
Women’s Perceptions and Attitudes to Household Air Pollution Exposure and Capability to Change Cooking Behaviours in Urban Rwanda

 ,
,  ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
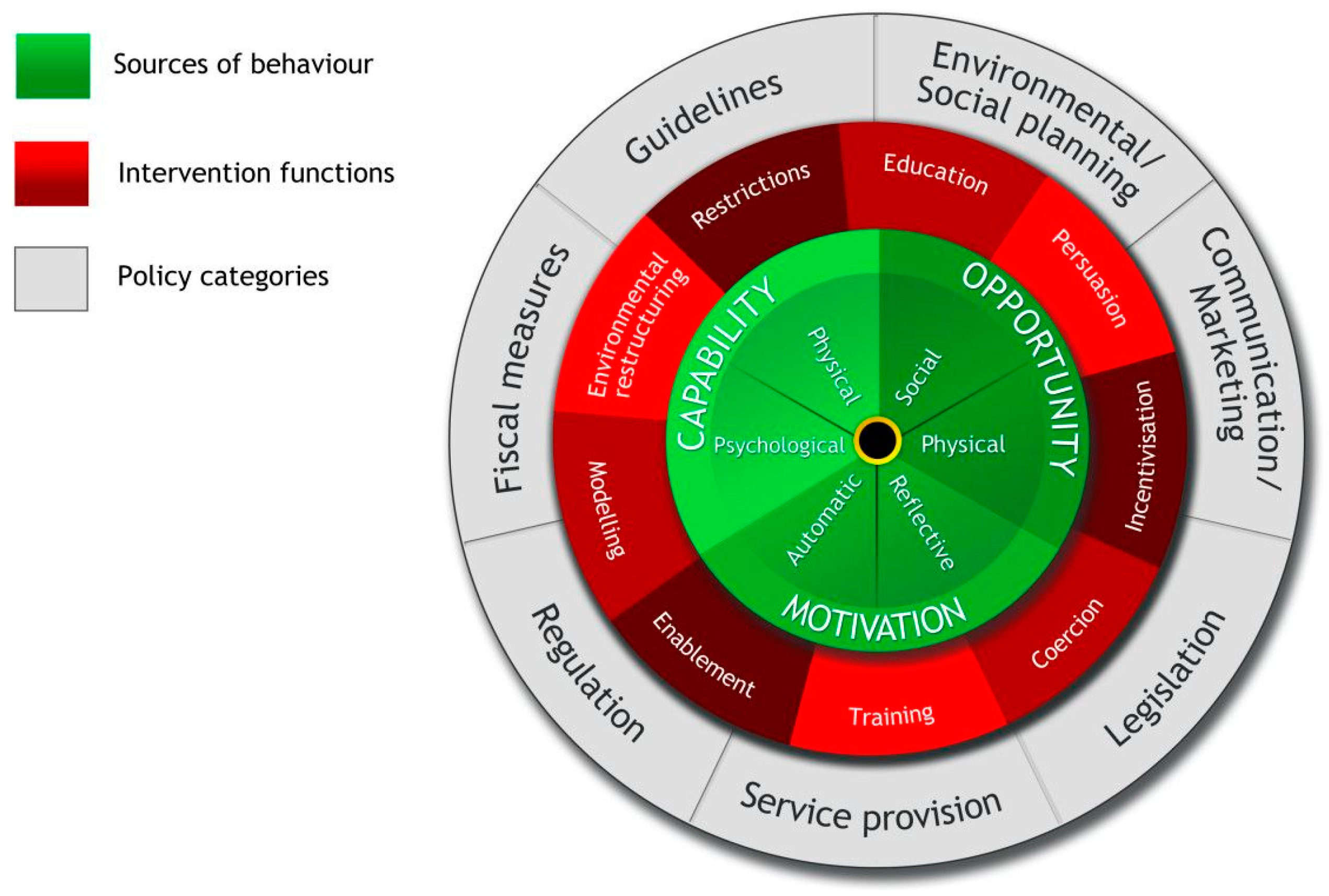
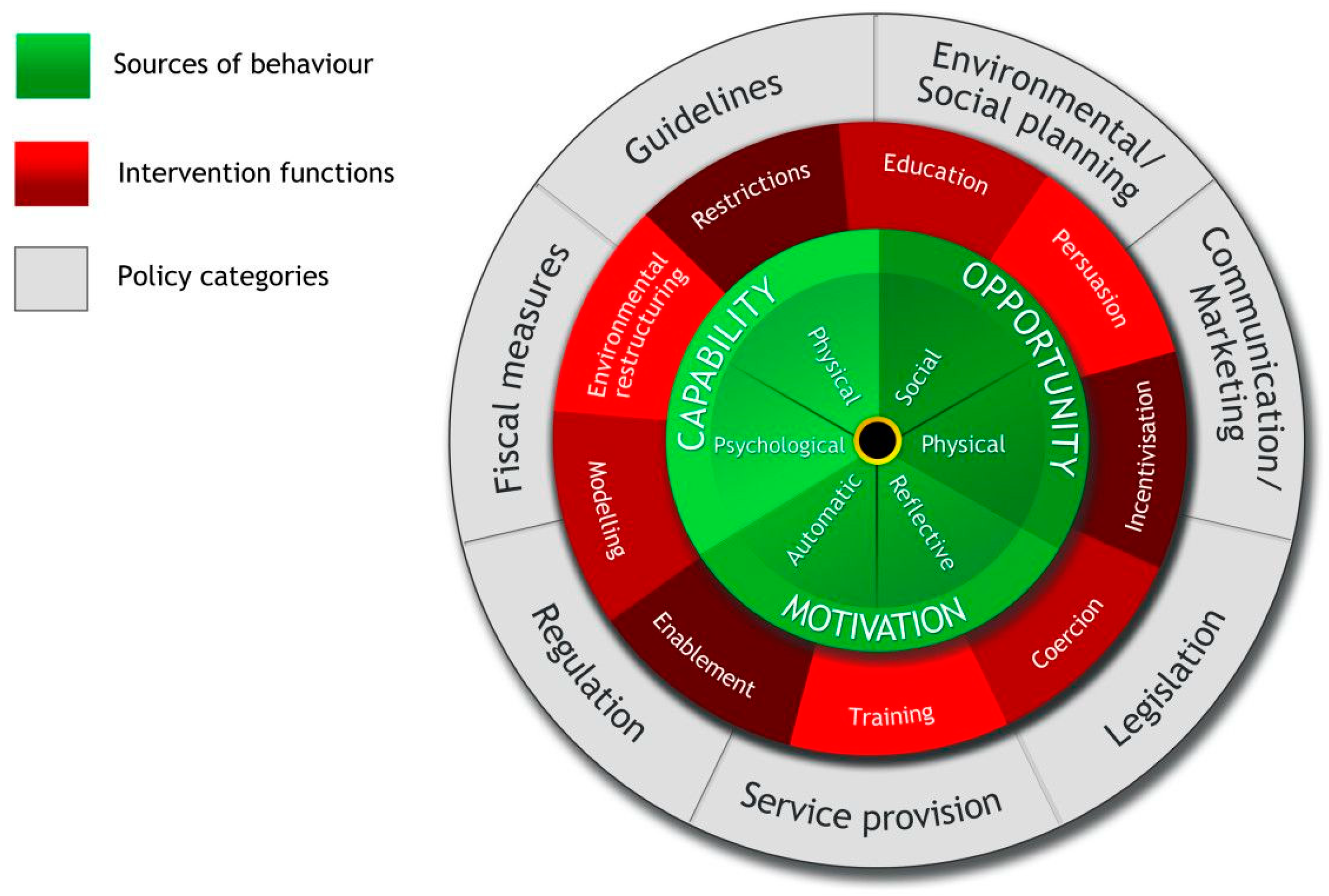
2.1. Theoretical Grounding
2.2. Study Setting
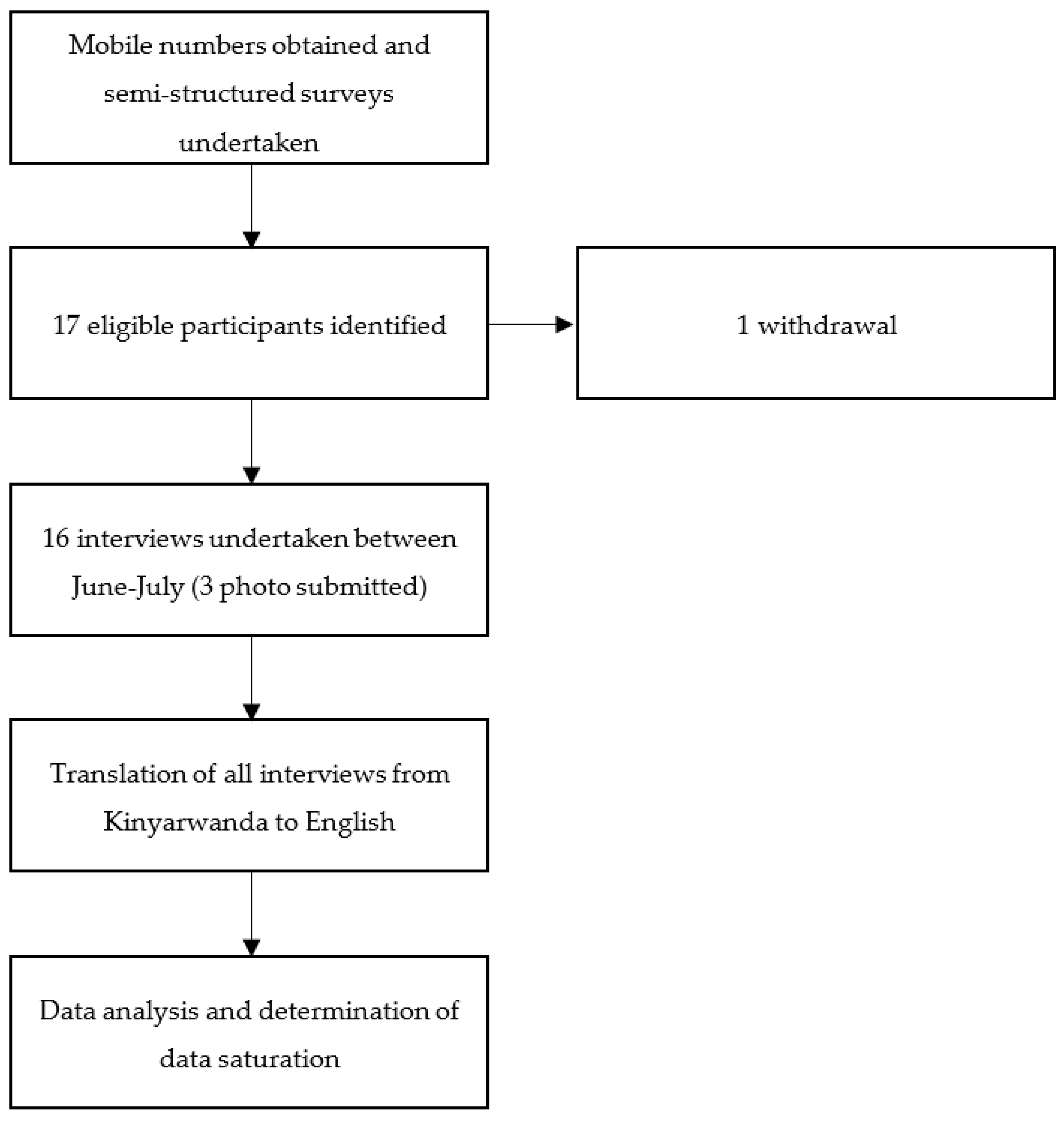
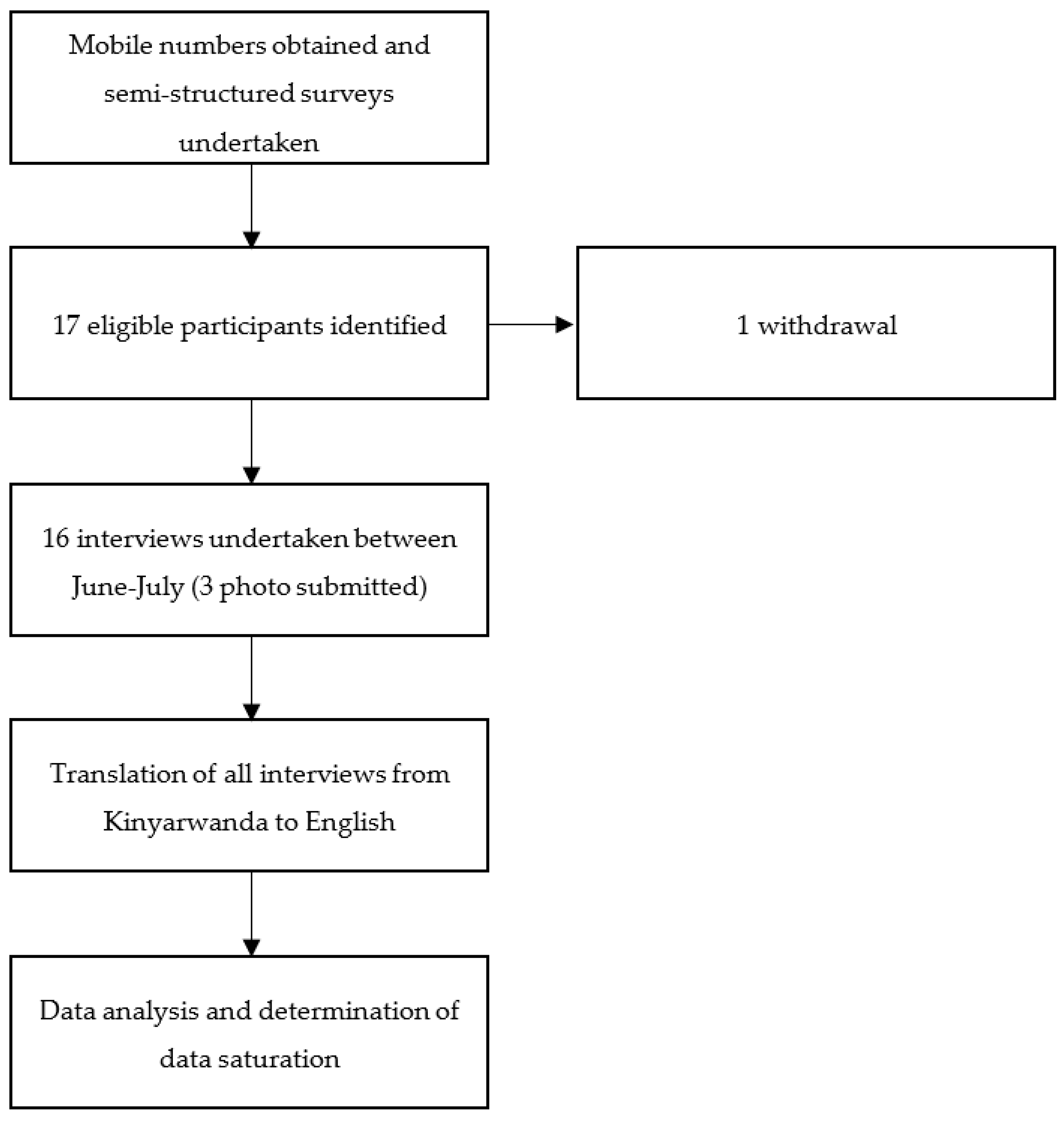
2.3. In-Depth Interviews
2.4. Data Analysis
2.5. Ethical Approval
3. Results
3.1. Participant Characteristics
3.2. Capability
Participant 9: “Smoke from cooking wood pollutes the air”
Participant 11: “The first thing is the smoke from the grass they burn. The second thing is the charcoal we burn and what we use to start the fire, like the plastic bags. The third thing is the cars that use petrol, I don’t know, they emit gases that pollute the air we breathe”
Participant 13: “Sometimes I bend down to fetch food from the pot or turn the food, and then the smoke rises in my face causing dizziness, tears, and mucus to run from the nose, and it becomes clear that the smoke is causing issues”
Participant 11: “I have a child among mine who suffers sinusitis, but that [smoke] wasn’t the cause”
Participant 3: “For me it takes time to be contaminated but the child not”
Participant 15: “What I can tell you now is that I now have a sick child at the hospital with breathing difficulties. I don’t know if it is because of the smokes”
Participant 6: “The reason is that if I cook from outside the children, who are playing, can be burnt. That’s why I don’t cook from outside”
