
Reducing the Environmental Impact of Sterilization Packaging for Surgical Instruments in the Operating Room: A Comparative Life Cycle Assessment of Disposable versus Reusable Systems

 , and
, and
Abstract
:1. Introduction
2. Method: Life Cycle Assessment
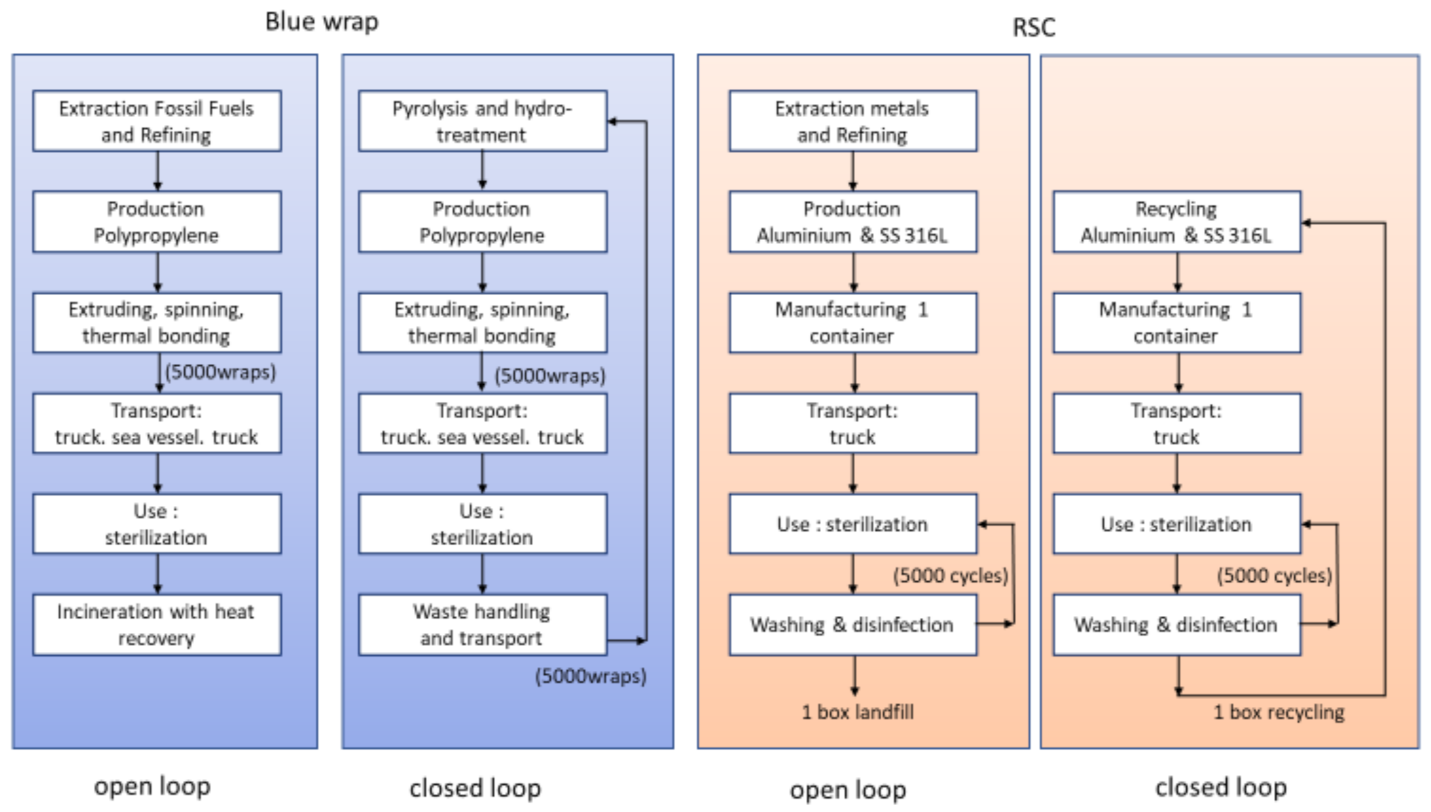
2.1. The System and the Functional Unit
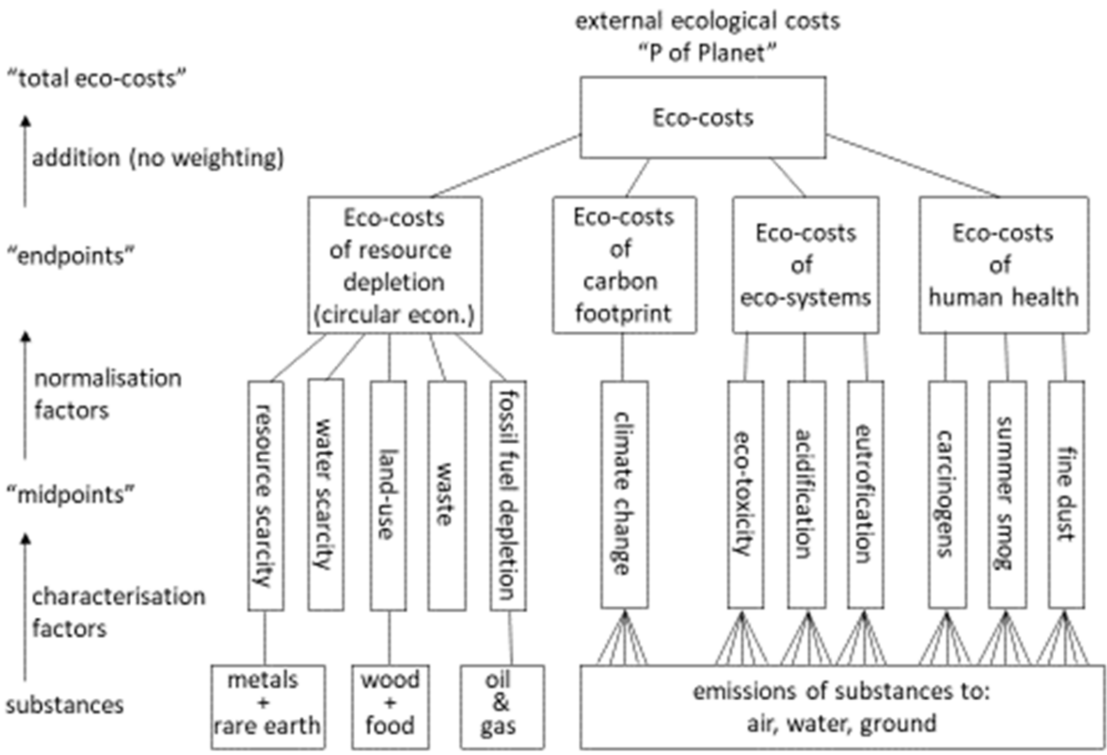
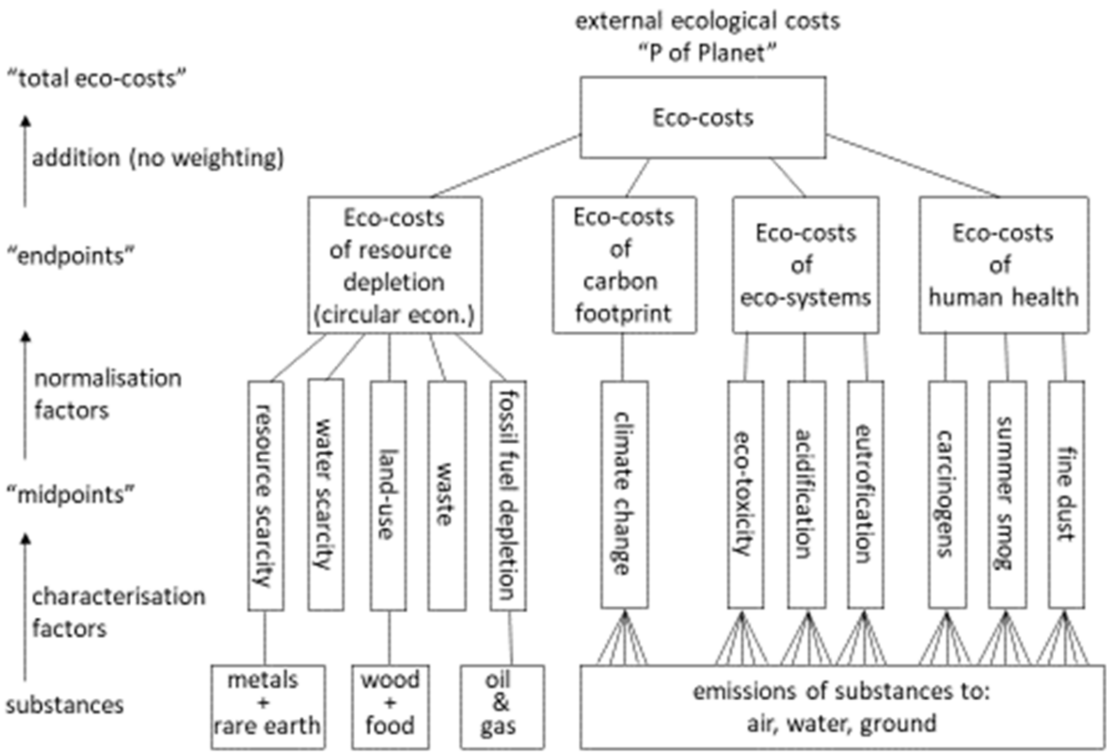
2.2. Choice of Single Indicators
2.3. Modelling Parameters
2.4. Three Scenarios for Electricity
3. Results
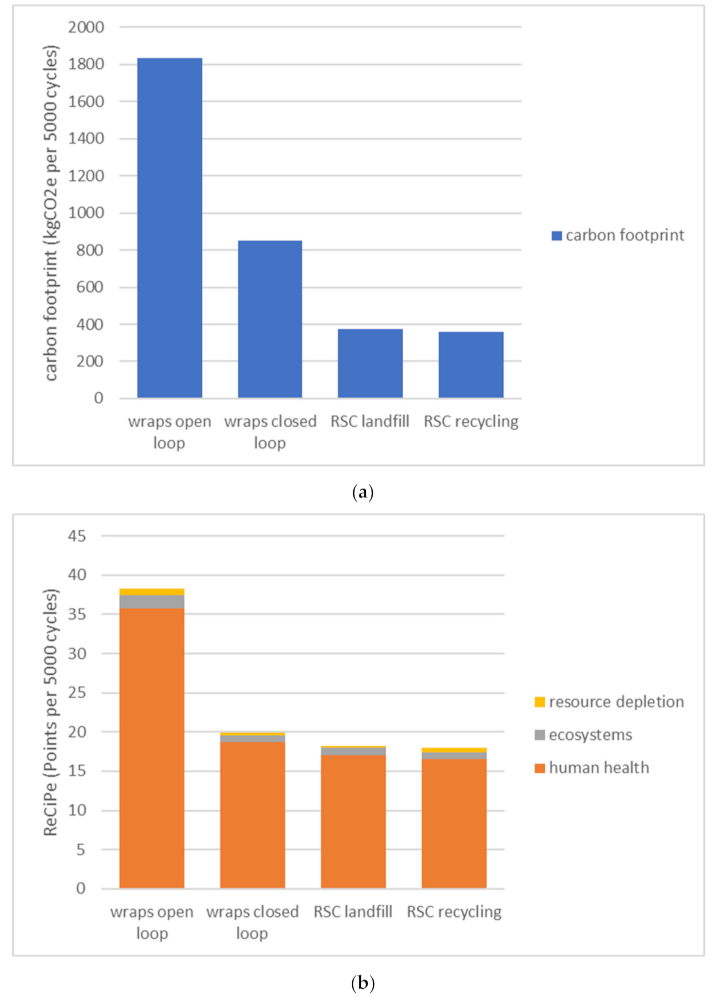
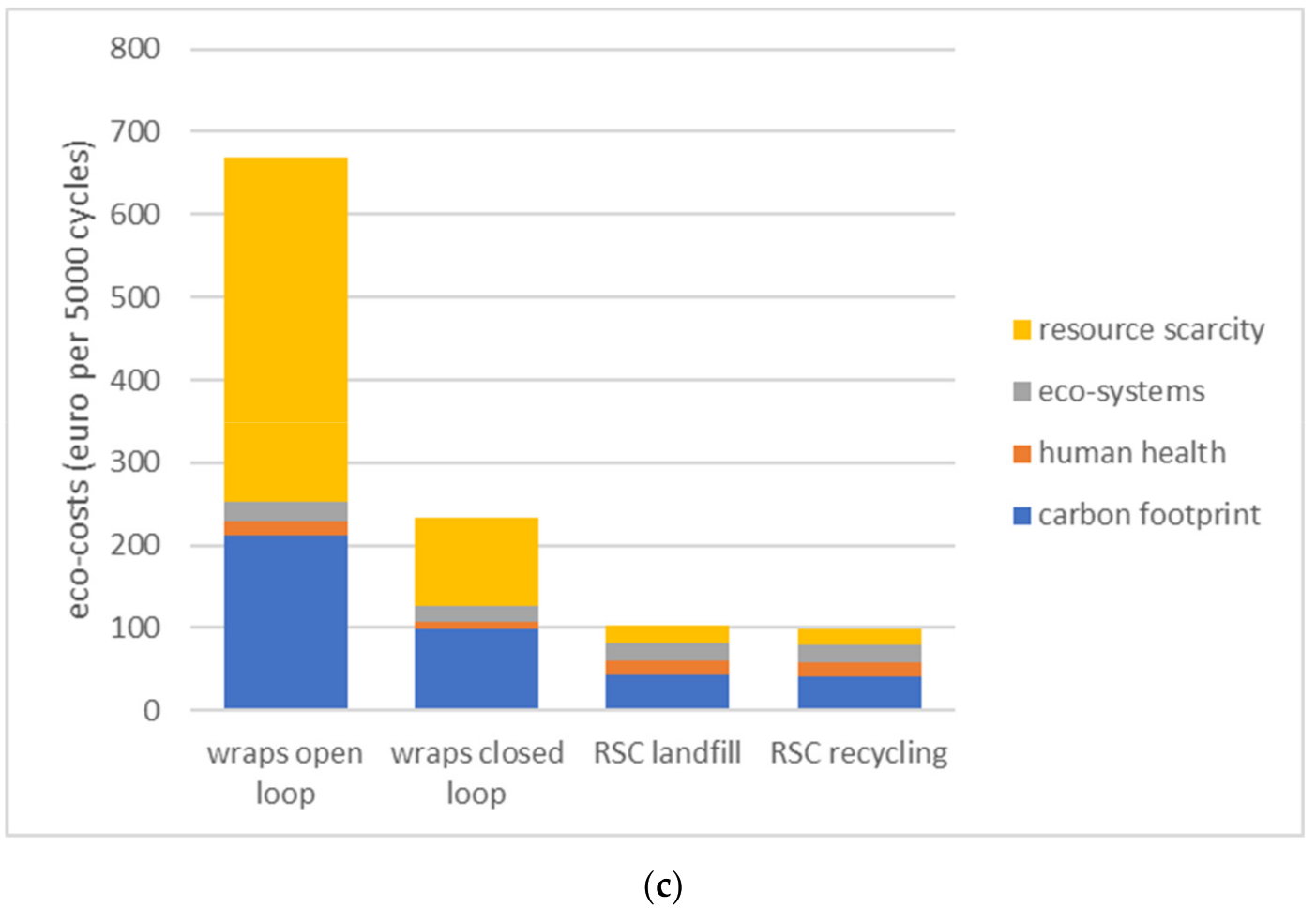
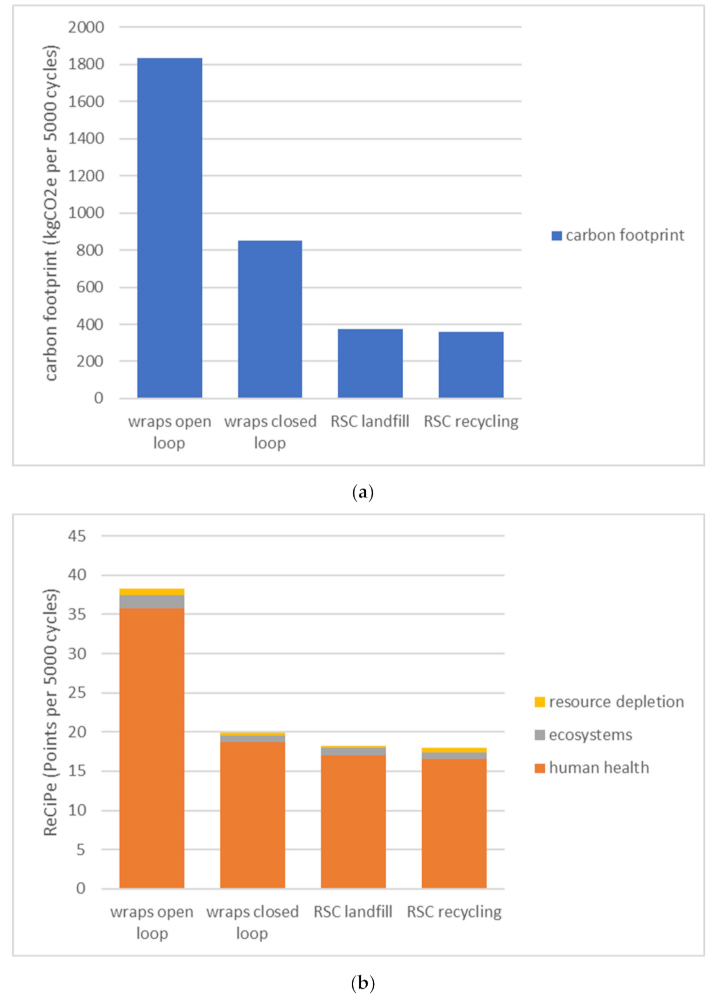
3.1. The Environmental Gain for 5000 Cycles (Research Question A)
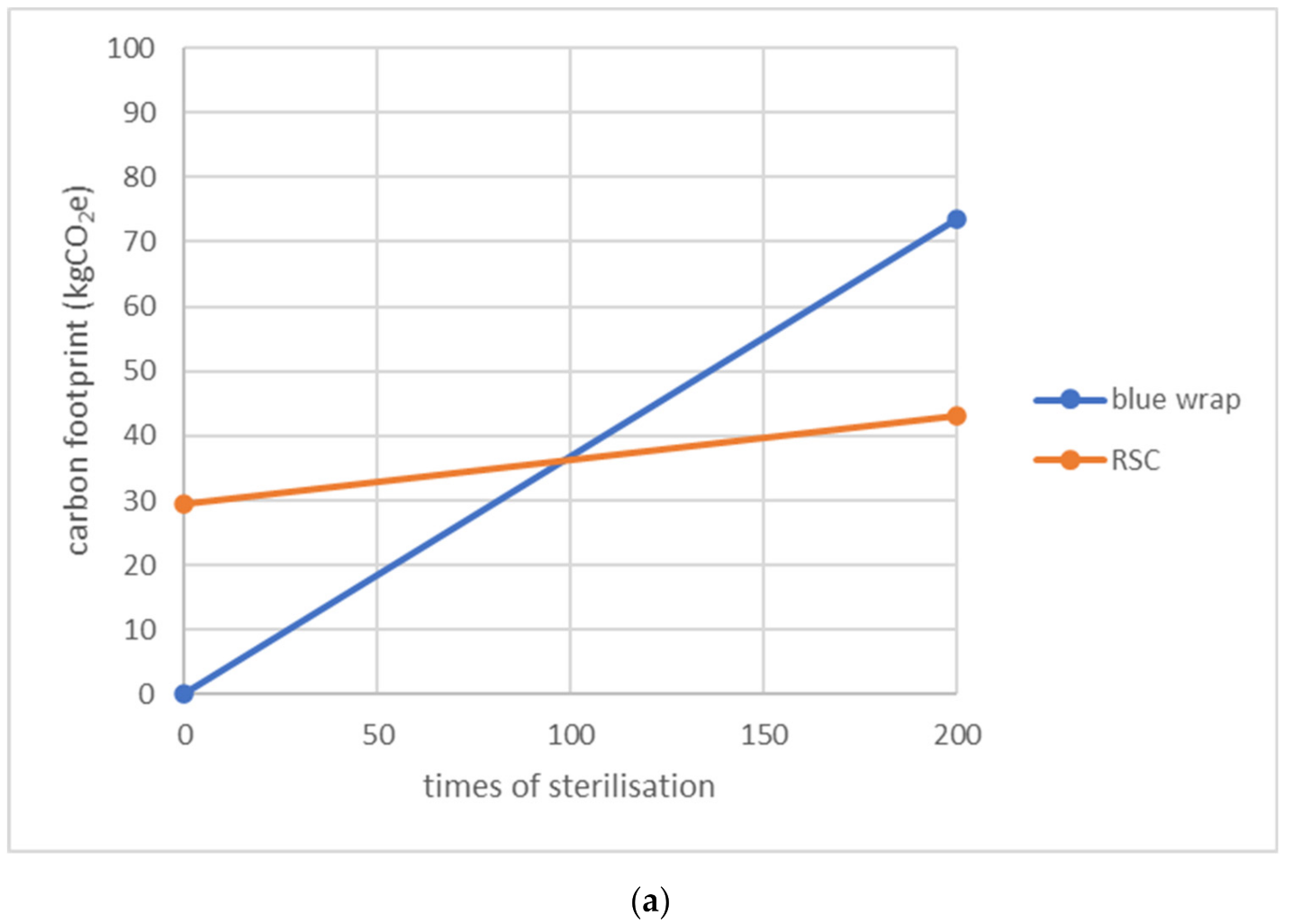
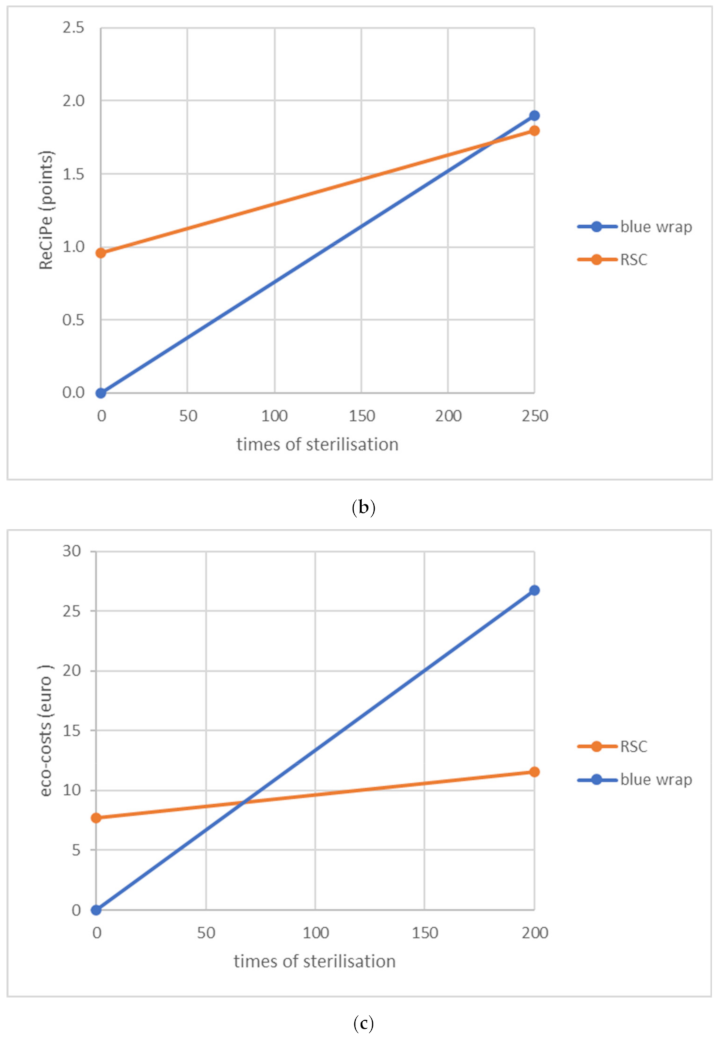
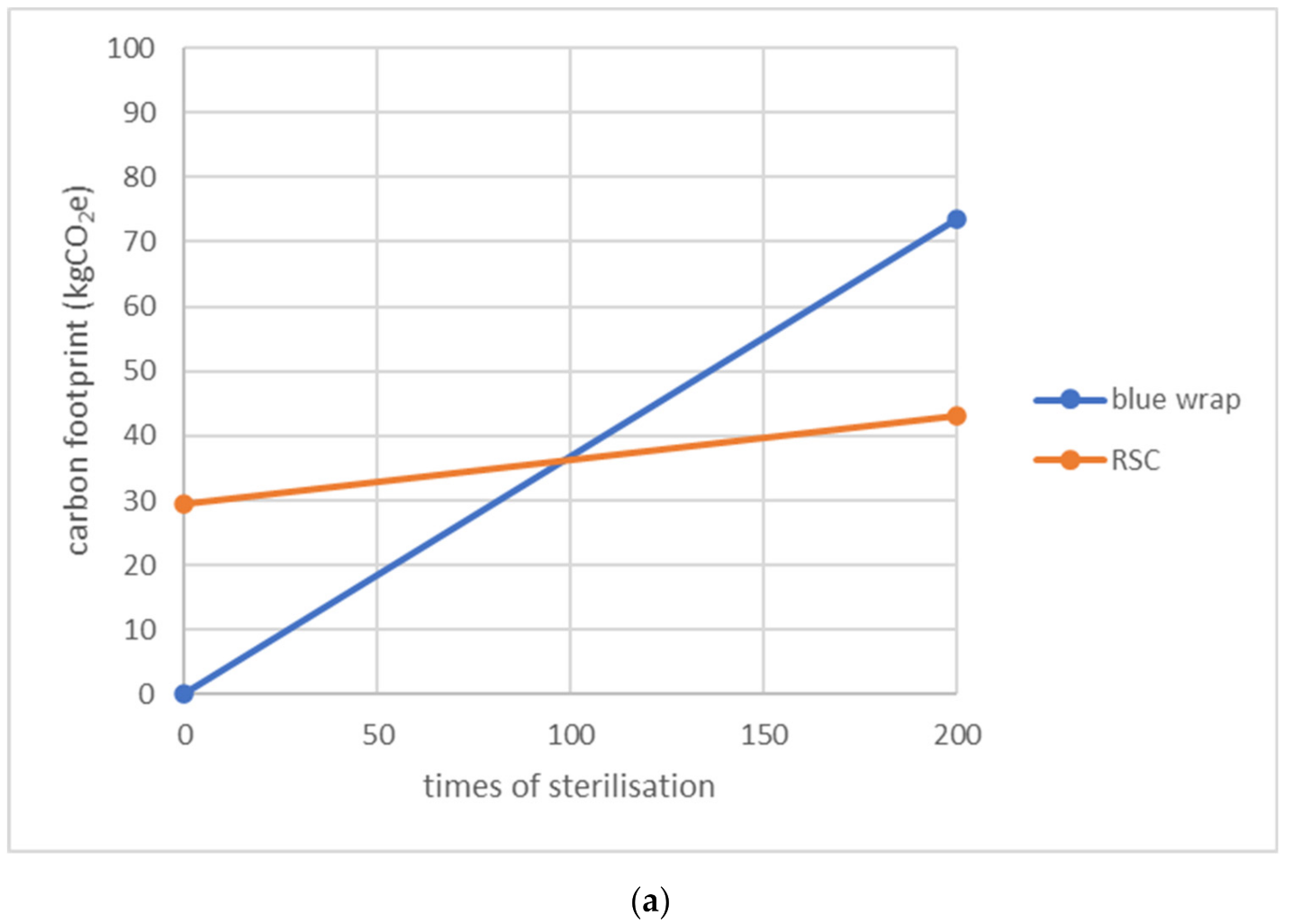
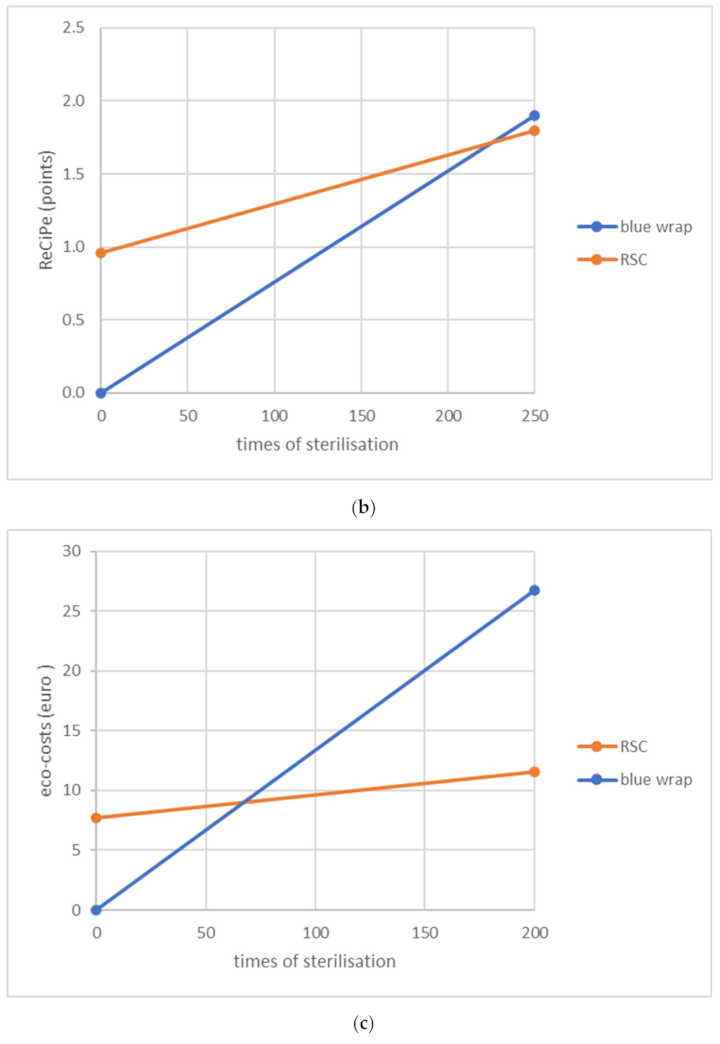
3.2. The Break-Even Points of Both Packaging Systems (Research Question B)
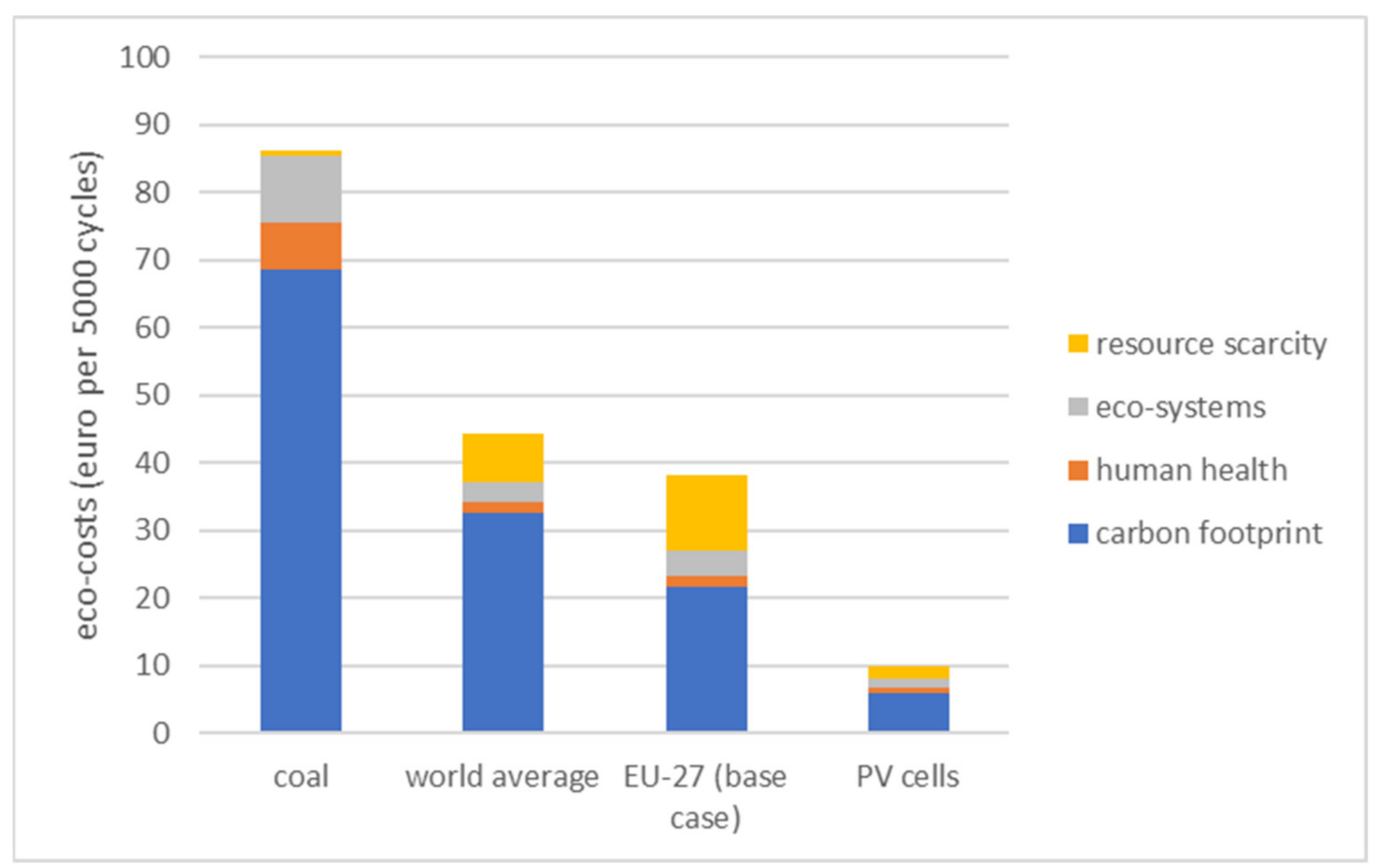
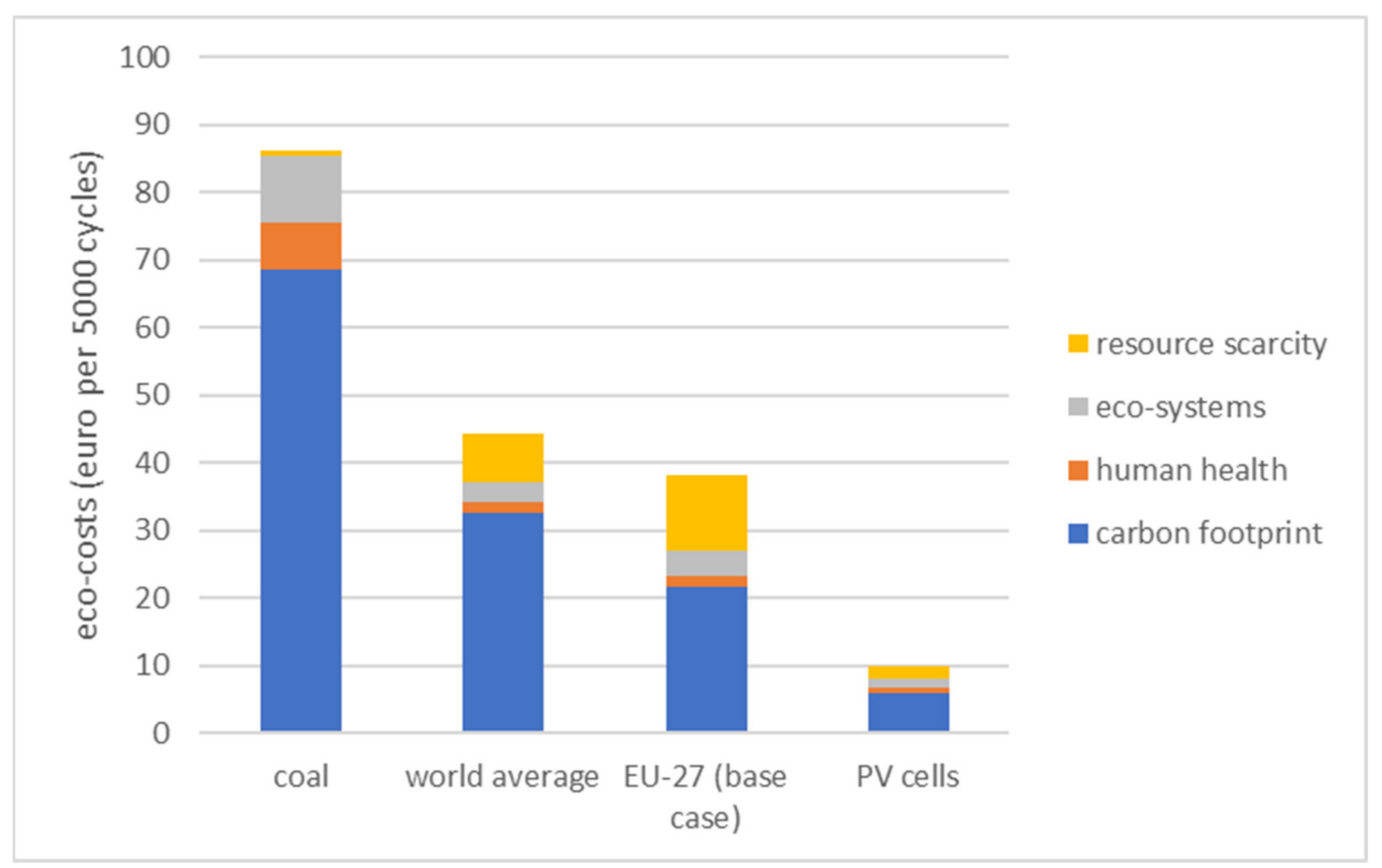
3.3. Alternative Scenarios for Electricity of the Use-Phase (Sterilization and Washing)
