
Managers’ Competences in Private Hospitals for Investment Decisions during the COVID-19 Pandemic




Abstract
1. Introduction
2. Materials and Methods
3. Results
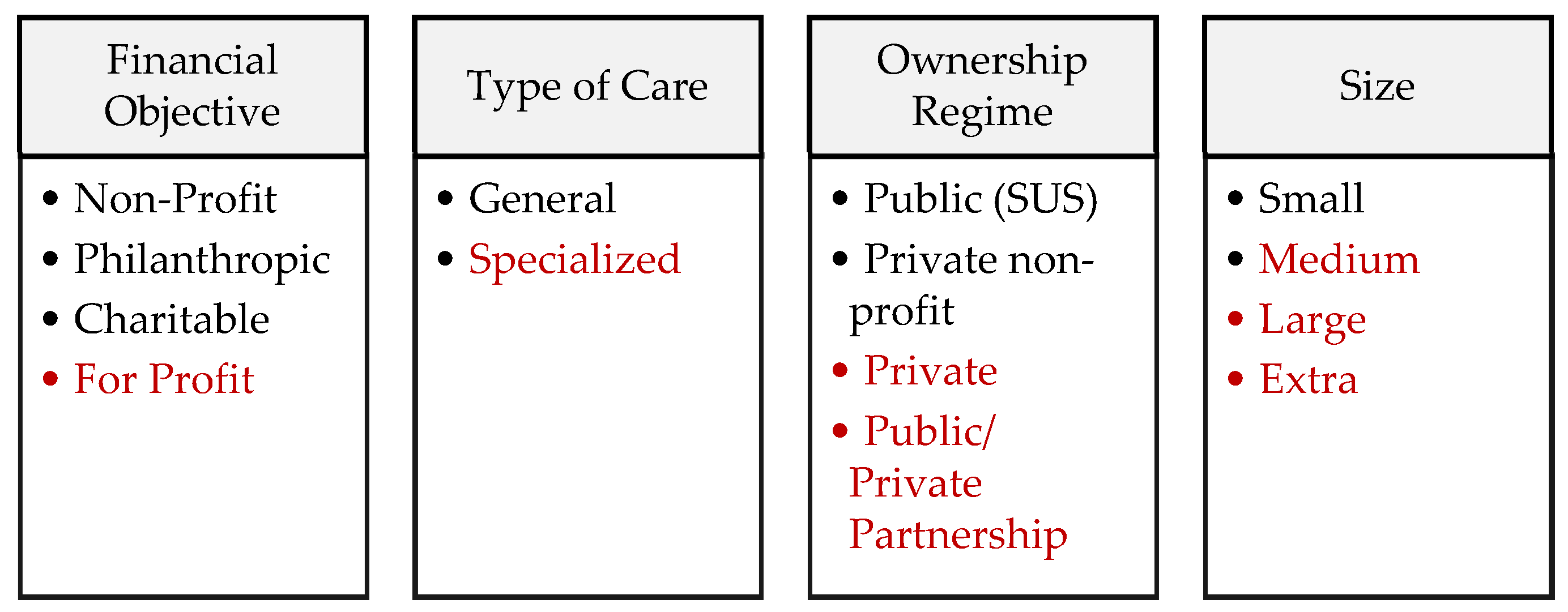
3.1. The National Health Systems Targeted by the Study
3.2. Hospital Characteristics, Manager Profile and Competences
3.3. Governance in Health
3.4. Hospital Financing and Investment
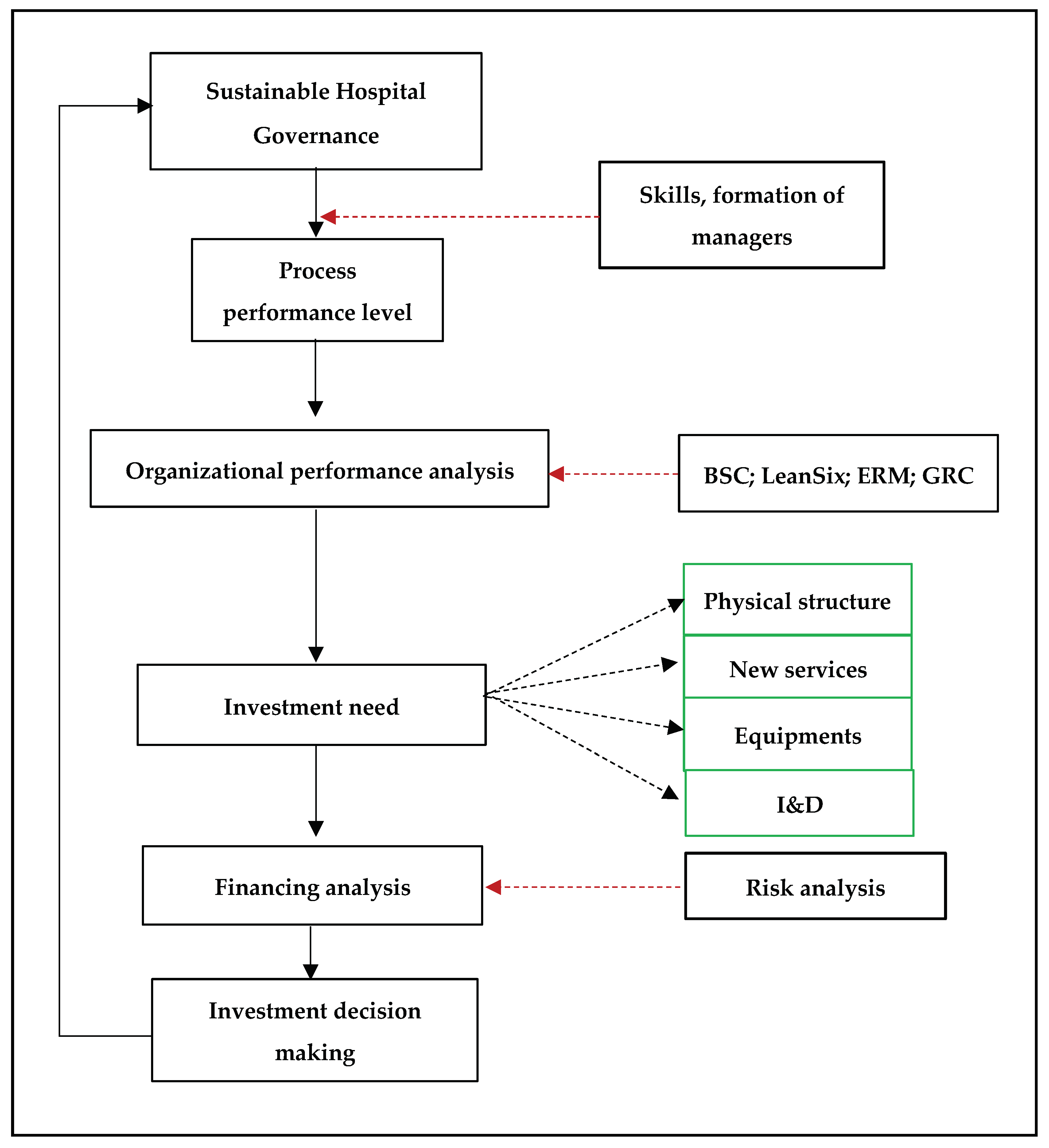
3.5. Performance Analyses and Investment Decision-Making
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- De Marco, A.; Mangano, G.; Cagliano, A.C.; Grimaldi, S. Public Financing into Build-Operate-Transfer Hospital Projects in Italy. J. Constr. Eng. Manag. 2012, 138, 1294–1302. [Google Scholar] [CrossRef]
- Akintoye, A.; Chinyio, E. Private Finance Initiative in the healthcare sector: Trends and risk assessment. Eng. Constr. Arch. Manag. 2005, 12, 601–616. [Google Scholar] [CrossRef]
- Ch, F.N.; Jola, S.P. Bank health level analysis using rbbr in financial services sector—Case in Indonesian stock exchange. Int. J. Econ. Res. 2017, 14, 181–192. [Google Scholar]
- Jizi, M.I.; Nehme, R. Board gender diversity and firms’ equity risk. Equal. Divers. Incl. Int. J. 2017, 36, 590–606. [Google Scholar] [CrossRef]
- Hsu, G.C.M.; Clarkson, P.; Ouyang, A.X. Do biotechnology and health-care firms have poorer continuous disclosure practices as reflected in ASX queries? Account. Res. J. 2019, 32, 88–112. [Google Scholar] [CrossRef]
- World Health Organization. WHO Announces COVID-19 Outbreak a Pandemic. Available online: http://www.euro.who.int/en/healthtopics/healthemergencies/coronaviruscovid19/news/news/2020/3/whoan-nounces-covid-19-outbreak-a-pandemic (accessed on 22 November 2020).
