Abstract
Background: Tobacco use is a global public health concern due to its association with a myriad of health hazards and costs. Previous studies have found that the disinhibiting influence of alcohol consumption may lead to an increase in tobacco use. In this study, we investigated why alcohol consumption is associated with tobacco use among older adults in Western China, and we attempted to explain the mechanisms that underlie the link between alcohol consumption and tobacco use. Methods: In this cross-sectional study, we employed a representative sample of 812 urban individuals aged 60 and older in 2017 in Western China. Results: We found that alcohol consumption (OR = 2.816, 95%CI: 1.770–4.479) was positively associated with tobacco use. Additionally, other factors, including gender (OR = 0.023, 95%CI: 0.009–0.060), age (OR = 0.758, 95%CI: 0.634–0.906), health literacy (OR = 0.977, 95%CI: 0.959–0.995) and functional impairment (OR = 0.871, 95%CI: 0.767–0.988) were also strongly related to tobacco use. Conclusions: Consistent with the results of existing studies, our findings demonstrated the disinhibiting influence of alcohol consumption on tobacco use, which confirmed the theoretical mechanisms that underlie the alcohol–tobacco link and implied the co-occurrence and co-use of alcohol and tobacco, which are used as “social lubricants” in the Chinese context. The importance of other factors related to tobacco use were also discussed. As the tobacco epidemic is combatted, joint interventions tailored to concurrent control over alcohol and tobacco need to be performed, and corresponding male-specific and age-specific health education and the reinforcement of health literacy must be considered as important priorities.
1. Introduction
Tobacco is an obvious barrier to sustainable development [1], and tobacco use is generally considered to be a global epidemic [2]. Successful tobacco control could be an effective method of not only improving population health but also protecting the environment and enabling socioeconomic development [1]. Therefore, over the past two decades, substantial global measures against the tobacco epidemic have been taken by the World Health Organization [3]. Growing attention has been paid to the health hazards and costs of smoking, and this issue has gained importance worldwide. Moreover, strengthening tobacco control is a vital development target within the 2030 Sustainable Development Goals [4,5]. Additionally, a set of strong tobacco control practices have been implemented in most countries [5].
There is evidence that tobacco use impacts the risk of mortality [6] and increases the incidence and prevalence of diseases [7]. Previous investigations indicated that the number of deaths related to smoking behaviors was about 7.69 million in 2019 [8,9]. Many respiratory infections and their severities are caused by tobacco use, and public health experts found that compared with non-smokers, smokers had a higher likelihood of developing severe illness due to COVID-19 [10]. This might be because smoking damages lung tissue, which prevents the lungs from functioning properly and fighting off coronaviruses and other diseases [10]. In addition, tobacco use impacts economic development worldwide. The worldwide smoking-related costs had reached around USD 1.4 trillion in 2012 [11], 40% of which occurred in developing countries [12]. By 2010, cigarette smoking resulted in 8.7% of annual healthcare spending in the U.S. [13]. The substantial burden represented by smoking-attributable diseases also has a negative role in economic development in China [14]. In 2019, Chinese researchers estimated that the cost of smoking in China was between RMB 57.162 and 368.273 billion in total; specifically, 49.17–68.94% of the direct costs were due to smoking-attributable outpatient visits, and 64.52–98.82% of the indirect costs resulted from smoking-related mortality [14].
Moreover, aging smokers in particular are more vulnerable to severe health status impairment than other groups. For instance, tobacco use increases the possibility of Alzheimer’s disease among older tobacco users [15]. In addition, the higher prevalence of tobacco use was observed among older adults in certain countries, including Thailand [16], Russia and Belarus [17] and China [18]. In order to combat the tobacco epidemic among older adults in China, a national tobacco control program was implemented by the Chinese Central Government in the Healthy China Action Plans (2019–2030) in 2019 [19]. Hence, it is important to explore and understand the predictors of tobacco use and to establish ways and mechanisms of successfully encouraging changes in smoking behaviors and improving health behaviors among older adults.
Moreover, previous studies have found that the disinhibiting influence of consuming alcohol may lead to increased tobacco use [20,21,22]. However, it was discovered that very few studies have investigated how alcohol consumption is associated with tobacco use in China. This study aimed to detect the influence of alcohol consumption on tobacco use among urban older adults in Western China.
2. Literature Review
2.1. Theoretical Mechanisms Underlying the Alcohol–Tobacco Link
Several theoretical mechanisms have been proposed to explain the alcohol–tobacco association and alcohol-induced increases in smoking. First, alcohol consumption may disrupt cognitive functions, such as attention, and may result in an increased urge and desire to smoke [23,24]. Furthermore, alcohol consumption may influence behavioral and neurobiological mechanisms, such as weakened self-control or self-regulation and increased impulsivity [20,21,22], and then lead to increased tobacco use. Moreover, the robust pharmacological effect of alcohol consumption may lead to an increased urge to smoke through mechanisms such as the interaction of alcohol with brain nicotinic receptors [25] and the ultimate activation of brain reward pathways and dopamine release [26].
In this study, the theoretical mechanisms discussed above were used to explain how alcohol consumption is associated with tobacco use.
2.2. Alcohol Consumption Associated with Tobacco Use
Studies have identified that alcohol consumption is a strong predictor of tobacco use. Alcohol consumption is positively associated with the frequency of tobacco use [27,28,29]. Additionally, in India, it was found that alcohol users are more likely to be tobacco users compared to their counterparts [30]. Data showed that in the U.S., the prevalence of tobacco use was more than two times higher among individuals who consumed alcohol compared to their counterparts [31]. Several studies have identified the impact of alcohol consumption on tobacco use in real-life situations [32,33]. Specifically, one study suggested that the role of alcohol consumption in tobacco use was larger for men than women among older African American adults [33].
2.3. Other Factors Associated with Tobacco Use
Many studies have focused on other factors associated with tobacco use among older adults, with findings indicating three main factors: socio-demographic attributes, health literacy and health status.