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A. Key Data for LCA
- − declared unit: 5000 blue wraps
- − transport: production site in Lexington, North Carolina, USA; use phase in Leiden, The Netherlands
- − open loop (cradle-to-grave): end-of-life is municipal waste incineration (in the region of the hospital)
- − closed loop (cradle-to-cradle): upcycled at the production location, transport back to North Carolina
- − weight of 5000 wraps: 457 kg
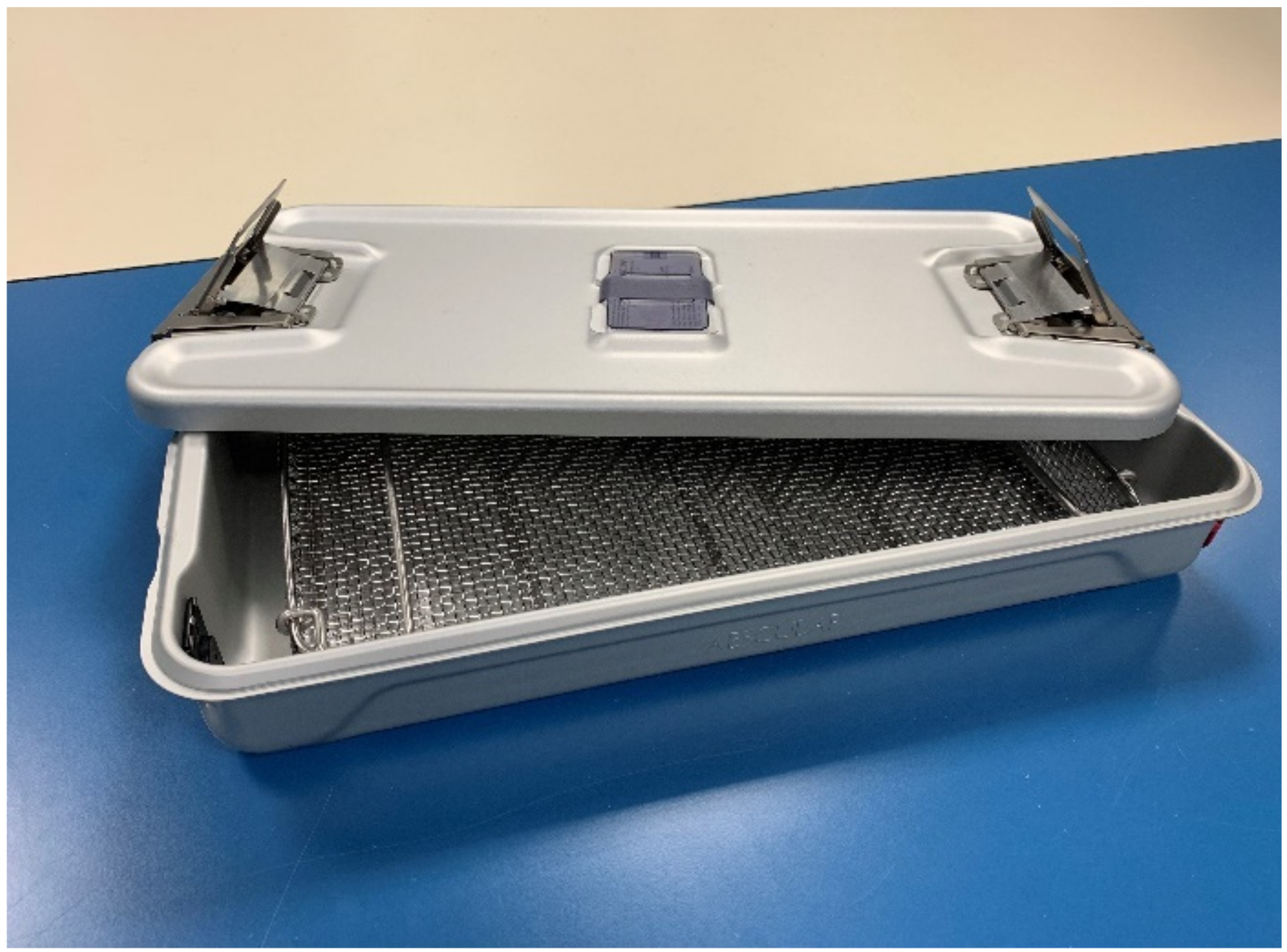
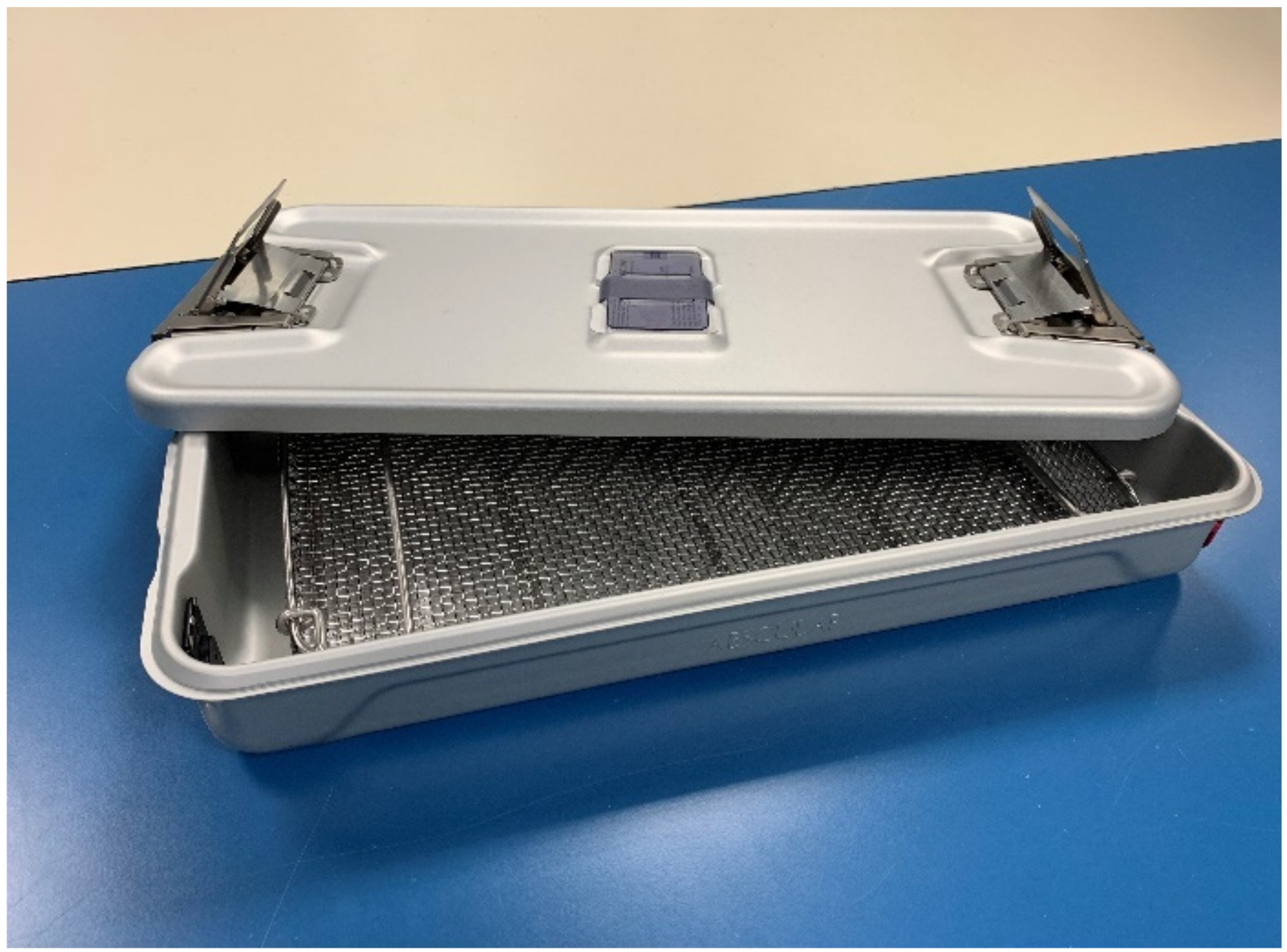
- − declared unit: 1 container, lifespan 5000 sterilization cycles
- − transport: production site in Tuttlinge, Germany; use phase in Leiden, The Netherlands
- − open loop (cradle to grave): end-of life is land fill
- − closed loop (cradle-to-cradle): upcycling
- − total weight of 1 box: 3.41 kg (AL 2.63 kg, SS 316L 0.49 kg, PTFE 0.24 kg, PDMS 0.05 kg)
Appendix B. Tables for Hot-Spot Analyses in Eco-Costs

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cradle-to-Grave 5000 Blue Wraps ‘Open Loop’ | Total | Climate Change | Human Health | Eco-Systems | Resource Depletion |