- Stark, P. Advancing Complex Case Management Competencies in a Health Care System. Prof. Case Manag. 2020, 25, 19–25. [Google Scholar] [CrossRef]
- Siskou, O.; Kaitelidou, D.; Papakonstantinou, V.; Liaropoulos, L. Private health expenditure in the Greek health care system: Where truth ends and the myth begins. Health Policy 2008, 88, 282–293. [Google Scholar] [CrossRef]
- Fernandes, A.C.; Nunes, A.M. Hospitals and the public-private combination in the portuguese health system. Acta Med. Port. 2016, 29, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Kakemam, E.; Dargahi, H. Competencies Gap in Hospital Management in Tehran, Iran: A Cross-sectional Survey. J. Health Manag. 2019, 21, 451–464. [Google Scholar] [CrossRef]
- Diaconu, K.; Falconer, J.; Vidal, N.; O’May, F.; Azasi, E.; Elimian, K.; Bou-Orm, I.; Sarb, C.; Witter, S.; Ager, A. Un-derstanding fragility: Implications for global health research and practice. Health Policy Plan. 2020, 35, 235–243. [Google Scholar] [CrossRef]
- Gordon, D.; McKay, S.; Marchildon, G.; Bhatia, R.S.; Shaw, J. Collaborative Governance for Integrated Care: Insights from a Policy Stakeholder Dialogue. Int. J. Integr. Care 2020, 20, 3. [Google Scholar] [CrossRef]
- Cunha, C.L.F.; Moreira, J.P.L.; Oliveira, B.L.C.A.; Bahia, L.; Luiz, R.R. Private health plans and the health of workers in Brazil. Collect. Sci. Health 2019, 24, 1959–1970. [Google Scholar]
- Gandhi, A.V.; Sharma, D. Technical efficiency of private sector hospitals in India using data envelopment analysis. Benchmarking Int. J. 2018, 25, 3570–3591. [Google Scholar] [CrossRef]
- Binci, D.; Belisari, S.; Appolloni, A. BPM and change management: An ambidextrous perspective. Bus. Process Manag. J. 2019, 26, 1–23. [Google Scholar] [CrossRef]
- Bonacci, I.; Mazzitelli, A.; Morea, D. Evaluating Climate between Working Excellence and Organizational Innovation: What Comes First? Sustainability 2020, 12, 3340. [Google Scholar] [CrossRef]
- Almeida, A.S. The role of private non-profit healthcare organizations in NHS systems: Implications for the por-tuguese hospital devolution program. Health Policy 2017, 121, 699–707. [Google Scholar] [CrossRef]
- Paes-Sousa, R.; Schramm, J.M.D.A.; Vilarinho, L. Fiscal austerity and the health sector: The cost of adjustments. Ciência Saúde Coletiva 2019, 24, 4375–4384. [Google Scholar] [CrossRef]
- Prémont, M.-C.; Verbauwhede, C. Canadian legislatures and the regulation of the private health-care industry. Univ. Tor. Law J. 2018, 68, 231–258. [Google Scholar] [CrossRef]
- Department of Informatics of the Unified Health System. DataSUS. Available online: http://www.cns.org.br/links/D_SETOR_DATES.htm (accessed on 1 February 2019).
- Hsieh, H.-F.; Shannon, S.E. Three Approaches to Qualitative Content Analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic analysis: Seeking to meet the reliability criteria. Int. J. Qual. Meth. 2017, 16, 1609406917733847. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Law No. 8,080, of September 19, 1990. Provides for the Conditions for the Promotion, Protection and Recovery of Health, the Organization and Functioning of the Corresponding Services and Provides Other Measures. Available online: http://www.planalto.gov.br/ccivil_03/leis/l8080.htm (accessed on 30 April 2020).
- Paim, J.S.; Travassos, C.; Almeida, C.; Bahia, L.; Macinko, J. The Brazilian health system: History, advances, and challenges. Lancet 2011, 377, 1778–1797. [Google Scholar] [CrossRef]
- Almeida, M.H.T. Federalism, democracy and government in Brazil: Ideas, hypotheses and evidence. Braz. J Bibliogr. Inf. Soc. Sci. BBI 2001, 51, 13–34. [Google Scholar]
- Canada Health Act. Minister of Justice. Available online: http://laws.justice.gc.ca/PDF/C-6.pdf (accessed on 10 March 2020).