Participant 13: “The method that could help me would be to find something that doesn’t emit smoke or excessive heat, so that I can start cooking inside the house. Because cooking outside the house isn’t a good practice. Sometimes dirt does fall into the pot, and it’s also possible that bad people might come and add dangerous stuff to the food and endanger the whole family. Cooking outside is good in terms of preventing smoke but it’s not generally a great thing”
Participant 5: “It is the security of the house, because you have a place to cook from and prepare things”
Participant 3: “No, where I cook is not where I want to cook, this is because of the lack of capacity. Because if I had the means, or if I was the owner of the house because I am the tenant, I should build for the gas in the right place and to cook there. This kitchen also, I will move it away from the door. In short, it’s the lack of means that forces me to cook where I cook today”
Participant 10: “The first thing is that I can’t carry gas and place it outside”
Participant 1: “It is the problem of high price. Gas is expensive and to find it is also expensive because they sell a big gas bottle, there is no small bottle with fewer kilograms”
Participant 1: “The suggestion is that the government would help us and reduce these gas prices and set up a way for one to go and put in a little gas he can afford, as we do when we buy a bucket of charcoal”
Participant 13: “There haven’t been any consequences except that when I am going to cook, I keep them at a distance and I tell their older sibling to keep them away so they don’t risk getting burned or spill something hot on themselves. So, there have been no consequences, because they don’t come near the fire”
