
State Incentives and Sustainable Motivation System in the Health Sector


 , ,
, ,
Abstract
1. Introduction
2. Literature Review and Theoretical Framework
3. Materials and Methods
- -
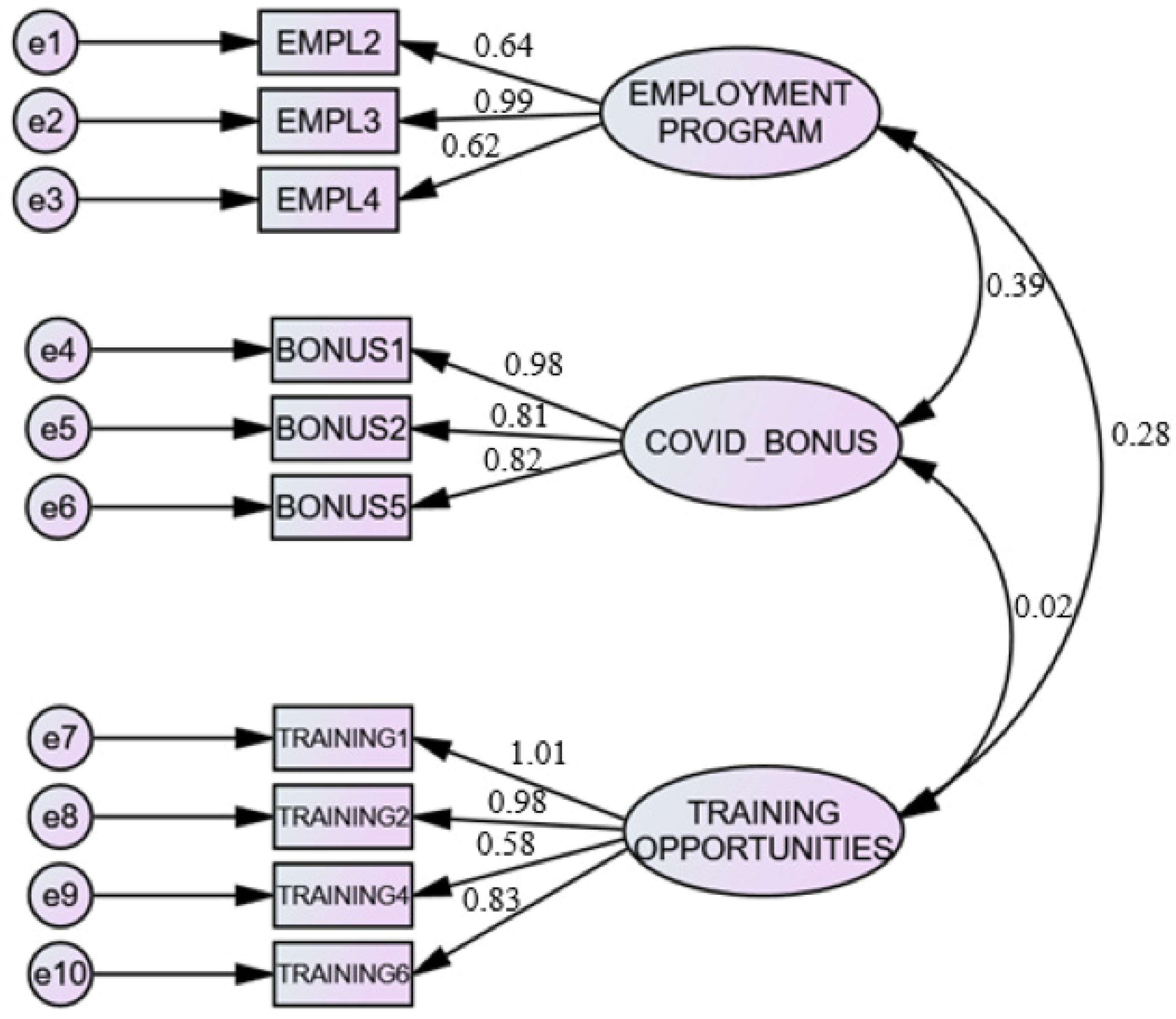
- Specific goal 1: To verify the existence of three dimensions of state incentives: employment program, COVID-19 bonus and training opportunities.
