
Sustainable Harm Reduction Needle and Syringe Programs for People Who Inject Drugs: A Scoping Review of Their Implementation Qualities



Abstract
1. Introduction
1.1. Harm Reduction Approaches: Sustainable Implementation Considerations
1.2. Health Policy Frameworks
1.3. Implementation Study Framework
1.4. Goal of the Review
Objectives
2. Materials and Methods
2.1. Search Strategy for Identification of Studies
2.1.1. Eligibility Criteria
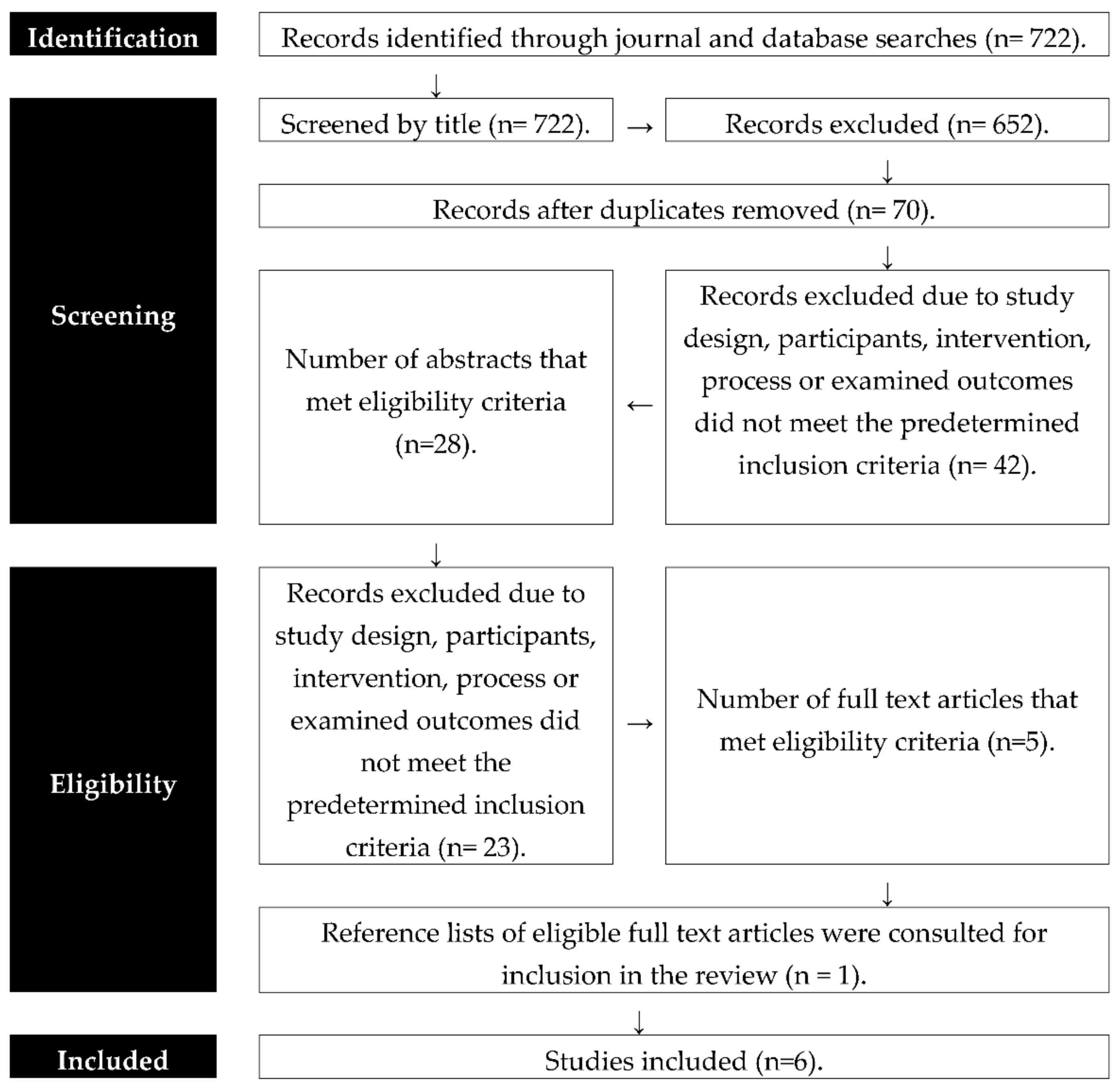
2.1.2. Search Tree Procedure and Outcomes
2.2. Data Extraction and Management
2.3. Data Analysis and Synthesis
3. Results and Discussion
3.1. Implementers and Internal Setting Factors of Sustainable NSPs
3.2. Sustainable Implementation Process and Characteristics
3.3. Sustainable NSP External Setting Characteristics
3.4. Implementation Determinants Interaction Factors
3.5. Implications for NSP Implementation Sustainability Research and Practice
3.6. Limitations of the Applicability of Evidence
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Peacock, A.; Leung, J.; Larney, S.; Colledge, S.; Hickman, M.; Rehm, J.; Giovino, G.A.; West, R.; Hall, W.; Griffiths, P.; et al. Global statistics on alcohol, tobacco and illicit drug use: 2017 status report. Addiction 2018, 113, 1905–1926. [Google Scholar] [CrossRef] [PubMed]
- United Nations Office on Drugs and Crime. World Drug Report 2016; United Nations: New York, NY, USA, 2016; ISBN 978-92-1-148286-7. [Google Scholar]
- Brandon, T.H.; Vidrine, J.I.; Litvin, E.B. Relapse and Relapse Prevention. Annu. Rev. Clin. Psychol. 2007, 3, 257–284. [Google Scholar] [CrossRef] [PubMed]
- Tran, B.X.; Moir, M.; Latkin, C.A.; Hall, B.J.; Nguyen, C.T.; Ha, G.H.; Nguyen, N.B.; Ho, C.S.H.; Ho, R.C.M. Global research mapping of substance use disorder and treatment 1971–2017: Implications for priority setting. Subst. Abus. Treat. Prev. Policy 2019, 14, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Watts, J.; MacDaniels, B.; Rivera, S.; Resiak, D.; Mpofu, E.; Redwine, S. Community Substance Use Safety; Mpofu, E., Ed.; Palgrave/Macmillan: New York, NY, USA, 2020. [Google Scholar]
- Toward Sustainable Transitions in Healthcare Systems; Routledge: London, UK, 2017.
- Shelton, R.C.; Cooper, B.R.; Stirman, S.W. The sustainability of evidence-based interventions and practices in public health and health care. Annu. Rev. Public Health 2018, 39, 55–76. [Google Scholar] [CrossRef]