|---|---|---|---|---|---|
| production | 590.09 | 136.75 | 19.71 | 27.54 | 406.09 |
| transport | 25.59 | 10.15 | 0.87 | 3.19 | 11.38 |
| use-phase | 1.97 | 1.12 | 0.08 | 0.20 | 0.58 |
| end-of-life incineration | 51.46 | 64.87 | −5.16 | −7.20 | −1.04 |
| total | 669.11 | 212.88 | 15.50 | 23.73 | 417.00 |
| Hotspot ‘Production’ 5000 Blue Wrap ‘Open Loop’ | Total | Climate Change | Human Health | Eco-Systems | Resource Depletion |
|---|---|---|---|---|---|
| PP (polypropylene), 456.85 kg | 485.69 | 86.61 | 16.03 | 17.31 | 365.75 |
| extrusion, 456.85 kg | 9.10 | 6.73 | 0.29 | 0.64 | 1.44 |
| spinning first layer, 152.28 kg | 21.54 | 15.92 | 0.69 | 1.52 | 3.41 |
| thermo forming, 152.28 kg | 5.34 | 3.95 | 0.17 | 0.38 | 0.85 |
| spinning 2nd layer, 152.28 kg | 21.54 | 15.92 | 0.69 | 1.52 | 3.41 |
| Pigments, 14.13 kg | 46.89 | 7.64 | 1.85 | 6.17 | 31.24 |
| total | 590.09 | 136.75 | 19.71 | 27.54 | 406.09 |
| Cradle-to-Cradle 5000 Blue Wrap ‘Closed Loop’ | Total | Climate Change | Human Health | Eco-Systems | Resource Depletion |
|---|---|---|---|---|---|