Participant 12: “You can’t be able to keep children away when you are cooking”
3.3. Opportunity
Participant 8: “So, when it rains, in the case of us who are renting houses without a kitchen, we who are poor, you just move the cooking stoves into the house when it rains”
Participant 15: “Cooking from outside, some time there is wind or charcoal are burnt quickly, but I do it to protect myself from the smokes of the stove. Because I had problems when I placed it, I cannot do it again”
Participant 7: “But if you have the ability you can build the one with an open space, to reduce the disease you can cook from outside. It is good”
Participant 3: “So when a person is sick, or physically damaged in that way, that person cannot work for development, because he is always sick and always at the doctor. And the money he had, it will be used to treat his illness”
Participant 16: “It can be better while government help its citizens to have access to Liquid Petroleum Gas”
Participant 13: “Yes, I feel like I want to know more about this issue, the danger of it, and how one can protect oneself from it, and the ultimate consequences that it leads to”
Participant 7: “Talks on the radio, some may not have TV but many listens to the radio”
Participant 16: “I also like to use telephone too, because it can be on radio while I am not around, so that can be lost”
3.4. Motivation
Participant 7: “Yes, we switched to charcoals, now I won’t try any other thing”
Participant 12: “Cooking outside shouldn’t be happening, people should be cooking in kitchens”
Participant 11: “Because it allows the smokes to get away and avoid polluting the house and disturb children”
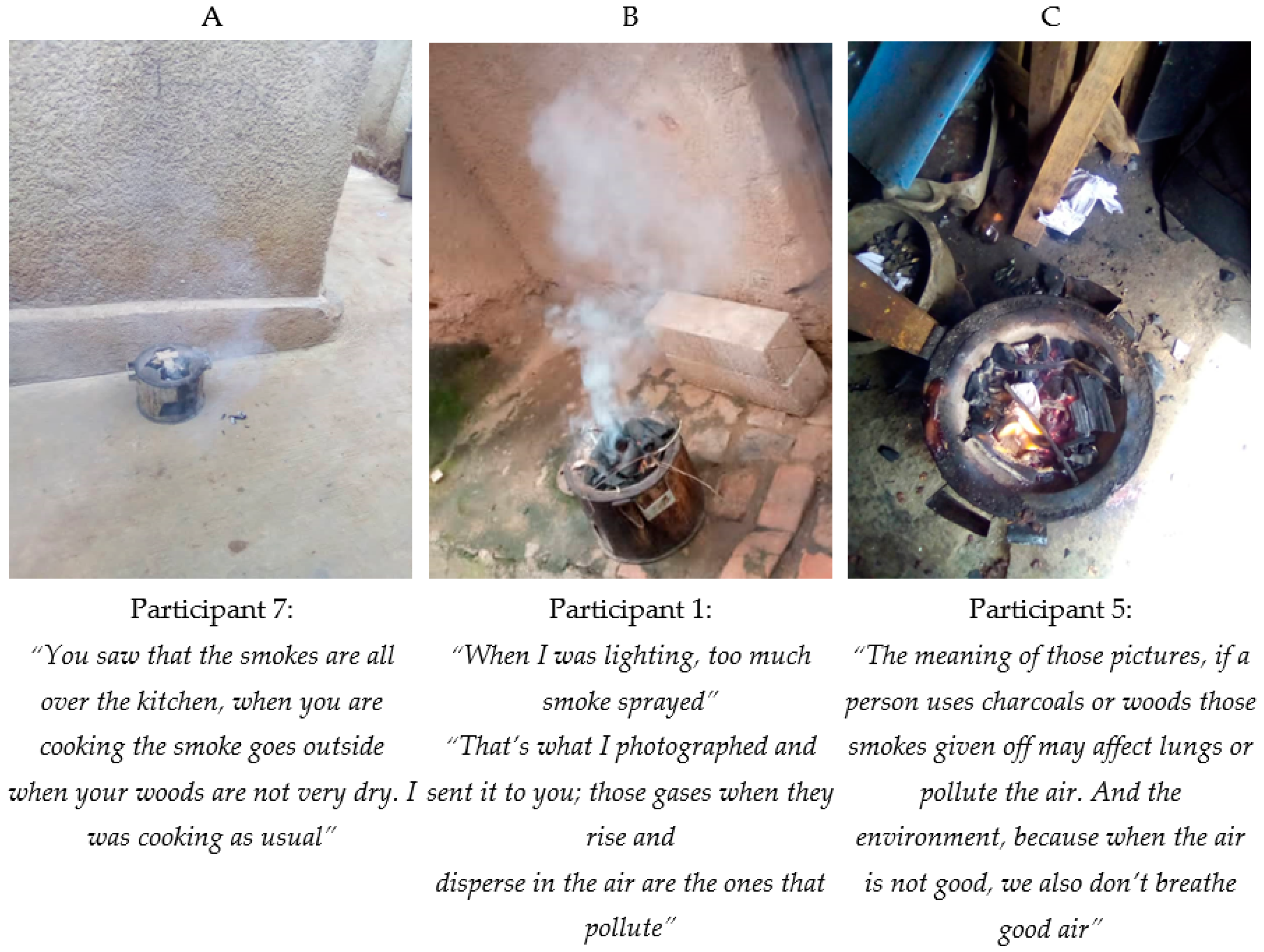
Participant 7: “When you start a fire the smoke spread all over and reach the neighbour”
Participant 12: “Cooking outside is difficult, it’s not easy. And it spreads smokes that pollute the atmosphere”
Participant 13: “Because cooking outside the house isn’t a good practice. Sometimes dirt does fall into the pot, and it’s also possible that bad people might come and add dangerous stuff to the food and endanger the whole family. Cooking outside is good in terms of preventing smoke but it’s not generally a great thing”
Participant 14: “Cooking on gas generates bad smoke in the house”
Participant 16: “lack of experience of using Liquid Petroleum Gas for cooking”
Participant 13: “The reason why I cook outside is that when you place the cooking stove on the house’s cemented floor, the fire burns quickly. And it could be possible that smoke can cloud the entire house and prevent you from breathing, causing you to cry and to drip mucus and sneeze a lot. It might also cause death to people, depending on who has a low tolerance to smoke, and that person might suffer consequences. That’s why I stopped cooking in the house and decided to cook outside. However, after realising that lesson, I started taking care of the situation, so it doesn’t lead to problems anymore”
3.5. Summary of Barriers and Facilitators
