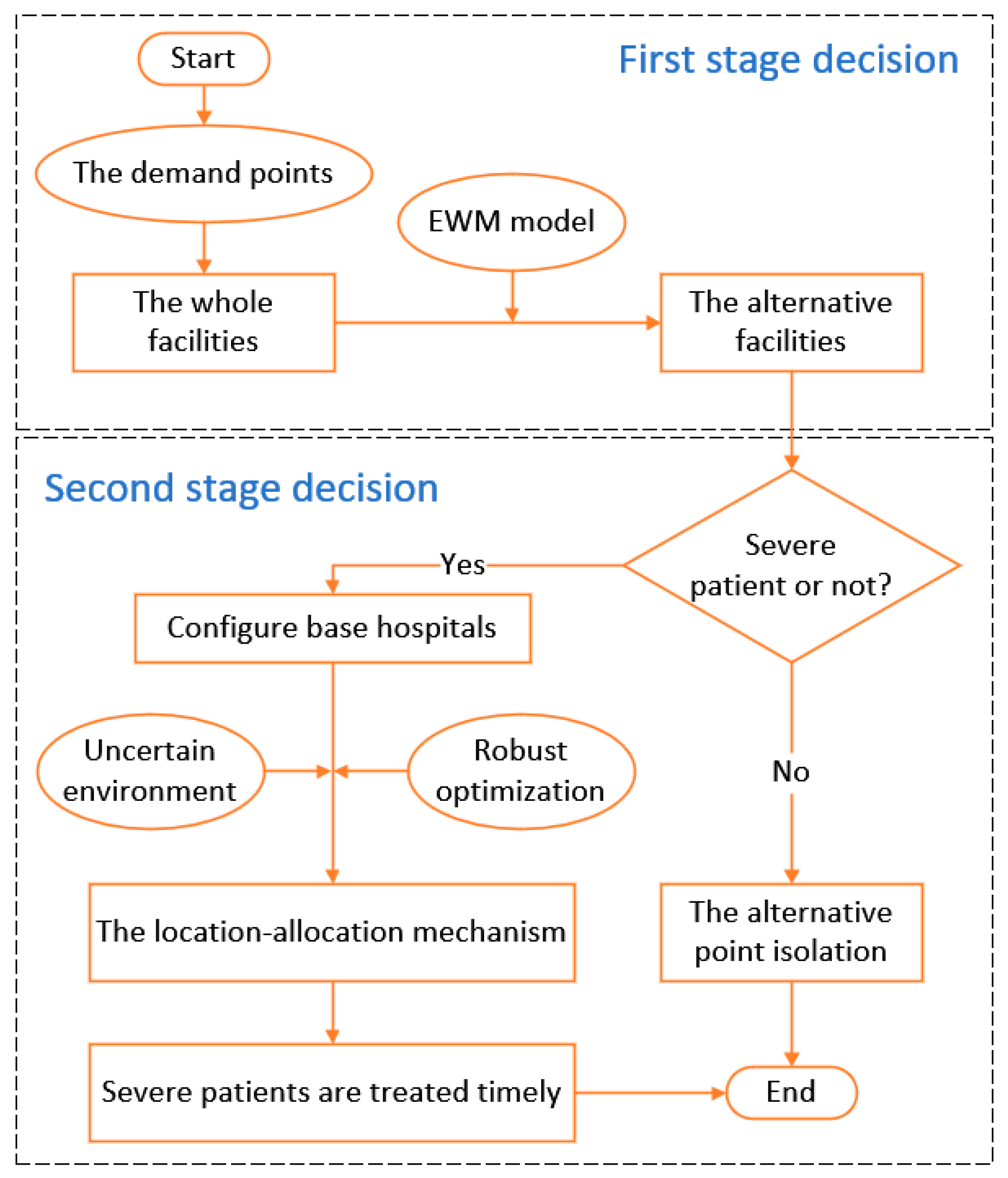
2.1. The Framewrok of This Paper
2.2. Assumptions and Notation
- The established emergency medical facilities can meet the medical needs of patients in the city, regardless of the situation of transferring patients to other cities.
- The radiation range of each facility is a small area, and the patients’ number, which they receive, is the sum of the patients’ number in the area.
- All critically ill patients are treated by large rear hospitals, which do not occupy the medical resources of the facility point. Additionally, the rear hospitals can meet the treatment needs of the assigned critically ill patients.