- Wodak, A.; McLeod, L. The role of harm reduction in controlling HIV among injecting drug users. AIDS 2008, 22, S81. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, T.; Hedrich, D. Harm reduction and the mainstream. In Harm Reduction: Evidence, Impacts and Challenges; Rhodes, T., Hedrich, D., Eds.; MONOGRAPHS: Lisbon, Portugal, 2010. [Google Scholar]
- Ritter, A.; Cameron, J. A review of the efficacy and effectiveness of harm reduction strategies for alcohol, tobacco and illicit drugs. Drug Alcohol Rev. 2006, 25, 611–624. [Google Scholar] [CrossRef]
- Edland-Gryt, M.; Skatvedt, A.H. Thresholds in a low-threshold setting: An empirical study of barriers in a centre for people with drug problems and mental health disorders. Int. J. Drug Policy 2012, 24, 257–264. [Google Scholar] [CrossRef]
- Kwon, A.J.; Anderson, C.J.; Kerr, J.C.; Thein, M.H.-H.; Zhang, G.L.; Iversen, P.J.; Dore, P.G.; Kaldor, P.J.; Law, P.M.; Maher, P.L.; et al. Estimating the cost-effectiveness of needle-syringe programs in Australia. AIDS 2012, 26, 2201–2210. [Google Scholar] [CrossRef] [PubMed]
- Treloar, C.; Rance, J.; Yates, K.; Mao, L. Trust and people who inject drugs: The perspectives of clients and staff of Needle Syringe Programs. Int. J. Drug Policy 2016, 27, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Somlai, A.M.; Kelly, J.A.; Otto-Salaj, L.; Nelson, D. “Lifepoint”: A case study in using social science community identification data to guide the implementation of a needle exchange program. AIDS Educ. Prev. 1999, 11, 187. [Google Scholar]
- Strike, C.; Watson, T.M.; Lavigne, P.; Hopkins, S.; Shore, R.; Young, D.; Leonard, L.; Millson, P. Guidelines for better harm reduction: Evaluating implementation of best practice recommendations for needle and syringe programs (NSPs). Int. J. Drug Policy 2010, 22, 34–40. [Google Scholar] [CrossRef]
- Resiak, D.; Mpofu, E.; Athanasou, J. Drug Treatment Policy in the Criminal Justice System: A Scoping Literature Review. Am. J. Crim. Justice 2016, 41, 3–13. [Google Scholar] [CrossRef]
- World Health Organisation. National Health Policies, Strategies and Plans. Available online: http://www.who.int/nationalpolicies/about/en/ (accessed on 27 February 2017).