Studies have found that many socio-demographic attributes of older adults are associated with tobacco use. Specifically, gender is strongly associated with smoking in the elderly, and in developed and developing countries, a vast majority of older men are smokers [2,30,34,35]. In the U.S., aging and the experience of older adulthood often results in reduced smoking consumption [36]. Educational attainment is an important factor associated with tobacco use in the elderly. In Singapore, Indonesia and Malaysia, a relationship between lower educational attainment and higher rates of smoking among older adults was found [2,35,37]. Research has demonstrated that ethnicity is negatively and significantly related to tobacco use. Research conducted in four geographic regions in China revealed that in older Han Chinese adults, there is typically a lower prevalence of smoking than in ethnic minorities [38]. It has also been well established that income negatively affects tobacco use among older Indian and American adults in particular [30,39].
It has been shown that health education and health literacy plans discourage older adults from smoking [40]. As stated by Sadeghi et al.: “the likelihood of smoking decreased as health literacy increased” [41]. Participation in health education plans is negatively related to unhealthy behaviors such as tobacco use [42,43]. Compared with those with adequate health literacy, aging ever-smokers with inadequate health literacy presented higher likelihoods to be current smokers [44]. It has been proven that older adults with low health literacy are more likely to report current tobacco use than those with high health literacy [40].
Physical and psychological health is an important determinant of smoking among older adults, as are self-rated health [36], depressive symptoms [45], functional impairment [46] and life satisfaction [47,48]. A very poor health condition would induce enough “fear or motivation” to cause an older adult to change their smoking status [46]. Having at least one chronic disease would decrease the likelihood of older smokers maintaining their current smoking status [49]. It has been shown that both former and current smokers have higher depressive scores compared with non-smokers [45]. A higher level of functional impairment predicts a reduced likelihood of continuous smoking behavior among older adults [46]. In Ghana [47] and England [48], life satisfaction has been shown to negatively impact tobacco use among older adults.
From the literature discussed above, we can see that previous studies have examined the association between alcohol consumption and tobacco use, but most of them did not focus on older adults. Moreover, information regarding the alcohol–tobacco link and its theoretical implications remains scarce among older adults in China. In the current study, we presented evidence pertaining to the influence of alcohol consumption on tobacco use among urban older adults in Western China.
2.4. Theoretical Framework
Based on the literature discussed above, the theoretical framework in the present study is shown in Figure 1.
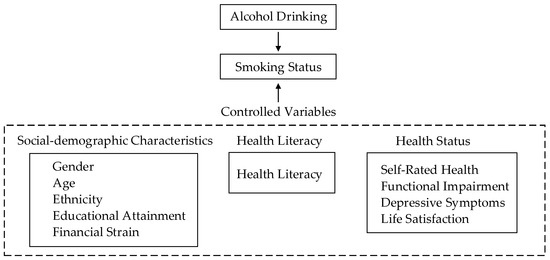
Figure 1.
The conceptual model.
3. Research Method
3.1. Data Collection
As explained in the work of Li et al. [50], the process of data collection used in this study is described below.
The cross-sectional survey was conducted from July to September 2017 in urban areas of Western China. Using a stratified multistage and cluster random sampling design, we randomly selected 812 urban older adults aged 60 and older who lived in Yinchuan city in the Ningxia Hui Autonomous Region, Wenshan city in Yunnan Province and the Yongchuan district in Chongqing municipality in Western China.
First, three provinces or municipalities were selected in Western China. Ningxia was selected from the northwest of China, and Yunnan and Chongqing were selected from the southwest of China. Second, within each province or municipality, one urban area was randomly selected. Yinchuan city was selected from Ningxia, Wenshan city was selected from Yunnan and Yongchuan district was selected from Chongqing. Third, three blocks were randomly selected within each city or district. Fourth, five urban residential communities were randomly selected within each block in Yinchuan city, 16 urban residential communities were randomly selected within each block in Wenshan city and 12 urban residential communities were randomly selected within each block in Yongchuan district. Fifth, households were randomly selected within each urban residential community in each province or municipality. In the case of households with more than one person aged 60 or older, one individual was selected at random using the Kish table. Therefore, 812 urban households were selected, and the number of randomly selected households in Ningxia, Yunnan and Chongqing were 203, 278 and 331, respectively.
Data collection was based on the implementation of a health literacy survey questionnaire in paper-assisted and face-to-face personal interviews. First, the participants were asked to provide written consent regarding the purposes and objectives of this study. Then, the interviewees agreed to participate. A total of 812 questionnaires were issued, and the response rate was 100% (812 of 812).
3.2. Measurement Instruments
Based on the literature discussed above, we examined potential predictors including health literacy, alcohol consumption and other factors (gender, age, educational attainment, ethnicity, financial strain, self-rated health, depressive symptoms, functional impairment and life satisfaction). We used a representative sample to help us understand and identify the relationships between these possible factors and tobacco use among urban older adults in Western China.
3.2.1. Tobacco Use
As outlined by Assari et al. [33], tobacco use is evaluated by asking participants about their smoking habits. In our survey, a single-item question, “How would you describe your tobacco smoking habits?”, was used to collect information regarding smoking from the respondents. Respondents who answered “never” to the question were classified as never-smokers, participants who answered “ever” to the question were classified as past smokers, and those who answered “occasionally or regularly” to the question were classified as current smokers [2,36]. In the current research, never-smokers and past smokers were combined and constituted the non-smoker category [35], and occasional or regular smokers were categorized as current smokers [16]. Thus, tobacco use status was classified by “smoker” (occasional or regular smoker) or “non-smoker” (past smoker/never-smoker) statuses [35,51]. It was operationalized as a dichotomous variable (0 = non-smoker; 1 = smoker).
3.2.2. Alcohol Consumption
As mentioned in the work of Kim et al. [52], alcohol consumption is evaluated by asking participants about their alcohol consumption status in their lifetime, and the subjects are classified into three categories, including non-drinkers, ex-drinkers, and current drinkers. Based on the definition and measurement above, a single-item question, “How would you describe your alcohol drinking status in your lifetime?”, was used to capture information regarding the alcohol consumption of respondents in our survey. We categorized those who said that they never drink as “non-drinkers”, participants who answered “ever” to the question were classified as “past drinkers” or “former drinkers”, and those who answered “occasionally or regularly” to the question were classified as “current drinkers”. For the purpose of statistical analysis, never-drinkers and past drinkers were combined and constituted the non-drinkers category, and occasional or regular drinkers were categorized as current drinkers. Thus, alcohol consumption status was divided into “drinker” (occasional or regular drinker) and “non-drinker” (past drinker/never-drinker) categories [53,54,55]. It was operationalized as a dichotomous variable (0 = non-drinker; 1 = drinker).