| production | 179.54 | 77.10 | 6.19 | 13.86 | 82.38 |
| transport | 25.59 | 10.15 | 0.87 | 3.19 | 11.38 |
| use-phase | 1.97 | 1.12 | 0.08 | 0.20 | 0.58 |
| end-of-life return | 25.59 | 10.15 | 0.87 | 3.19 | 11.38 |
| total | 232.68 | 98.51 | 8.01 | 20.44 | 105.72 |
| Hotspot ‘Production’ 5000 Blue Wraps ‘Closed Loop’ | Total | Climate Change | Human Health | Eco-Systems | Resource Depletion |
|---|---|---|---|---|---|
| mechanical rec. PP, 411.17 kg | 26.57 | 18.30 | 0.91 | 1.89 | 5.47 |
| extrusion, 456.85 kg | 9.10 | 6.73 | 0.29 | 0.64 | 1.44 |
| spinning first layer, 152.28 kg | 21.54 | 15.92 | 0.69 | 1.52 | 3.41 |
| thermo forming, 152.28 kg | 5.34 | 3.95 | 0.17 | 0.38 | 0.85 |
| spinning 2nd layer, 152.28 kg | 21.54 | 15.92 | 0.69 | 1.52 | 3.41 |
| Pigments, 14.13 kg | 46.89 | 7.64 | 1.85 | 6.17 | 31.24 |
| PP (olypropylene), 45.68 kg | 48.56 | 8.66 | 1.60 | 1.73 | 36.57 |
| total | 179.54 | 77.10 | 6.19 | 13.86 | 82.38 |
| RSC B.Braun ‘Open Loop’ (Landfill) | Total | Climate Change | Human Health | Eco-Systems | Resource Depletion |
|---|---|---|---|---|---|
| production | 7.58 | 3.35 | 0.23 | 0.97 | 3.04 |