- Allen, S.T.; Ruiz, M.S.; O’Rourke, A. The evidence does not speak for itself: The role of research evidence in shaping policy change for the implementation of publicly funded syringe exchange programs in three US cities. Int. J. Drug Policy 2015, 26, 688–695. [Google Scholar] [CrossRef]
- World Health Organisation. National Health Policies, Strategies, and Plans: From Vision to Operation. Available online: http://www.who.int/nationalpolicies/processes/operational/en/ (accessed on 27 February 2017).
- Wallace, B.; van Roode, T.; Pagan, F.; Phillips, P.; Wagner, H.; Calder, S.; Aasen, J.; Pauly, B.; Hore, D. What is needed for implementing drug checking services in the context of the overdose crisis? A qualitative study to explore perspectives of potential service users. Harm Reduct. J. 2020, 17, 29. [Google Scholar] [CrossRef] [PubMed]
- Demiris, G.; Parker Oliver, D.; Capurro, D.; Wittenberg-Lyles, E. Implementation science: Implications for intervention research in hospice and palliative care. Gerontologist 2014, 54, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Bluthenthal, R.N.; Heinzerling, K.G.; Anderson, R.; Flynn, N.M.; Kral, A.H. Approval of Syringe Exchange Programs in California: Results From a Local Approach to HIV Prevention. Am. J. Public Health 2008, 98, 278–283. [Google Scholar] [CrossRef]
- Silverman, B.; Davis, C.S.; Graff, J.; Bhatti, U.; Santos, M.; Beletsky, L. Harmonizing disease prevention and police practice in the implementation of HIV prevention programs: Up-stream strategies from Wilmington, Delaware. Harm Reduct. J. 2012, 9, 17. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Peters, M.D.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid. Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef]
- Goodin, A.; Fallin-Bennett, A.; Green, T.; Freeman, P.R. Pharmacists’ role in harm reduction: A survey assessment of Kentucky community pharmacists’ willingness to participate in syringe/needle exchange. Harm Reduct. J. 2018, 15, 4. [Google Scholar] [CrossRef] [PubMed]
- Ngo, A.D.; Schmich, L.; Higgs, P.; Fischer, A. Qualitative evaluation of a peer-based needle syringe programme in Vietnam. Int. J. Drug Policy 2007, 20, 179–182. [Google Scholar] [CrossRef] [PubMed]
- White, B.; Haber, P.S.; Day, C.A. Community attitudes towards harm reduction services and a newly established needle and syringe automatic dispensing machine in an inner-city area of Sydney, Australia. Int. J. Drug Policy 2015, 27, 121–126. [Google Scholar] [CrossRef]
- Downing, M.; Riess, T.H.; Vernon, K.; Mulia, N.; Hollinquest, M.; McKnight, C.; Jarlais, D.C.D.; Edlin, B.R. What’s Community Got to Do with It? Implementation Models of Syringe Exchange Programs. AIDS Educ. Prev. 2005, 17, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Saso, S.; Panesar, S.S.; Siow, W.; Athanasiou, T. Systematic Review and Meta-analysis in Clinical Practice. In Evidence Synthesis in Healthcare: A Practical Handbook for Clinicians; Darzi, A., Athanasiou, T., Eds.; Springer: London, UK, 2011; pp. 67–113. [Google Scholar]
- Louie, E.; Barrett, E.L.; Baillie, A.; Haber, P.; Morley, K.C. Implementation of evidence-based practice for alcohol and substance use disorders: Protocol for systematic review. Syst. Rev. 2020, 9, 25–26. [Google Scholar] [CrossRef] [PubMed]
- Clark, F. Global drug policy fuels hepatitis C epidemic, report warns. Lancet 2013, 381, 1891. [Google Scholar] [CrossRef]
- Mathers, B.M.; Degenhardt, L.; Phillips, B.; Wiessing, L.; Hickman, M.; Strathdee, S.A.; Wodak, A.; Panda, S.; Tyndall, M.; Toufik, A.; et al. Global epidemiology of injecting drug use and HIV among people who inject drugs: A systematic review. Lancet 2008, 372, 1733–1745. [Google Scholar] [CrossRef]
- Naserirad, M.; Beulaygue, I.C. Accessibility of Needle and Syringe Programs and Injecting and Sharing Risk Behaviors in High Hepatitis C Virus Prevalence Settings. Subst. Use Misuse 2020, 55, 1–9. [Google Scholar] [CrossRef]
