
Determinants of Physical Activity Practices in Metropolitan Context: The Case of Lisbon Metropolitan Area, Portugal



Abstract
1. Introduction
- Intrapersonal dimension: age; sex; physical problems; fear of falling; fatigue; lack of interest or motivation; pain; laziness; financial cost; individual beliefs; household chores; security concerns; single or widower status; unpleasant experience; lack of self-discipline; low level of education; heavy weight, among others;
- Interpersonal dimension: having no companion; family responsibilities; inadequate information; social pressure; need to spent time with other activities; lack of exercise clubs devoted to youth, among others;
- Environmental dimension: physical barriers to walking; season and weather, namely very high or low temperature or rain; lack of facilities for exercise; high traffic; inappropriateness of the timing of sports classes; lack of personal safety; difficulty commuting and distance from home to sports facilities.
- Does an urban occupation model generate distinct practices of physical activity?
- Is income a differentiating factor when compared with other sociodemographic characteristics of households?
- Can individual perceptions of oneself and of the neighborhood promotes physical activity practices?
2. Materials and Methods
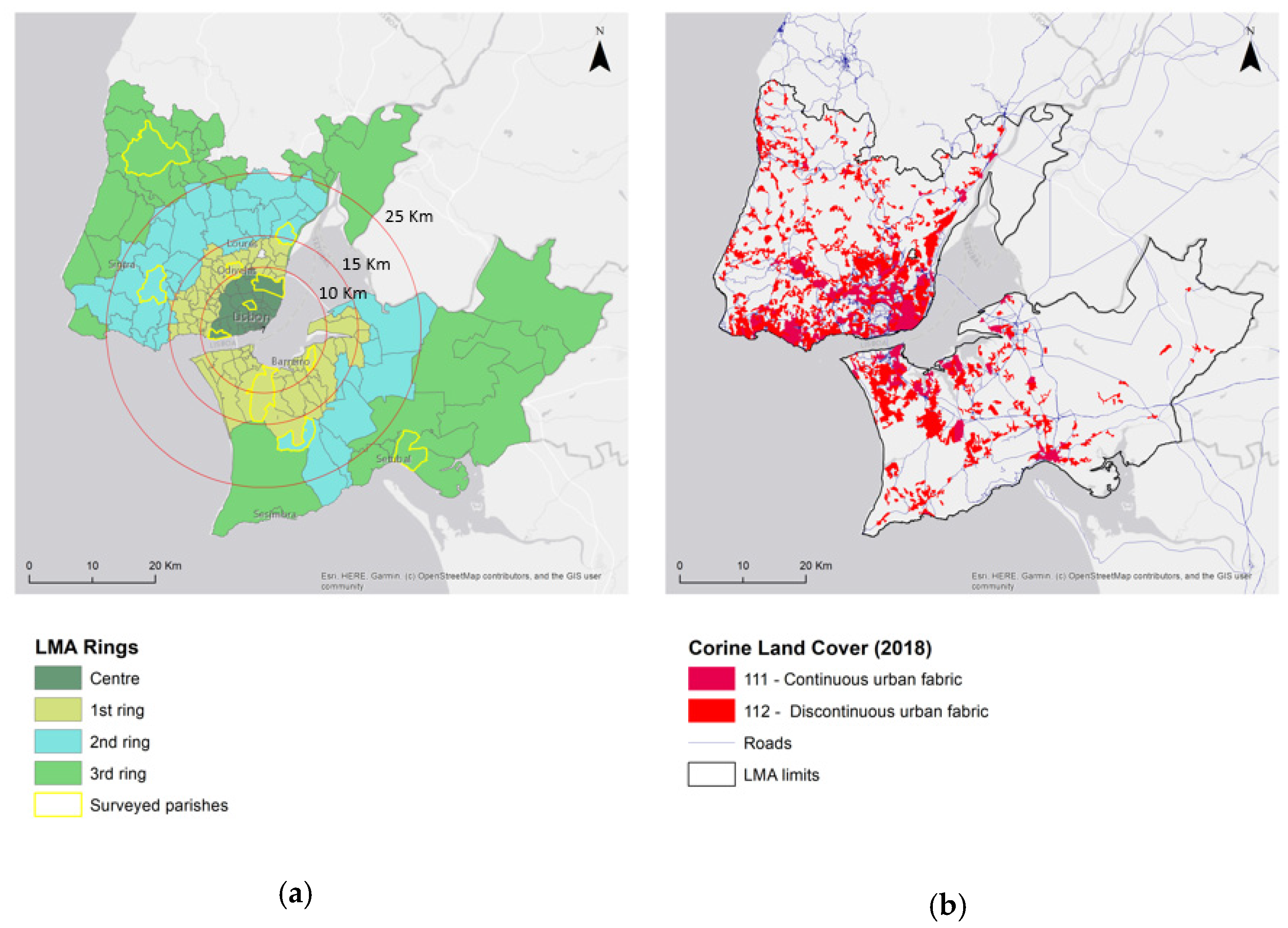
2.1. Study Design and Sampling
2.2. Data Processing and Statistical Analysis
- Descriptive and bivariate data analysis to understand the physical activity practices of the families, namely the characteristics of the demands (Which activities are developed? Where are the practices? When do they occur?);
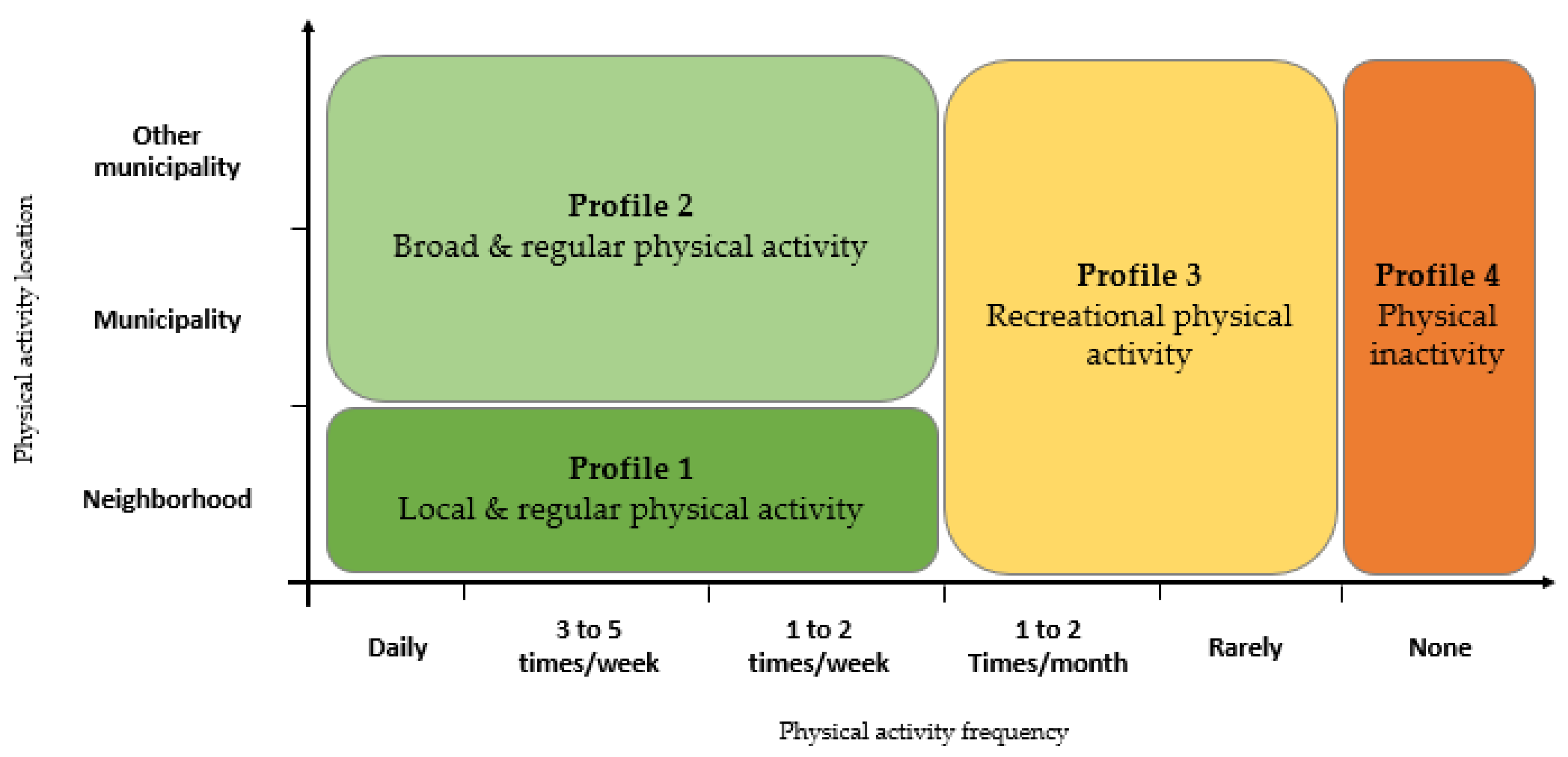
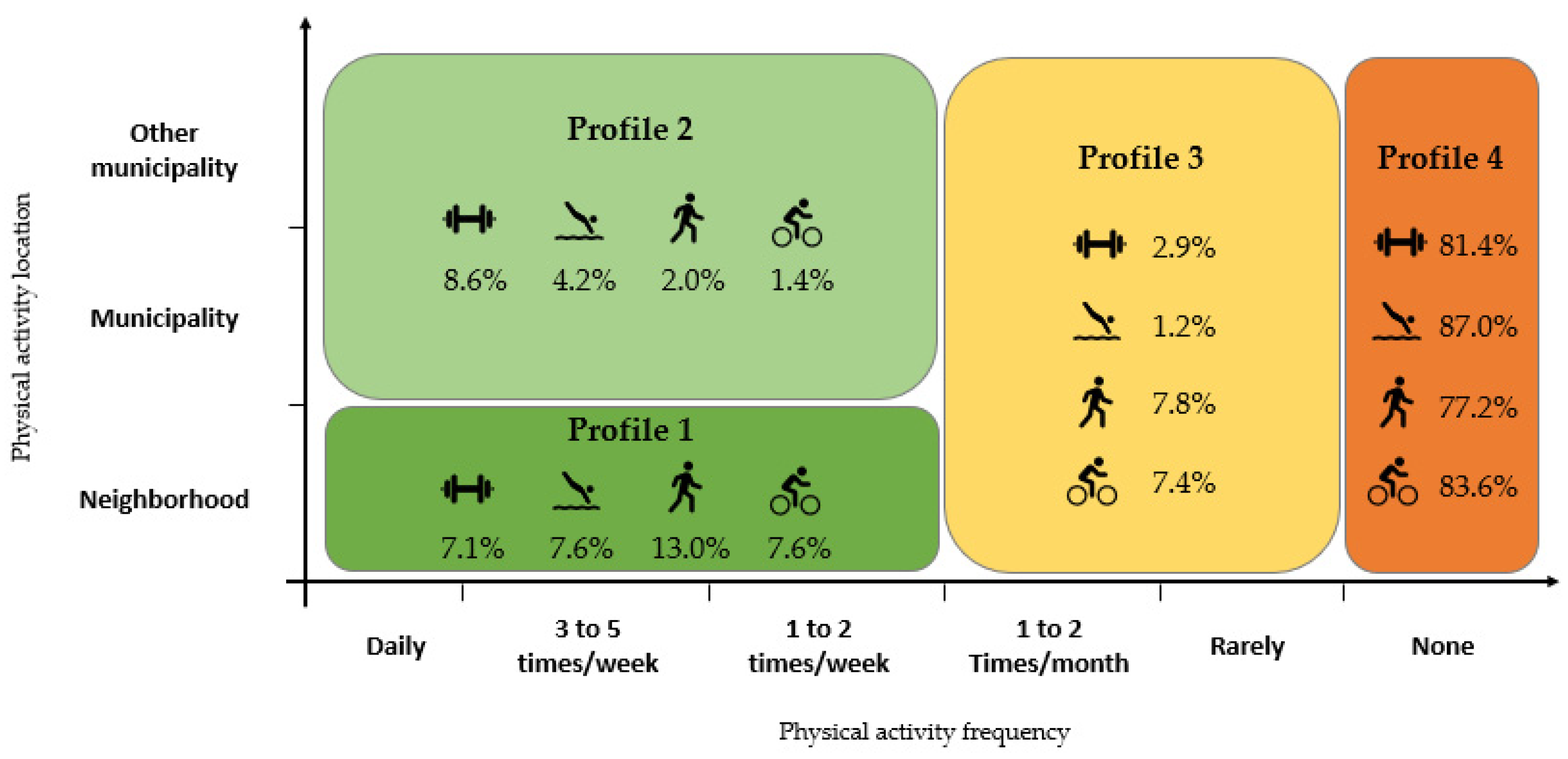
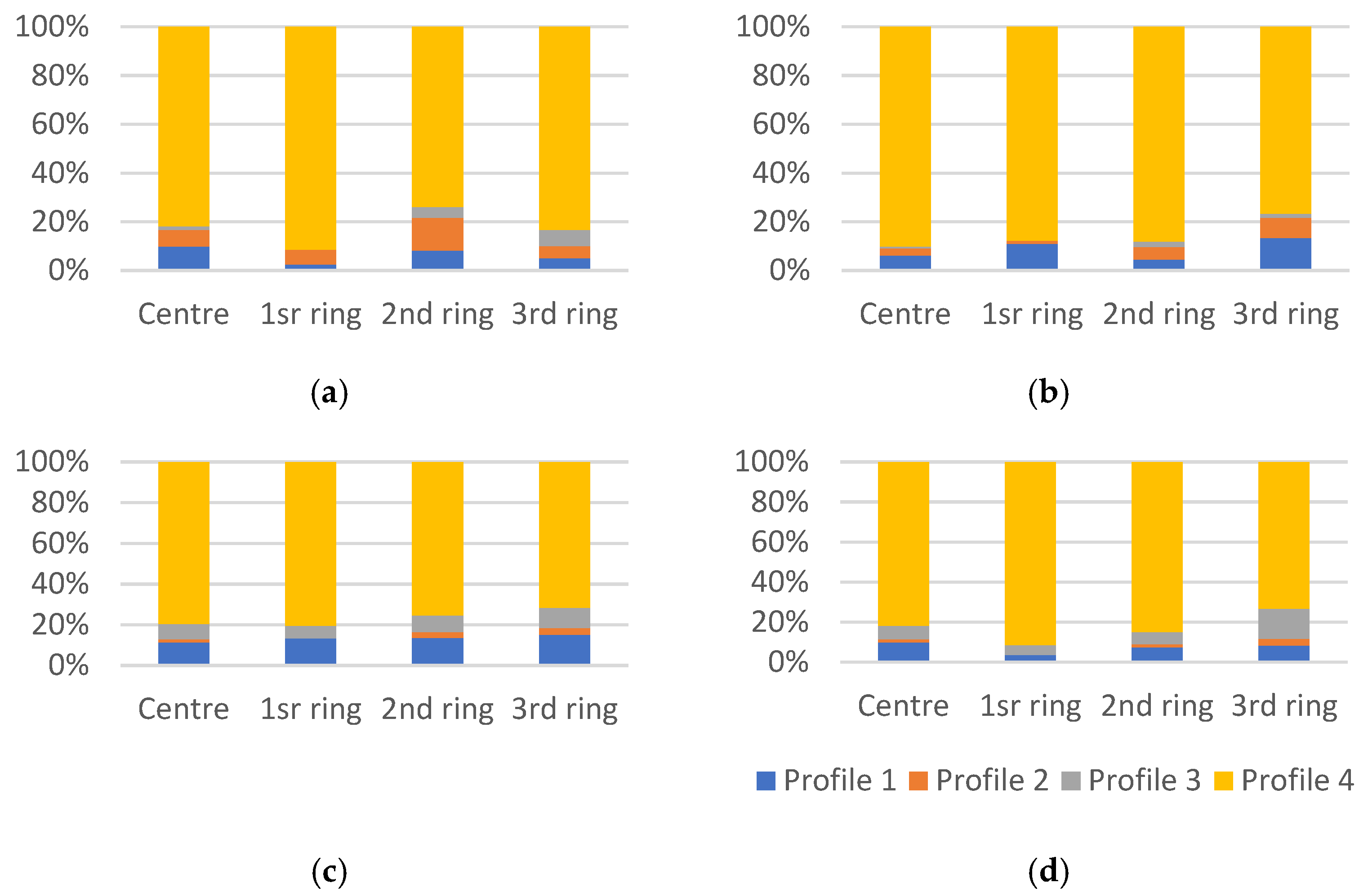
- Definition of four physical activity profiles of families (based on frequency and location of the practice of each physical activity in study) and analysis of the profiles’ distribution by each physical activity. Physical activity profiles of families followed the scheme shown in Figure 2:
- Profile 1. Local and regular physical activity—representing families that practice a certain activity at least once a week in the neighborhood of residence.
- Profile 2. Broad and regular physical activity—representing families that practice a certain activity at least once a week in the municipality (excluding the neighborhood of residence) or in another municipality.
- Profile 3. Recreational physical activity—representing families that practice a certain activity with low regularity (maximum of twice a month);
- Profile 4. Physical inactivity—representing families that do not practice a certain activity at all.