| transport | 0.12 | 0.05 | 0.01 | 0.01 | 0.06 |
| use phase | 96.31 | 39.92 | 16.01 | 22.22 | 18.16 |
| end-of-life landfill | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
| total | 104.02 | 43.32 | 16.25 | 23.20 | 21.26 |
| RSC B.Braun Hotspot ‘Use Phase’ | Total | Climate Change | Human Health | Eco-Systems | Resource Depletion |
|---|---|---|---|---|---|
| ultrapure water, 5312.5 kg | 10.37 | 1.84 | 1.10 | 6.46 | 0.97 |
| deionised water, 115625 kg | 15.93 | 5.90 | 3.31 | 3.86 | 2.86 |
| xHelematic cleaner, 106.25 kg | 31.80 | 10.44 | 10.15 | 8.05 | 3.16 |
| electricity EU-27, 1996 MJ | 38.21 | 21.74 | 1.46 | 3.85 | 11.17 |
| total | 96.31 | 39.92 | 16.01 | 22.22 | 18.16 |
References
- Pichler, P.P.; Jaccard, I.S.; Weisz, U.; Weisz, H. International comparison of health care carbon footprints. Environ. Res. Lett. 2019, 14, 064004. [Google Scholar] [CrossRef] [Green Version]
- Eckelman, M.J.; Sherman, J.D. Estimated Global Disease Burden From US Health Care Sector Greenhouse Gas Emissions. Am. J. Public Health 2018, 108, S120–S122. [Google Scholar] [CrossRef] [PubMed]