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Household Air Pollution and Health: Fact Sheet. Available online: http://www.who.int/news-room/fact-sheets/detail/household-air-pollution-and-health (accessed on 19 November 2018).
- Amegah, A.K.; Quansah, R.; Jaakkola, J.J.K. Household air pollution from solid fuel use and risk of adverse pregnancy outcomes: A systematic review and meta-analysis of the empirical evidence. PLoS ONE 2014, 9, e113920. [Google Scholar] [CrossRef] [PubMed]
- Kurmi, O.P.; Semple, S.; Simkhada, P.; Cairns S Smith, W.; Ayres, J.G. COPD and chronic bronchitis risk of indoor air pollution from solid fuel: A systematic review and meta-analysis. Thorax 2010, 65, 221–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thakur, M.; Nuyts, P.W.A.W.; Boudewijns, E.A.; Kim, J.F.; Faber, T.; Babu, G.R.; van Schayck, O.C.P.; Been, J.V. Impact of improved cookstoves on women’s and child health in low and middle income countries: A systematic review and meta-analysis. Thorax 2018, 73, 1026–1040. [Google Scholar] [CrossRef] [PubMed]
- Saenz, J.L.; Adar, S.D.; Zhang, Y.S.; Wilkens, J.; Chattopadhyay, A.; Lee, J.; Wong, R. Solid cooking fuel use and cognitive decline among older Mexican adults. Indoor Air 2021, 156, 1522–1532. [Google Scholar] [CrossRef]
- Bailis, R.; Drigo, R.; Ghilardi, A.; Masera, O. The carbon footprint of traditional woodfuels. Nat. Clim. Chang. 2015, 5, 266–272. [Google Scholar] [CrossRef]
- Vos, J.; Vis, M. Making Charcoal Production in Sub Sahara Africa Sustainable. Available online: https://english.rvo.nl/sites/default/files/2013/12/ReportCharcoal-BTG-NPSB_0.pdf (accessed on 15 April 2021).