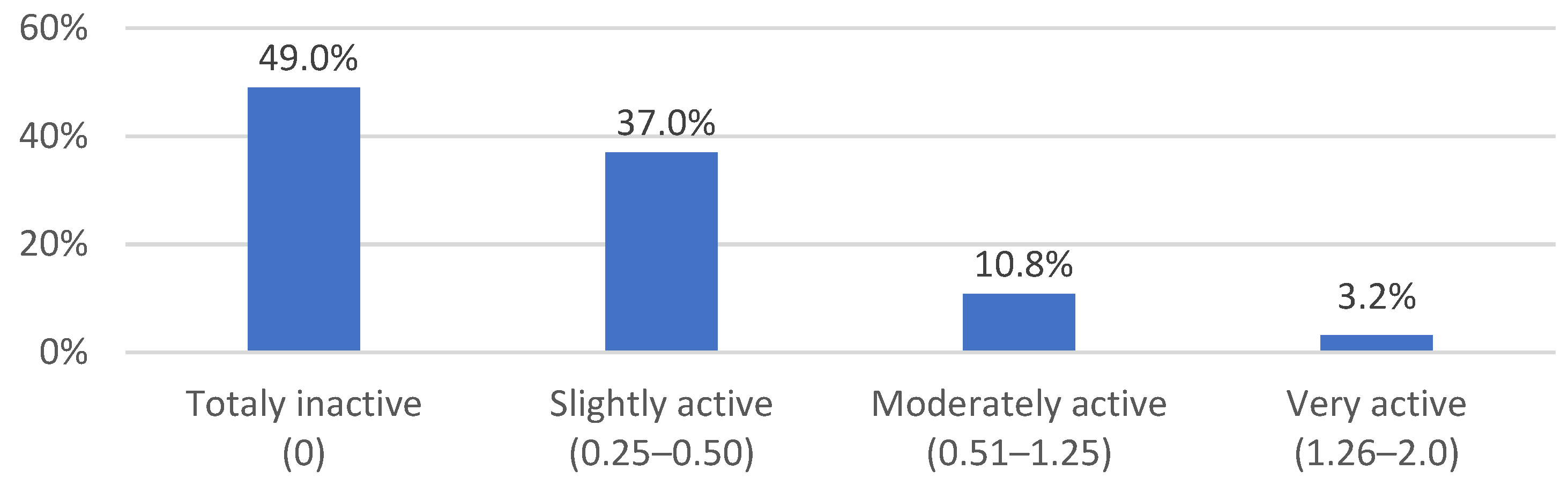
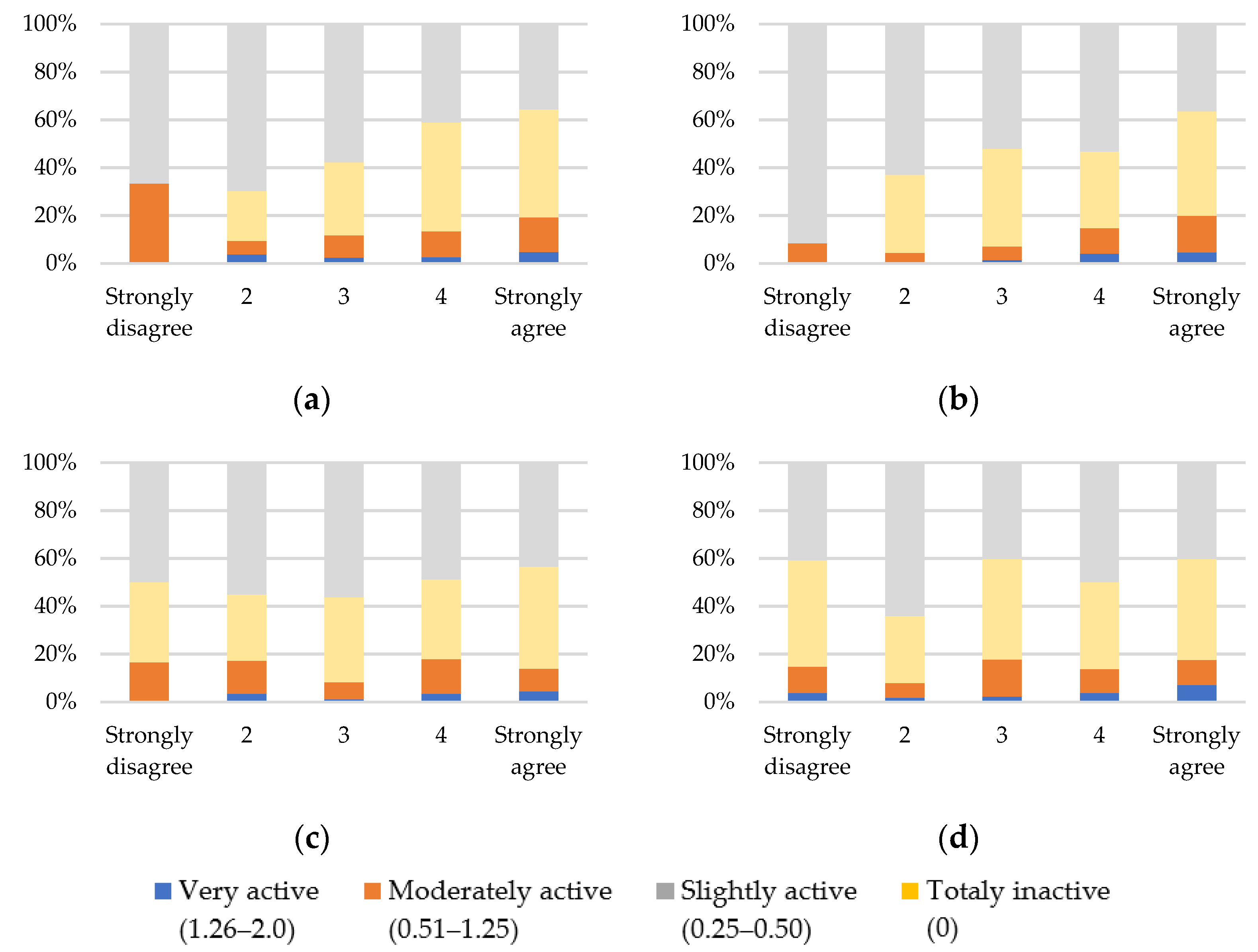
- Definition of the intensity level of physical activity of families. The intensity level is calculated through the average of the weight given by the physical activity profile of each family for every physical activity. The weights are as follows: 2 points for Profiles 1 and 2; 1 point for profile 3; 0 points for profile 4. The level of intensity is thus between 0, representing families that do not perform any of the physical activities, and 2, representing families that perform the four studied activities (gym, swimming, walking, and cycling) frequently (twice a week minimum). This produced four levels of physical activity intensity:
- Level 1. Totally inactive family (0)—representing families that practice none of the four activities;
- Level 2. Slightly active family (0.25 to 0.5)—representing families that practice some activity but not in a regular manner;
- Level 3. Moderately active family (0.51 to 1.25)—representing families that practice some activities in a regular and/or in a recreational manner;
- Level 4. Very active family (1.26 to 2.0)—representing families that practice several of the studied activities in a regular manner.