3.2.3. Health Literacy
We assessed health literacy using the Chinese version of the Citizen Health Literacy Questionnaire, which was developed by the China Health Educational Center. The health literacy questionnaire consisted of 80 items covering three dimensions: 38 items for the health knowledge dimension, 22 items for the health behavior dimension and 20 items for the health skill dimension. In our research, the Cronbach’s alpha of health knowledge, health behavior, health skill literacy and total health literacy was 0.886, 0.782, 0.793 and 0.937, respectively. More details regarding the 80 items of health literacy were presented in Nie et al. [56].
The format of all of the test items was in the form of four types of questions: true-or-false questions, single-answer questions (a score of one for a correct answer and a score of zero for an incorrect answer), multiple-answer questions (a score of two for all correct answers and a score of zero for all incorrect answers) and situation questions in the form of reading comprehension questions regarding common information, instructions and knowledge related to medicine and health in everyday life, which included single-answer questions and multiple-answer questions (with the same scoring criteria as the single- or multiple-answer questions described above). In each item, an answer of “I don’t know” was given a score of 0. The total health literacy score was calculated by adding up the scores of the 80 items with equal weighting [56,57]. The range of scores of health literacy was 1–94 in the current study.
3.2.4. Other Factors
Socio-demographic characteristics consisted of gender (0 = male and 1 = female), age (1 = 60–64, 2 = 65–69, 3 = 70–74, 4 = 75–79 and 5 = 80+), educational attainment (1 = illiterate, 2 = primary school, 3 = junior high school, 4 = polytechnic school or senior high school and 5 = college and above), ethnicity (1 = Han and 2 = minority) and financial strain, which was measured using a single item: ‘How do you assess your financial status?’ Respondents were asked to rate their financial status on a 3-point Likert scale (1 = enough, 2 = approximately enough and 3 = difficult).
Physical and psychological health were measured in terms of self-rated health, depressive symptoms, functional impairment and life satisfaction. Self-rated health was measured using a single item: ‘How do you asses your health status now?’ Respondents rated their health on a 5-point Likert scale (1 = bad, 2 = fair and 3 = good). Depressive symptoms were measured using the 15-item Geriatric Depression Short Form Scale (GDS-15) [58], which has been widely applied in research regarding psychological health. More details about the items, scales and calculations of GDS-15 were presented in the work of Li et al. [50]. The scores from the 15 items were added up to create an overall score with a range of 0–15. In the present sample, Cronbach’s alpha for the GDS-15 was 0.802. Functional impairment was assessed using two well-established instruments of functional status: activities of daily living (ADLs) [59] and instrumental activities of daily living (IADLs) [60]. More details about the items, scales and calculations of ADLs and IADLs were presented in the work of Li et al. [50]. In our current sample, the Cronbach’s alpha of the ADL and IADL measures were 0.818 and 0.856, respectively. An overall score of functional impairment (combining ADLs and IADLs) was calculated, with a range of 11–33. Higher cumulative scores indicated more limited functional ability. Life satisfaction [50] was measured using a single item: ‘Overall, how satisfied are you with your present life?’ Respondents were asked to rate this item on a 5-point Likert scale (1 = very unsatisfied, 2 = fairly unsatisfied, 3 = fair, 4 = fairly satisfied and 5 = very satisfied).
3.3. Data Analysis
First, the analysis included the calculation of detailed descriptive statistics with frequencies, percentages, means and standard deviations for all measures of tobacco use and its potential predictors. Second, a binary logistic regression model was used to detect the influence of the selected factors on tobacco use, and the regression coefficients(B), Exp(B), confidence intervals (95% CI) and p-values were reported in this sample. IBM SPSS 22.0 software (SPSS Inc., Chicago, IL, USA) was used for all analyses. Statistical significance was set at 0.05.
4. Results
4.1. Characteristics of the Respondents
Table 1 displays the descriptive statistics of the current sample (percentage distribution or means and standard deviations, and t-test or chi-square test results for all variables). It can be seen from the table that 17.5% of the participants were smokers, and 23.4% of the participants were alcohol drinkers.

Table 1.
Characteristics of the sample by smoking status.
4.2. Logistic Regression Model
A logistic regression model I—with alcohol consumption introduced as an independent variable—explained 11.8% of the variance in smoking (Table 2). Among the participants, alcohol consumption (OR = 7.402, 95%CI: 4.999–10.961) was significantly and positively associated with tobacco use. Specifically, the likelihood of being a smoker was 7.402 times higher for those who were alcohol drinkers compared to their counterparts.
Table 2.
Binary logistic regression model of alcohol consumption associated with tobacco use among urban older adults.
Moreover, by applying a new binary logistic regression model and controlling other factors, such as socio-demographic variables, health literacy and health status, we could conduct a better examination of the influence of alcohol consumption on tobacco use, as mentioned above. Before conducting the regression models, we examined multicollinearity among all of the independent variables. The results showed that all of the tolerance values of the independent variables were greater than the common threshold of 0.1, meaning that multicollinearity was at an acceptable level. In addition, the proportions of the independent information provided by all of the selected variables made up more than 32% of the variance.
As shown in Table 3, the logistic regression model II was adjusted to include other factors to examine whether alcohol consumption was still significantly linked to tobacco use. The variables used in the regression analysis explained 27.5% of the variance in participants in terms of tobacco use, which indicated strong predictive power.
Table 3.
Binary logistic regression model of alcohol consumption associated with tobacco use among urban older adults (controlling social–demographic variables, health literacy and health status).
Among the participants, alcohol consumption (OR = 2.816, 95%CI: 1.770–4.479) was still statistically associated with tobacco use. In addition, gender (OR = 0.023, 95%CI: 0.009–0.060), age (OR = 0.758, 95%CI: 0.634–0.906), health literacy (OR = 0.977, 95%CI: 0.959–0.995) and functional impairment (OR = 0.871, 95%CI: 0.767–0.988) were also significantly linked to tobacco use (Table 3). Specifically, the likelihood of being a smoker was 2.816 times higher for those who were alcohol drinkers compared to their counterparts. Female respondents experienced a reduction of 97.7% in the likelihood of becoming a smoker compared to male respondents. Each additional increase of one year in age was associated with a 24.2% decrease in the likelihood of becoming a smoker. As the level of health literacy increased, participants showed a decrease of 2.3% in the likelihood of becoming a smoker. As the level of functional impairment increased, participants showed a reduction of 12.9% in the likelihood of becoming a smoker.