- -
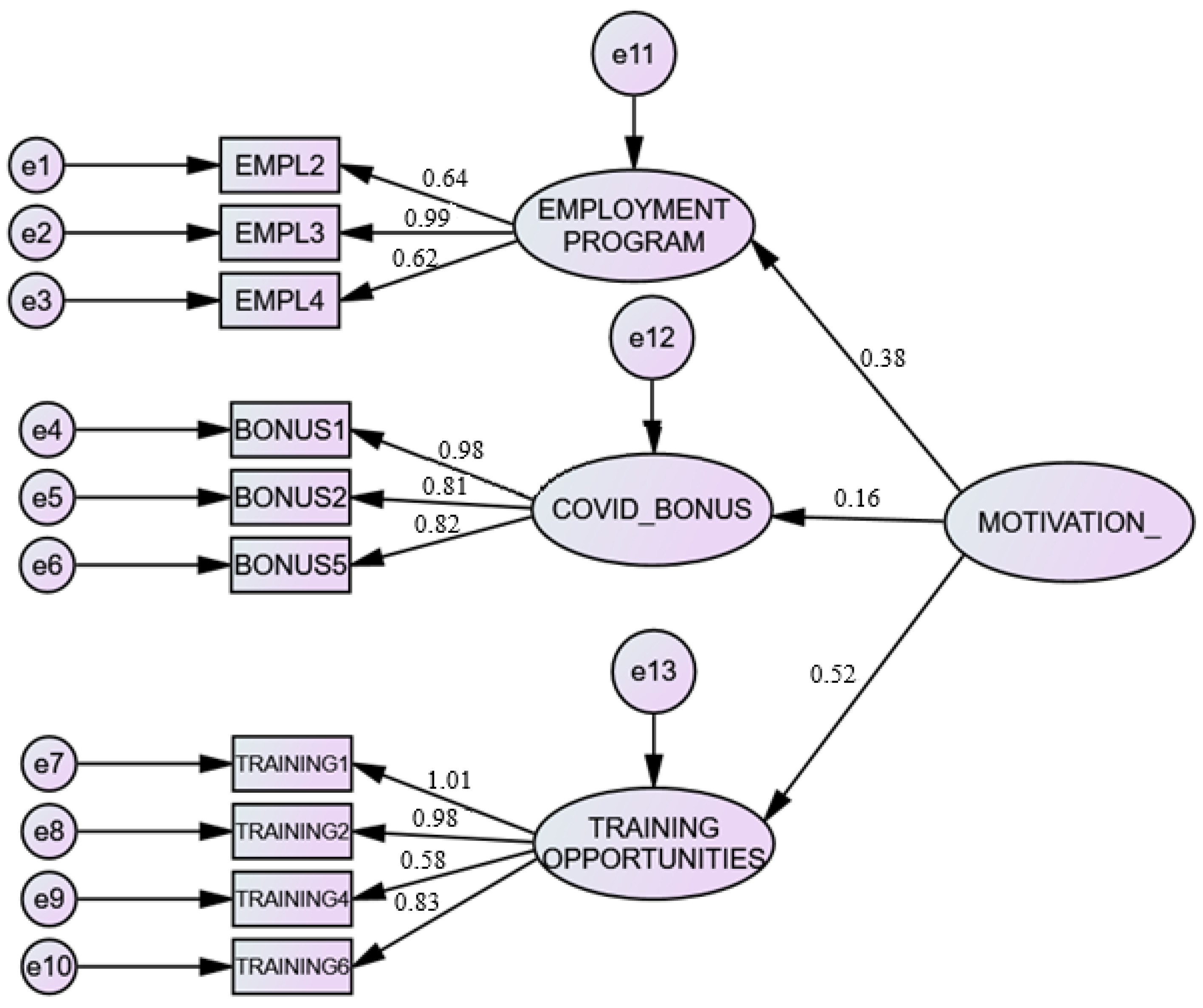
- Specific goal 2: To analyse the effect of each dimension of state incentives on healthcare workers’ motivation and the sustainability of healthcare system and to determine which dimension has the strongest impact on these variables.
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Eurostat. Healthcare Expenditure Across the EU: 10% of GDP. Available online: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/ddn-20201202-1 (accessed on 14 August 2021).
- Šahman-Zaimović, M.; Salihbegović-Šahman, S.; Zver, E. Analysis of the funding sources of health systems in the ex-Yugoslavia countries. Med. Časopis 2018, 52, 39–55. [Google Scholar] [CrossRef]
- The World Bank. Current Health Expenditure (% of GDP) Serbia. Available online: https://data.worldbank.org/indicator/SH.XPD.CHEX.GD.ZS?locations=RS (accessed on 15 August 2021).