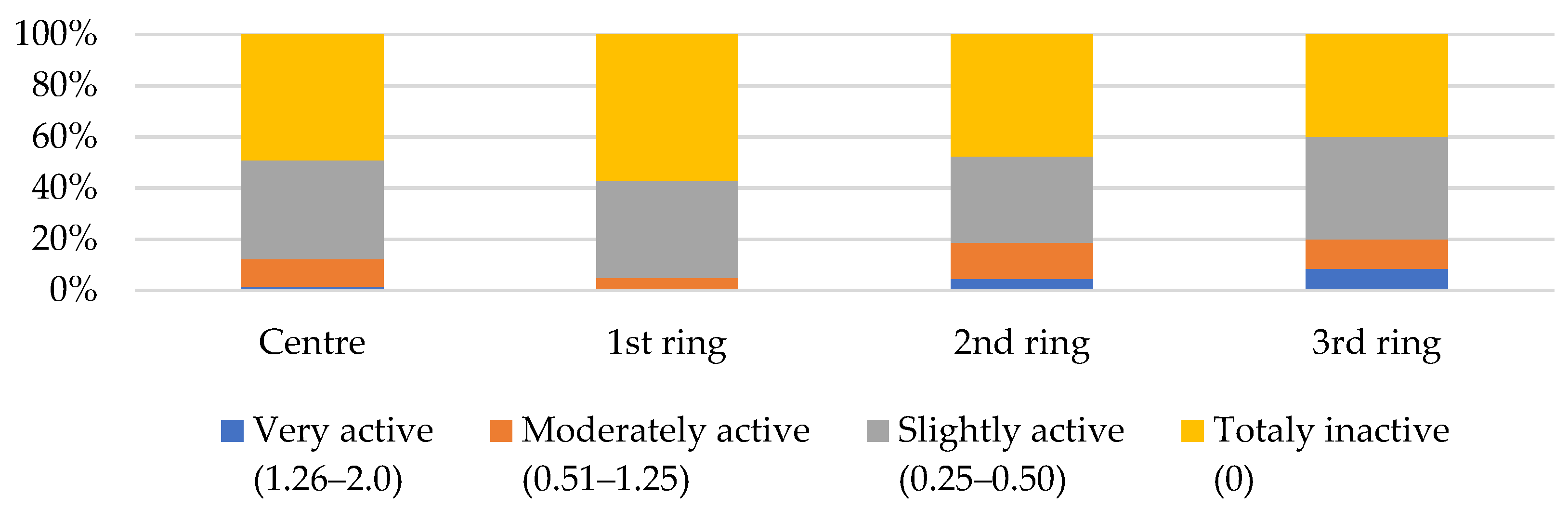
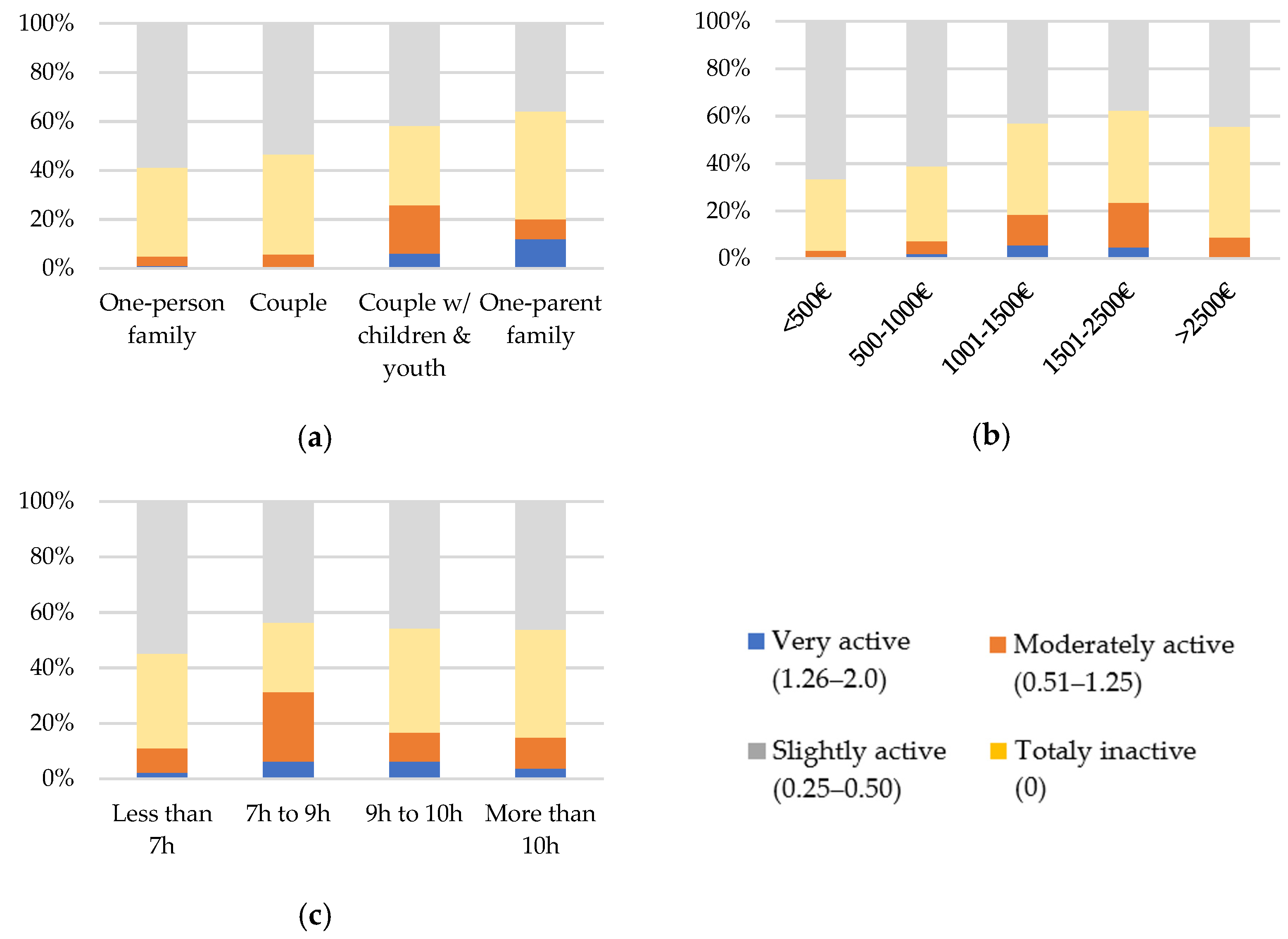
- Bivariate data analysis of the relationship between the previous profiles and intensity of physical activity level of families and various territorial and individual specificities:
- (i)
- (ii)
- (iii)
3. Results
3.1. Physical Activity Practices in the LMA
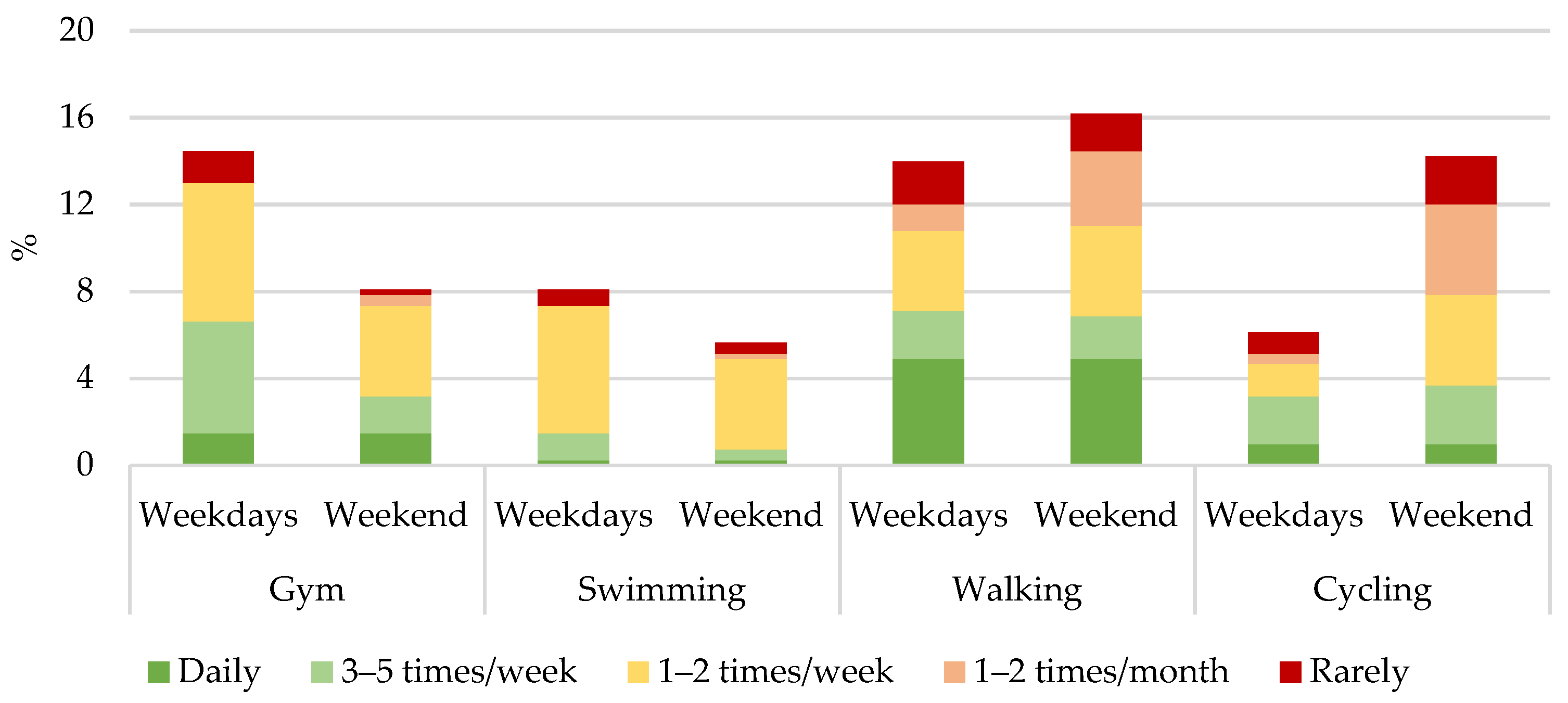
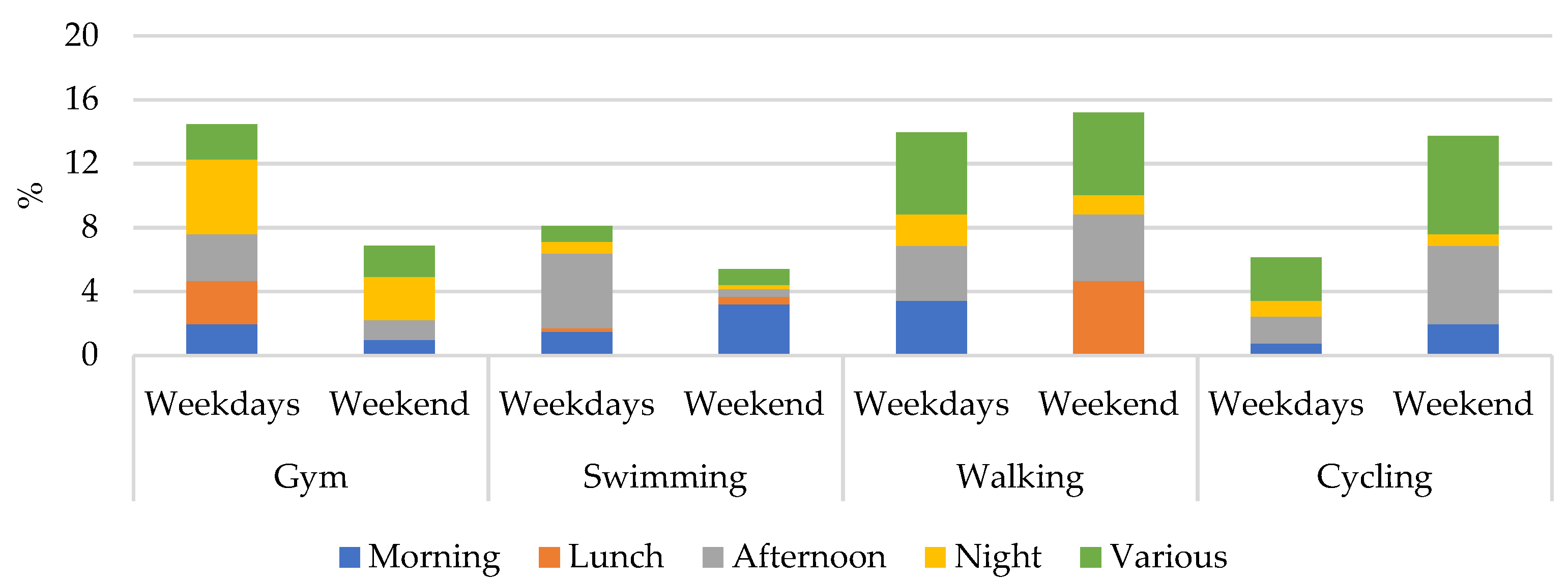
3.1.1. Physical Activity in the Daily Life of Families
3.1.2. Physical Activity Profile and Intensity Level of Families
3.2. Relation between Physical Activity and Urban and Individual Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Carrapato, P.; Correia, P.; Garcia, B. Determinante da saúde no Brasil: A procura da equidade na saúde. Saude Soc. 2017, 26, 676–689. [Google Scholar] [CrossRef]
- Marmot, M.; Allen, J.; Bell, R.; Bloomer, E.; Goldblatt, P. WHO European review of social determinants of health and the health divide. Lancet 2012, 380, 1011–1029. [Google Scholar] [CrossRef]
- Marmot, M.; Bell, R. Fair society, healthy lives. Public Health 2012, 126, S4–S10. [Google Scholar] [CrossRef] [PubMed]
- Marques da Costa, E.; Kállay, T. Impacts of Green Spaces on Physical and Mental Health—Thematic Report. EU, URBACT. Available online: https://urbact.eu/impacts-green-spaces-physical-and-mental-health-thematic-report (accessed on 30 August 2021).
- World Urbanization Prospects—United Nations. Available online: https://population.un.org/wup/Download/ (accessed on 10 June 2021).
