
The Association of Falls Risk in Older Adults and Their Living Environment: A Case Study of Rural Area, Thailand





Abstract
1. Introduction
2. Methodology
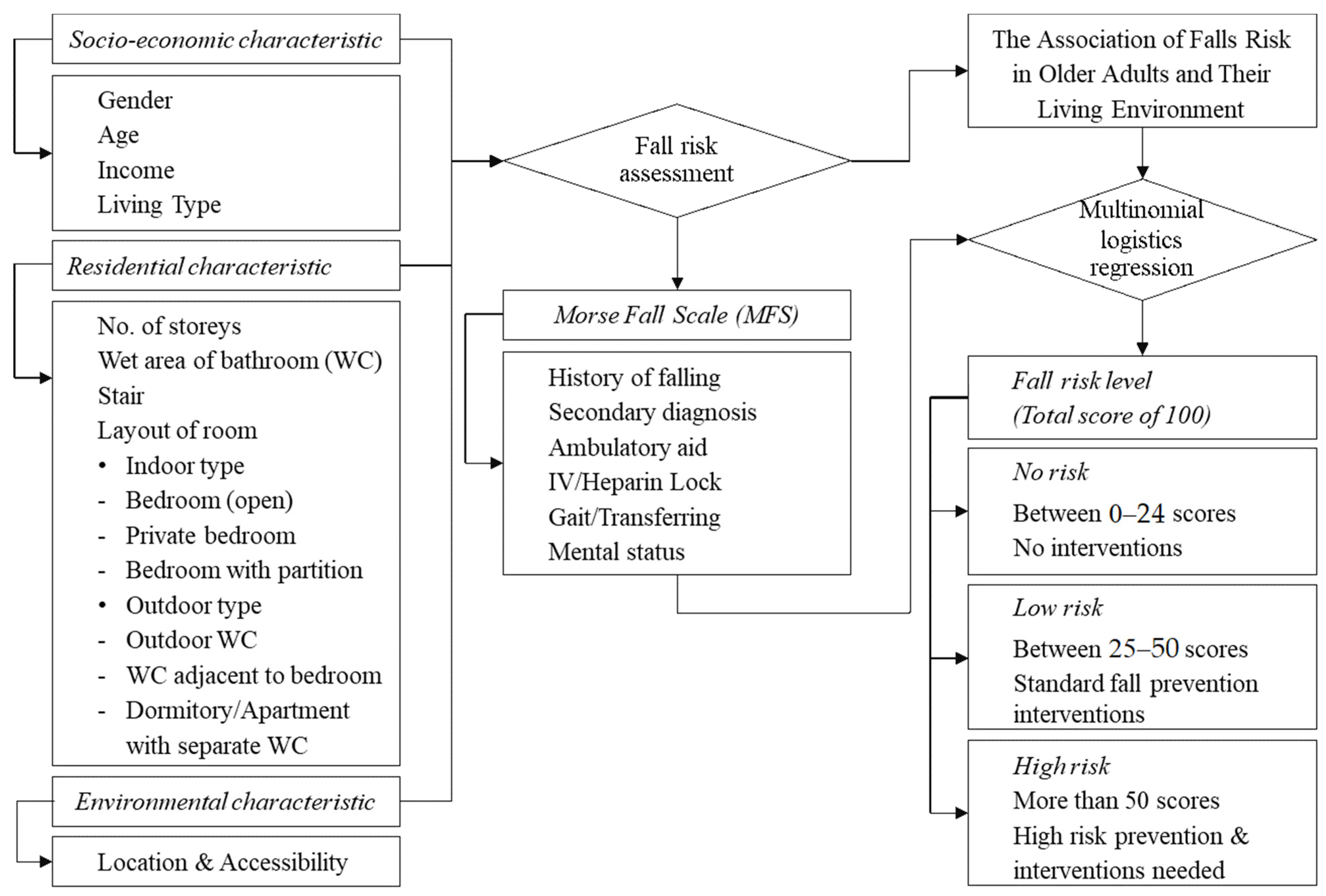
2.1. Framework of Fall Risk Identification
2.2. Sample Size
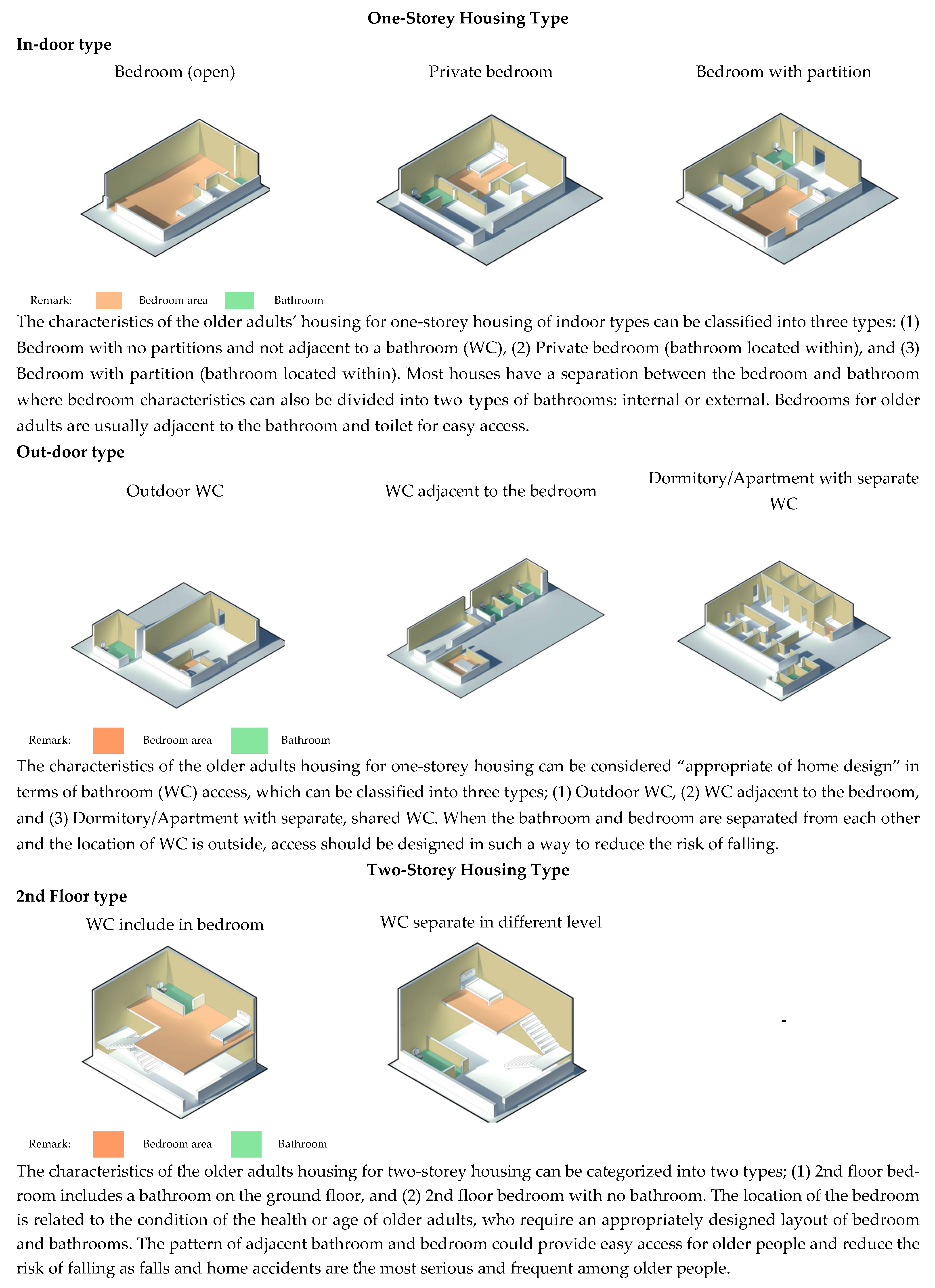
2.3. Living Environment Assessment
- Home location and approach: Housing should be located close to public services and facilities. An affordable home must be provided to enable older people, especially those who are frail, to remain at home. The residence must be clean and located at a safe distance from road traffic.
- Access and circulation: Each house should have its own access and its own entrance. There should be sufficient space to enable older people to move around freely. The surfaces and passages should be wide enough for wheelchairs with appropriately designed bathrooms, toilets, and kitchen.