- Okello, G.; Devereux, G.; Semple, S. Women and girls in resource poor countries experience much greater exposure to household air pollutants than men: Results from Uganda and Ethiopia. Environ. Int. 2018, 119, 429–437. [Google Scholar] [CrossRef]
- Muller, C.; Yan, H. Household fuel use in developing countries: Review of theory and evidence. Energy Econ. J. 2016, 70, 429–439. [Google Scholar] [CrossRef] [Green Version]
- Masera, O.R.; Saatkamp, B.D.; Kammen, D.M. From linear fuel switching to multiple cooking strategies: A critique and alternative to the energy ladder model. World Dev. 2000, 28, 2083–2103. [Google Scholar] [CrossRef]
- Puzzolo, E.; Stanistreet, D.; Pope, D.; Bruce, N.; Rehfuess, E. Factors Influencing the Large-Scale Uptake by Households of Cleaner and More Efficient Household Energy Technologies; EPPI-Centre, Social Science Research Unit, Institute of Education, University of London: London, UK, 2013. [Google Scholar]
- Nsamba, H.; Ssali, R.; Ssali, S.N.; Matovu, F.; Wasswa, J.; Balimunsi, H.K. Evaluation of the cooking cultures and practices in rural Uganda. J. Sustain. Bio-Energy Syst. 2021, 11, 33–44. [Google Scholar] [CrossRef]
- Ravindra, K.; Kaur-Sidhu, M.; Mor, S.; Chakma, J.; Pillarisetti, A. Impact of the COVID-19 pandemic on clean fuel programmes in India and ensuring sustainability for household energy needs. Environ. Int. 2021, 147, 106335. [Google Scholar] [CrossRef]
- Ardrey, J.; Jehan, K.; Desmond, N.; Kumbuyo, C.; Mortimer, K.; Tolhurst, R. ‘Cooking is for everyone?’: Exploring the complexity of gendered dynamics in a cookstove intervention study in rural Malawi. Glob. Health Action 2021, 14, 2006425. [Google Scholar] [CrossRef] [PubMed]
- Pope, D.; Bruce, N.; Dherani, M.; Jagoe, K.; Rehfuess, E. Real-life effectiveness of ‘improved’ stoves and clean fuels in reducing PM 2.5 and CO: Systematic review and meta-analysis. Environ. Int. 2017, 101, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Puzzolo, E.; Pope, D.; Stanistreet, D.; Rehfuess, E.A.; Bruce, N.G. Clean fuels for resource-poor settings: A systematic review of barriers and enablers to adoption and sustained use. Environ. Res. 2016, 146, 218–234. [Google Scholar] [CrossRef] [PubMed]
- Hollada, J.; Williams, K.N.; Miele, C.H.; Danz, D.; Harvey, S.A.; Checkley, W.; Hollada, J.; Williams, K.N.; Miele, C.H.; Danz, D.; et al. Perceptions of improved biomass and liquefied petroleum gas stoves in Puno, Peru: Implications for promoting sustained and exclusive adoption of clean cooking technologies. Int. J. Environ. Res. Public Health 2017, 14, 182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nantanda, R.; Buteme, S.; Van Kampen, S.; Cartwright, L.; Pooler, J.; Barton, A.; Callaghan, L.; Mirembe, J.; Ndeezi, G.; Tumwine, J.K.; et al. Feasibility and acceptability of a midwife-led health education strategy to reduce exposure to biomass smoke among pregnant women in Uganda, A FRESH AIR project. Glob. Public Health 2019, 14, 1770–1783. [Google Scholar] [CrossRef] [PubMed]
- Stanistreet, D.; Hyseni, L.; Puzzolo, E.; Higgerson, J.; Ronzi, S.; Anderson de Cuevas, R.; Adekoje, O.; Bruce, N.; Mbatchou Ngahane, B.; Pope, D. Barriers and facilitators to the adoption and sustained use of cleaner fuels in Southwest Cameroon: Situating ‘lay’ knowledge within evidence-based policy and practice. Int. J. Environ. Res. Public Health 2019, 16, 4702. [Google Scholar] [CrossRef] [Green Version]
- Ronzi, S.; Puzzolo, E.; Hyseni, L.; Higgerson, J.; Stanistreet, D.; Ngahane, M.; Hugo, B.; Bruce, N.; Pope, D. Using photovoice methods as a community-based participatory research tool to advance uptake of clean cooking and improve health: The LPG adoption in Cameroon evaluation studies. Soc. Sci. Med. 2019, 228, 30–40. [Google Scholar] [CrossRef]
- Devakumar, D.; Qureshi, Z.; Mannell, J.; Baruwal, M.; Sharma, N.; Rehfuess, E.; Saville, N.; Manandhar, D.; Osrin, D.; Devakumar, D.; et al. Women’s ideas about the health effects of household air pollution, developed through focus group discussions and artwork in Southern Nepal. Int. J. Environ. Res. Public Health 2018, 15, 248. [Google Scholar] [CrossRef] [Green Version]
- Hengstermann, M.; Díaz-Artiga, A.; Otzóy-Sucúc, R.; Laura Maria Ruiz-Aguilar, A.; Thompson, L.M.; Aravindalochanan, V.; Balakrishnan, K.; Barr, D.B.; Burrowes, V.; Campbell, D.; et al. Developing Visual Messages to Support Liquefied Petroleum Gas Use in Intervention Homes in the Household Air Pollution Intervention Network (HAPIN) Trial in Rural Guatemala. Health Educ. Behav. 2021, 48, 651–669. [Google Scholar] [CrossRef]
- The World Bank. Rwanda|Data. Available online: https://data.worldbank.org/country/rwanda (accessed on 12 August 2021).
- The World Bank. GDP per Capita (Current US$)—Rwanda|Data. Available online: https://data.worldbank.org/indicator/NY.GDP.PCAP.CD?locations=RW (accessed on 12 August 2021).
- World Bank Group; Goverment of Rwanda (GoR). Future Drivers of Growth in Rwanda: Innovation, Intergration, Agglomeration, and Competition. Available online: https://openknowledge.worldbank.org/handle/10986/30732 (accessed on 15 October 2019).
- ICF. The DHS Program STATcompiler. Available online: http://www.statcompiler.com (accessed on 3 September 2020).
- The New Times. Government to Ban Charcoal Use in Kigali. Available online: https://www.newtimes.co.rw/ (accessed on 12 June 2020).