- Baptista, F.; Silva, A.M.; Santos, D.A.; Mota, J.; Santos, R.; Vale, S.; Ferreira, J.P.; Raimundo, A.; Moreira, M.H. Livro Verde da Actividade Física; IDP: Lisboa, Portugal, 2011. [Google Scholar]
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.-P.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Connor Gorber, S.; Kho, M.E. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, S197–S239. [Google Scholar] [CrossRef]
- Valdés-Badilla, P.A.; Gutiérrez-García, C.; Pérez-Gutiérrez, M.; Vargas-Vitoria, R.; López-Fuenzalida, A. Effects of physical activity governmental programs on health status in independent older adults: A systematic review. J. Aging Phys. Act 2019, 27, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Naci, H.; Ioannidis, J.P.A. Comparative effectiveness of exercise and drug interventions on mortality outcomes: Metaepidemiological study. Br. J. Sports Med. 2015, 49, 1414–1422. [Google Scholar] [CrossRef] [PubMed]
- Blair, S.N.; Cheng, Y.; Holder, S.; Barlow, C.E.; Kampert, J.B. Physical Activity or Cardiorespiratory Fitness. Med. Sci. Sport. Exerc. 2001, 33, S275. [Google Scholar] [CrossRef]
- Jakicic, J.M.; Kraus, W.E.; Powell, K.E.; Campbell, W.W.; Janz, K.F.; Troiano, R.P.; Sprow, K.; Torres, A.; Piercy, K.L. Association between bout duration of physical activity and health: Systematic review. Med. Sci. Sport. Exerc. 2019, 51, 1213–1219. [Google Scholar] [CrossRef]