- Spaces for living: Housing should be appropriately designed and equipped with a range of appropriate facilities and amenities to provide a safe and comfortable environment. Housing should be integrated with the surrounding community to allow neighborhood connections for more social interactions among residents.
- Design and Facilities: Housing should be made of appropriate materials and well-constructed with a range of facilities available for older people. Housing design should take into account the specific needs of the older adults with safety and ease of movement in mind. The integration of special assistive devices or home modifications can be recommended to accommodate physical impairments.
2.4. Variables
2.5. Method of Analysis
3. Results
3.1. Socio-Economic Characteristics and Risk of Falling
3.2. Living Environment Characteristics in Banphaeo
3.3. Relationship between Home Hazards and Level of Fall Risk
4. Discussion
4.1. Analysis of the Factors Affecting Risk of Falls in Older Adults in Rural Areas
4.2. Limitations and Suggestions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 10 August 2021).
- Department of Older Persons. Elderly Statistics. Available online: http://www.dop.go.th/th/know/1 (accessed on 20 May 2020).
- National Statistical Office. Report on the 2017 Survey of the Older Persons in Thailand. Available online: http://www.nso.go.th/sites/2014en/Survey/social/domographic/OlderPersons/2017/Full%20Report_080618.pdf (accessed on 11 April 2020).
- World Health Organization. Falls. Available online: https://www.who.int/news-room/fact-sheets/detail/falls (accessed on 10 August 2021).
- Peden, M.; McGee, K.; Sharma, G. The Injury Chart Book: A Graphical Overview of the Global Burden of Injuries; World Health Or-ganization: Geneva, Switzerland, 2002. [Google Scholar]
- Close, J.C.; Lord, S.L.; Menz, H.B.; Sherrington, C. What is the role of falls? Best Pr. Res. Clin. Rheumatol. 2005, 19, 913–935. [Google Scholar] [CrossRef] [PubMed]
- Newbury, J.W.; Marley, J.E.; Beilby, J.J. A randomised controlled trial of the outcome of health assessment of people aged 75 years and over. Med. J. Aust. 2001, 175, 104–107. [Google Scholar] [CrossRef] [PubMed]
- O’Loughlin, J.L.; Robitaille, Y.; Boivin, J.-F.; Suissa, S. Incidence of and Risk Factors for Falls and Injurious Falls among the Community-dwelling Elderly. Am. J. Epidemiol. 1993, 137, 342–354. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Speechley, M.; Ginter, S.F. Risk Factors for Falls among Elderly Persons Living in the Community. N. Engl. J. Med. 1988, 319, 1701–1707. [Google Scholar] [CrossRef]
- Wagner, E.H.; Lacroix, A.Z.; Grothaus, L.; Leveille, S.G.; Hecht, J.A.; Artz, K.; Odle, K.; Buchner, D.M. Preventing disability and falls in older adults: A population-based randomized trial. Am. J. Public Health 1994, 84, 1800–1806. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Public Health. Statistic of Public Health 2014, 1st ed.; The War Veterans Organization of Thailand Press: Bangkok, Thailand, 2015. [Google Scholar]
- Ministry of Public Health. Statistic Information: Falls in the Elderly. Available online: http://www.thaincd.com/2016/mission/documents.php?tid=39&gid=1-027 (accessed on 5 August 2021).
- Hill, A.-M.; Hoffmann, T.; Haines, T.P. Circumstances of falls and falls-related injuries in a cohort of older patients following hospital discharge. Clin. Interv. Aging 2013, 8, 765–774. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Report on Falls PREVENTION in Older Age. Available online: https://extranet.who.int/agefriendlyworld/wp-content/uploads/2014/06/WHo-Global-report-on-falls-prevention-in-older-age.pdf (accessed on 15 April 2020).
- Evci, E.D.; Ergin, F.; Beser, E. Home Accidents in the Elderly in Turkey. Tohoku J. Exp. Med. 2006, 209, 291–301. [Google Scholar] [CrossRef]
- Chang, J.T.; Morton, S.C.; Rubenstein, L.; Mojica, W.A.; Maglione, M.; Suttorp, M.J.; Roth, E.A.; Shekelle, P.G. Interventions for the prevention of falls in older adults: Systematic review and meta-analysis of randomised clinical trials. BMJ 2004, 328, 680. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Baker, D.I.; McAvay, G.; Claus, E.B.; Garrett, P.; Gottschalk, M.; Koch, M.L.; Trainor, K.; Horwitz, R.I. A Multifactorial Intervention to Reduce the Risk of Falling among Elderly People Living in the Community. N. Engl. J. Med. 1994, 331, 821–827. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Kumar, C. The Patient Who Falls: “It’s always a trade-off”. JAMA 2010, 303, 258–266. [Google Scholar] [CrossRef] [PubMed]
- FAO. Guidelines on Defining Rural Areas and Compiling Indicators for Development Policy. Available online: http://www.fao.org/3/ca6392en/ca6392en.pdf (accessed on 12 April 2020).