- Chanes, M. The challenges in training leading health managers. World Health Sao Paulo 2006, 30, 326–333. [Google Scholar]
- Tavangar, H.; Sherafat, A.; Vaezi, A.; Vafaeenasab, M.; Ehrampoush, M.; Fallahzadeh, H. Responsibility-evading performance: The experiences of healthcare staff about triage in emergency departments: A qualitative study. Iran. J. Nurs. Midwifery Res. 2019, 24, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Carsen, S.; Xia, C. The physician as leader. Mcgill J. Med. 2006, 9, 12. [Google Scholar] [CrossRef]
- Shepheard, J.; Lapiz, E.; Read, C.; Jackson, T. Reconciling hospital-acquired complications and CHADx+ in Victorian coded hospital data. Health Inf. Manag. J. 2018, 48, 76–86. [Google Scholar] [CrossRef]
- Pillay, R. The skills gap in hospital management: A comparative analysis of hospital managers in the public and private sectors in South Africa. Health Serv. Manag. Res. 2010, 23, 30–36. [Google Scholar] [CrossRef]
- Shan, C.M.; Ab Razak, N.H.; Ali, A.B.I. The impact of board of directors’ characteristics and remuneration on companies’ performance in Malaysia. Indian J. Public Health Res. Dev. 2018, 9, 1220. [Google Scholar] [CrossRef]
- Luleci, N.E.; Gemlik, H.N.; Bektas, G.; Manioglu, Y. The awareness of experience innovation and an application in private hospitals. J. Pak. Med. Assoc. 2015, 65, 1108–1111. [Google Scholar]
- Wong, C.A.; Cummings, G.G.; Ducharme, L. The relationship between nursing leadership and patient outcomes: A systematic review update. J. Nurs. Manag. 2013, 21, 709–724. [Google Scholar] [CrossRef]
- Phipps, F.M. Challenges of 21st-century health governance. Int. J. Health Gov. 2020, 25, 12–18. [Google Scholar] [CrossRef]
- Fleet, R.; Dupuis, G.; Fortin, J.-P.; Gravel, J.; Ouimet, M.; Poitras, J.; Légaré, F. Rural emergency care 360°: Mobilising healthcare professionals, decision-makers, patients and citizens to improve rural emergency care in the province of Quebec, Canada: A qualitative study protocol. BMJ Open 2017, 7, e016039. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zhu, L.; Peng, Z.; Liu, L.; Ling, S. Combining Resource, Structure and Institutional Environment: A Configurational Approach to the Mode Selection of the Integrated Healthcare in County. Int. J. Environ. Res. Public Health 2019, 16, 2975. [Google Scholar] [CrossRef] [PubMed]
- Helmers, R.A.; Harper, C.M. The mayo clinic model of clinical integration. Healthcare 2019, 7, 100330. [Google Scholar] [CrossRef]
- Fidler, D. The Challenges of Global Health Governance; Council on Foreign Relations: New York, NY, USA, 2010. [Google Scholar]
- Health Services Circular. Clinical Governance. Quality in the New NHS. Available online: http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_4012043.pdf (accessed on 4 June 2020).
- Price, T.; Tredinnick-Rowe, J.; Walshe, K.; Tazzyman, A.; Ferguson, J.; Boyd, A.; Archer, J.; Bryce, M. Reviving clinical governance? A qualitative study of the impact of professional regulatory reform on clinical governance in healthcare organizations in England. Health Policy 2020, 124, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Turner, J. Predicting Long-Term Debt in the Healthcare Sector; Scholars’ Press: Saarbrucken, Germany, 2015. [Google Scholar]
- Wernz, C.; Zhang, H.; Phusavat, K. International study of technology investment decisions at hospitals. Ind. Manag. Data Syst. 2014, 114, 568–582. [Google Scholar] [CrossRef]
- Leite, H.; Hodgkinson, I.R.; Gruber, T. New development: ‘Healing at a distance’—Telemedicine and COVID-19. Public Money Manag. 2020, 40, 483–485. [Google Scholar] [CrossRef]
- Panigutti, C.; Perotti, A.; Pedreschi, D. Doctor XAI: An ontology-based approach to blackbox sequential data classification explanations. In Proceedings of the 2020 Conference on Fairness, Accountability, and Transparency, Barcelona, Spain, 27–30 January 2020; pp. 629–693. [Google Scholar]
- Navarro, T.M.; Durán, F.M.; Santos, J.L. A regional competitiveness index for Spain. Rev. Estud. Reg. 2017, 109, 67–94. (In Spanish) [Google Scholar]
- Abedi, G.; Malekzadeh, R.; Moosazadeh, M.; Abedini, E.; Hasanpoor, E. Nurses’ Perspectives on the Impact of Marketing Mix Elements (7Ps) on Patients’ Tendency to Kind of Hospital. Ethiop. J. Health Sci. 2019, 29, 223–230. [Google Scholar] [CrossRef]
- Shamayleh, A.; Awad, M.; Farhat, J. IoT Based Predictive Maintenance Management of Medical Equipment. J. Med. Syst. 2020, 44, 1–12. [Google Scholar] [CrossRef]
- Fasterholdt, I.; Krahn, M.; Kidholm, K.; Yderstræde, K.B.; Pedersen, K.M. Review of early assessment models of innovative medical technologies. Health Policy 2017, 121, 870–879. [Google Scholar] [CrossRef] [PubMed]
- Myers, S.C. The Capital Structure Puzzle. J. Financ. 1984, 39, 575. [Google Scholar] [CrossRef]
- Myers, S.C.; Majluf, N.S. Corporate financing and investment decisions when firms have information that investors do not have. J. Financ. Econ. 1984, 13, 187–221. [Google Scholar] [CrossRef]