- Global Health Security Index. 2019 GHS Index Country Profile for Serbia. Available online: https://www.ghsindex.org/wp-content/uploads/2019/08/Serbia.pdf (accessed on 15 August 2021).
- Piroozi, B.; Moradi, G.; Nouri, B.; Bolbanabad, A.M.; Safari, H. Catastrophic health expenditure after the implementation of health sector evolution plan: A case study in the west of Iran. Int. J. Health Policy Manag. 2016, 5, 417. [Google Scholar] [CrossRef]
- Souliotis, K.; Golna, C.; Tountas, Y.; Siskou, O.; Kaitelidou, D.; Liaropoulos, L. Informal payments in the Greek health sector amid the financial crisis: Old habits die last. Eur. J. Health Econ. 2016, 17, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Jeppsson, A.; Okuonzi, S.A. Vertical or holistic decentralization of the health sector? Experiences from Zambia and Uganda. Int. J. Health Plan. Manag. 2000, 15, 273–289. [Google Scholar] [CrossRef] [PubMed]
- Bloom, G.; Xingyuan, G. Health sector reform: Lessons from China. Soc. Sci. Med. 1997, 45, 351–360. [Google Scholar] [CrossRef]
- Cassels, A. Health sector reform: Key issues in less developed countries. J. Int. Dev. 1995, 7, 329–347. [Google Scholar] [CrossRef] [PubMed]
- Franco, L.M.; Bennett, S.; Kanfer, R. Health sector reform and public sector health worker motivation: A conceptual framework. Soc. Sci. Med. 2002, 54, 1255–1266. [Google Scholar] [CrossRef]
- Clark, M.A. Health Sector Reform in Costa Rica: Reinforcing a Public System; Woodrow Wilson Center Workshops on the Politics of Education and Health Reforms: Washington, DC, USA, 2002. [Google Scholar]
- Collins, C.; Green, A.; Hunter, D. Health sector reform and the interpretation of policy context. Health Policy 1999, 47, 69–83. [Google Scholar] [CrossRef]
- Islam, A. Health sector reform in Pakistan: Future directions. J. Pak. Med. Assoc. 2002, 52, 174. [Google Scholar]
- Berdud, M.; Cabasés, J.M.; Nieto, J. Incentives and intrinsic motivation in healthcare. Gac. Sanit. 2016, 30, 408–414. [Google Scholar] [CrossRef]
- Tzeng, H.M. The influence of nurses’ working motivation and job satisfaction on intention to quit: An empirical investigation in Taiwan. Int. J. Nurs. Stud. 2002, 39, 867–878. [Google Scholar] [CrossRef]
- Shah, S.M.; Zaidi, S.; Ahmed, J.; Rehman, S.U. Motivation and retention of physicians in primary healthcare facilities: A qualitative study from Abbottabad, Pakistan. Int. J. Health Policy Manag. 2016, 5, 467. [Google Scholar] [CrossRef]
- Muthuri, R.N.D.K.; Senkubuge, F.; Hongoro, C. Determinants of motivation among healthcare workers in the East African Community between 2009–2019: A systematic review. Healthcare 2020, 8, 164. [Google Scholar] [CrossRef] [PubMed]
- Millar, R.; Chen, Y.; Wang, M.; Fang, L.; Liu, J.; Xuan, Z.; Li, G. It’s all about the money? A qualitative study of healthcare worker motivation in urban China. Int. J. Equity Health 2017, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Latham, G.P.; Ernst, C.T. Keys to motivating tomorrow’s workforce. Hum. Resour. Manag. Rev. 2006, 16, 181–198. [Google Scholar] [CrossRef]
- Meyer, J.P.; Becker, T.E.; Vandenberghe, C. Employee commitment and motivation: A conceptual analysis and integrative model. J. Appl. Psychol. 2004, 89, 991. [Google Scholar] [CrossRef]
- Tella, A.; Ayeni, C.O.; Popoola, S.O. Work Motivation, Job Satisfaction, and Organisational Commitment of Library Personnel in Academic and Research Libraries in Oyo State, Nigeria. Libr. Philos. Pract. 2007, 9, 1–6. Available online: https://digitalcommons.unl.edu/cgi/viewcontent.cgi?article=1118&context=libphilprac (accessed on 28 August 2021).