- Scott, V.; Wagar, B.; Sum, A.; Metcalfe, S.; Wagar, L. A Public Health Approach to Fall Prevention Among Older Persons in Canada. Clin. Geriatr. Med. 2010, 26, 705–718. [Google Scholar] [CrossRef]
- Swain, G.R. How Does Economic and Social Disadvantage Affect Health? Focus 2016, 33, 1–6. [Google Scholar]
- Braun, B.L. Knowledge and perception of fall-related risk factors and fall-reduction techniques among community-dwelling elderly individuals. Phys. Ther. 1998, 78, 1262–1276. [Google Scholar] [CrossRef]
- Vaillant, G.E.; Mukamal, K. Successful Aging. Am. J. Psychiatry 2001, 158, 839–847. [Google Scholar] [CrossRef]
- Lamb, S.E.; Jorstad-Stein, E.C.; Hauer, K.; Becker, C. Development of a Common Outcome Data Set for Fall Injury Prevention Trials: The Prevention of Falls Network Europe Consensus. J. Am. Geriatr. Soc. 2005, 53, 1618–1622. [Google Scholar] [CrossRef] [PubMed]
- Schiller, J.S.; Kramarow, E.A.; Dey, A.N. Fall Injury Episodes Among Noninstitutionalized Older Adults: United States, 2001–2003. Adv. Data 2007, 392, 1–16. [Google Scholar] [CrossRef]
- Mack, K.A.; Rudd, R.A.; Mickalide, A.D.; Ballesteros, M.F. Fatal Unintentional Injuries in the Home in the U.S., 2000–2008. Am. J. Prev. Med. 2013, 44, 239–246. [Google Scholar] [CrossRef]
- Murphy, S.L. Deaths: Final Data for 1998 National Vital Statistics Reports, 48(11); National Center for Health Statistics: Hyattsville, MD, USA, 2000. [Google Scholar]
- Howland, J.; Peterson, E.W.; Levin, W.C.; Fried, L.; Pordon, D.; Bak, S. Fear of Falling among the Community-Dwelling Elderly. J. Aging Health 1993, 5, 229–243. [Google Scholar] [CrossRef]
- Vellas, B.J.; Wayne, S.J.; Romero, L.J.; Baumgartner, R.N.; Garry, P.J. Fear of falling and restriction of mobility in elderly fallers. Age Ageing 1997, 26, 189–193. [Google Scholar] [CrossRef]
- Rubenstein, L.Z. Falls in older people: Epidemiology, risk factors and strategies for prevention. Age Ageing 2006, 35, ii37–ii41. [Google Scholar] [CrossRef]
- Stalenhoef, P.A.; Crebolder, H.F.; Knottnerus, J.A.; Van Der Horst, F.G. Injuries. Incidence, risk factors and consequences of falls among elderly subjects living in the community. A criteria-based analysis. Eur. J. Public Health 1997, 7, 328–334. [Google Scholar] [CrossRef]
- Carter, N.D.; Kannus, P.; Khan, K.M. Exercise in the Prevention of Falls in Older People: A Systematic Literature Review Ex-amining the Rationale and the Evidence. Sports Med. 2001, 31, 427–438. [Google Scholar] [CrossRef] [PubMed]
- Kannus, P.; Sievänen, H.; Palvanen, M.; Järvinen, T.; Parkkari, J. Prevention of falls and consequent injuries in elderly people. Lancet 2005, 366, 1885–1893. [Google Scholar] [CrossRef]
- Letts, L.; Moreland, J.; Richardson, J.A.; Coman, L.; Edwards, M.; Ginis, K.M.; Wilkins, S.; Wishart, L. The physical environment as a fall risk factor in older adults: Systematic review and meta-analysis of cross-sectional and cohort studies. Aust. Occup. Ther. J. 2010, 57, 51–64. [Google Scholar] [CrossRef]
- Desforges, J.F.; Tinetti, M.E.; Speechley, M. Prevention of Falls among the Elderly. N. Engl. J. Med. 1989, 320, 1055–1059. [Google Scholar] [CrossRef] [PubMed]
- Liu-Ambrose, T.Y.; Ashe, M.C.; Graf, P.; Beattie, B.L.; Khan, K.M. Increased Risk of Falling in Older Community-Dwelling Women with Mild Cognitive Impairment. Phys. Ther. 2008, 88, 1482–1491. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, N.; Bhatti, T. Population Health Promotion: An Integrated Model of Population Health and Health Promotion. Available online: http://www.phac-aspc.gc.ca/ph-sp/php-psp/index-eng.php (accessed on 15 April 2020).
