
The Effects of Knowledge Types on Consumer Decision Making for Non-Toxic Housing Materials and Products


Abstract
:1. Introduction
2. Literature Review
2.1. Consumer Knowledge
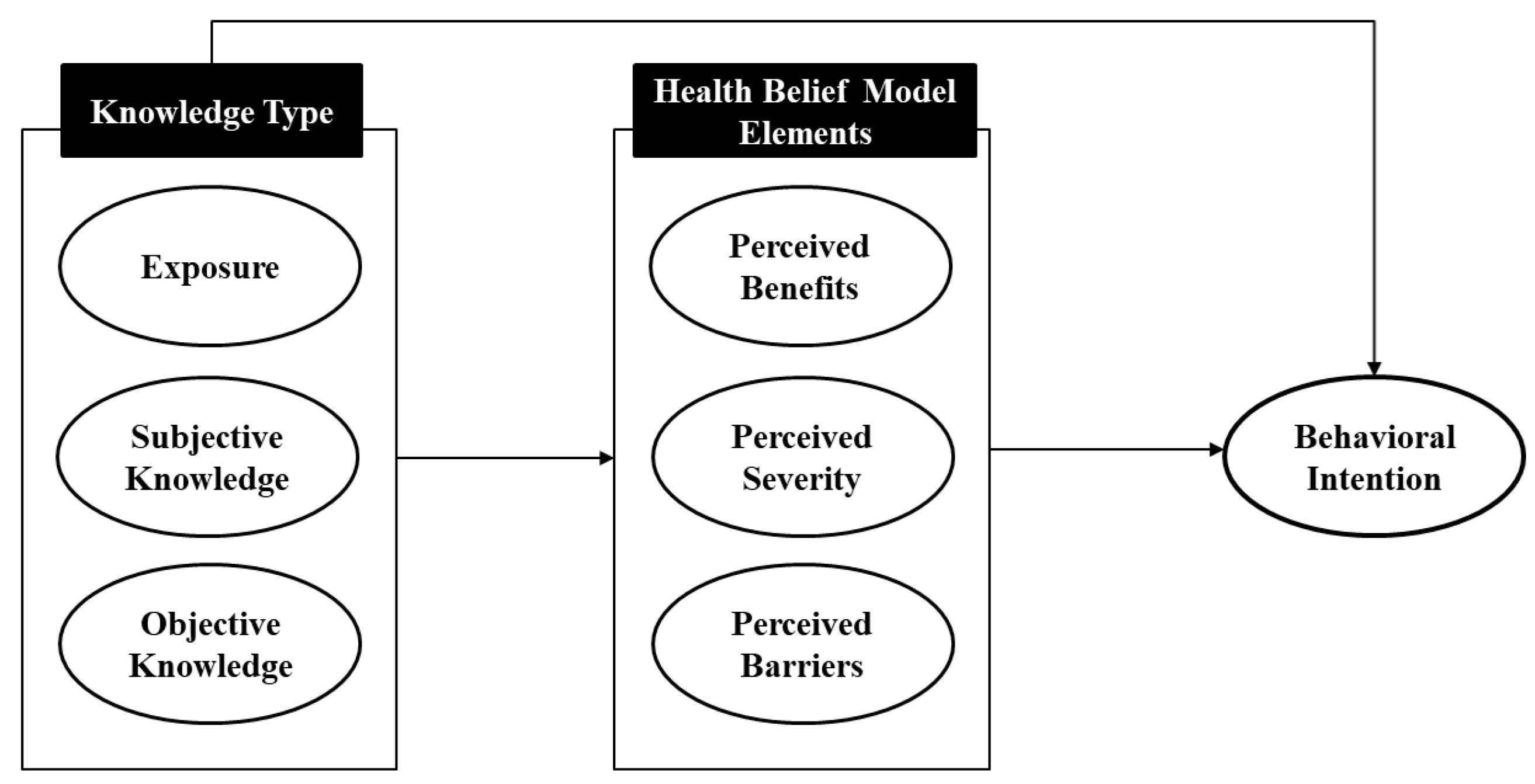
2.2. Health Belief Model
2.3. Interior Materials and Health
2.4. Hypotheses
3. Method
3.1. Data Collection and Sample
3.2. Instruments
3.3. Data Analysis
4. Results
4.1. Measurement Model Testing
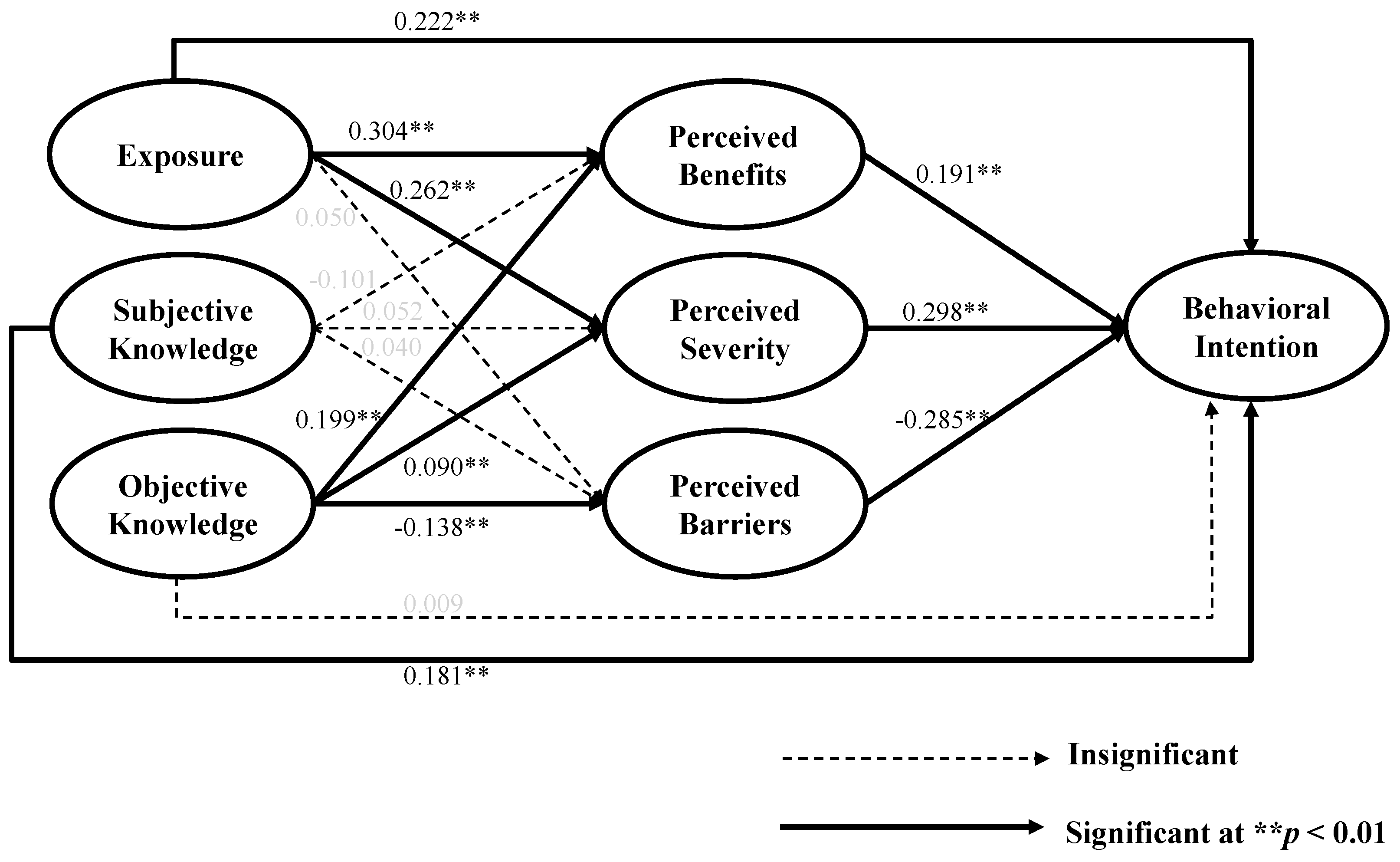
4.2. Structural Model Testing
4.2.1. Direct Effects
4.2.2. Indirect Effects
5. Discussion
6. Implications and Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Klepeis, N.E.; Nelson, W.C.; Ott, W.R.; Robinson, J.P.; Tsang, A.M.; Switzer, P.; Engelmann, W.H. The National Human Activity Pattern Survey (NHAPS): A resource for assessing exposure to environmental pollutants. J. Expo. Sci. Environ. Epidemiol. 2001, 11, 231–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Green Building Council. Green Building 101: What Is Indoor Environmental Quality? Available online: https://www.usgbc.org/articles/green-building-101-what-indoor-environmental-quality (accessed on 25 August 2021).