- Korzynski, P. Employee motivation in new working environment. Int. J. Acad. Res. 2013, 5, 184–188. [Google Scholar] [CrossRef]
- Maslow, A.H. A theory of human motivation. Psychol. Rev. 1943, 50, 370. [Google Scholar] [CrossRef]
- Herzberg, F. One More Time: How Do You Motivate Employees? Harvard Business Review Press: Watertown, MA, USA, 2008. [Google Scholar]
- Lekić, S.; Bogetić, S.; Vidas-Bubanja, M. Educated and satisfied worker: Foundation of modern and successful company. J. Eng. Manag. Compet. (JEMC) 2014, 4, 27–33. [Google Scholar]
- Latham, G.P. Work Motivation: History, Theory, Research, and Practice; Sage: Thousand Oaks, CA, USA, 2012. [Google Scholar]
- Lorincová, S.; Štarchoň, P.; Weberová, D.; Hitka, M.; Lipoldová, M. Employee motivation as a tool to achieve sustainability of business processes. Sustainability 2019, 11, 3509. [Google Scholar] [CrossRef]
- Kovačević, M.; Blagojević, S.; Kuzmanović, B. Sustainability of the motivation policy model for employees in state administration. Sustainability 2020, 12, 7974. [Google Scholar] [CrossRef]
- Van Eerde, W. Motivation and Reward Systems; Wiley Encyclopedia of Management: Hoboken, NJ, USA, 2015; pp. 1–4. [Google Scholar]
- Robescu, O.; Iancu, A.G. The effects of motivation on employees performance in organizations. Valahian J. Econ. Stud. 2016, 7, 49–56. [Google Scholar] [CrossRef][Green Version]
- Tsounis, A.; Bamidis, P.D.; Sarafis, P. Motivation among physicians in Greek public health-care sector. Br. J. Med. Med. Res. 2014, 4, 1094–1105. [Google Scholar] [CrossRef]
- Papac, N.; Pejanović-Škobić, N.; Lesko Bošnjak, L. Non-material motivation strategies of health sector. Zbornik. Radova Ekonomskog. Fakulteta. Sveučilišta u Mostaru. 2020, 26, 165–182. [Google Scholar]
- World Health Organization & United Nations Children’s Fund (UNICEF). In Proceedings of the Report of Global Conference on Primary Health Care: From Alma-Ata towards Universal Health Coverage and the Sustainable Development Goals, Astana, Kazakhstan, 25–26 October 2018.
- Hitka, M.; Rózsa, Z.; Potkány, M.; Ližbetinová, L. Factors forming employee motivation influenced by regional and age-related differences. J. Bus. Econ. Manag. 2019, 20, 674–693. [Google Scholar] [CrossRef]
- Hitka, M.; Balážová, Ž.; Gražulis, V.; Lejskova, P. Differences in employee motivation in selected countries of CEE (Slovakia, Lithuania and the Czech Republic). Eng. Econ. 2018, 29, 536–547. [Google Scholar]
- Salas-Vallina, A.; Ferrer-Franco, A.; Herrera, J. Fostering the healthcare workforce during the COVID-19 pandemic: Shared leadership, social capital, and contagion among health professionals. Int. J. Health Plan. Manag. 2020, 35, 1606–1610. [Google Scholar] [CrossRef]
- Republika Srbija, Ministarstvo Finansija. Ekonomske Mere za Pomoć Privredi i Građanima. Available online: https://mfin.gov.rs/sr/aktivnosti-1/ekonomske-mere-za-pomoc-privredi-i-gradjanima-1 (accessed on 15 August 2021).
- Fajgelj, S. Metode Istraživanja Ponašanja; Centar za Primenjenu Psihologiju: Beograd, Serbia, 2007. [Google Scholar]
- Tabachnick, B.; Fidell, L. Using Multivariate Statistics, 6th ed.; Pearson: New York, NY, USA, 2013. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 8th ed.; Cengage Learning: New York, NY, USA, 2019. [Google Scholar]
- Marsh, H.W.; Hocevar, D. Application of confirmatory factor analysis to the study of self-concept: First-and higher order factor models and their invariance across groups. Psychol. Bull. 1985, 97, 562–582. [Google Scholar] [CrossRef]
- Hu, L.-T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new Alternatives. Struct. Equ. Modeling Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Pallant, J. SPSS Survival Manual—A Step by Step Guide to Data Analysis Using SPSS for Windows, 3rd ed.; Maidenhead Open University Press: Maidenhead, UK, 2016. [Google Scholar]
- Fornell, C.; Larcker, D. Structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- López-Cabarcos, M.; López-Carballeira, A.; Ferro-Soto, C. New ways of working and public healthcare professionals’ well-being: The response to face the COVID-19 pandemic. Sustainability 2020, 12, 8087. [Google Scholar] [CrossRef]
- Kitsios, F.; Kamariotou, M. Job satisfaction behind motivation: An empirical study in public health workers. Heliyon 2021, 7, e06857. [Google Scholar] [CrossRef]
- Optimizacija Mreže Zdravstvenih Ustanova u Srbiji. Novi Master Plan za Novi Zdravstveni Sistem do 2035. Available online: https://optimizacijazdravstva.rs/novi-masterplan-za-novi-zdravstveni-sistem-do-2035 (accessed on 15 August 2021).