- Carter, S.E.; Campbell, E.M.; Sanson-Fisher, R.; Redman, S.; Gillespie, W.J. Environmental hazards in the homes of older people. Age Ageing 1997, 26, 195–202. [Google Scholar] [CrossRef]
- Lord, S.R.; Menz, H.; Sherrington, C. Home environment risk factors for falls in older people and the efficacy of home modifications. Age Ageing 2006, 35, ii55–ii59. [Google Scholar] [CrossRef]
- Lucht, U. A prospective study of accidental falls and resulting injuries in the home among elderly people. Acta Socio. Med. Scand. 1971, 3, 105–120. [Google Scholar]
- Schelp, L.; Svanström, L. One-year Incidence of Home Accidents in a Rural Swedish Municipality. Scand. J. Soc. Med. 1986, 14, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Wild, D.; Nayak, U.S.; Isaacs, B. How dangerous are falls in old people at home? BMJ 1981, 282, 266–268. [Google Scholar] [CrossRef] [PubMed]
- Edelman, M.; Ficorelli, C.T. Keeping older adults safe at home. Nursing 2012, 42, 65–66. [Google Scholar] [CrossRef]
- McCullagh, M.C. Home modification. Am. J. Nurs. 2006, 106, 54–63. [Google Scholar] [CrossRef]
- Hornbrook, M.C.; Stevens, V.J.; Wingfield, P.D.J.; Hollis, J.F.; Greenlick, M.R.; Ory, M.G. Preventing Falls Among Community-Dwelling Older Persons: Results from a Randomized Trial. Gerontologist 1994, 34, 16–23. [Google Scholar] [CrossRef]
- Nikolaus, T.; Bach, M. Preventing Falls in Community-Dwelling Frail Older People Using a Home Intervention Team (HIT): Results from the Randomized Falls-HIT Trial. J. Am. Geriatr. Soc. 2003, 51, 300–305. [Google Scholar] [CrossRef]
- Centre for Clinical Practice at NICE (UK). Falls: Assessment and Prevention of Falls in Older People; National Institute for Health and Care Excellence: London, UK, 2013. [Google Scholar]
- US National Library of Medicine. Available online: https://medlineplus.gov/lab-tests/fall-risk-assessment/ (accessed on 4 August 2020).
- Morse, J.M.; Black, C.; Oberle, K.; Donahue, P. A prospective study to identify the fall-prone patient. Soc. Sci. Med. 1989, 28, 81–86. [Google Scholar] [CrossRef]
- Morse Fall Scale. Available online: https://networkofcare.org/library/Morse%20Fall%20Scale.pdf (accessed on 4 August 2021).
- Ministry of Social Development and Human Security. Aging Population in Thailand. Available online: http://www.dop.go.th/download/knowledge/knowledge_th_20160106135752_1.pdf (accessed on 12 April 2020).
- Preedy, V.; Watson, R. Handbook of Disease Burdens and Quality of Life Measures; Springer: New York, NY, USA, 2010. [Google Scholar]
- Yamane, T. Statistics: An Introductory Analysis, 2nd ed.; Harper and Row: New York, NY, USA, 1967. [Google Scholar]
- Universal Design Approach for Dementia Friendly Dwellings. Available online: http://universaldesign.ie/Web-Content-/UD-DFD-Guidelines-Intro-June-15.pdf (accessed on 10 April 2020).