- Warburton, D.E.R.; Nicol, C.W.; Bredin, S.S.D. Health benefits of physical activity: The evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef]
- World Health Organization. Steps to Health: A European Framework to Promote Physical Activity for Health; WHO Regional Office for Europe: Copenhagen, Denmark, 2007. [Google Scholar]
- World Health Organization. Recommended Amount of Physical Activity; WHO Regional Office for Europe: Copenhagen, Denmark, 2008. [Google Scholar]
- World Health Organization. NCDs|Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World, WHO; World Health Organization: Copenhagen, Denmark, 2019. [Google Scholar]
- Zaitune, M.P.D.A.; Barros, M.B.D.A.; César, C.L.G.; Carandina, L.; Goldbaum, M. Fatores associados ao sedentarismo no lazer em idosos, Campinas, São Paulo, Brasil. Cad. Saude Publica 2007, 23, 1329–1338. [Google Scholar] [CrossRef]
- Cavill, N.; Kahlmeier, S.; Racioppi, F. Physical Activity and Health in Europe: Evidence for Action; World Health Organization: Copenhagen, Denmark, 2006. [Google Scholar]
- World Health Organization. Good Health Starts with Healthy Behaviour; World Health Organization: Copenhagen, Denmark, 2011. [Google Scholar]
- Miles, L. Physical activity and health. Nutr. Bull. 2007, 32, 314–363. [Google Scholar] [CrossRef]
- The Global Health Observatory—Indicators. Available online: https://www.who.int/data/gho/data/indicators (accessed on 10 December 2020).