- Spiegel, R.; Meadows, D. Green Building Materials: A Guide to Product Selection and Specification; John Wiley & Sons: New York, NY, USA, 2010. [Google Scholar]
- American Lung Association. Where VOCs Come from. Clean Air. Available online: https://www.lung.org/clean-air/at-home/indoor-air-pollutants/volatile-organic-compounds (accessed on 25 July 2020).
- Manuel, J. A healthy home environment? Environ. Health Perspect. 1999, 107, A352–A357. [Google Scholar] [CrossRef]
- United States Environmental Protection Agency. Technical Overview of Volatile Organic Compounds. Indoor Air Quality. Available online: https://www.epa.gov/indoor-air-quality-iaq/technical-overview-volatile-organic-compounds (accessed on 25 July 2021).
- Saalberg, Y.; Wolff, M. VOC breath biomarkers in lung cancer. Clin. Chim. Acta 2016, 459, 5–9. [Google Scholar] [CrossRef]
- Ade, R.; Rehm, M. Home is where the health is: What indoor environment quality delivers a “healthy” home? Pac. Rim. Prop. Res. J. 2020, 26, 1–17. [Google Scholar] [CrossRef]
- Sundell, J. On the history of indoor air quality and health. Indoor Air 2004, 14, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.J.; Ahn, M. Boomers’ Intention to Choose Healthy Housing Materials: An Application of the Health Belief Model. Sustainability 2019, 11, 4869. [Google Scholar] [CrossRef] [Green Version]
- Suki, N.M. Green products purchases: Structural relationships of consumers’ perception of eco-label, eco-brand and environmental advertisement. J. Sustain. Sci. Manag. 2013, 8, 1–10. [Google Scholar]
- Wunderlich, S.; Gatto, K.; Smoller, M. Consumer knowledge about food production systems and their purchasing behavior. Environ. Dev. Sustain. 2018, 20, 2871–2881. [Google Scholar] [CrossRef]
- Cook, L.A. Health Belief Model and healthy consumption: Toward an integrated model. J. Food Prod. Mark. 2018, 24, 22–38. [Google Scholar] [CrossRef]
- Hornik, J.; Cherian, J.; Madansky, M.; Narayana, C. Determinants of recycling behavior: A synthesis of research results. J. Socio-Econ. 1995, 24, 105–127. [Google Scholar] [CrossRef]
- Yoon, H.J.; Kim, Y.J. Understanding green advertising attitude and behavioral intention: An application of the health belief model. J. Promot. Manag. 2016, 22, 49–70. [Google Scholar] [CrossRef]
- Lee, J.K.; Lee, W.-N. Country-of-origin effects on consumer product evaluation and purchase intention: The role of objective versus subjective knowledge. J. Int. Consum. Mark. 2009, 21, 137–151. [Google Scholar] [CrossRef]
- Park, C.W.; Lessig, V.P. Familiarity and its impact on consumer decision biases and heuristics. J. Consum. Res. 1981, 8, 223–230. [Google Scholar] [CrossRef]
- Alba, J.W.; Hutchinson, J.W. Dimensions of consumer expertise. J. Consum. Res. 1987, 13, 411–454. [Google Scholar] [CrossRef]
- Flynn, L.R.; Goldsmith, R.E. A short, reliable measure of subjective knowledge. J. Bus. Res. 1999, 46, 57–66. [Google Scholar] [CrossRef]
- Bandura, A. Health promotion by social cognitive means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef] [PubMed]
- Hazavehei, S.; Sharifirad, G.; Mohabi, S. The effect of educational program based on health belief model on diabetic foot care. Int. J. Diabetes Dev. Ctries. 2007, 27, 18–23. [Google Scholar] [CrossRef]
- Sharifirad, G.; Entezari, M.H.; Kamran, A.; Azadbakht, L. The effectiveness of nutritional education on the knowledge of diabetic patients using the health belief model. J. Res. Med. Sci. Off. J. Isfahan Univ. Med. Sci. 2009, 14, 1–6. [Google Scholar]
- Shojaeizadeh, D.; Hashemi, S.Z.; Moeini, B.; Poorolajal, J. The effect of educational program on increasing cervical cancer screening behavior among women in Hamadan, Iran: Applying health belief model. J. Res. Health Sci. 2011, 1, 20–25. [Google Scholar]