- Morse, J. Preventing Patient Falls: Establishing a Fall Intervention Program; Springer Publishing Company: New York, NY, USA, 2008; pp. 9–11. [Google Scholar]
- Campbell, A.; Spears, G.F.; Borrie, M.J. Examination by logistic regression modelling of the variables which increase the relative risk of elderly women falling compared to elderly men. J. Clin. Epidemiol. 1990, 43, 1415–1420. [Google Scholar] [CrossRef]
- Lawlor, D.A.; Patel, R.; Ebrahim, S. Association between falls in elderly women and chronic diseases and drug use: Cross sectional study. BMJ 2003, 327, 712–717. [Google Scholar] [CrossRef]
- Luukinen, H.; Koski, K.; Laippala, P.; Kivelä, S.-L. Predictors for recurrent falls among the home-dwelling elderly. Scand. J. Prim. Health Care 1995, 13, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Wickham, C.; Cooper, C.; Margetts, B.M.; Barker, D.J.P. Muscle Strength, Activity, Housing and the Risk of Falls in Elderly People. Age Ageing 1989, 18, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Hanley, A.; Silke, C.; Murphy, J. Community-based health efforts for the prevention of falls in the elderly. Clin. Interv. Aging 2010, 6, 19–25. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Morgan, S.P.; Teachman, J.D. Logistic Regression: Description, Examples, and Comparisons. J. Marriage Fam. 1988, 50, 929. [Google Scholar] [CrossRef]
- Fuller, G.F. Falls in the elderly. Am. Fam. Physician 2000, 61, 2173–2174. [Google Scholar]
- Prudham, D.; Evans, J.G. Factors Associated with Falls in the Elderly: A Community Study. Age Ageing 1981, 10, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Samutsakhon Province. Available online: http://www.samutsakhon.go.th/_new/frontpage (accessed on 10 April 2020).
- World Bank. Aging in Thailand—Addressing Unmet Health Needs of the Elderly Poor. Available online: https://www.worldbank.org/th/news/press-release/2016/04/08/aging-in-thailand---addressing-unmet-health-needs-of-the-elderly-poor (accessed on 15 April 2020).
- Rukumnuaykit, P.; Palakawong-na-ayudhya, S. The Diversity of Migrant Groups in Thailand: Population and Social Perspec-tives. Dev. Econ. Rev. 2019, 13, 84–122. [Google Scholar]
- Thailand Productivity Institute. Strategy, General Public Articles, Knowledge. Available online: https://www.ftpi.or.th/2015/172 (accessed on 12 April 2020).
- Clemson, L.; Cumming, R.; Roland, M. Case–Control Study of Hazards in the Home and Risk of Falls and Hip Fractures. Age Ageing 1996, 25, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Rogers, M.E.; Rogers, N.L.; Takeshima, N.; Islam, M.M. Reducing the Risk for Falls in the Homes of Older Adults. J. Hous. Elder. 2004, 18, 29–39. [Google Scholar] [CrossRef]
- Deandrea, S.; Lucenteforte, E.; Bravi, F.; Foschi, R.; La Vecchia, C.; Negri, E. Risk Factors for Falls in Community-Dwelling Older People: A Systematic Review and Meta-Analysis. Epidemiology 2010, 21, 658–668. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Srivastava, D.K.; Verma, A.; Kumar, S.; Singh, N.P.; Kaushik, A. The problems of fall, risk factors and their management among geriatric population in India. Indian J. Community Health 2013, 25, 89–94. [Google Scholar]