5. Discussion
This study revealed that participants who consumed more alcohol were more likely to be smokers, and alcohol consumption and tobacco use were closely linked behaviors. Consistent with previous studies [21,22], we found that as a stimulating factor, alcohol consumption increased the likelihood of smoking. The reason for the disinhibiting influence of alcohol consumption is that alcohol may enhance the rewarding effects of nicotine [61]. Moreover, in the current study, there were two possible reasons for the alcohol–tobacco association. First, the association might have been because of the pattern of co-occurrence and co-use of alcohol and tobacco in real-life situations. As Shiffman and Balabanis stated, “Drinkers smoke and smokers drink” [32]. Alcohol and tobacco use seem to commonly occur together [62,63], and the co-use of both drugs is highly prevalent [64], especially in India [65], Ghana [47] and the U.S. [66]. Several studies have identified the fact that smokers reported an increased prevalence of smoking in drinking situations [67]. Alcohol consumption increases the prevalence of cigarette smoking behavior [68,69,70]. Alcohol consumption has also been shown to increase the urge to smoke in the absence of smoking cues or cigarette availability [24,71,72] and cause increased attention to smoking-related cues [73]. Furthermore, this pattern and evidence displayed in the current study can be explained by theoretical mechanisms, such as the interaction of alcohol with brain nicotinic receptors [25] and the ultimate activation of brain reward pathways and dopamine release [26]. Additionally, this finding also extends and enriches the applicability of the theoretical mechanisms that underlie the alcohol–tobacco link in the Chinese context.
Secondly, this association might be because the concurrent use of alcohol and tobacco often serve as “social lubricants” in social situations, especially in the context of China. Similar findings were observed in previous studies conducted in the U.S. [66] and India [30]. Moreover, the concurrent use of alcohol and tobacco can often be used to deal with emotional problems or stressful situations among older adults [30].
In addition, these findings also highlighted the importance of factors other than alcohol consumption. Other factors including gender, age, health literacy and functional impairment were also strongly associated with tobacco use.
Gender as a predisposing factor had the strongest influence on tobacco use. There was a huge difference in smoking prevalence, and the pattern of male domination in smoking was clear. Similar findings were examined in previous studies conducted in global areas [74] and specific countries, including Singapore [2], the U.S. [33], India [30] and Malaysia [35]. Gender differences in smoking were considered to be the result of social norms, gender inequality and social power disparity [2]. First, according to social norms and the usual stereotypes, tobacco use has been typically treated as a male behavior, while women’s smoking behaviors were considered to be inappropriate [75], especially in Asian society [30]. Furthermore, due to obligatory gender socialization in terms of culture’s gender-related rules and expectations in society, women may not have been able to be fully transparent about their smoking behaviors, and women had less opportunity to smoke cigarettes [75,76,77]. Furthermore, a previous study demonstrated that in Asia, absolute social power has been consistently greater for males than females [2]. This social power disparity restricts women’s behavior and could in turn lead to gender differences in tobacco use.
Age was inversely associated with tobacco use among older adults. Consistent with previous studies, current smokers were younger than never-smokers and past smokers among African American older adults in South Los Angeles in the U.S. [36] and older men, in particular in Korea [78] and Iran [79]. This might be because older adults felt more vulnerable due to increasing health problems with age. This feeling of vulnerability could help older adults consider improving their health behaviors and quitting smoking to prevent diseases [80].
The present study’s findings highlighted the influence of health literacy on tobacco use among older adults. First, the likelihood of continuing to smoke was lower among ever-smokers with adequate health literacy [44]. This might be because health literacy includes a complex set of abilities [81], including reading and numeracy skills, and health-related knowledge [82]. With health education and interventions [82], health knowledge and health literacy could be increased, and this in turn could contribute to better health outcomes [83]. Secondly, the specific mechanism of the link between inadequate health literacy and adverse health behaviors has been well-documented. Health literacy, as an inhibitive predictor, has been shown to reduce the odds of smoking. Most of the time, those who have a higher level of health literacy are more likely to adopt health-information-seeking behaviors and other health-related behaviors [84,85] and participate in health-promotion activities and programs, which might in turn contribute to reducing the likelihood of smoking. Similar findings were shown in previous studies conducted in a number of countries, including the U.S. [40,86], England [44], Iran [41] and Japan [87].
A mechanism through which functional impairment could affect tobacco use might be that older adults with functional impairment could evaluate the severity and threats of a smoking-related disease. According to the health belief model, perceived severity and threats among older adults were likely to make them restrict their smoking behavior to prevent functional impairment. A previous analysis of aging cohorts in the UK also confirmed that smoking, whether it be current smoking or ever-smoking, was linked to poor physical capacity, including the parameters of walking speed, balance and grip strength [88].
6. Implications and Limitations
6.1. Implications
The current study had several important implications. Tobacco cessation interventions were warranted in older adults, focusing on those who were alcohol users, men, younger old people and those with lower health literacy and functional impairment. First, the integration of alcohol and tobacco control programs might particularly benefit older adults in giving up smoking. Another implication was the need to develop gender-specific and age-specific tobacco cessation interventions. The pattern of male domination in tobacco use implied that smoking cessation interventions, particularly in male older adults, should be strengthened. Furthermore, the findings highlighted the importance of reinforcing health literacy to help guide and empower older adults to sustainably give up smoking and make health-related decisions. Specifically, spending more time and energy on regular health communication, education and intervention programs would be an effective way to increase health literacy among urban older adults in Western China.