3. Emergencies Facilities Location Modeling
3.1. Emergency Medical Facilities Alternatives Selection Based on EWM
3.2. The Deterministic Model
3.3. The Robust Model
3.3.1. Budgeted Uncertainty Set
3.3.2. Box Uncertainty Set
3.3.3. Ellipsoid Uncertainty Set
4. Simulations
4.1. Background and Data Sources
4.2. The Alternative Facilities Selection Based on EWM
4.3. Robust Solution Process
4.4. Result Analysis
5. Conclusions
5.1. Discussions
5.2. Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, J.; Bai, J.Y.; Wu, D.S. Medical supplies scheduling in major public health emergencies. Transp. Res. Part E Logist. Transp. Rev. 2021, 154, 102464. [Google Scholar] [CrossRef]
- Xu, Y.; Li, J.; Liu, Y.W. Quantitative evaluation of provincial government plans for public health emergencies in China. Int. J. Disast. Risk Reduct. 2022, 81, 103292. [Google Scholar] [CrossRef]
- Alsafi, R.T. Lessons from SARS-CoV, MERS-CoV, and SARS-CoV-2 Infections: What We Know So Far. Can. J. Infect. Dis. Med. 2022, 2022, 1156273. [Google Scholar] [CrossRef] [PubMed]
- Hartt, M. COVID-19: A lonely pandemic. Cities Health 2021, 5, S80–S82. [Google Scholar] [CrossRef]
- Zhang, X.; Ding, Z.J.; Hang, J.Q.; He, Q.Z. How do stock price indices absorb the COVID-19 pandemic shocks? N. Am. J. Econ. Financ. 2022, 60, 101672. [Google Scholar] [CrossRef]
- Zhu, L.; Chen, P.L.; Dong, D.D.; Wang, Z.X. Can artificial intelligence enable the government to respond more effectively to major public health emergencies? Taking the prevention and control of Covid-19 in China as an example. Socio Econ. Plan. Sci. 2022, 80, 101029. [Google Scholar] [CrossRef]
- Liu, M.; Xu, X.F.; Cao, J.; Zhang, D. Integrated planning for public health emergencies: A modified model for controlling H1N1 pandemic. J. Oper. Res. Soc. 2020, 71, 748–761. [Google Scholar] [CrossRef]
- Zhang, L.; Zhao, W.J.; Sun, B.B.; Huang, Y.; Glänzel, W. How scientific research reacts to international public health emergencies: A global analysis of response patterns. Scientometrics 2020, 124, 747–773. [Google Scholar] [CrossRef]
- Jin, R.; Xia, T.; Liu, X.; Murata, T.; Kim, K.S. Predicting Emergency Medical Service Demand With Bipartite Graph Convolutional Networks. IEEE Access 2021, 9, 9903–9915. [Google Scholar] [CrossRef]
- Xu, Z.Q.; Cheng, Y.K.; Yao, S.L. Tripartite Evolutionary Game Model for Public Health Emergencies. Discrete Dyn. Nat. Soc. 2021, 2021, 6693597. [Google Scholar] [CrossRef]
- Tessema, F.S.; Koya, P.R.; Bole, B.K. Optimal Control and Cost-Effectiveness Analysis of Cholera with Vaccination. J. Math. 2022, 2022, 1705277. [Google Scholar] [CrossRef]
- Deng, X.C. Location-Routing Problem of Emergency Facilities under Uncertain Demand by Branch-Price and Cut. J. Math. 2021, 2021, 9152989. [Google Scholar] [CrossRef]
- Yang, N.; Shen, L.Y.; Shu, T.H.; Liao, S.J.; Peng, Y.; Wang, J.H. An integrative method for analyzing spatial accessibility in the hierarchical diagnosis and treatment system in China. Soc. Sci. Med. 2021, 270, 113656. [Google Scholar] [CrossRef] [PubMed]
- Schullerus, G.; Supavatanakul, P.; Krebs, V.; Lunze, J. Modelling and hierarchical diagnosis of timed discrete-event systems. Math. Comp. Model. Dyn. 2006, 12, 519–542. [Google Scholar] [CrossRef]
- Toregas, C.; Swain, R.; ReVelle, C.; Bergman, L. The Location of Emergency Service Facilities. Oper. Res. 1971, 19, 1363–1373. [Google Scholar] [CrossRef]