- Janz, N.K.; Becker, M.H. The health belief model: A decade later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [Green Version]
- Brucks, M. The effects of product class knowledge on information search behavior. J. Consum. Res. 1985, 12, 1–16. [Google Scholar] [CrossRef]
- Lichtenstein, S.; Fischhoff, B. Do those who know more also know more about how much they know? Organ. Behav. Hum. Perform. 1977, 20, 159–183. [Google Scholar] [CrossRef]
- Skinner, C.S.; Tiro, J.; Champion, V.L. The Health Belief Model. In Health Behavior and Health Education: Theory, Research, and Practice; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; John Wiley & Sons: New York, NY, USA, 2008; pp. 75–94. [Google Scholar]
- Chen, M.-F.; Wang, R.-H.; Schneider, J.K.; Tsai, C.-T.; Jiang, D.D.-S.; Hung, M.-N.; Lin, L.-J. Using the health belief model to understand caregiver factors influencing childhood influenza vaccinations. J. Community Health Nurs. 2011, 28, 29–40. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Wong, P.-F.; Lee, H.Y.; AbuBakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccines Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef]
- Yarbrough, S.S.; Braden, C.J. Utility of health belief model as a guide for explaining or predicting breast cancer screening behaviours. J. Adv. Nurs. 2001, 33, 677–688. [Google Scholar] [CrossRef] [PubMed]
- Abood, D.A.; Black, D.R.; Feral, D. Nutrition education worksite intervention for university staff: Application of the health belief model. J. Nutr. Educ. Behav. 2003, 35, 260–267. [Google Scholar] [CrossRef]
- Huang, X.; Dai, S.; Xu, H. Predicting tourists’ health risk preventative behaviour and travelling satisfaction in Tibet: Combining the theory of planned behaviour and health belief model. Tour. Manag. Perspect. 2020, 33, 100589. [Google Scholar] [CrossRef]
- Msengi, I.G. Development and evaluation of innovative recycling intervention program using the health belief model (HBM). Open J. Prev. Med. 2019, 9, 29–41. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.-S.; Ahn, J.; No, J.-K. Applying the Health Belief Model to college students’ health behavior. Nutr. Res. Pract. 2012, 6, 551–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Didarloo, A.; Nabilou, B.; Khalkhali, H.R. Psychosocial predictors of breast self-examination behavior among female students: An application of the health belief model using logistic regression. BMC Public Health 2017, 17, 861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayele, K.; Tesfa, B.; Abebe, L.; Tilahun, T.; Girma, E. Self care behavior among patients with diabetes in Harari, Eastern Ethiopia: The health belief model perspective. PLoS ONE 2012, 7, e35515. [Google Scholar] [CrossRef] [Green Version]
- Rosenstock, I.M. Why people use health services. Milbank Q. 2005, 83, 94–124. [Google Scholar] [CrossRef]
- Sim, S.W.; Moey, K.S.P.; Tan, N.C. The use of facemasks to prevent respiratory infection: A literature review in the context of the Health Belief Model. Singap. Med. J. 2014, 55, 160–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carpenter, C.J. A meta-analysis of the effectiveness of health belief model variables in predicting behavior. Health Commun. 2010, 25, 661–669. [Google Scholar] [CrossRef] [Green Version]
- Loftness, V.; Hakkinen, B.; Adan, O.; Nevalainen, A. Elements that contribute to healthy building design. Env. Health Perspect. 2007, 115, 965–970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Häyrinen, L.; Toppinen, A.; Toivonen, R. Finnish young adults’ perceptions of the health, well-being and sustainability of wooden interior materials. Scand. J. Res. 2020, 35, 394–402. [Google Scholar] [CrossRef]