- Sarig, O.H. The effect of leverage on bargaining with a corporation. Financ. Rev. 1998, 33, 1–16. [Google Scholar] [CrossRef]
- Lemmon, M.L.; Roberts, M.R.; Zender, J.F. Back to the beginning: Persistence and the crosssection of corporate capital structure. J. Financ. 2008, 63, 1575–1608. [Google Scholar] [CrossRef]
- Kaper, M.S.; Reijneveld, S.A.; van Es, F.D.; de Zeeuw, J.; Almansa, J.; Koot, J.A.R.; de Winter, A.F. Effectiveness of a comprehensive health literacy consultation skills training for undergraduate medical students: A randomized controlled trial. Int. J. Environ. Res. Public Health 2020, 17, 81. [Google Scholar] [CrossRef]
- Mohan, D.; Wallace, D.J.; Kerti, S.J.; Angus, D.C.; Rosengart, M.R.; Barnato, A.E.; Yealy, D.M.; Fischhoff, B.; Chang, C.-C.; Kahn, J.M. Association of Practitioner Interfacility Triage Performance With Outcomes for Severely Injured Patients With Fee-for-Service Medicare Insurance. JAMA Surg. 2019, 154, e193944. [Google Scholar] [CrossRef] [PubMed]
- Neves, J.B.; Shepherd, S.; Cullen, D.; Powles, T.; Aitchison, M.; Tran, M.G.B. Performance and cost of a renal cancer specialist multidisciplinary team meeting: Results from 1500 discussions. J. Clin. Urol. 2019, 12, 314–319. [Google Scholar] [CrossRef]
- Luo, L.; Li, J.; Liu, C.; Shen, W. Using machine-learning methods to support health-care professionals in making admission decisions. Int. J. Health Plan. Manag. 2019, 34, e1236–e1246. [Google Scholar] [CrossRef]
- Kulkarni, S.S.; Barnato, A.E.; Rosengart, M.R.; Fischhoff, B.; Angus, D.C.; Yealy, N.M.; Wallace, D.J.; Mohan, D. Does Preexisting Practice Modify How Video Games Recalibrate Physician Heuristics in Trauma Triage? J. Surg. Res. 2019, 242, 55–61. [Google Scholar] [CrossRef]
- Salampessy, B.H.; Bijlsma, W.R.; Van Der Hijden, E.; Koolman, X.; Portrait, F.R.M. On selecting quality indicators: Preferences of patients with breast and colon cancers regarding hospital quality indicators. BMJ Qual. Saf. 2020, 29, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Comendeiro-Maaløe, M.; Ridao-López, M.; Gorgemans, S.; Bernal-Delgado, E. A comparative performance analysis of a renowned public private partnership for health care provision in Spain between 2003 and 2015. Health Policy 2019, 123, 412–418. [Google Scholar] [CrossRef]
- Arora, S.; Bhaukhandi, K.D.; Mishra, P.K. Coronavirus lockdown helped the environment to bounce back. Sci. Total. Environ. 2020, 742, 140573. [Google Scholar] [CrossRef]
- Carnevale, J.B.; Hatak, I. Employee adjustment and well-being in the era of COVID-19: Implications for human resource management. J. Bus. Res. 2020, 116, 183–187. [Google Scholar] [CrossRef]
- Garzotto, F.; Ceresola, E.; Panagiotakopoulou, S.; Spina, G.; Menotto, F.; Benozzi, M.; Casarotto, M.; Lanera, C.; Bonavina, M.G.; Gregori, D.; et al. COVID-19: Ensuring our medical equipment can meet the challenge. Expert Rev. Med Devices 2020, 17, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Goniewicz, K.; Khorram-Manesh, A.; Hertelendy, A.J.; Goniewicz, M.; Naylor, K.; Burkle, J.F.M. Current Response and Management Decisions of the European Union to the COVID-19 Outbreak: A Review. Sustainability 2020, 12, 3838. [Google Scholar] [CrossRef]
- Kalyaev, V.; Salimon, A.I.; Korsunsky, A.M.; Denisov, A.A. Fast Mass-Production of Medical Safety Shields under COVID-19 Quarantine: Optimizing the Use of University Fabrication Facilities and Volunteer Labor. Int. J. Environ. Res. Public Health 2020, 17, 3418. [Google Scholar] [CrossRef] [PubMed]
- Nikpay, S.S.; Smith, D.G. Hospital financial preparedness and covid-19. J. Health Care Financ. 2020, 46, 45–52. [Google Scholar]
- Alexander, J.A.; Morrisey, M.A.; Shortell, S.M. Effects of competition, regulation and corporatization on hospital-medical relations. J. Health Soc. Behav. 1986, 27, 220–235. [Google Scholar] [CrossRef]
- Abor, P.A. The effects of health governance and ownership structure on the performance of hospitals in Ghana. Int. J. Law Manag. 2015, 57, 107–140. [Google Scholar] [CrossRef]
- Huhs, E.; Gliebe, W.; Sendlhofer, G. Qualitative analysis of lean management in healthcare: Perspectives of Aus-trian and Swiss experts. Z. Evidenz Fortbild. Qual. Gesundh. 2019, 143, 8–14. (In German) [Google Scholar] [CrossRef] [PubMed]
- Tasi, M.C.; Keswani, A.; Bozic, K.J. Does physician leadership affect hospital quality, operational efficiency, and financial performance? Health Care Manag. Rev. 2019, 44, 256–262. [Google Scholar] [CrossRef]
- Van De Riet, M.C.P.; Berghout, M.A.; Buljac-Samardžić, M.; Van Exel, J.; Hilders, C.G.J.M. What makes an ideal hospital-based medical leader? Three views of healthcare professionals and managers: A case study. PLoS ONE 2019, 14, e0218095. [Google Scholar] [CrossRef]