- Kwan, M.M.-S.; Close, J.C.; Wong, A.K.W.; Lord, S.R. Falls Incidence, Risk Factors, and Consequences in Chinese Older People: A Systematic Review. J. Am. Geriatr. Soc. 2011, 59, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Inouye, S.K.; Gill, T.M.; Doucette, J.T. Shared risk factors for falls, incontinence, and functional dependence. Unifying the approach to geriatric syndromes. JAMA 1995, 273, 1348–1353. [Google Scholar] [CrossRef]
- Kemoun, G.; Thibaud, M.; Roumagne, N.; Carette, P.; Albinet, C.; Toussaint, L.; Paccalin, M.; Dugue, B. Effects of a Physical Training Programme on Cognitive Function and Walking Efficiency in Elderly Persons with Dementia. Dement. Geriatr. Cogn. Disord. 2010, 29, 109–114. [Google Scholar] [CrossRef]
- Jesmin, S.; Amin, I.; Ingman, S. Ageing and caregiving crisis in the low and middle income societies. Indian J. Gerontol. 2011, 25, 309–328. [Google Scholar]
- Cojocari, T.; Cupcea, R. Aging in Moldova: A Country with Orphan Older Adults. Gerontologist 2018, 58, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Norris-Baker, C.; Scheidt, R.J. From ‘Our Town’ to ‘Ghost Town’?: The Changing Context of Home for Rural Elders. Int. J. Aging Hum. Dev. 1994, 38, 181–202. [Google Scholar] [CrossRef] [PubMed]
- Iamtrakul, P.; Chayphong, S.; Klaylee, J. The Study on Age-Friendly Environments for an Improvement of Quality of Life for Elderly, Asian Mega City, Thailand. Lowl. Technol. Int. 2019, 21, 123–133. [Google Scholar]
- Iamtrakul, P.; Chayphong, S. Healthy Aging in Home Environment Exposures. GMSARN Int. J. 2021, 15, 175–184. [Google Scholar]
- Iamtrakul, P.; Chayphong, S. Aging and Environment in Role of Rural Older Adults. GMSARN Int. J. 2021, 15, 236–243. [Google Scholar]
- Chaisomboon, M.; Jomnonkwao, S.; Ratanavaraha, V. Elderly Users’ Satisfaction with Public Transport in Thailand Using Different Importance Performance Analysis Approaches. Sustainability 2020, 12, 9066. [Google Scholar] [CrossRef]
- Clemson, L.; Stark, S.; Pighills, A.C.; Torgerson, D.J.; Sherrington, C.; Lamb, S.E. Environmental interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2019, 2019, 013258. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Fall Risk Assessment (N, %) | p-Value a | ||
|---|---|---|---|---|
| No Risk (0–24 Score) | Low Risk (25–50 Score) | High Risk (>50 Score) | ||
| Sex | 0.000 | |||
| Female | 397 (41.8%) | 151 (15.9%) | 37 (3.9%) | |
| Male | 290 (30.5%) | 58 (6.1) | 17 (1.8%) | |
| Age | 0.000 | |||
| 60–69 years | 338 (35.6%) | 52 (5.5%) | 6 (0.6%) | |
| 70–79 years | 232 (24.4%) | 80 (8.4%) | 24 (2.5%) | |
| >80 years | 117 (12.3%) | 77 (8.1%) | 24 (2.5%) | |
| Status | 0.000 | |||
| Married | 363 (38.2%) | 73 (7.7%) | 30 (3.2%) | |
| Divorced | 69 (7.3%) | 27 (2.8%) | 3 (0.3%) | |
| Single | 255 (26.8%) | 109 (11.5%) | 21 (2.2%) | |
| Income (baht) | 0.000 | |||
| Less than 2000 | 420 (44.2%) | 168 (17.7%) | 51 (5.4%) | |
| More than 2000 | 267 (28.1%) | 41 (4.3%) | 3 (0.3%) | |
| Fall experience | 0.000 | |||
| Yes | 1 (0.1%) | 76 (8.0%) | 21 (2.2%) | |
| No | 686 (72.2%) | 133 (14.0%) | 33 (3.5%) | |
| Diseases | 0.000 | |||
| No disease | 504 (53.1%) | 116 (12.2%) | 14 (1.5%) | |
| More than one disease | 183 (19.3%) | 93 (9.8%) | 40 (4.2%) | |
| Living type | 0.460 | |||
| Living alone | 38 (4.0%) | 13 (1.4%) | 1 (0.1%) | |
| Living alone (near family) | 22 (2.3%) | 10 (1.1%) | 0 (0.0%) | |
| Living with the family | 627 (66.0%) | 186 (19.6%) | 53 (5.6%) | |