- He, Q.Z.; Tong, H.; Liu, J.B. How Does Inequality Affect the Residents’ Subjective Well-Being: Inequality of Opportunity and Inequality of Effort. Front. Psychol. 2022, 13, 843854. [Google Scholar] [CrossRef] [PubMed]
- Gigovic, L.; Pamucar, D.; Bozanic, D.; Ljubojevic, S. Application of the GIS-DANP-MABAC multi-criteria model for selecting the location of wind farms: A case study of Vojvodina, Serbia. Renew. Energ. 2017, 103, 501–521. [Google Scholar] [CrossRef]
- Biswas, S.; Pamucar, D. Facility Location Selection for B-Schools in Indian Context: A Multi-Criteria Group Decision Based Analysis. Axioms 2020, 9, 77. [Google Scholar] [CrossRef]
- Pamucar, D.; Gigovic, L.; Bajic, Z.; Janosevic, M. Location Selection for Wind Farms Using GIS Multi-Criteria Hybrid Model: An Approach Based on Fuzzy and Rough Numbers. Sustainability 2017, 9, 1315. [Google Scholar] [CrossRef]
- Boonmee, C.; Arimura, M.; Asada, T. Facility location optimization model for emergency humanitarian logistics. Int. J. Disast. Risk Reduct. 2017, 24, 485–498. [Google Scholar] [CrossRef]
- Zhang, H.Z.; Zhang, K.; Chen, Y.T.; Ma, L. Multi-objective two-level medical facility location problem and tabu search algorithm. Inf. Sci. 2022, 608, 734–756. [Google Scholar] [CrossRef]
- Liu, K.N. GIS-based MCDM framework combined with coupled multi-hazard assessment for site selection of post-earthquake emergency medical service facilities in Wenchuan, China. Int. J. Disast. Risk Reduct. 2022, 73, 102873. [Google Scholar] [CrossRef]
- Yücel, E.; Salman, F.S.; Bozkaya, B.; Gökalp, C. A data-driven optimization framework for routing mobile medical facilities. Ann. Oper. Res. 2020, 291, 1077–1102. [Google Scholar] [CrossRef]
- Zhen, L.; Wang, K.; Liu, H.C. Disaster Relief Facility Network Design in Metropolises. IEEE Trans. Syst. Man Cybern. Syst. 2015, 45, 751–761. [Google Scholar] [CrossRef]
- Ji, Y.; Li, H.H.; Zhang, H.J. Risk-Averse Two-Stage Stochastic Minimum Cost Consensus Models with Asymmetric Adjustment Cost. Group Decis. Negot. 2022, 31, 261–291. [Google Scholar] [CrossRef]
- Soyster, A.L. Technical Note—Convex Programming with Set-Inclusive Constraints and Applications to Inexact Linear Programming. Oper. Res. 1973, 21, 1154–1157. [Google Scholar] [CrossRef]
- Ben-Tal, A.; Nemirovski, A. Robust solutions of uncertain linear programs. Oper. Res. Lett. 1999, 88, 411–424. [Google Scholar] [CrossRef]
- Ben-Tal, A.; Nemirovski, A. Robust Convex Optimization. Math. Oper. Res. 1998, 23, 769–805. [Google Scholar] [CrossRef]
- Bertsimas, D.; Sim, M. Robust discrete optimization and network flows. Math. Program. 2003, 98, 49–71. [Google Scholar] [CrossRef]
- Bertsimas, D.; Sim, M. The Price of Robustness. Oper. Res. 2004, 52, 35–53. [Google Scholar] [CrossRef]
- Ji, Y.; Jin, X.W.; Xu, Z.S.; Qu, S.J. A mixed 0-1 programming approach for multiple attribute strategic weight manipulation based on uncertainty theory. J. Intell. Fuzzy Syst. 2021, 41, 6739–6754. [Google Scholar] [CrossRef]
- Qu, S.J.; Li, Y.M.; Ji, Y. The mixed integer robust maximum expert consensus models for large-scale GDM under uncertainty circumstances. Appl. Soft Comput. 2021, 107, 107369. [Google Scholar] [CrossRef]
- Zhang, H.J.; Ji, Y.; Qu, S.J.; Li, H.H.; Huang, R.P. The robust minimum cost consensus model with risk aversion. Inf. Sci. 2022, 587, 283–299. [Google Scholar] [CrossRef]
- Han, Y.; Qu, S.J.; Wu, Z.; Huang, R.P. Robust consensus models based on minimum cost with an application to marketing plan. J. Intell. Fuzzy Syst. 2019, 37, 5655–5668. [Google Scholar] [CrossRef]