6.2. Limitations
The limitations of the current study are presented in this section. First, we acknowledge that the data presented here have a limitation. In the past 5 years, significant changes have been witnessed in society, especially due to the COVID-19 epidemic. We failed to consider the effect of the epidemic on smoking in our current data and study. Second, the cross-sectional design of this study prevented causal associations between various predictors and tobacco use among older adults from being made; therefore, future studies could employ a stricter research design, such as longitudinal studies to establish the determination of cause and effect. Third, tobacco use was discussed as a whole but not based on specific smoking patterns, which might have resulted in different significance in the relations with various factors. Moreover, we measured tobacco use with a single item rather than with more comprehensive measurements, and this measurement could lead to a reduction in the validity [33]. Finally, the definitions of drinker and non-drinker statues varied widely between studies [53], and this limitation caused difficulties in making comparisons across different studies. Therefore, further studies based on intensive designs are needed.
7. Conclusions
Consistent with previous studies, the current findings demonstrate the disinhibiting influence of alcohol consumption on tobacco use. Moreover, the current study has theoretical implications that confirm and extend the well-documented phenomenon of the co-occurrence and co-use of alcohol and smoking, which serve as “social lubricants” in the Chinese context, and these implications also enrich the applicability of the theoretical mechanisms that underlie the alcohol–tobacco link. In addition, the current findings also indicate gender and age differences in smoking prevalence and identify the impact of health literacy on tobacco use. Thus, the current results suggest that concurrent control over alcohol and tobacco needs to be exerted to encourage changes in smoking behaviors, and corresponding male-specific and age-specific health education and the reinforcement of health literacy must be considered as important priorities.
Author Contributions
Conceptualization, C.L. (Chengbo Li); formal analysis, C.L. (Chengbo Li); funding acquisition, C.L. (Chengbo Li); investigation, C.L. (Chengbo Li); project administration, C.L. (Chengbo Li), C.L. (Chun Long), M.Z. and L.Z.; resources, C.L. (Chengbo Li); software, C.L. (Chengbo Li), C.L. (Chun Long), M.Z., L.Z., M.S., Y.C. and G.C.; writing—original draft, C.L. (Chun Long) and C.L. (Chengbo Li); writing—review and editing, C.L. (Chengbo Li), C.L. (Chun Long), M.Z., L.Z. and M.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Planning Office of Philosophy and Social Science grant number [16CRK014] and China Central Universities Fundamental Research Funds grant number [2020CDJSK07XK09].
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Academic Board of the School of Journalism and communication, Chongqing University (date of approval: 4 May 2017).
Informed Consent Statement
Informed consent was obtained from all of the subjects involved in the study.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author. The data are not publicly available due to privacy restrictions.
Acknowledgments
We would like to extend our sincere gratitude to all of the participants in the Survey on the Aged Population in West China.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Singh, P.K.; Thamarangsi, T. Accelerating tobacco control in South-East Asia in the sustainable development goal era. Indian J. Public Health 2017, 61 (Suppl. 1), 1–2. [Google Scholar] [CrossRef] [PubMed]
- Pang, S.; Subramaniam, M.; Abdin, E.; Lee, S.P.; Chua, B.Y.; Shafie, B.S.; Vaingankar, J.; Picco, L.; Zhang, Y.J.; Chong, S.A. Prevalence and predictors of tobacco use in the elderly. Int. J. Geriatr. Psychiatry 2016, 31, 716–722. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Framework Convention on Tobacco Control; World Health Organization: Geneva, Switzerland, 2003. Available online: https://www.who.int/fctc/text_download/en/ (accessed on 4 May 2020).
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development; United Nations: New York, NY, USA, 2015. Available online: https://sustainabledevelopment.un.org/post2015/transformingourworld/publication (accessed on 15 February 2021).
- Flor, L.S.; Reitsma, M.B.; Gupta, V.; Ng, M.; Gakidou, E. The effects of tobacco control policies on global smoking prevalence. Nat. Med. 2021, 27, 239–243. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks; World Health Organization: Geneva, Switzerland, 2009; ISBN 9789241563871. [Google Scholar]
- Countries Health Rankings & Roadmaps. Health Behaviors. 2020. Available online: https://www.countyhealthrankings.org/explore-health-rankings/measures-data-sources/county-health-rankings-model/health-factors/health-behaviors (accessed on 2 June 2020).
- GBD 2019 Tobacco Collaborators. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990–2019: A systematic analysis from the Global Burden of Disease Study 2019. Lancet 2021, 397, 2337–2360. [Google Scholar] [CrossRef]
- The Lancet. Tobacco control: Far from the finish line. Lancet 2021, 398, 1939. [Google Scholar] [CrossRef]
- World Health Organization. WHO Statement: Tobacco Use and COVID-19; World Health Organization: Geneva, Switzerland, 2020. Available online: https://www.who.int/news-room/detail/11-05-2020-who-statement-tobacco-use-and-covid-19 (accessed on 2 June 2020).
- Goodchild, M.; Nargis, N.; Tursan d’Espaignet, E. Global economic cost of smoking-attributable diseases. Tob. Control. 2018, 27, 58–64. [Google Scholar] [CrossRef]
- World Health Organization. Tobacco-Impact; World Health Organization: Geneva, Switzerland, 2019. Available online: https://www.who.int/health-topics/tobacco#tab=tab_2 (accessed on 18 June 2020).
- Xu, X.; Bishop, E.E.; Kennedy, S.M.; Simpson, S.A.; Pechacek, T.F. Annual Healthcare Spending Attributable to Cigarette Smoking. Am. J. Prev. Med. 2015, 48, 326–333. [Google Scholar] [CrossRef]
- Shi, L.; Zhong, L.; Cai, Y. Economic burden of smoking-attributable diseases in China: A systematic review. Tob. Induc. Dis. 2020, 18, 42. [Google Scholar] [CrossRef]
- Zhong, G.; Wang, Y.; Zhang, Y.; Guo, J.J.; Zhao, Y. Smoking is associated with an increased risk of dementia: A meta-analysis of prospective cohort studies with investigation of potential effect modifiers. PLoS ONE 2015, 10, e0118333. [Google Scholar] [CrossRef]
- Aungkulanon, S.; Pitayarangsarit, S.; Bundhamcharoen, K.; Akaleephan, C.; Chongsuvivatwong, V.; Phoncharoen, R.; Tangcharoensathien, V. Smoking prevalence and attributable deaths in Thailand: Predicting outcomes of different tobacco control interventions. BMC Public Health 2019, 19, 984. [Google Scholar] [CrossRef]
- Gugushvili, A.; Mckee, M.; Azarova, A.; Murphy, M.; Irdam, D.; King, L. Parental transmission of smoking among middle-aged and older populations in Russia and Belarus. Int. J. Public Health 2018, 63, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Chinese Center for Disease Control and Prevention. Global Adult Tobacco Survey China 2018; Chinese Center for Disease Control and Prevention: Beijing, China, 2019. Available online: http://www.chinacdc.cn/jkzt/sthd_3844/slhd_4156/201908/t20190814_204616.html (accessed on 21 July 2020).