- Eckelman, M.J.; Sherman, J. Environmental Impacts of the US. Health Care System and Effects on Public Health. PLoS ONE 2016, 11, e0157014. [Google Scholar] [CrossRef] [Green Version]
- MacNeill, A.J.; Lillywhite, R.; Brown, C.J. The impact of surgery on global climate: A carbon footprinting study of operating theatres in three health systems. Lancet Planet Health 2017, 1, e381–e388. [Google Scholar] [CrossRef] [Green Version]
- McGain, E.; Hendel, S.A.; Story, D.A. An audit of potentially recyclable waste from anaesthetic practice. Anaesth. Intensive Care 2009, 37, 820–823. [Google Scholar] [CrossRef] [Green Version]
- McGain, F.; Jarosz, K.M.; Nguyen, M.N.; Bates, S.; O’Shea, C.J. Auditing Operating Room Recycling: A Management Case Report. A A Case Rep. 2015, 5, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Azouz, S.; Boyll, P.; Swanson, M.; Castel, N.; Maffi, T.; Rebecca, A.M. Managing barriers to recycling in the operating room. Am. J. Surg. 2019, 217, 634–638. [Google Scholar] [CrossRef]
- Kagoma, Y.; Stall, N.; Rubinstein, E.; Naudie, D. People, planet and profits: The case for greening operating rooms. CMAJ 2012, 184, 1905–1911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wyssusek, K.H.; Keys, M.T.; van Zundert, A.A.J. Operating room greening initiatives—The old, the new, and the way forward: A narrative review. Waste Manag. Res. 2019, 37, 3–19. [Google Scholar] [CrossRef]
- Sustainable Healthcare Waste Management in the EU Circular Economy Model. Available online: https://noharm-europe.org/documents/sustainable-healthcare-waste-management-eu-circular-economy-model (accessed on 30 December 2021).
- Guetter, C.R.; Williams, B.J.; Slama, E.; Arrington, A.; Henry, M.C.; Moller, M.G.; Tuttle-Newhall, J.E.; Stein, S.; Crandall, M. Greening the operating room. Am. J. Surg. 2018, 216, 683–688. [Google Scholar] [CrossRef]
- Joseph, B.; James, J.; Kalarikkal, N.; Thomas, S. Recycling of medical plastics. Adv. Ind. Eng. Polym. Res. 2021, 4, 199–208. [Google Scholar] [CrossRef]
- Rigid Sterilization Containers in the OR. Available online: https://practicegreenhealth.org/sites/default/files/upload-files/gorimpmod-rigidsterilcont_r5_web_0.pdf (accessed on 30 December 2021).