- World Health Organization. WHO, UNODC, UNAIDS Technical Guide for Countries to Set Targets for Universal Access to HIV Prevention, Treatment and Care for Injecting Drug Users–2012 Revision; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Iversen, J.; Grebely, J.; Topp, L.; Wand, H.; Dore, G.; Maher, L. Uptake of hepatitis C treatment among people who inject drugs attending Needle and Syringe Programs in Australia, 1999–2011. J. Viral Hepat. 2014, 21, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Aspinall, E.J.; Nambiar, D.; Goldberg, D.J.; Hickman, M.; Weir, A.; Van Velzen, E.; Palmateer, N.; Doyle, J.S.; Hellard, M.E.; Hutchinson, S.J. Are needle and syringe programmes associated with a reduction in HIV transmission among people who inject drugs: A systematic review and meta-analysis. Int. J. Epidemiol. 2014, 43, 235–248. [Google Scholar] [CrossRef] [PubMed]
- Vuong, Q.-H.; Ho, T.-M.; Nguyen, H.-K.; Vuong, T.-T. Healthcare consumers’ sensitivity to costs: A reflection on behavioural economics from an emerging market. Palgrave Commun. 2018, 4, 1–10. [Google Scholar] [CrossRef]
- Torgerson, C.J. Publication Bias: The achilles’ heel of systematic reviews? Br. J. Educ. Stud. 2006, 54, 89–102. [Google Scholar] [CrossRef]


{kind=link}
| Topic | Key Words/Phrases Searched | CFIR Criteria |
|---|---|---|
| Needle and syringe program/Syringe (exchange program implementation) | Needle and syringe program, AND implementation, AND people who inject drugs, OR implementation science, addiction, dependence OR sustainable needle and syringe, program characteristics, AND community, health policy, accessibility, feasibility, affordability, cost evaluation. | (1) Service delivery (e.g., their knowledge and beliefs about the intervention), (2) Internal organization setting (e.g., leadership engagement), (3) Implementation processes (e.g., executing the innovation), (4) Program/intervention characteristics (e.g., complexity, accessibility, quality, affordability and acceptability) (5) the external setting (client needs and resources). |
| Needle and Syringe program/Syringe protocols. | Harm minimization, OR harm reduction, dependency, addiction, substance use disorder, AND individual characteristics, long-term, adherence, fidelity, AND regulations, providers, sites. |
| Variable | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Study Design | Empirical studies. | Literature reviews and studies that were not peer-reviewed. |
| Publication Years | 2000—present. | Published prior to the year 2000. |
| Participants | People who inject drugs, needle and syringe service providers and related stakeholders inclusive of community members, policymakers, and police. | Participants who could not be identified as either a needle and syringe program implementer, member of an NSP internal setting or external setting. |
| Intervention | Needle and syringe program/syringe exchange program implementation and evaluation. | Other harm reduction programs inclusive of; opioid substitution treatments and medically supervised injecting centers/drug consumption rooms. |
| Process | Description of implementation protocol, process evaluation procedure. | Missing details on implementation protocol. |
| Outcomes | Sustainable needle and syringe program implementation characteristics relating to implementers, inner setting, implementation process, intervention characteristics or outer setting. | Sustainable implementation characteristics not relating to the implementation of needle and syringe programs. |
| Authorship | Study Design and Objectives | Participants and Context | Sustainability of Implementation Qualities | ||
|---|---|---|---|---|---|
| Implementers and Inner Setting | Implementation Process and Characteristics | External Setting | |||
| [18] | In-depth qualitative interviews examining the historical, social, political, and scientific contexts for the implementation of publicly funded NSPs. | Key stakeholders (policy makers, community stakeholders and advocates) from three US cities; Baltimore, Philadelphia, and Washington. | Sustainable Needle and Syringe program implementation is supported by an implementation willingness of policy makers based on community sentiment. | Community implementation models top down versus community activist impact program sustainability. | Empirical research evidence has a fear and concern mitigating role in driving policy change for the sustainable implementation of NSPs. |