- Huber, P.; Schubert, H.J. Attitudes about work engagement of different generations—A cross-sectional study with nurses and supervisors. J. Nurs. Manag. 2019, 27, 1341–1350. [Google Scholar] [CrossRef] [PubMed]
- Schopman, L.M.; Kalshoven, K.; Boon, C. When health care workers perceive high-commitment HRM will they be motivated to continue working in health care? It may depend on their supervisor and intrinsic motivation. Int. J. Hum. Resour. Manag. 2017, 28, 657–677. [Google Scholar] [CrossRef]
- Chmielewska, M.; Stokwiszewski, J.; Filip, J.; Hermanowski, T. Motivation factors affecting the job attitude of medical doctors and the organizational performance of public hospitals in Warsaw, Poland. BMC Health Serv. Res. 2020, 20, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Morishita, K.; Takase, K.; Ishikane, M.; Otomo, Y. Impact of incentives for health-care workers wearing personal protective equipment while dealing with coronavirus disease in Japan. J. Occup. Health 2021, 63, e12213. [Google Scholar] [CrossRef]
- Almaghrabi, R.H.; Alfaradi, H.; Al Hebshi, W.A.; Albaadani, M.M. Healthcare workers experience in dealing with Coronavirus (COVID-19) pandemic. Saudi Med. J. 2020, 41, 657. [Google Scholar] [CrossRef]
- Cardona, L.; Nour, S.; Huffman, K.; Al Qubaisi, S. Short reports: Well-being support of healthcare workers during COVID-19 in the Middle East. Middle East. J. Posit. Psychol. 2020, 6, 97–102. [Google Scholar]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Majumder, P.; Jeve, Y.; Sales, C.P. Voices from the frontline: The psychological impact and coping mechanisms used by healthcare staff during COVID-19. Br. J. Healthc. Manag. 2021, 27, 1–11. [Google Scholar] [CrossRef]
- Neto, M.L.R.; Almeida, H.G.; Esmeraldo, J.D.A.; Nobre, C.B.; Pinheiro, W.R.; de Oliveira, C.R.T.; da Silva, C.G.L. When health professionals look death in the eye: The mental health of professionals who deal daily with the 2019 coronavirus outbreak. Psychiatry Res. 2020, 288, 112972. [Google Scholar] [CrossRef]
- Mitsakis, F.V. Human Resource Development (HRD) resilience: A new ‘success element’ of organizational resilience? Hum. Resour. Dev. Int. 2019, 23, 321–328. [Google Scholar] [CrossRef]
- Li, H.; Yuan, B.; Wang, D.; Meng, Q. Motivating factors on performance of primary care workers in China: A systematic review and meta-analysis. BMJ Open 2019, 9, e8619. [Google Scholar] [CrossRef] [PubMed]
- Adzei, F.A.; Atinga, R.A. Motivation and retention of health workers in Ghana’s district hospitals: Addressing the critical issues. J. Health Organ. Manag. 2012, 26, 467–485. [Google Scholar] [CrossRef] [PubMed]
- Malesic, N.; Mavrak, M.; Rustempasic, N. Management of human resources: Significance of motivation strategy implementation in case of health care workers. Balk. J. Health Sci. 2013, 1, 218. [Google Scholar]



{kind=link}
{kind=link}
| Variables | Percent (%) |
|---|---|
| Gender | |
| Female | 63.8 |
| Male | 36.2 |
| Age | |
| Up to 24 | 18.4 |
| 25–54 | 59.9 |
| ≥55 | 21.7 |
| Education level | |
| High school | 27.1 |
| Bachelor | 49.8 |
| Master | 3.4 |
| Doctoral | 19.8 |
| Employment | |
| Full-time | 51.2 |
| Part-time | 48.8 |
| Working experience | |
| Up to 5 years | 36.7 |
| 6–10 years | 10.6 |
| 11–15 years | 28.5 |
| Over 15 years | 24.2 |
| Working position | |
| Medical staff | 30.4 |
| Head of medical staff | 10.1 |
| Trainee | 26.6 |
| Specialist | 26.6 |
| Head of Department | 6.3 |
| Dimensions | Items |
|---|---|