- Single-Use Sterilization Wraps Market: Global Industry Analysis 2013–2017 and Opportunity Assessment 2018–2028. Available online: https://www.futuremarketinsights.com/reports/single-use-sterilization-wraps-market (accessed on 9 June 2020).
- Krohn, M.; Fengler, J.; Mickley, T.; Flessa, S. Analysis of processes and costs of alternative packaging options of sterile goods in hospitals—A case study in two German hospitals. Health Econ. Rev. 2019, 9, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Overcash, M. A comparison of reusable and disposable perioperative textiles: Sustainability state-of-the-art 2012. Anesth. Analg. 2012, 114, 1055–1066. [Google Scholar] [CrossRef] [PubMed]
- Vozzola, E.; Overcash, M.; Griffing, E. Environmental considerations in the selection of isolation gowns: A life cycle assessment of reusable and disposable alternatives. Am. J. Infect. Control 2018, 46, 881–886. [Google Scholar] [CrossRef] [Green Version]
- Vozzola, E.; Overcash, M.; Griffing, E. An Environmental Analysis of Reusable and Disposable Surgical Gowns. AORN J. 2020, 111, 315–325. [Google Scholar] [CrossRef]
- Ibbotson, S.; Dettmer, T.; Kara, S.; Herrmann, C. Eco-efficiency of disposable and reusable surgical instruments—A scissors case. Int. J. Life Cycle Assess. 2013, 18, 1137–1148. [Google Scholar] [CrossRef]
- McGain, F.; McAlister, S.; McGavin, A.; Story, D. The financial and environmental costs of reusable and single-use plastic anaesthetic drug trays. Anaesth. Intensive Care 2010, 38, 538–544. [Google Scholar] [CrossRef] [Green Version]
- McGain, F.; McAlister, S.; McGavin, A.; Story, D. A life cycle assessment of reusable and single-use central venous catheter insertion kits. Anesth. Analg. 2012, 114, 1073–1080. [Google Scholar] [CrossRef]
- Eckelman, M.; Mosher, M.; Gonzalez, A.; Sherman, J. Comparative life cycle assessment of disposable and reusable laryngeal mask airways. Anesth. Analg. 2012, 114, 1067–1072. [Google Scholar] [CrossRef]
- Sherman, J.D.; Raibley, L.A.t.; Eckelman, M.J. Life Cycle Assessment and Costing Methods for Device Procurement: Comparing Reusable and Single-Use Disposable Laryngoscopes. Anesth. Analg. 2018, 127, 434–443. [Google Scholar] [CrossRef]
- Olindo, R.; Schmitt, N.; Vogtländer, J. Life Cycle Assessments on Battery Electric Vehicles and Electrolytic Hydrogen: The Need for Calculation Rules and Better Databases on Electricity. Sustainability 2021, 13, 5250. [Google Scholar] [CrossRef]
- Kägi, T.; Dinkel, F.; Frischknecht, R.; Humbert, S.; Lindberg, J.; Mester, S.; Ponsioen, T.; Sala, S.; Schenker, U. Session “Midpoint, endpoint or single score for decision-making?”—SETAC Europe 25th Annual Meeting, May 5th, 2015. Int. J. Life Cycle Assess. 2015, 21, 129–132. [Google Scholar] [CrossRef]
- Sala, S.; Cerutti, A.; Pant, R. Development of a weighting approach for the Environmental Footprint; EUR 28562 EN; Publications Office of the European Union: Luxembourg, 2017. [Google Scholar] [CrossRef]
- Huijbregts, M.A.J.; Steinmann, Z.J.N.; Elshout, P.M.F.; Stam, G.; Verones, F.; Vieira, M.; Zijp, M.; Hollander, A.; van Zelm, R. ReCiPe2016: A harmonised life cycle impact assessment method at midpoint and endpoint level. Int. J. Life Cycle Assess. 2017, 22, 138–147. [Google Scholar] [CrossRef]
- ISO 14008:2019; Monetary Valuation of Environmental Impacts and Related Environmental Aspects; International Organization for Standardization: Geneva, Switzerland. 2019. Available online: https://www.iso.org/standard/43243.html (accessed on 2 November 2021).
- Vogtländer, J.G. A Practical Guide to LCA for Students Designers and Business Managers: Cradle-to-Grave and Cradle-to-Cradle, 5th ed.; Delft Academic Press: Delft, The Netherlands, 2017. [Google Scholar]
- The Model of the Eco-Costs/Value Ratio (EVR). Available online: https://www.ecocostsvalue.com/index.html (accessed on 26 May 2020).
- McGain, F.; Moore, G.; Black, J. Steam sterilisation’s energy and water footprint. Aust. Health Rev. 2017, 41, 26–32. [Google Scholar] [CrossRef]
- Babu, M.A.; Dalenberg, A.K.; Goodsell, G.; Holloway, A.B.; Belau, M.M.; Link, M.J. Greening the Operating Room: Results of a Scalable Initiative to Reduce Waste and Recover Supply Costs. Neurosurgery 2019, 85, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Link, T. Guidelines in Practice: Sterilization Packaging Systems. AORN J. 2020, 112, 248–260. [Google Scholar] [CrossRef]
- Waked, W.R.; Simpson, A.K.; Miller, C.P.; Magit, D.P.; Grauer, J.N. Sterilization Wrap Inspections Do Not Adequately Evaluate Instrument Sterility. Clin. Orthop. Relat. Res. 2007, 462, 207–211. [Google Scholar] [CrossRef]
- Rashidifard, C.H.; Mayassi, H.A.; Bush, C.M.; Opalacz, B.M.; Richardson, M.W.; Muccino, P.M.; DiPasquale, T.G. Looking for Holes in Sterile Wrapping: How Accurate Are We? Clin. Orthop. Relat. Res. 2018, 476, 1076–1080. [Google Scholar] [CrossRef]
- Solomon, C.G.; LaRocque, R.C. Climate Change—A Health Emergency. N. Engl. J. Med. 2019, 380, 209–211. [Google Scholar] [CrossRef]
- Sherman, J.D.; Hopf, H.W. Balancing Infection Control and Environmental Protection as a Matter of Patient Safety: The Case of Laryngoscope Handles. Anesth. Analg. 2018, 127, 576–579. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Friedericy, H.J.; van Egmond, C.W.; Vogtländer, J.G.; van der Eijk, A.C.; Jansen, F.W. Reducing the Environmental Impact of Sterilization Packaging for Surgical Instruments in the Operating Room: A Comparative Life Cycle Assessment of Disposable versus Reusable Systems. Sustainability 2022, 14, 430. https://doi.org/10.3390/su14010430
Friedericy HJ, van Egmond CW, Vogtländer JG, van der Eijk AC, Jansen FW. Reducing the Environmental Impact of Sterilization Packaging for Surgical Instruments in the Operating Room: A Comparative Life Cycle Assessment of Disposable versus Reusable Systems. Sustainability. 2022; 14(1):430. https://doi.org/10.3390/su14010430
Chicago/Turabian StyleFriedericy, Herman J., Cas W. van Egmond, Joost G. Vogtländer, Anne C. van der Eijk, and Frank Willem Jansen. 2022. "Reducing the Environmental Impact of Sterilization Packaging for Surgical Instruments in the Operating Room: A Comparative Life Cycle Assessment of Disposable versus Reusable Systems" Sustainability 14, no. 1: 430. https://doi.org/10.3390/su14010430
APA StyleFriedericy, H. J., van Egmond, C. W., Vogtländer, J. G., van der Eijk, A. C., & Jansen, F. W. (2022). Reducing the Environmental Impact of Sterilization Packaging for Surgical Instruments in the Operating Room: A Comparative Life Cycle Assessment of Disposable versus Reusable Systems. Sustainability, 14(1), 430. https://doi.org/10.3390/su14010430