| Private bedroom (toilet availability) | 0.003 | |||
| No | 412 (43.4%) | 152 (16.0%) | 37 (3.9%) | |
| Included | 275 (28.9%) | 57 (6.0%) | 17 (1.8%) | |
| Using stairs | 0.942 | |||
| No | 469 (49.4%) | 142 (14.9%) | 38 (4.0%) | |
| Yes | 218 (22.9%) | 67 (7.1%) | 16 (1.7%) | |
| Variables | B | Std. Error | Wald | df | Sig. | Exp(B) | 95% Confidence Interval for Exp(B) | ||
|---|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||||
| Low risk | |||||||||
| Intercept | 5.285 | 1.073 | 24.284 | 1 | 0.000 * | ||||
| Sex | Male | −0.518 | 0.217 | 5.671 | 1 | 0.017 * | 0.596 | 0.389 | 0.912 |
| Female | (reference) | ||||||||
| Age (years) | 60–69 | −1.675 | 0.266 | 39.503 | 1 | 0.000 * | 0.187 | 0.111 | 0.316 |
| 70–79 | −0.729 | 0.234 | 9.757 | 1 | 0.002 * | 0.482 | 0.305 | 0.762 | |
| >80 | (reference) | ||||||||
| Income (baht) | <2000 | 1.430 | 0.294 | 23.652 | 1 | 0.000 * | 4.179 | 2.348 | 7.435 |
| ≥2000 | (reference) | ||||||||
| Diseases | No diseases | −0.953 | 0.208 | 20.990 | 1 | 0.000 * | 0.386 | 0.257 | 0.580 |
| >1 disease | (reference) | ||||||||
| Fall experience | No | −6.848 | 1.048 | 42.726 | 1 | 0.000 * | 0.001 | 0.000 | 0.008 |
| Yes | (reference) | ||||||||
| Private bedroom (toilet availability) | No | 0.649 | 0.219 | 8.777 | 1 | 0.003 * | 1.913 | 1.246 | 2.939 |
| Yes | (reference) | ||||||||
| High risk | |||||||||
| Intercept | 3.703 | 1.267 | 8.545 | 1 | 0.003 * | ||||
| Sex | Male | −0.222 | 0.352 | 0.398 | 1 | 0.528 | 0.801 | 0.402 | 1.597 |
| Female | (reference) | ||||||||
| Age (years) | 60–69 | −2.525 | 0.523 | 23.345 | 1 | 0.000 * | 0.080 | 0.029 | 0.223 |
| 70–79 | −0.888 | 0.364 | 5.938 | 1 | 0.015 | 0.412 | 0.201 | 0.841 | |
| >80 | (reference) | ||||||||
| Income (baht) | <2000 | 2.841 | 0.668 | 18.065 | 1 | 0.000 * | 17.129 | 4.622 | 63.480 |
| ≥2000 | (reference) | ||||||||
| Diseases | No diseases | −2.250 | 0.358 | 39.403 | 1 | 0.000 * | 0.105 | 0.052 | 0.213 |
| >1 diseases | (reference) | ||||||||
| Fall experience | No | −7.295 | 1.098 | 44.122 | 1 | 0.000 * | 0.001 | 7.887 × 10−5 | 0.006 |
| Yes | (reference) | ||||||||
| Private bedroom (toilet availability) | No | 0.508 | 0.353 | 2.066 | 1 | 0.151 | 1.662 | 0.831 | 3.321 |
| Yes | (reference) | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iamtrakul, P.; Chayphong, S.; Jomnonkwao, S.; Ratanavaraha, V. The Association of Falls Risk in Older Adults and Their Living Environment: A Case Study of Rural Area, Thailand. Sustainability 2021, 13, 13756. https://doi.org/10.3390/su132413756
Iamtrakul P, Chayphong S, Jomnonkwao S, Ratanavaraha V. The Association of Falls Risk in Older Adults and Their Living Environment: A Case Study of Rural Area, Thailand. Sustainability. 2021; 13(24):13756. https://doi.org/10.3390/su132413756
Chicago/Turabian StyleIamtrakul, Pawinee, Sararad Chayphong, Sajjakaj Jomnonkwao, and Vatanavongs Ratanavaraha. 2021. "The Association of Falls Risk in Older Adults and Their Living Environment: A Case Study of Rural Area, Thailand" Sustainability 13, no. 24: 13756. https://doi.org/10.3390/su132413756
APA StyleIamtrakul, P., Chayphong, S., Jomnonkwao, S., & Ratanavaraha, V. (2021). The Association of Falls Risk in Older Adults and Their Living Environment: A Case Study of Rural Area, Thailand. Sustainability, 13(24), 13756. https://doi.org/10.3390/su132413756