| [26] | Electronic Survey to assess community pharmacists’ willingness to participate in one harm reduction initiative: syringe/needle exchange. | Kentucky community pharmacists with active licenses (n = 827) for NSP services. | Pharmacists were willing to provide NSP services although fewer were willing to dispose of needles/syringes. Agreement with the public health impact of NSPs impacted pharmacist’s willingness for service provision. | Barriers to the sustainable implementation of an NSP were reported to include clientele, ethics surrounding supply of materials for abuse or illegitimate use, company policy conflict, legal concerns, record keeping, time, reputation, supply problems and finding/handling needles. | None identified. |
| [27] | Qualitative study to assesses barriers and effectiveness of NSP’s, effectiveness and barriers across Vietnam. | Key informant interviews (n = 23), focus group discussions (n = 6–8 participants per group) Peer Educators (8 groups) IDU’s (5 groups) Local residents (7 groups), in-depth interviews (n = 8). | Peer Educator led NSP would be more sustainable with higher literacy and retention with NSP programs. | Sterile water ampules were not provided at NSPs due to concerns from implementing partners. Trust building would therefore contribute to sustainable NSP implementation that fosters adequate equipment provision. | Implementation sustainability is improved with law enforcement support and intensive advocacy with community stakeholders, local government, mass organizations and local residents. |
| [28] | Face-to-face survey to examine community-level support for a newly implemented ADM in an inner-city Sydney area known for high levels of drug use. | Local area residents (n = 118) and businesses (n = 35) located within the vicinity of needle and syringe program (NSP) services including the ADM. | Business entities showed greater support for fixed-site NSPs in general comparatively to those situated locally. | Offering extended hours for NSP via ADM would be cost effective. Anonymity for clients may increase sterile injecting equipment use. | Community member support would be important for the sustainability of NSPs. |
| [29] | Qualitative (interviews) to identify factors and conditions that facilitated or deterred the adoption of NSPs. | Key informants (n = 17) from nine U.S. cities. | Program leadership a key facilitator to sustainable implementation of NSPs. and when leaders with access to local power and resources. | NSP program processes that (a) respectful of political and cultural norm sensitivities, and (b) prioritized coalition building and community involvement, would be sustainable. | NSPs would be more successful aligned to community values and public policy. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Resiak, D.; Mpofu, E.; Rothwell, R. Sustainable Harm Reduction Needle and Syringe Programs for People Who Inject Drugs: A Scoping Review of Their Implementation Qualities. Sustainability 2021, 13, 2834. https://doi.org/10.3390/su13052834
Resiak D, Mpofu E, Rothwell R. Sustainable Harm Reduction Needle and Syringe Programs for People Who Inject Drugs: A Scoping Review of Their Implementation Qualities. Sustainability. 2021; 13(5):2834. https://doi.org/10.3390/su13052834
Chicago/Turabian StyleResiak, Danielle, Elias Mpofu, and Rodd Rothwell. 2021. "Sustainable Harm Reduction Needle and Syringe Programs for People Who Inject Drugs: A Scoping Review of Their Implementation Qualities" Sustainability 13, no. 5: 2834. https://doi.org/10.3390/su13052834
APA StyleResiak, D., Mpofu, E., & Rothwell, R. (2021). Sustainable Harm Reduction Needle and Syringe Programs for People Who Inject Drugs: A Scoping Review of Their Implementation Qualities. Sustainability, 13(5), 2834. https://doi.org/10.3390/su13052834