- Shupler, M.; Mwitari, J.; Gohole, A.; Anderson de Cuevas, R.; Puzzolo, E.; Čukić, I.; Nix, E.; Pope, D. COVID-19 impacts on household energy & food security in a Kenyan informal settlement: The need for integrated approaches to the SDGs. Renew. Sustain. Energy Rev. 2021, 144, 111018. [Google Scholar] [CrossRef]
- Campbell, C.A.; Bartington, S.E.; Woolley, K.E.; Pope, F.D.; Thomas, G.N.; Singh, A.; Avis, W.R.; Tumwizere, P.R.; Uwanyirigira, C.; Abimana, P.; et al. Investigating cooking activity patterns and perceptions of air quality interventions among women in urban Rwanda. Int. J. Environ. Res. Public Health 2021, 18, 5984. [Google Scholar] [CrossRef] [PubMed]
- Seguin, R.; Flax, V.L.; Jagger, P. Barriers and facilitators to adoption and use of fuel pellets and improved cookstoves in urban Rwanda. PLoS ONE 2019, 13, e0203775. [Google Scholar] [CrossRef] [PubMed]
- Iribagiza, C.; Sharpe, T.; Coyle, J.; Nkubito, P.; Piedrahita, R.; Johnson, M.; Thomas, E.A. Evaluating the Effects of Access to Air Quality Data on Household Air Pollution and Exposure—An Interrupted Time Series Experimental Study in Rwanda. Sustainability 2021, 13, 11523. [Google Scholar] [CrossRef]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michie, S.; Atkins, L.; West, R. The Behaviour Change Wheel: A Guide to Designing Interventions. Available online: http://www.behaviourchangewheel.com/ (accessed on 29 June 2020).
- Kabera, T.; Bartington, S.; Uwanyirigira, C.; Abimana, P.; Pope, F. Indoor PM 2.5 characteristics and CO concentration in households using biomass fuel in Kigali, Rwanda. Int. J. Environ. Stud. 2020, 77, 998–1011. [Google Scholar] [CrossRef]
- Jupp, V. The SAGE Dictionary of Social Research Methods; SAGE Publications, Ltd.: Thousand Oaks, CA, USA, 2006. [Google Scholar]
- Faulkner, S.L.; Trotter, S.P. Data Saturation. In The International Encyclopedia of Communication Research Methods; Wiley: Hoboken, NJ, USA, 2017; pp. 1–2. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- NVivo.11, Version 11; NVivo Qualitative Data Analysis Software; QSR International: Burlington, MA, USA, 2012.
- Saldana, J. The Coding Manual for Qualitative Researchers; SAGE Publications Led: London, UK, 2009; ISBN 978-1-84787-548-8. [Google Scholar]
- Shankar, A.; Johnson, M.; Kay, E.; Pannu, R.; Beltramo, T.; Derby, E.; Harrell, S.; Davis, C.; Petach, H. Maximizing the benefits of improved cookstoves: Moving from acquisition to correct and consistent use. Glob. Health Sci. Pract. 2014, 2, 268–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labriet, M.; Alfaro, O. Scaling Up Demand for LPG in Guatemala: Motivators, Barriers and Opportunities; Public Health Institute: Oakland, CA, USA, 2015. [Google Scholar]
- Muindi, K.; Egondi, T.; Kimani-Murage, E.; Rocklov, J.; Ng, N. “We are used to this”: A qualitative assessment of the perceptions of and attitudes towards air pollution amongst slum residents in Nairobi. BMC Public Health 2014, 14, 226. [Google Scholar] [CrossRef]
- Cecelski, E.; Matinga, M.M. Why Women in Developing Countries Want LPG and How They Can Get It. Available online: https://www.wlpga.org/wp-content/uploads/2019/07/Cooking-with-Gas-Why-Women-in-Developing-Countries-Want-LPG-and-How-They-can-Get-It.pdf (accessed on 20 September 2021).
- Perros, T.; Büttner, P.; Leary, J.; Parikh, P. Pay-as-you-go LPG: A mixed-methods pilot study in urban Rwanda. Energy Sustain. Dev. 2021, 65, 117–129. [Google Scholar] [CrossRef]
- Kumar, P.; Mehta, S. Poverty, gender, and empowerment in sustained adoption of cleaner cooking systems: Making the case for refined measurement. Energy Res. Soc. Sci. 2016, 19, 48–52. [Google Scholar] [CrossRef]
- Odo, D.B.; Yang, I.A.; Green, D.; Knibbs, L.D. Women’s empowerment and household fuel use in 31 African countries: A cross-sectional analysis of households in the Demographic and Health Survey. Environ. Res. Lett. 2021, 16, 025012. [Google Scholar] [CrossRef]
- Jagger, P.; Das, I.; Handa, S.; Nylander-French, L.A.; Yeatts, K.B. Early Adoption of an Improved Household Energy System in Urban Rwanda. EcoHealth 2019, 16, 7–20. [Google Scholar] [CrossRef] [PubMed]
- Das, I.; Klug, K.; Krishnapriya, P.; Plutshack, V.; Saparapa, R.; Scott, S.; Pattanayak, S.K. A Virtuous Cycle? Reviewing the Evidence on Women’s Empowerment and Energy Access, Frameworks, Metrics and Methods. Available online: https://energyaccess.duke.edu/wp-content/uploads/2020/11/White-paper-on-gender-and-energy-access-Oct-2020.pdf (accessed on 23 November 2021).