- The Healthy China Promotion Committee. The Healthy China Action (2019–2030); The Healthy China Promotion Committee: Beijing, China, 2019. Available online: http://www.gov.cn/xinwen/2019-07/15/content_5409694.htm (accessed on 19 April 2021).
- Niaura, R.S.; Rohsenow, D.J.; Binkoff, J.A.; Monti, P.M.; Pedraza, M.; Abrams, D.B. Relevance of cue reactivity to understanding alcohol and smoking relapse. J. Abnorm. Psychol. 1988, 97, 133–152. [Google Scholar] [CrossRef] [PubMed]
- David, B.A.; Damaris, J.R.; Raymond, S.N.; Magda, P.; Richard, L.; Martha, C.B.; Jody, A.B.; Nora, E.N.; Peter, M.M. Smoking and treatment outcome for alcoholics: Effects on coping skills, urge to drink, and drinking rates. Behav. Ther. 1992, 23, 283–297. [Google Scholar] [CrossRef]
- Piasecki, T.M.; McCarthy, D.E.; Fiore, M.C.; Baker, T.B. Alcohol consumption, smoking urge, and the reinforcing effects of cigarettes: An ecological study. Psychol. Addict. Behav. 2008, 22, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Steele, C.M.; Josephs, R.A. Alcohol myopia. Its prized and dangerous effects. Am. Psychol. 1990, 45, 921–933. [Google Scholar] [CrossRef]
- Sayette, M.A.; Martin, C.S.; Wertz, J.M.; Perrott, M.A.; Peters, A.R. The effects of alcohol on cigarette craving in heavy smokers and tobacco chippers. Psychol. Addict. Behav. 2005, 19, 263–270. [Google Scholar] [CrossRef]
- Allan, C.C.; James, B.B.; Christopher, M.F.; Michael, J.M. Tolerance to and cross tolerance between ethanol and nicotine. Pharmacol. Biochem. Behav. 1988, 29, 365–373. [Google Scholar] [CrossRef]
- Balogh, S.A.; Owens, J.C.; Butt, C.M.; Wehner, J.M.; Collins, A.C. Animal models as a tool for studying mechanisms of co-abuse of alcohol and tobacco. Alcohol. Clin. Exp. Res. 2002, 26, 1911–1914. [Google Scholar] [CrossRef]
- Blazer, D.G.; Wu, L.T. The epidemiology of substance use and disorders among middle aged and elderly community adults: National Survey on Drug Use and Health. Am. J. Geriatr. Psychiatry 2009, 17, 237–245. [Google Scholar] [CrossRef]
- Bryant, A.N.; Kim, G. Racial/ethnic differences in prevalence and correlates of binge drinking among older adults. Aging Ment. Health 2012, 16, 208–217. [Google Scholar] [CrossRef]
- King, A.; Epstein, A.; Conrad, M.; McNamara, P.; Cao, D. Sex differences in the relationship between alcohol-associated smoking urge and behavior: A pilot study. Am. J. Addict. 2008, 17, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Mini, G.; Sarma, P.; Thankappan, K. Pattern of tobacco use and its correlates among older adults in India. Asian Pac. J. Cancer Prev. 2014, 15, 6195–6198. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Weinberger, A.H.; Gbedemah, M.; Goodwin, R.D. Cigarette smoking quit rates among adults with and without alcohol use disorders and heavy alcohol use, 2002–2015: A representative sample of the United States population. Drug Alcohol Depend. 2017, 18, 204–207. [Google Scholar] [CrossRef] [PubMed]
- Shiffman, S.; Balabanis, M. Do Drinking and Smoking Go Together? Alcohol Health Res. World 1996, 20, 107–110. [Google Scholar] [PubMed]
- Assari, S.; Smith, J.; Zimmerman, M.; Mohsen, B. Cigarette smoking among economically disadvantaged African-American older adults in South Los Angeles: Gender differences. Int. J. Environ. Res. Public Health 2019, 16, 1208. [Google Scholar] [CrossRef]
- Si, Y.; Zhou, Z.; Su, M.; Wang, X.; He, S.; Li, D.; Wang, D.; He, S.; Hong, Z.; Chen, X. Socio-Economic Inequalities in Tobacco Consumption of the Older Adults in China: A Decomposition Method. Int. J. Environ. Res. Public Health 2018, 15, 1466. [Google Scholar] [CrossRef]
- Lim, K.H.; Jasvindar, K.; Cheong, S.M.; Ho, B.K.; Lim, H.L.; The, C.H.; Lau, K.J.; Suthahar, A.; Ambigga, D. Prevalence of smoking and its associated factors with smoking among elderly smokers in Malaysia: Findings from a nationwide population-based study. Tob. Induc. Dis. 2016, 14, 8. [Google Scholar] [CrossRef]
- Bazargan, M.; Cobb, S.; Sandoval, J.C.; Assari, S. Smoking Status and Well-Being of Underserved African American Older Adults. Behav. Sci. 2020, 10, 78. [Google Scholar] [CrossRef]
- Pengpid, S.; Peltzer, K. Prevalence and predictors of current and former tobacco use among older adults in Indonesia. Asian Pac. J. Cancer Prev. 2019, 20, 395–401. [Google Scholar] [CrossRef]
- Yang, T.; Li, F.; Yang, X.; Wu, Z.; Feng, X.; Wang, Y.; Wang, X.; Abdullah, A.S.M. Smoking patterns and sociodemographic factors associated with tobacco use among Chinese rural male residents: A descriptive analysis. BMC Public Health 2008, 8, 248. [Google Scholar] [CrossRef]
- Blazer, D.G.; Wu, L. Patterns of tobacco use and tobacco-related psychiatric morbidity and substance use among middle-aged and older adults in the United States. Aging Ment. Health 2012, 16, 296–304. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, D.M.; Larson, J.L.; Zikmund-Fisher, B.J. Associations between health literacy and preventive health behaviors among older adults: Findings from the health and retirement study. BMC Public Health 2016, 16, 596. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, R.; Mahmoodabad, S.S.M.; Khanjani, N.; Fallahzadeh, H.; Rezaeian, M. The association between health literacy and smoking (Hookah and Cigarette) among the young men in Sirjan, Iran. J. Subst. Use 2009, 24, 546–549. [Google Scholar] [CrossRef]