- Vaske, J.J.; Needham, M.D.; Stafford, N.T.; Green, K.; Petchenik, J. Information sources and knowledge about chronic wasting disease in Colorado and Wisconsin. Hum. Dimens. Wildl. 2006, 11, 191–202. [Google Scholar] [CrossRef]
- Pieniak, Z.; Aertsens, J.; Verbeke, W. Subjective and objective knowledge as determinants of organic vegetables consumption. Food Qual. Prefer. 2010, 21, 581–588. [Google Scholar] [CrossRef]
- House, L.O.; Lusk, J.; Jaeger, S.R.; Traill, B.; Moore, M.; Valli, C.; Yee, W. Objective and subjective knowledge: Impacts on consumer demand for genetically modified foods in the United States and the European Union. AgBioForum 2004, 7, 113–123. [Google Scholar]
- Cottrell, M. Guide to the LEED Green Associate Exam; John Wiley & Sons: New York, NY, USA, 2010; Volume 17. [Google Scholar]
- Lindsay, J.J.; Strathman, A. Predictors of recycling behavior: An application of a modified health belief model 1. J. Appl. Soc. Psychol. 1997, 27, 1799–1823. [Google Scholar] [CrossRef]
- Deshpande, S.; Basil, M.D.; Basil, D.Z. Factors influencing healthy eating habits among college students: An application of the health belief model. Health Mark. Q. 2009, 26, 145–164. [Google Scholar] [CrossRef] [PubMed]
- Gadenne, D.; Sharma, B.; Kerr, D.; Smith, T. The influence of consumers’ environmental beliefs and attitudes on energy saving behaviours. Energy Policy 2011, 39, 7684–7694. [Google Scholar] [CrossRef]
- Häkkinen, T.; Belloni, K. Barriers and drivers for sustainable building. Build. Res. Inf. 2011, 39, 239–255. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Conner, M.; Norman, P.; Bell, R. The theory of planned behavior and healthy eating. Health Psychol. 2002, 21, 194–201. [Google Scholar] [CrossRef]
- Wiles, J.L.; Leibing, A.; Guberman, N.; Reeve, J.; Allen, R.E. The meaning of “aging in place” to older people. Gerontologist 2012, 52, 357–366. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; Guilford Publications: New York, NY, USA, 2015. [Google Scholar]
- Nunnally, J.C. Psychometric Theory, 3rd ed.; Tata McGraw-Hill Education: New York, NY, USA, 1994. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservablevariables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Anwar, K.; Climis, R. Analyzing the relationship between types of advertisement and customer choice: A study of retailer stores in erbil. Int. J. Acc. Bus. Soc. 2017, 25, 43–52. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.J.; Yoon, H.J. Predicting green advertising attitude and behavioral intention in South Korea. Soc. Behav. Personal. Int. J. 2017, 45, 1345–1364. [Google Scholar] [CrossRef]
- Fredrica, R. Consumer Food Selection and Nutrition Information; Praeger: New York, NY, USA, 1979. [Google Scholar]
- Park, C.W.; Mothersbaugh, D.L.; Feick, L. Consumer knowledge assessment. J. Consum. Res. 1994, 21, 71–82. [Google Scholar] [CrossRef]
- Lee, M.; Zhao, J.; Sun, Q.; Pan, Y.; Zhou, W.; Xiong, C.; Zhang, L. Human mobility trends during the early stage of the COVID-19 pandemic in the United States. PLoS ONE 2020, 15, e0241468. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographics and Housing Specifications | n | % |
|---|---|---|
| Gender | ||
| Male | 501 | 47.7 |
| Female | 534 | 50.9 |
| Race | ||
| White | 468 | 44.6 |
| Hispanic | 176 | 16.8 |
| Other | 94 | 9.0 |
| Marital Status | ||
| Married | 490 | 46.7 |
| Other a | 560 | 53.3 |
| Work Status | ||
| Full time b | 392 | 37.3 |
| Part time c | 133 | 12.7 |
| Not working d | 525 | 50.0 |
| Education | ||
| High school or lower | 333 | 31.7 |
| College or higher | 717 | 68.3 |
| Annual Household Income | ||