- Quinn, A.K.; Bruce, N.; Puzzolo, E.; Dickinson, K.; Sturke, R.; Jack, D.W.; Mehta, S.; Shankar, A.; Sherr, K.; Rosenthal, J.P. An analysis of efforts to scale up clean household energy for cooking around the world. Energy Sustain. Dev. 2018, 46, 1–10. [Google Scholar] [CrossRef]
- Namagembe, A.; Muller, N.; Scott, L.M.; Zwisler, G.; Johnson, M.; Arney, J.; Charron, D.; Mugisha, E. Factors influencing the acquisition and correct and consistent use of the top-lit updraft cookstove in Uganda. J. Health Commun. 2015, 20, 76–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alam, A.; Tawale, N.; Patel, A.; Dibley, M.J.; Jadhao, S.; Raynes-Greenow, C. Household air pollution intervention implications: Findings from qualitative studies and a field trial of clean cookstoves in two rural villages in India. Int. J. Environ. Res. Public Health 2016, 13, 893. [Google Scholar] [CrossRef]
- Barstow, C.K.; Ngabo, F.; Rosa, G.; Majorin, F.; Boisson, S.; Clasen, T.; Thomas, E.A. Designing and piloting a program to provide water filters and improved cookstoves in Rwanda. PLoS ONE 2014, 9, e92403. [Google Scholar] [CrossRef]
- Pickering, A.J.; Djebbari, H.; Lopez, C.; Coulibaly, M.; Alzua, M.L. Effect of a community-led sanitation intervention on child diarrhoea and child growth in rural Mali: A cluster-randomised controlled trial. Lancet Glob. Health 2015, 3, e701–e711. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Participant | Age (Years) | Occupation | Income (RFW) | Cooking Fuel | Cooking Location |
|---|---|---|---|---|---|
| Participant 1 | 35–44 | Teacher | 180,000 | Wood | Outdoors |
| Participant 2 | 35–44 | Housewife | 60,000 | Charcoal | Outdoors |
| Participant 3 | 35–44 | Security worker | 100,000 | Charcoal | Outdoors |
| Participant 4 | 25–34 | Casual worker | 300,000 | Charcoal | Separate kitchen |
| Participant 5 | 25–34 | Housewife | 60,000 | Charcoal | Separate kitchen |
| Participant 6 | 35–44 | Casual worker | 20,000 | Wood | Indoors |
| Participant 7 | 55–64 | House cleaner | 50,000 | Charcoal | Outdoors |
| Participant 8 | 35–44 | Casual worker | 30,000 | Charcoal | Outdoors |
| Participant 9 | 45–54 | Housewife | 100,000 | Charcoal | Outdoors |
| Participant 10 | 35–44 | Hair dresser | 250,000 | Charcoal | Indoors |
| Participant 11 | 25–34 | Casual worker | 40,000 | Wood | Outdoors |
| Participant 12 | 35–44 | Casual worker | 30,000 | Charcoal | Outdoors |
| Participant 13 | 35–44 | Mobile seller of vegetables | 60,000 | Wood | Outdoors |
| Participant 14 | 35–44 | Casual worker | 20,000 | Charcoal | Outdoors |
| Participant 15 | 25–34 | Casual worker | 50,000 | Charcoal | Outdoors |
| Participant 16 | 25–34 | Business woman | 150,000 | Charcoal | Outdoors |
| Cooking Behaviour | Code | Theme | Barrier | Facilitator |
|---|---|---|---|---|
| Outdoor cooking | Weather | Opportunity | X | |
| Housing constraints | Capability | X | ||
| Benefits of outdoor cooking | Motivation | X | ||
| Negatives of outdoor cooking | Motivation | X | ||
| Safety | Capability | X | ||
| Belief about where cooking should take place | Motivation | X | ||
| Impact of indoor cooking | Motivation | X | ||
| Keeping children out of the cooking area | Outdoor cooking | Capability | X | |
| Keeping children occupied | Capability | X | ||
| LPG | Ability to use LPG –equipment, security, safety | Capability | X | |
| Financial constraints | Capability | X | ||
| Health improvements | Motivation | X | ||
| Governmental help | Opportunity | X | ||
| Poverty cycle | Opportunity | X | ||
| Education | Awareness of sources, consequences and options | Capability | X | X |
| Previous experience and neighbours’ experience | Motivation | X |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Woolley, K.E.; Bartington, S.E.; Thomas, G.N.; Pope, F.D.; Muhizi, A.; Mugabe, C.; Ahishakiye, O.; Kabera, T.; Greenfield, S.M. Women’s Perceptions and Attitudes to Household Air Pollution Exposure and Capability to Change Cooking Behaviours in Urban Rwanda. Sustainability 2022, 14, 1608. https://doi.org/10.3390/su14031608
Woolley KE, Bartington SE, Thomas GN, Pope FD, Muhizi A, Mugabe C, Ahishakiye O, Kabera T, Greenfield SM. Women’s Perceptions and Attitudes to Household Air Pollution Exposure and Capability to Change Cooking Behaviours in Urban Rwanda. Sustainability. 2022; 14(3):1608. https://doi.org/10.3390/su14031608
Chicago/Turabian StyleWoolley, Katherine E., Suzanne E. Bartington, G. Neil Thomas, Francis D. Pope, Aldo Muhizi, Claude Mugabe, Omar Ahishakiye, Telesphore Kabera, and Sheila M. Greenfield. 2022. "Women’s Perceptions and Attitudes to Household Air Pollution Exposure and Capability to Change Cooking Behaviours in Urban Rwanda" Sustainability 14, no. 3: 1608. https://doi.org/10.3390/su14031608
APA StyleWoolley, K. E., Bartington, S. E., Thomas, G. N., Pope, F. D., Muhizi, A., Mugabe, C., Ahishakiye, O., Kabera, T., & Greenfield, S. M. (2022). Women’s Perceptions and Attitudes to Household Air Pollution Exposure and Capability to Change Cooking Behaviours in Urban Rwanda. Sustainability, 14(3), 1608. https://doi.org/10.3390/su14031608