- Brandt, L.; Schultes, M.T.; Yanagida, T.; Maier, G.; Spiel, C. Differential associations of health literacy with Austrian adolescents’ tobacco and alcohol use. Public Health 2019, 174, 74–82. [Google Scholar] [CrossRef]
- Stewart, D.W.; Cano, M.A.; Correa-Fernandez, V.; Spears, C.A.; Li, Y.; Waters, A.J.; Wetter, D.W.; Vidrine, J.I. Lower health literacy predicts smoking relapse among racially/ethnically diverse smokers with low socioeconomic status. BMC Public Health 2014, 14, 716. [Google Scholar] [CrossRef] [PubMed]
- Fawns-Ritchie, C.; Starr, J.M.; Deary, I.J. Health literacy, cognitive ability and smoking: A cross-sectional analysis of the English Longitudinal Study of Ageing. BMJ Open 2018, 8, e023929. [Google Scholar] [CrossRef]
- Kinnunen, T.; Haukkala, A.; Korhonen, T.; Quiles, Z.; Spiro, A.; Garvey, A. Depression and Smoking across 25 Years of the Normative Aging Study. Int. J. Psychiatry Med. 2006, 36, 413–426. [Google Scholar] [CrossRef]
- Tsai, C.H.; Lin, Y.A.; Tsai, H.J. Predictors of smoking cessation in 50–66-year-old male Taiwanese smokers: A 7-year national cohort study. Arch. Gerontol. Geriatr. 2012, 55, 295–300. [Google Scholar] [CrossRef]
- Yawson, A.E.; Baddoo, A.; Hagan-Seneadza, N.A.; Calys-Tagoe, B.; Hewlett, S.; Dako-Gyeke, P.; Mensah, G.; Minicuci, N.; Naidoo, N.; Chatterji, S.; et al. Tobacco use in older adults in Ghana: Sociodemographic characteristics, health risks and subjective wellbeing. BMC Public Health 2013, 13, 979. [Google Scholar] [CrossRef]
- Lappan, S.; Thorne, C.B.; Long, D.; Hendricks, P.S. Longitudinal and Reciprocal Relationships between Psychological Well-Being and Smoking. Nicotine Tob. Res. 2018, 22, 18–23. [Google Scholar] [CrossRef]
- Chaaya, M.; Mehio-Sibai, A.; El-Chemaly, S. Smoking patterns and predictors of smoking cessation in elderly populations in Lebanon. Int. J. Tuberc. Lung Dis. 2006, 10, 917–923. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Chi, I.; Zhang, X.; Cheng, Z.; Zhang, L.; Chen, G. Urban and rural factors associated with life satisfaction among older Chinese adults. Aging Ment. Health 2015, 19, 947–954. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.B.; Liu, L.; Li, Y.F.; Chen, Y.L. Relationship between health literacy, health-related behaviors and health status: A survey of elderly Chinese. Int. J. Environ. Res. Public Health 2015, 12, 9714–9725. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Shin, J.; Kweon, S.S.; Shin, D.H.; Lee, Y.H.; Chun, B.Y.; Choi, B.Y. Harmful and beneficial relationships between alcohol consumption and subclinical atherosclerosis. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 767–776. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Yang, H.; Cao, J. Association between alcohol consumption and cancers in the Chinese population--a systematic review and meta-analysis. PLoS ONE 2011, 6, e18776. [Google Scholar] [CrossRef]
- Liu, K.; Ding, Y.; Lu, X.; Wang, Z. Trends and socioeconomic factors in smoking and alcohol consumption among Chinese people: Evidence from the 2008-2018 National Health Service Surveys in Jiangsu Province. Arch. Public Health 2021, 79, 127. [Google Scholar] [CrossRef]
- Mihailovic, N.; Szőllősi, G.J.; Rancic, N.; János, S.; Boruzs, K.; Nagy, A.C.; Timofeyev, Y.; Dragojevic-Simic, V.; Antunovic, M.; Reshetnikov, V.; et al. Alcohol Consumption among the Elderly Citizens in Hungary and Serbia—Comparative Assessment. Int. J. Environ. Res. Public Health 2020, 17, 1289. [Google Scholar] [CrossRef]
- Nie, X.Q.; Li, Y.H.; Li, L. Statistic analysis of 2012 Chinese residents health literacy monitoring. Chin. J. Health Educ. 2014, 30, 178–181. [Google Scholar] [CrossRef]
- Shen, M.; Hu, M.; Liu, S.; Chang, Y.; Sun, Z. Assessment of the Chinese Resident Health Literacy Scale in a population-based sample in South China. BMC Public Health 2015, 15, 637. [Google Scholar] [CrossRef]
- Sheikh, J.I.; Yesavage, J.A. Geriatric Depression Scale (GDS): Recent evidence and development of a shorter version. Clin. Gerontol. 1986, 5, 165–173. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Rose, J.E.; Brauer, L.H.; Behm, F.M.; Cramblett, M.; Calkins, K.; Lawhon, D. Psychopharmacological interactions between nicotine and ethanol. Nicotine Tob. Res. 2004, 6, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Batel, P.; Pessione, F.; Maıtre, C.; Rueff, B. Relationship between alcohol and tobacco dependencies among alcoholics who smoke. Addition 1995, 90, 977–980. [Google Scholar] [CrossRef]
- Burton, S.M.; Tiffany, S.T. The effect of alcohol consumption on craving to smoke. Addiction 1997, 92, 15–26. [Google Scholar] [CrossRef]
- Harris, J.C.; Mereish, E.H.; Faulkner, M.L.; Assari, S.; Choi, K.; Leggio, L.; Farokhnia, M. Racial Differences in the Association between Alcohol Drinking and Cigarette Smoking: Preliminary Findings from an Alcohol Research Program. Alcohol Alcohol. 2021, 57, agab038. [Google Scholar] [CrossRef]
- Gupta, P.C.; Maulik, P.K.; Pednekar, M.S.; Saxena, S. Concurrent alcohol and tobacco use among a middle-aged and elderly population in Mumbai. Natl. Med. J. India 2005, 18, 88–91. [Google Scholar]