- Li, C.N.; Guo, T.Y.; Chen, Y. Robust Emission Reduction Strategies under Cap-and-Trade and Demand Uncertainty. Sustainability 2022, 14, 13445. [Google Scholar] [CrossRef]
- Qu, S.J.; Wei, J.P.; Wang, Q.H.; Li, Y.M.; Jin, X.W.; Chaib, L. Robust minimum cost consensus models with various individual preference scenarios under unit adjustment cost uncertainty. Inf. Fusion 2023, 89, 510–526. [Google Scholar] [CrossRef]
- Huang, R.P.; Qu, S.J.; Yang, X.G.; Xu, F.M.; Xu, Z.S.; Zhou, W. Sparse portfolio selection with uncertain probability distribution. Appl. Intell. 2021, 51, 6665–6684. [Google Scholar] [CrossRef]
- Cacador, S.; Dias, J.M.; Godinho, P. Portfolio selection under uncertainty: A new methodology for computing relative-robust solutions. Int. T. Oper. Res. 2021, 28, 1296–1329. [Google Scholar] [CrossRef]
- Gubu, L.; Rosadi, D.; Abdurakhman. A New Approach for Robust Mean-Variance Portfolio Selection Using Trimmed k-Means Clustering. Ind. Eng. Manag. Syst. 2021, 20, 782–794. [Google Scholar] [CrossRef]
- Luan, D.Q.; Wang, C.M.; Wu, Z.; Xia, Z.J. Two-Stage Robust Optimization Model for Uncertainty Investment Portfolio Problems. J. Math. 2021, 2021, 3087066. [Google Scholar] [CrossRef]
- Xu, L.J.; Zhou, Y.J. New Robust Reward-Risk Ratio Models with CVaR and Standard Deviation. J. Math. 2022, 2022, 8304411. [Google Scholar] [CrossRef]
- Qu, S.J.; Xu, Y.T.; Ji, Y.; Feng, C.; Wei, J.P.; Jiang, S. Data-Driven Robust Data Envelopment Analysis for Evaluating the Carbon Emissions Efficiency of Provinces in China. Sustainability 2022, 14, 13318. [Google Scholar] [CrossRef]
- Qu, S.J.; Feng, C.; Jiang, S.; Wei, J.P.; Xu, Y.T. Data-Driven Robust DEA Models for Measuring Operational Efficiency of Endowment Insurance System of Different Provinces in China. Sustainability 2022, 14, 9954. [Google Scholar] [CrossRef]
- Ji, Y.; Du, J.H.; Han, X.Y.; Wu, X.Q.; Huang, R.P.; Wang, S.L.; Liu, Z.M. A mixed integer robust programming model for two-echelon inventory routing problem of perishable products. Physica A 2020, 548, 124481. [Google Scholar] [CrossRef]
- Liu, Z.M.; Qu, S.J.; Raza, H.; Wu, Z.; Qu, D.Q.; Du, J.H. Two-stage mean-risk stochastic mixed integer optimization model for location-allocation problems under uncertain environment. J. Ind. Manag. Optim. 2021, 17, 2783–2804. [Google Scholar] [CrossRef]
- Liu, H.R.; Qu, S.J.; Li, R.J.; Razaa, H. Bi-objective robust project scheduling with resource constraints and flexible activity execution lists. Comput. Ind. Eng. 2021, 156, 107288. [Google Scholar] [CrossRef]
- Kumar Tarei, P.; Kumar, G.; Ramkumar, M. A Mean-Variance robust model to minimize operational risk and supply chain cost under aleatory uncertainty: A real-life case application in petroleum supply chain. Comput. Ind. Eng. 2022, 166, 107949. [Google Scholar] [CrossRef]
- Savoji, H.; Mousavi, S.M.; Antucheviciene, J.; Pavlovskis, M. A Robust Possibilistic Bi-Objective Mixed Integer Model for Green Biofuel Supply Chain Design under Uncertain Conditions. Sustainability 2022, 14, 13675. [Google Scholar] [CrossRef]
- Kaoud, E.; Abdel-Aal, M.A.M.; Sakaguchi, T.; Uchiyama, N. Robust Optimization for a Bi-Objective Green Closed-Loop Supply Chain with Heterogeneous Transportation System and Presorting Consideration. Sustainability 2022, 14, 10281. [Google Scholar] [CrossRef]