| EMPLOYMENT: Employment program | I am motivated by engaging in a permanent employment relationship (EMPLOY1) |
| I am motivated by engaging on fixed-term (EMPLOY2) | |
| I am motivated by occasional engagement by other institutions (EMPLOY3) | |
| I am motivated by the possibility of employment in another institution (EMPLOY4) | |
| BONUS: COVID-19 bonus | I am motivated by a one-time financial aid in the amount of 100 euros in dinar equivalent (BONUS1) |
| I am motivated by a one-time financial aid in the amount of 200 euros in dinar equivalent (BONUS2) | |
| I am motivated by a one-time financial aid in the amount of 300 euros in dinar equivalent (BONUS3) | |
| I am motivated by a one-time financial aid in the amount of more than 300 euros in dinar equivalent (BONUS4) | |
| I am motivated by a 10% salary increase (BONUS5) | |
| I am motivated by a 20% salary increase (BONUS6) | |
| I am motivated by a 30% salary increase (BONUS7) | |
| I am motivated by a salary increase of more than 30% (BONUS8) | |
| I am motivated by material rewards for additional work (BONUS9) | |
| I am motivated by material rewards in the form of discounts on travel arrangements (BONUS10) | |
| I am motivated by material rewards in the form of discounts on plane tickets (BONUS11) | |
| TRAINING: Training opportunities | I am motivated by the possibility of specialization (TRAINING1) |
| I am motivated by the possibility of additional training (TRAINING2) | |
| I am motivated by free (paid) online seminars (TRAINING3) | |
| I am motivated by free (paid) online conferences (TRAINING4) | |
| I am motivated by public recognition form my work (TRAINING5) | |
| I am motivated by the possibility of progress (TRAINING6) |
| Dimensions | Items | Eigen Value | % of Variance | Factor Loading |
|---|---|---|---|---|
| Employment program | EMPLOY2 | 1.368 | 13.682 | 0.705 |
| EMPLOY3 | 0.835 | |||
| EMPLOY4 | 0.906 | |||
| COVID-19 bonus | BONUS1 | 2.918 | 29.177 | 0.954 |
| BONUS2 | 0.843 | |||
| BONUS5 | 0.896 | |||
| Training opportunities | OPPORT1 | 3.945 | 39.455 | 0.975 |
| OPPORT2 | 0.958 | |||
| OPPORT4 | 0.706 | |||
| OPPORT6 | 0.910 |
| Dimensions (Factors) | CA | CR | AVE | Employment Program | COVID-19 Bonus | Training Opportunities |
|---|---|---|---|---|---|---|
| Employment program | 0.790 | 0.859 | 0.672 | 0.820 | ||
| COVID-19 bonus | 0.875 | 0.926 | 0.808 | 0.252 | 0.899 | |
| Training opportunities | 0.918 | 0.940 | 0.799 | 0.388 | 0.060 | 0.893 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ćulafić, S.; Janovac, T.; Jovanović, S.V.; Tadić, J.; Jaganjac, J.; Milošević, A.; Bibić, A. State Incentives and Sustainable Motivation System in the Health Sector. Sustainability 2021, 13, 13592. https://doi.org/10.3390/su132413592
Ćulafić S, Janovac T, Jovanović SV, Tadić J, Jaganjac J, Milošević A, Bibić A. State Incentives and Sustainable Motivation System in the Health Sector. Sustainability. 2021; 13(24):13592. https://doi.org/10.3390/su132413592
Chicago/Turabian StyleĆulafić, Slobodan, Tatjana Janovac, Saša Virijević Jovanović, Jelena Tadić, Jamila Jaganjac, Aleksandra Milošević, and Aleksandra Bibić. 2021. "State Incentives and Sustainable Motivation System in the Health Sector" Sustainability 13, no. 24: 13592. https://doi.org/10.3390/su132413592
APA StyleĆulafić, S., Janovac, T., Jovanović, S. V., Tadić, J., Jaganjac, J., Milošević, A., & Bibić, A. (2021). State Incentives and Sustainable Motivation System in the Health Sector. Sustainability, 13(24), 13592. https://doi.org/10.3390/su132413592