- Govindan, K.; Mina, H.; Alavi, B. A decision support system for demand management in healthcare supply chains considering the epidemic outbreaks: A case study of coronavirus disease 2019 (COVID-19). Transp. Res. Part E Logist. Transp. Rev. 2020, 138, 101967. [Google Scholar] [CrossRef]
- Dexter, F.; Elhakim, M.; Loftus, R.W.; Seering, M.S.; Epstein, R.H. Strategies for daily operating room management of ambulatory surgery centers following resolution of the acute phase of the COVID-19 pandemic. J. Clin. Anesth. 2020, 64, 109854. [Google Scholar] [CrossRef] [PubMed]
- Manca, D.; Caldiroli, D.; Storti, E. A simplified math approach to predict ICU beds and mortality rate for hospital emergency planning under Covid-19 pandemic. Comput. Chem. Eng. 2020, 140, 106945. [Google Scholar] [CrossRef]
- Smith, B.A. A novel IDEA: The impact of serial interval on a modified-Incidence Decay and Exponential Adjustment (m-IDEA) model for projections of daily COVID-19 cases. Infect. Dis. Model. 2020, 5, 346–356. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Baxter, D.; Casady, C.B. A Coronavirus (COVID-19) Triage Framework for (Sub) National Public–Private Part-nership (PPP) Programs. Sustainability 2020, 12, 5253. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Administration (1) | Hospital Size (2) | Hospital Complexity (3) | ||
|---|---|---|---|---|
| Private | Medium | 50 to 149 beds | Medium | Intensive therapy, surgery and anesthetics, and mother and child care |
| Large | 150 or more beds | High | The characteristics of medium complexity plus radiotherapy, chemotherapy and chronic renal Disease | |
| Origin | Quotation from the Interview |
|---|---|
| Training | |
| G BR | “Directors should have a minimum of knowledge about managing people, resources, computing, clinical and administrative processes, but clinical knowledge is imperative; even if the organization aims for profit, in our view, quality of service for the patient predominates”. |
| G PT | “I believe they must be competent people with the capacity to integrate all teams and competences regarding everyday decisions that have to be made”. |
| G CAN | “Management involves different competences. In the field of health, the range should be even greater due to the complexity of these institutions. Knowledge of strategies, change management, innovation, sustainability are fundamental examples of what a hospital manager should have”. |
| Responsibilities and skills | |
| G BR | “Knowledge about financial administration, resource management; the ability to recognize and manage the quality of services the organization provides to the community; willingness to learn and change; leadership, pro-activeness and empathy”. |
| G PT | “Administrative, financial and human resources management is important”. |
| G CAN | “Competence in managing information systems; knowledge of the target population regarding socio-demographic and behavioral factors; knowledge of financial administration, resource management”. |
| Origin | Quotation from the Interview |
|---|---|
| Perception of corporate, hospital, clinical and integrated governance. | |
| G BR | “Corporate governance and hospital governance have the same format; both present similar ways, for top administration, to manage relations with those involved in processes. Integrated (clinical and corporate) management aims to minimize the risks involving patients, as well as risks associated with organizational decision-making on investments”. |
| G PT | “Corporate governance reflects the institutional arrangement between shareholders and administrators while hospital governance covers resource management. When these are in harmony, strategies tend to be aligned, contributing to achieving the organization’s objectives”. |
| G CAN | “Corporate management concerns the shareholders, their relations with stakeholders and how processes are managed. Clinical governance refers to how patient treatment is carried out by the multi-disciplinary team. I believe that hospital governance is in fact a mediation between administrative and clinical processes, aiming to align them to obtain better institutional performance”. |
| Is there a board of directors that decides on questions of investment, financing and other matters? How is this board formed? Does nursing management belong to it? | |
| G BR | “Yes, the Board is formed of shareholder representatives (3): medical, administrative and financial directors (all doctors) and an administrator, but Nursing management is not part of it. We recommend doctors’ participation in the Board of Directors as we judge it important to control costs; a lot of wastage or badly used resources can originate in the doctor’s pen”. |
| G PT | “We have Clinical Direction, a Nursing Director, Pharmaceutical Direction and Technical Medical Coordinators from all areas. Every week we have a meeting with each manager, and every month, we have a meeting with all the Coordinators and management team”. |