- Sun, H.P.; Li, Y.C.; Zhang, J.H. Collaboration-based reliable optimal casualty evacuation network design for large-scale emergency preparedness. Socio. Econ. Plan. Sci. 2021, 81, 101192. [Google Scholar] [CrossRef]
- Zhang, J.H.; Liu, H.Y.; Yu, G.D.; Ruan, J.H.; Chan, F.T.S. A three-stage and multi-objective stochastic programming model to improve the sustainable rescue ability by considering secondary disasters in emergency logistics. Comput. Ind. Eng. 2019, 135, 1145–1154. [Google Scholar] [CrossRef]
- Zhang, Y.W.; Li, Z.P.; Jiao, P.B.; Zhu, S. Two-stage stochastic programming approach for limited medical reserves allocation under uncertainties. Complex Intell. Syst. 2021, 7, 3003–3013. [Google Scholar] [CrossRef]
- Jamali, A.; Ranjbar, A.; Heydari, J.; Nayeri, S. A multi-objective stochastic programming model to configure a sustainable humanitarian logistics considering deprivation cost and patient severity. Ann. Oper. Res. 2021, 2021, 1–35. [Google Scholar] [CrossRef]
- Yin, X.C.; Büyüktahtakın, İ.E. A multi-stage stochastic programming approach to epidemic resource allocation with equity considerations. Health Care Manag. Sci. 2021, 24, 597–622. [Google Scholar] [CrossRef]
- Zhang, Z.; Li, Z.L. Consensus-based TOPSIS-Sort-B for multi-criteria sorting in the context of group decision-making. Ann. Oper. Res. 2022, 2022, 1–28. [Google Scholar] [CrossRef]
- Gai, T.T.; Cao, M.S.; Chiclana, F.; Zhang, Z.; Dong, Y.C.; Herrera-Viedma, E.; Wu, J. Consensus-trust Driven Bidirectional Feedback Mechanism for Improving Consensus in Social Network Large-group Decision Making. Group Decis. Negot. 2022, 2022, 1–30. [Google Scholar] [CrossRef]
- Zhang, Z.; Li, Z.L. Personalized Individual Semantics-Based Consistency Control and Consensus Reaching in Linguistic Group Decision Making. IEEE Trans. Syst. Man Cybern. Syst. 2022, 52, 5623–5635. [Google Scholar] [CrossRef]
- Gao, Y.; Zhang, Z. Consensus reaching with non-cooperative behavior management for personalized individual semantics-based social network group decision making. J. Oper. Res. Soc. 2021, 2021, 1–18. [Google Scholar] [CrossRef]
- Pamucar, D.; Torkayesh, A.E.; Biswas, S. Supplier selection in healthcare supply chain management during the COVID-19 pandemic: A novel fuzzy rough decision-making approach. Ann. Oper. Res. 2022, 2022, 1–43. [Google Scholar] [CrossRef]
- Biswas, S.; Pamucar, D.; Bozanic, D.; Halder, B. A New Spherical Fuzzy LBWA-MULTIMOOSRAL Framework: Application in Evaluation of Leanness of MSMEs in India. Math. Probl. Eng. 2022, 5480848. [Google Scholar] [CrossRef]
- Qu, S.J.; Shu, L.L.; Yao, J.Y. Optimal pricing and service level in supply chain considering misreport behavior and fairness concern. Comput. Ind. Eng. 2022, 174, 108759. [Google Scholar] [CrossRef]
- Qu, S.J.; Xu, L.; Mangla, S.K.; Chan, F.T.S.; Zhu, J.L.; Arisian, S. Matchmaking in reward-based crowdfunding platforms: A hybrid machine learning approach. Int. J. Prod. Res. 2022, 2022, 1–21. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sets | |
| The collection of the whole emergency medical facilities (reconfigurable convention and exhibition centers, sports venues, schools), | |
| The collection of existing large rear hospitals (Grade II and above), | |
| The collection of patient types (mild, moderate, and severe three disease grades, represented by 1, 2, 3), | |
| Decision variables | |
| Parameters | |
| Number of emergency medical facilities opened. | |
| Operating cost of emergency medical facility point . | |