| Less than $25,000 | 252 | 24.0 |
| $25,000–$49,999 | 309 | 29.5 |
| $50,000–$99,999 | 322 | 30.6 |
| $100,00–$149,000 | 110 | 10.5 |
| $150,000 or more | 57 | 5.4 |
| House Type | ||
| Single family home | 698 | 66.5 |
| Other e | 352 | 33.5 |
| Location | ||
| Rural areas | 244 | 23.2 |
| City suburb | 500 | 47.6 |
| Urban areas | 306 | 29.1 |
| Tenant Type | ||
| Own | 646 | 61.5 |
| Rent | 404 | 38.5 |
| Length of Residency | ||
| Less than 10 years | 562 | 53.5 |
| 11–20 years | 248 | 23.6 |
| 21–30 years | 142 | 13.5 |
| More than 30 years | 98 | 9.3 |
| Total Valid Responses | 1050 f | 100.0 |
| Construct (Scale) |
| Exposure |
| EI1. I have heard and/or read about non-toxic housing materials and products from (you can choose more than one answer). |
| Print news articles or magazines |
| TV |
| Radio |
| Internet |
| Friends and family |
| Organizations |
| Sales person |
| EI2. How often did you see or hear about non-toxic housing materials and products within the last year? (1 = never; 5 = very often) |
| Subjective Knowledge (1 = strongly disagree; 5 = strongly agree) |
| SN1. I feel comfortable purchasing non-toxic housing materials and products due to my prior knowledge. * |
| SN2. Compared to others, I think I know less about non-toxic housing materials and products. (R) ** |
| SN3. When it comes to non-toxic housing materials and products, I don’t know a lot. (R) * |
| SN4. I am knowledgeable about how to evaluate the quality of non-toxic housing materials and products. |
| SN5. People who know me consider me as an expert in non-toxic housing materials and products. |
| Objective Knowledge (0 = All incorrect; 7 = All correct) |
| ON1. I have heard about Sick Building Syndrome. (1 = Yes; 0 = No) |
| ON2. Carpet adhesives may contain toxic chemicals. (1 = Yes; 0 = No) |
| ON3. Chemical cleaning products may affect indoor air quality and health. (1 = Yes; 0 = No) |
| ON4. Low-emitting housing materials should be used rather than conventional products because of their reduced off-gassing with harmful contaminants. (1 = Yes; 0 = No) |
| ON5. Formaldehyde is a toxic building material. (1 = Yes; 0 = No) |
| ON6. Asbestos is a good building material related to health. (1 = No; 0 = Yes) |
| ON7. VOCs (Volatile organic compounds) are toxic building materials. (1 = Yes; 0 = No) |
| Perceived Benefits |
| PBN1. To what extend to do you think using non-toxic housing materials and products is good for your health? (1 = not at all good; 5 = extremely good) |
| PBN2. To what extend to do you think using non-toxic housing materials and products is good for your quality of life? (1 = not at all good; 5 = extremely good) |
| PBN3. I think I could save on medical expenses if I choose non-toxic housing materials and products. (1 = strongly disagree; 5 = strongly agree) * |
| Perceived Severity (1 = strongly disagree; 5 = strongly agree) |
| PS1. How severe would it be to your health if you do not use non-toxic housing materials and products in your house? (1 = not at all severe; 5 = extremely severe) |
| PS2. I will have long-lasting effects. |
| PS3. I will be bed-ridden for a long time. * |
| PS4. I will have high medical expenses. |
| PS5. It will be harmful for my family life. |
| Perceived Barriers (1 = strongly disagree; 5 = strongly agree) |
| PBR1. I think there are enough options of non-toxic housing materials and products for my house. (R) ** |
| PBR2. I think most non-toxic housing materials and products look good. (R) * |
| PBR3. I think non-toxic housing materials and products have poor brand images. |
| PBR4. I think it would take too much time choosing non-toxic housing materials and products. * |