| G CAN | “There is a Board of Administration and an Executive Team. The Board is formed of the president of the Board of Administration, vice-president, treasurer and secretary. As for management of nursing services, the director belongs to the Board and her services cover academic professional practice, clinical operations, quality, patient safety, corporate risk management, information technology, sustainability and operational readiness, as well as strategic initiatives for clinical, administrative and academic change”. |
| Communication and spread of information throughout the institution. How is this done? | |
| G BR | “Through monthly meetings with all managers, a WhatsApp group and e-mail”. |
| G PT | “Through specific meetings, with the different work groups”. |
| G CAN | “There are different weekly meetings, in various areas of the whole hospital complex. Then, every month, the main resolutions, initiatives are passed to the Board of Administration by the executive leaders”. |
| How is the institution’s capital formed? Open or closed capital (company status)? | |
| G BR | “Closed. A company”. |
| G PT | “100% of the capital belongs to the North-American group”. |
| G CAN | “This is a Foundation with the founders’ own capital and is financed, mainly, by the province of Ontario, according to budgetary arrangements established by both”. |
| Origin | Quotation from the Interview |
|---|---|
| How are investment opportunities identified? What investments have been made in the last 5 years. | |
| G BR | “They are identified through market demand and technological development in the field of health. Opportunities to improve internal processes and growing demands for health services are always observed. Extending the structure: increased number of beds (35 more); acquisition of a new tomograph (due to increased patient demand); in terms of I&D, specific hospital costing software was acquired. A new project is being developed (unannounced due to being strategic)”. |
| G PT | “In the analyses we do, we assess by sector what we need to continue growing, always assessing cost-benefit. We keep 5% of the amount destined to investment for “diverse”, as a safety margin. Briefly, investments above 15 thousand euros must have a Business Plan, above 300 thousand euros besides the Group’s approval, it must be approved by the American group. The only condition is that the amount approved must not be exceeded”. |
| G CAN | “In-depth studies are elaborated, by different departments, to analyze the needs of the general population. Physical structure: modernization of the emergency department, extending the operating theatres, Intensive Care Units, main out-patient areas, and a new hospitalization unit. Equipment: new emergency vehicles, increased reserve of surgical equipment, integrated equipment to monitor patients in intensive care. I&D: service innovation; advanced training of Human Resources”. |
| What are the main limitations to investment and what sources (types of financing) are used when deciding on investment for the hospital’s projects? In the case of using External Capital as the source of finance, how is the risk of failing to meet the hospital’s commitment to creditors dealt with? | |
| G BR | “The main limitation is the low net profit margin. We normally prefer to use equity when we decide to invest, and as a last resort, we turn to banks and others. When it is necessary to use outside capital, we look for medium-term financing so that new investment can generate income and in that way help to cover the funding”. |
| G PT | “The only condition we have concerning investment is that the amount approved must not be exceeded. All the financing source comes from the group in the USA. In our investment analysis, we check the various alternatives and scenarios. Financing choices are adapted looking to optimize the investments we make as much as possible”. |
| G CAN | “The capacity to decide which investments can produce the greatest financial results and which, at the same time, can satisfy the needs of the target population. The hospital is exposed to a variety of financial risks, including credit risk, liquidity risk and market risk, and so it has adopted an integrated risk management structure. Credit risk is attributed principally to payments it is owed”. |
| To determine the amount of capital necessary for new investment, does the institution contrast short-term financial needs with medium and long-term needs? Does the institution have and follow strategic planning (for 3, 5 years)? Is an estimate made of the time for return on investments? Is the economic-financial viability of the investment analyzed? | |
| G BR | “According to the investment, medium-term financial needs are contrasted. The country’s economic instability and the group’s focus on equity as the source of finance does not allow us long-term debt”. “Yes; five-year planning, seeking to meet targets to achieve objectives”. |