| Distance from facility point to hospital . | |
| Unit driving cost from facility point to hospital . | |
| Patients’ number of type at facility point . | |
| The proportion of type patients, respectively represents the severity level of patients. | |
| The maximum service capacity of large rear hospital . | |
| No. | Coordinate | Population | No. | Coordinate | Population | No. | Coordinate | Population |
|---|---|---|---|---|---|---|---|---|
| 1 | 114.66064,31.45983 | 80,798 | 44 | 115.65594,30.76541 | 19,731 | 87 | 115.69542,30.30748 | 50,072 |
| 2 | 114.60284,31.27431 | 119,425 | 45 | 115.63523,30.88881 | 22,065 | 88 | 115.85314,30.51451 | 30,936 |
| 3 | 114.49922,31.28993 | 39,658 | 46 | 115.75470,30.99033 | 32,412 | 89 | 115.82113,30.31645 | 36,759 |
| 4 | 114.55444,31.15556 | 50,883 | 47 | 115.90135,31.00211 | 18,108 | 90 | 115.56911,29.85114 | 161,582 |
| 5 | 114.56646,31.05605 | 32,145 | 48 | 115.75740,30.88672 | 32,279 | 91 | 115.56400,29.85043 | 34,026 |
| 6 | 114.44895,31.30736 | 35,447 | 49 | 115.76842,30.81582 | 42,325 | 92 | 115.42095,29.91312 | 18,948 |
| 7 | 114.64585,31.02003 | 30,639 | 50 | 115.61337,30.64183 | 25,045 | 93 | 115.70016,29.88795 | 4083 |
| 8 | 114.64488,30.96300 | 23,432 | 51 | 115.63833,30.83598 | 19,318 | 94 | 115.61056,30.11381 | 113,247 |
| 9 | 114.70241,31.14612 | 56,044 | 52 | 115.93407,30.90572 | 7477 | 95 | 115.73690,30.08317 | 50,297 |
| 10 | 114.53016,31.45716 | 43,804 | 53 | 114.86957,30.63203 | 71,185 | 96 | 115.71488,30.01275 | 64,690 |
| 11 | 114.64299,31.28841 | 86,479 | 54 | 114.88533,30.74325 | 57,183 | 97 | 115.62547,29.93993 | 44,857 |
| 12 | 114.66770,31.38754 | 2049 | 55 | 115.07828,30.69643 | 24,063 | 98 | 115.61438,29.99534 | 35,921 |
| 13 | 114.99998,31.16661 | 55,601 | 56 | 115.19036,30.76037 | 41,226 | 99 | 115.55408,30.02849 | 32,203 |
| 14 | 115.02587,31.18524 | 68,485 | 57 | 115.09952,30.64720 | 29,827 | 100 | 115.47552,29.94930 | 47,311 |
| 15 | 115.04128,31.17716 | 80,722 | 58 | 115.02658,30.65196 | 19,640 | 101 | 115.70678,29.86632 | 37,082 |
| 16 | 114.80704,31.06828 | 50,109 | 59 | 114.98275,30.60512 | 32,134 | 102 | 115.93927,30.07392 | 141,488 |
| 17 | 115.12917,31.20715 | 31,297 | 60 | 115.08718,30.79427 | 19,117 | 103 | 115.92131,29.88258 | 98,543 |
| 18 | 115.01422,31.03803 | 61,839 | 61 | 115.05516,30.79163 | 18,816 | 104 | 115.98622,29.75636 | 97,956 |
| 19 | 114.88605,31.12271 | 42,918 | 62 | 114.93149,30.67896 | 22,811 | 105 | 116.00873,30.05003 | 21,945 |
| 20 | 114.98878,31.35650 | 47,632 | 63 | 115.26651,30.43888 | 193,988 | 106 | 115.84793,30.08979 | 59,759 |
| 21 | 115.09380,31.47408 | 36,169 | 64 | 115.02802,30.42591 | 113,356 | 107 | 115.98671,30.21229 | 33,323 |
| 22 | 115.18852,31.07276 | 36,567 | 65 | 115.34092,30.55166 | 71,852 | 108 | 115.94173,30.17009 | 13,971 |
| 23 | 115.17771,30.96000 | 32,079 | 66 | 115.12536,30.59354 | 66,860 | 109 | 115.89000,30.00755 | 65,122 |
| 24 | 115.31886,31.04682 | 37,066 | 67 | 115.17918,30.61747 | 49,785 | 110 | 115.80776,29.87894 | 71,168 |
| 25 | 115.23286,31.32758 | 40,083 | 68 | 115.23300,30.72709 | 78,925 | 111 | 115.82248,29.81693 | 55,883 |
| 26 | 115.07628,31.37152 | 34,513 | 69 | 115.44597,30.59109 | 14,885 | 112 | 116.03935,30.07820 | 27,127 |
| 27 | 114.83977,31.33245 | 43,233 | 70 | 115.41237,30.56442 | 35,562 | 113 | 115.90764,29.78591 | 47,872 |
| 28 | 114.75598,31.01214 | 20,520 | 71 | 115.47997,30.46645 | 49,312 | 114 | 115.95513,30.27099 | 12,357 |