- David, J.D. Concurrent Alcohol and Tobacco Dependence Mechanisms and Treatment. Alcohol Res. Health 2002, 26, 136–142. [Google Scholar] [CrossRef]
- Reed, M.B.; Wang, R.; Shillington, A.M.; Clapp, J.D.; Lange, J.E. The relationship between alcohol use and cigarette smoking in a sample of undergraduate college students. Addict. Behav. 2007, 32, 449–464. [Google Scholar] [CrossRef]
- Henningfield, J.E.; Chait, L.D.; Griffiths, R.R. Effects of ethanol on cigarette smoking by volunteers without histories of alcoholism. Psychopharmacology 1984, 82, 1–5. [Google Scholar] [CrossRef]
- Mintz, J.; Boyd, G.; Rose, J.E.; Charuvastra, V.C.; Jarvik, M.E. Alcohol increases cigarette smoking: A laboratory demonstration. Addict. Behav. 1985, 10, 203–207. [Google Scholar] [CrossRef]
- Mitchell, S.H.; de Wit, H.; Zacny, J.P. Effects of varying ethanol dose on cigarette consumption in healthy normal volunteers. Behav. Pharmacol. 1995, 6, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Epstein, A.M.; Sher, T.G.; Young, M.A.; King, A.C. Tobacco chippers show robust increases in smoking urge after alcohol consumption. Psychopharmacology 2007, 190, 321–329. [Google Scholar] [CrossRef] [PubMed]
- King, A.C.; Epstein, A.M. Alcohol dose-dependent increases in smoking urge in light smokers. Alcohol. Clin. Exp. Res. 2005, 29, 547–552. [Google Scholar] [CrossRef] [PubMed]
- Field, M.; Mogg, K.; Bradley, B.P. Alcohol increases cognitive biases for smoking cues in smokers. Psychopharmacology 2005, 180, 63–72. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Report on Trends in Prevalence of Tobacco Smoking 2000–2025; World Health Organization: Geneva, Switzerland, 2019; ISBN 978-92-4-000003-2. [Google Scholar]
- Beasley, G.M.; Ostbye, T.; Muhlbaier, L.H.; Foley, C.; Scarborough, J.; Turley, R.S.; Shapiro, M.L. Age and gender differences in substance screening may underestimate injury severity: A study of 9793 patients at level 1 trauma center from 2006 to 2010. J. Surg. Res. 2014, 188, 190–197. [Google Scholar] [CrossRef]
- Buu, A.; Dabrowska, A.; Heinze, J.E.; Hsieh, H.F.; Zimmerman, M.A. Gender differences in the developmental trajectories of multiple substance use and the effect of nicotine and marijuana use on heavy drinking in a high-risk sample. Addict. Behav. 2015, 50, 6–12. [Google Scholar] [CrossRef]
- Kim, Y.; Park, I.; Kang, S. Age and gender differences in health risk perception. Cent. Eur. J. Public Health 2018, 26, 54–59. [Google Scholar] [CrossRef]
- Cho, H.J.; Khang, Y.H.; Jun, H.J.; Kawachi, I. Marital status and smoking in Korea: The influence of gender and age. Soc. Sci. Med. 2008, 66, 609–619. [Google Scholar] [CrossRef]
- Moghadam, T.Z.; Zandian, H.; Pourfarzi, F.; Poustchi, H. Environmental and economics-related factors of smoking among Iranian adults aged 35–70: A PERSIAN cohort–based cross-sectional study. Environ. Sci. Pollut. Res. 2021, 28, 45365–45374. [Google Scholar] [CrossRef]
- Levy, D.T.; Hyland, A.; Higbee, C.; Remer, L.; Compton, C. The role of public policies in reducing smoking prevalence in California: Results from the California Tobacco Policy Simulation Model. Health Policy 2007, 82, 167–185. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Health Literacy: A Prescription to End Confusion; National Academies Press: Washington, DC, USA, 2004. [Google Scholar] [CrossRef]
- Chin, J.; Morrow, D.G.; Stine-Morrow, E.A.; Conner-Garcia, T.; Graumlich, J.F.; Murray, M.D. The process-knowledge model of health literacy: Evidence from a componential analysis of two commonly used measures. J. Health Commun. 2011, 16, 222–241. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rothman, R.L.; DeWalt, D.A.; Malone, R.; Bryant, B.; Shintani, A.; Crigler, B.; Weinberger, M.; Pignone, M. Influence of patient literacy on the effectiveness of a primary care-based diabetes disease management program. JAMA 2004, 292, 1711–1716. [Google Scholar] [CrossRef] [PubMed]
- Manafo, E.; Wong, S. Health literacy programs for older adults: A systematic literature review. Health Educ. Res. 2012, 27, 947–960. [Google Scholar] [CrossRef]
- Bostock, S.; Steptoe, A. Association between low functional health literacy and mortality in older adults: Longitudinal cohort study. BMJ 2012, 344, e1602. [Google Scholar] [CrossRef]
- Hoover, D.S.; Vidrine, J.I.; Shete, S.; Spears, C.A.; Cano, M.A.; Correa-Fernández, V.; Wetter, D.W.; McNeill, L.H. Health Literacy, Smoking, and Health Indicators in African American Adults. J. Health Commun. 2015, 20, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Sudo, A.; Kuroda, Y. Media exposure, interactive health literacy, and adolescents’ susceptibility to future smoking. International J. Adolesc. Med. Health 2017, 29, 1–6. [Google Scholar] [CrossRef] [PubMed]
- North, T.L.; Palmer, T.M.; Lewis, S.J.; Cooper, R.; Power, C.; Pattie, A.; Starr, J.M.; Deary, I.J.; Martin, R.M.; Sayer, A.A.; et al. Effect of smoking on physical and cognitive capability in later life: A multicohort study using observational and genetic approaches. BMJ Open 2015, 5, e008393. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).