| PBR5. I think it would take too much effort to choose non-toxic housing materials and products. |
| PBR6. I think choosing non-toxic housing materials and products would be too expensive. |
| PBR7. I don’t expect non-toxic housing materials and products to be cost-effective. |
| PBR8. Due to lack of information, it is hard to choose non-toxic housing materials and products. * |
| PBR9. Even though there are non-toxic housing materials and products information, it is hard to believe the labeling/measurement standard. * |
| PBR10. It is hard to believe the performance of the non-toxic housing materials and products. |
| Behavioral Intention |
| INT1. I intend to choose non-toxic housing materials and products in the future. (1 = definitely do not; 5 = definitely do) |
| INT2. I want to choose non-toxic housing materials and products in the future. (1 = strongly disagree; 5 = strongly agree) * |
| INT3. I am determined to choose non-toxic housing materials and products in the future. (1 = very unlikely; 5 = very likely) |
| INT4. How likely is it that you will choose non-toxic housing materials and products in the future? (1 = very unlikely; 5 = very likely) |
| Construct/Items | M | SD | CFA Loading | α | Composite Reliability | AVE | |
|---|---|---|---|---|---|---|---|
| Exposure | 0.63 | 0.66 | 0.50 | ||||
| EI1 | 1.80 | 1.16 | 0.56 | ||||
| EI2 | 2.34 | 1.00 | 0.83 | ||||
| Subjective Knowledge | 2.97 | 1.19 | 0.79 | 0.79 | 0.65 | ||
| SN4 | 3.08 | 1.14 | 0.79 | ||||
| SN5 | 2.37 | 1.25 | 0.82 | ||||
| Objective Knowledge | N/A | N/A | |||||
| ON | 5.19 | 1.27 | N/A | N/A | |||
| Perceived Benefits | 3.92 | 0.97 | 0.89 | 0.89 | 0.80 | ||
| PBN1 | 3.93 | 0.98 | 0.89 | ||||
| PBN2 | 3.92 | 0.96 | 0.90 | ||||
| Perceived Severity | 3.30 | 1.12 | 0.79 | 0.80 | 0.51 | ||
| PS1 | 3.20 | 1.12 | 0.54 | ||||
| PS2 | 3.50 | 1.00 | 0.67 | ||||
| PS4 | 3.07 | 1.14 | 0.79 | ||||
| PS5 | 3.44 | 1.12 | 0.82 | ||||
| Perceived Barriers | 2.99 | 1.03 | 0.78 | 0.79 | 0.43 | ||
| PBR3 | 2.85 | 0.96 | 0.52 | ||||
| PBR5 | 2.67 | 1.10 | 0.77 | ||||
| PBR6 | 3.28 | 1.06 | 0.69 | ||||
| PBR7 | 3.09 | 1.04 | 0.59 | ||||
| PBR10 | 3.09 | 0.99 | 0.66 | ||||
| Behavioral Intention | 3.94 | 0.97 | 0.92 | 0.92 | 0.80 | ||
| INT1 | 3.94 | 0.94 | 0.83 | ||||
| INT3 | 3.80 | 1.00 | 0.93 | ||||
| INT4 | 3.88 | 0.98 | 0.92 | ||||
| Construct | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| 1 = Exposure | 0.50 | ||||||
| 2 = Subjective Knowledge | 0.15 | 0.65 | |||||
| 3 = Objective Knowledge | 0.01 | 0.00 | N/A | ||||
| 4 = Perceived Benefits | 0.04 | 0.00 | 0.05 | 0.80 | |||
| 5 = Perceived Severity | 0.04 | 0.03 | 0.01 | 0.10 | 0.51 | ||
| 6 = Perceived Barriers | 0.00 | 0.00 | 0.01 | 0.01 | 0.00 | 0.43 | |
| 7 = Behavioral Intention | 0.10 | 0.10 | 0.02 | 0.12 | 0.18 | 0.05 | 0.80 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, H.J.; Ahn, M.; Kang, J. The Effects of Knowledge Types on Consumer Decision Making for Non-Toxic Housing Materials and Products. Sustainability 2021, 13, 11024. https://doi.org/10.3390/su131911024
Kwon HJ, Ahn M, Kang J. The Effects of Knowledge Types on Consumer Decision Making for Non-Toxic Housing Materials and Products. Sustainability. 2021; 13(19):11024. https://doi.org/10.3390/su131911024
Chicago/Turabian StyleKwon, Hyun Joo, Mira Ahn, and Jiyun Kang. 2021. "The Effects of Knowledge Types on Consumer Decision Making for Non-Toxic Housing Materials and Products" Sustainability 13, no. 19: 11024. https://doi.org/10.3390/su131911024
APA StyleKwon, H. J., Ahn, M., & Kang, J. (2021). The Effects of Knowledge Types on Consumer Decision Making for Non-Toxic Housing Materials and Products. Sustainability, 13(19), 11024. https://doi.org/10.3390/su131911024