| G PT | “There are meetings between all units of the Group to decide where we should invest. For example, in a certain year we decide to invest in the Diagnosis and Therapy Support Service, we identify all the equipment that has to be acquired for the Group, and in that way we have more negotiating power. Depending on the investment project, our strategic planning covers somewhere between 10 and 20 years”. |
| G CAN | “It contrasts; however, there is the relation between the size of the investment and the availability of capital. Depending on this factor, short or medium and long-term investment is decided on, always analyzing the interest rates of bank financing. The institution’s planning is always long-term”. |
| Origin | Quotation from the Interview |
|---|---|
| Types of analysis made. | |
| G BR | “BSC—Balanced Scorecard (tool to measure performance); Lean Six Sigma (practice of product and process improvement); ERM (Enterprise Risk Management), PDCA (Plan–Do–Check–Act) Cycle for internal processes”. |
| G PT | “The Group uses BSC and the Lean Six Sigma mainly to obtain an analysis and process efficiency. Hospital management by the Group is relatively recent and here we are still molding the processes using the experience acquired by the group”. |
| G CAN | “BSC—Balanced Scorecard (tool to measure performance); Lean Six Sigma (practice of product and process improvement); ERM (Enterprise Risk Management); GRC (Governance, Risk and Compliance), PDCA (Plan–Do–Check–Act) Cycle”. |
| Use of a costing method to determine the results of service to patients. | |
| G BR | “Yes, software has been implemented for activity-based costing (ABC method). This method provides analyses of clinical or surgical hospitalization costs, as well as information about the costs of procedures by medical specialty or surgical team, which makes it easier to monitor where resources are being consumed”. |
| G PT | “We have tools that let us know the costs. In the Clinic, we use data that come from analytical accounting. Surgery costs are analyzed at the level of the teams carrying out the operation; we don’t yet have the costs of procedures specifically, but there is monitoring of the use of inputs by medical team, both as regards exams and the operating theatre”. |
| G CAN | “Even if a product or information does not have a price, it certainly has a cost and this is determined in all areas, by different methods; there is a department dealing with these activities”. |
| How are the risks of new investments assessed? | |
| G BR | “We always assess the market demand, the sustainability of the chain and competitors’ quality/efficiency”. |
| G PT | “We use the Enterprise Risk Management (ERM) method”. |
| G CAN | “In relation to future situations, nobody can be certain that a given event will occur. As the project’s forecast cash-flow is a future event, it may be of the amount foreseen or any other. We currently use two methods: sensitivity analysis and scenario creation”. |
| Origin | Quotation from the Interview |
|---|---|
| Statements made: | |
| G BR | “Staff reduction, closure of services, financial loss of about 22% per month, drastic reduction in non-emergency treatment, increased expenditure on disposable supplies and individual protection equipment, emergency investment in intensive therapy equipment”. |
| G PT | “We had to close the hospital for a few weeks; maternity was re-allocated to another hospital in the Group, a lot of people lost their jobs, the operating theatres were almost idle”. |
| G CAN | “Here, nothing was different from in other countries... even with the population’s cooperation in terms of prevention, we had to make major investment in equipment due to the high demand for ventilators. It was also necessary to close various services that, during the pandemic, are not being used. There was certainly a great loss of income”. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marques, I.; Serrasqueiro, Z.; Nogueira, F. Managers’ Competences in Private Hospitals for Investment Decisions during the COVID-19 Pandemic. Sustainability 2021, 13, 1757. https://doi.org/10.3390/su13041757
Marques I, Serrasqueiro Z, Nogueira F. Managers’ Competences in Private Hospitals for Investment Decisions during the COVID-19 Pandemic. Sustainability. 2021; 13(4):1757. https://doi.org/10.3390/su13041757
Chicago/Turabian StyleMarques, Isabel, Zélia Serrasqueiro, and Fernanda Nogueira. 2021. "Managers’ Competences in Private Hospitals for Investment Decisions during the COVID-19 Pandemic" Sustainability 13, no. 4: 1757. https://doi.org/10.3390/su13041757
APA StyleMarques, I., Serrasqueiro, Z., & Nogueira, F. (2021). Managers’ Competences in Private Hospitals for Investment Decisions during the COVID-19 Pandemic. Sustainability, 13(4), 1757. https://doi.org/10.3390/su13041757