| 29 | 115.03054,30.96647 | 26,470 | 72 | 115.27209,30.38250 | 35,922 | 115 | 115.98193,30.10304 | 34,299 |
| 30 | 115.37487,31.18694 | 37,992 | 73 | 115.11897,30.23280 | 60,655 | 116 | 115.90153,30.13119 | 27,634 |
| 31 | 114.84998,31.03664 | 40,457 | 74 | 115.14533,30.35013 | 48,792 | 117 | 116.10982,29.83206 | 15,919 |
| 32 | 115.27363,30.83227 | 57,980 | 75 | 115.53676,30.52150 | 22,214 | 118 | 114.88374,30.44167 | 156,011 |
| 33 | 115.46262,31.12651 | 59,219 | 76 | 115.44136,30.25094 | 150,600 | 119 | 114.90441,30.47002 | 21,939 |
| 34 | 115.67112,31.14024 | 30,041 | 77 | 115.33968,30.07489 | 67,040 | 120 | 114.88198,30.47291 | 22,977 |
| 35 | 115.60163,31.00290 | 29,204 | 78 | 115.38161,30.30637 | 68,543 | 121 | 114.97287,30.45216 | 16,593 |
| 36 | 115.47994,30.84096 | 30,825 | 79 | 115.50228,30.36850 | 30,920 | 122 | 114.94966,30.48861 | 21,550 |
| 37 | 115.19510,30.81844 | 35,918 | 80 | 115.61687,30.38513 | 42,447 | 123 | 114.91279,30.54566 | 25,416 |
| 38 | 115.39093,30.98976 | 50,823 | 81 | 115.79129,30.41924 | 42,065 | 124 | 115.03657,30.59585 | 25,856 |
| 39 | 115.55835,30.69722 | 59,270 | 82 | 115.80244,30.49354 | 19,624 | 125 | 114.98103,30.53740 | 19,654 |
| 40 | 115.40694,30.68214 | 33,132 | 83 | 115.42998,30.20307 | 49,666 | 126 | 115.00178,30.58077 | 4753 |
| 41 | 115.39610,30.78371 | 114,890 | 84 | 115.28774,30.14920 | 20,547 | 127 | 114.91652,30.44885 | 52,020 |
| 42 | 115.67654,30.74001 | 121,669 | 85 | 115.28122,30.27222 | 35,569 | |||
| 43 | 115.61889,30.59068 | 16,027 | 86 | 115.58902,30.29642 | 67,756 |
| No. | Coordinate | Capacity | Attraction Factor | No. | Coordinate | Capacity | Attraction Factor |
|---|---|---|---|---|---|---|---|
| 1 | 114.63284,31.31431 | 27,840 | 1.3 | 16 | 114.89070,30.64937 | 4478 | 1.3 |
| 2 | 115.00939,31.16563 | 17,043 | 1.2 | 17 | 115.70328,30.81313 | 90,032 | 1.1 |
| 3 | 114.73256,31.10384 | 9100 | 1.1 | 18 | 114.95961,30.52801 | 29,708 | 1.2 |
| 4 | 115.95857,30.09049 | 118,450 | 1 | 19 | 115.41705,30.79636 | 49,879 | 1.3 |
| 5 | 115.55704,30.00018 | 6998 | 1.2 | 20 | 115.78056,30.90014 | 5282 | 1.2 |
| 6 | 115.10718,31.31427 | 10,989 | 1.4 | 21 | 115.38103,30.49740 | 73,502 | 1 |
| 7 | 114.62315,31.29476 | 104,917 | 1.1 | 22 | 115.20200,30.48535 | 8220 | 1.1 |
| 8 | 114.93146,30.62063 | 73,426 | 1.2 | 23 | 115.62718,30.00019 | 64,520 | 1.1 |
| 9 | 115.08277,30.23464 | 30,964 | 1.3 | 24 | 114.98103,30.53740 | 7598 | 1.2 |
| 10 | 115.02813,31.18019 | 35,097 | 1.1 | 25 | 115.05760,30.52585 | 45,008 | 1.4 |
| 11 | 115.93927,30.11392 | 9320 | 1 | 26 | 115.02813,31.18019 | 2890 | 1 |
| 12 | 115.01814,31.17779 | 3233 | 1.2 | 27 | 115.09380,30.96408 | 5354 | 1.1 |
| 13 | 114.90714,30.43954 | 52,560 | 1.1 | 28 | 115.41122,30.23686 | 6210 | 1.2 |
| 14 | 115.16036,30.64037 | 39,088 | 1 | 29 | 114.89070,30.64937 | 10,879 | 1.2 |
| 15 | 115.43629,30.23262 | 8352 | 1.4 | 30 | 115.55681,29.85051 | 4877 | 1.1 |
| No. | Coordinate | Number of Beds | No. | Coordinate | Number of Beds |
|---|---|---|---|---|---|
| 1 | 114.62522,31.28687 | 810 | 5 | 114.89880,30.47378 | 600 |
| 2 | 115.03035,31.18547 | 560 | 6 | 115.59644,29.87249 | 400 |
| 3 | 115.66802,30.73284 | 780 | 7 | 115.95089,30.08262 | 350 |
| 4 | 114.88141,30.45194 | 1050 |
| Region | Number of Patients | Region | Number of Patients |
|---|---|---|---|
| Huangzhou District | 968 | Xishui County | 303 |
| Tuanfeng County | 173 | Qichun County | 265 |
| Hongan County | 316 | Huangmei County | 284 |
| Luotian County | 69 | Macheng County | 243 |
| Yingshan County | 62 | Wuxue County | 224 |
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| Information entropy εj | 0.86431 | 0.96559 | 0.83973 | 0.95249 | 0.91932 | 0.94877 |
| Entropy weight wj | 0.26617 | 0.06749 | 0.31439 | 0.09319 | 0.15826 | 0.10049 |
| Facility Points | Large Base Rear Hospital | ||||||
|---|---|---|---|---|---|---|---|
| 199.1641 | 319.1826 | 235.1414 | 505.2721 | 626.4589 | 281.9618 | 8.558354 | |
| 0.906985 | 93.74792 | 395.6967 | 392.0141 | 481.4094 | 1149.629 | 1399.142 | |
| 81.52122 | 127.5054 | 248.5002 | 78.25099 | 46.62485 | 667.7027 | 897.0696 | |
| 46.33759 | 1.272584 | 260.4087 | 330.3708 | 399.213 | 951.1418 | 1115.944 | |
| 99.2809 | 168.108 | 271.98 | 12.69828 | 19.58887 | 595.4059 | 858.4737 | |
| 93.30548 | 124.6055 | 172.1071 | 149.7007 | 72.38121 | 589.0629 | 752.9345 | |
| 130.9173 | 171.0052 | 29.24747 | 399.2292 | 485.3551 | 631.5039 | 600.2825 | |
| 103.5559 | 121.9797 | 86.34575 | 283.1968 | 339.3343 | 627.7912 | 693.6411 | |
| 121.5096 | 171.719 | 63.80801 | 223.1036 | 268.3869 | 440.9306 | 548.5269 | |
| 181.3071 | 295.079 | 244.7432 | 387.752 | 482.9592 | 87.61668 | 259.9675 | |
| Γ | Disturbance in Proportion | |||
|---|---|---|---|---|
| 2% | 5% | 10% | 20% | |
| 0 | 4-7,7-1,8-5,10-2,13-4,14-5,17-3,19-3,21-3,23-6 | 4-7,7-1,8-5,10-2,13-4,14-5,17-3,19-3,21-3,23-6 | 4-7,7-1,8-5,10-2,13-4,14-5,17-3,19-3,21-3,23-6 | 4-7,7-1,8-5,10-2,13-4,14-5,17-3,19-3,21-3,23-6 |
| 2 | 4-7,7-1,8-5,10-2,13-4,14-5,17-3,19-3,21-5,23-6 | 4-7,7-1,8-5,10-2,13-4,14-5,17-3,19-3,21-5,23-6 | 4-7,7-1,8-4,10-2,13-5,14-5,17-3,19-3,21-5,23-6 | 4-7,7-1,8-4,10-2,13-5,14-5,17-3,19-3,21-5,23-6 |
| 4 | 4-7,7-1,8-5,10-2,13-4,14-5,17-3,19-3,21-5,23-6 | 4-7,7-1,8-5,10-2,13-4,14-5,17-3,19-3,21-5,23-6 | 4-7,7-1,8-4,10-2,13-5,14-5,17-3,19-3,21-5,23-6 | 4-7,7-1,8-4,10-2,13-5,14-4,17-3,19-2,21-5,23-6 |
| 6 | 4-7,7-1,8-4,10-2,13-5,14-5,17-3,19-3,21-5,23-6 | 4-7,7-1,8-4,10-2,13-5,14-5,17-3,19-3,21-5,23-6 | 4-7,7-1,8-4,10-2,13-5,14-4,17-3,19-2,21-5,23-6 | 4-7,7-1,8-4,10-2,13-5,14-4,17-3,19-2,21-5,23-6 |
| 8 | 4-7,7-1,8-4,10-2,13-5,14-4,17-3,19-2,21-5,23-6 | 4-7,7-1,8-4,10-2,13-5,14-4,17-3,19-2,21-5,23-6 | 4-7,7-1,8-4,10-2,13-5,14-4,17-3,19-2,21-5,23-7 | 4-7,7-1,8-4,10-2,13-5,14-4,17-3,19-2,21-5,23-7 |
| 10 | 4-7,7-1,8-4,10-2,13-5,14-4,17-3,19-2,21-5,23-6 | 4-7,7-1,8-4,10-2,13-5,14-4,17-3,19-2,21-5,23-7 | 4-7,7-1,8-4,10-2,13-5,14-4,17-3,19-2,21-5,23-7 | 4-7,7-1,8-4,10-2,13-5,14-4,17-3,19-2,21-5,23-7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, F.; Yan, M.; Wang, L.; Qu, S. The Robust Emergency Medical Facilities Location-Allocation Models under Uncertain Environment: A Hybrid Approach. Sustainability 2023, 15, 624. https://doi.org/10.3390/su15010624
Xu F, Yan M, Wang L, Qu S. The Robust Emergency Medical Facilities Location-Allocation Models under Uncertain Environment: A Hybrid Approach. Sustainability. 2023; 15(1):624. https://doi.org/10.3390/su15010624
Chicago/Turabian StyleXu, Fang, Mengfan Yan, Lun Wang, and Shaojian Qu. 2023. "The Robust Emergency Medical Facilities Location-Allocation Models under Uncertain Environment: A Hybrid Approach" Sustainability 15, no. 1: 624. https://doi.org/10.3390/su15010624
APA StyleXu, F., Yan, M., Wang, L., & Qu, S. (2023). The Robust Emergency Medical Facilities Location-Allocation Models under Uncertain Environment: A Hybrid Approach. Sustainability, 15(1), 624. https://doi.org/10.3390/su15010624