- Direção-Geral da Saúde. Programa Nacional Para a Promoção da Atividade Física; DGS: Lisboa, Portugal, 2019. [Google Scholar]
- Inquérito Nacional de Saúde—Instituto Nacional de Estatística. Available online: https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_destaques&DESTAQUESdest_boui=414434213&DESTAQUESmodo=2 (accessed on 10 December 2020).
- Kretschmer, A.C.; Dumith, S.C. Prática de atividade física no lazer e ambiente percebido: Um estudo de base populacional com adultos e idosos do Sul do Brasil. Rev. Bras. Epidemiol. 2020, 23, 1–13. [Google Scholar] [CrossRef]
- Bolívar, J.; Daponte, A.; Rodríguez, M.; Sánchez, J.J. The Influence of Individual, Social and Physical Environment Factors on Physical Activity in the Adult Population in Andalusia, Spain. Int. J. Environ. Res. Public Health 2010, 7, 60–77. [Google Scholar] [CrossRef]
- Bauman, A.; Reis, R.; Sallis, J.; Wells, J.; Loos, R.; Martin, B. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Kelso, A.; Reimers, A.K.; Abu-Omar, K.; Wunsch, K.; Niessner, C.; Wäsche, H.; Demetriou, Y. Locations of Physical Activity: Where Are Children, Adolescents, and Adults Physically Active? A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 1240. [Google Scholar] [CrossRef]
- Marques da Costa, E.; Fumega, J.; Louro, A. Defining sustainable communities: Development of a toolkit for policy orientation. J. Urban Regen. Renew. 2013, 6, 278–292. [Google Scholar]
- Flood, S.M.; Moen, P. Healthy Time Use in the Encore Years: Do Work, Resources, Relations, and Gender Matter? J. Health Soc. Behav. 2015, 56, 74–97. [Google Scholar] [CrossRef] [PubMed]
- Nossa, P. Abordagem Geográfica da Oferta e Consumo de Cuidados de Saúde. Doctorate Thesis, Universidade do Minho, Guimarães, Portugal, 2005. [Google Scholar]
- Franco, P.; Marques da Costa, E. Atividade física no quotidiano familiar das periferias: Uma visão a partir de Rio de Mouro—Sintra. Finisterra 2021, 56, 183–203. [Google Scholar] [CrossRef]
- Malta, F.S.; da Costa, E.M.; Magrini, A. Socio-environmental vulnerability index: A methodological proposal based on the case of Rio de Janeiro, Brazil/Indice de vulnerabilidade socioambiental: Uma proposta metodológica utilizando o caso do Rio de Janeiro, Brasil. Cien Saude Colet 2017, 22, 3933–3944. [Google Scholar] [CrossRef] [PubMed]
- Malta, F.S.; Marques da Costa, E. Socio-Environmental vulnerability Index: An Application to Rio de Janeiro-Brazil. Int. J. Public Health 2021, 66, 584308. [Google Scholar] [CrossRef]
- Gomes, D.F.; Dias, M.; Martins, F.; Damásio, A.; Campos, F. Relação entre frequência de prática e importância atribuída pelos praticantes. Phys. Educ. Sport. Pedagog. 2020, 6, 20–25. [Google Scholar] [CrossRef]
- Cohen, D.A.; Han, B.; Derose, K.P.; Williamson, S.; Marsh, T.; Raaen, L.; McKenzie, T.L. Promoting physical activity in high-poverty neighborhood parks: A cluster randomized controlled trial. Soc. Sci. Med. 2017, 186, 130–138. [Google Scholar] [CrossRef]
- Gómez, A.; Costa, C.; Santana, P. Acessibilidade e utilização dos espaços verdes urbanos nas cidades de Coimbra (Portugal) e Salamanca (Espanha). Finisterra 2014, 49, 49–68. [Google Scholar] [CrossRef]
- Greer, A.E.; Castrogivanni, B.; Marcello, R. Park Use and Physical Activity Among Mostly Low-to-Middle Income, Minority Parents and Their Children. J. Phys. Act. Health 2017, 14, 83–87. [Google Scholar] [CrossRef]
- Gintoli, I.; Bellisario, V.; Squillacioti, G.; Caputo, M.; Borraccino, A.; Dalmasso, P.; Bono, R.; Lemma, P. Urbanization and greenness in HBSC survey: Association with life satisfaction and health complaints. Eur. J. Public Health 2020, 30, ckaa166.099. [Google Scholar] [CrossRef]
- Matisziw, T.C.; Nilon, C.H.; Wilhelm Stanis, S.A.; LeMaster, J.W.; McElroy, J.A.; Sayers, S.P. The right space at the right time: The relationship between children’s physical activity and land use/land cover. Landsc. Urban Plan. 2016, 151, 21–32. [Google Scholar] [CrossRef]
- Jáuregui, A.; Lambert, E.V.; Panter, J.; Moore, C.; Salvo, D. Scaling up urban infrastructure for physical activity in the COVID-19 pandemic and beyohd. Lancet 2021, 398, 370–372. [Google Scholar] [CrossRef]
- Louro, A.; Marques da Costa, N. Mobilidade urbana e municípios saudáveis na AML: Tendências entre as últimas duas décadas (2000 e 2010). Finisterra 2019, 54, 71–95. [Google Scholar] [CrossRef]
- Morseth, B.; Jacobsen, B.K.; Emaus, N.; Wilsgaard, T.; Jørgensen, L. Secular trends and correlates of physical activity: The Tromsø Study 1979-2008. BMC Public Health 2016, 16, 1215. [Google Scholar] [CrossRef]
- Fan, X.; Zhu, Z.; Zhuang, J.; Liu, Y.; Tang, Y.; Chen, P.; Cao, Z.B. Gender and age differences in the association between living arrangement and physical activity levels among youth aged 9–19 years in Shanghai, China: A cross-sectional questionnaire study. BMC Public Health 2019, 19, 1030. [Google Scholar] [CrossRef]
- Meijer, E.; Goris, A.; Wouters, L.; Westerterp, K.R. Physical inactivity as a determinant of the physical activity level in the elderly. Int. J Obes. 2001, 25, 935–939. [Google Scholar] [CrossRef]
- Pereira, M.; Mota, J.; Nogueira, H.; Santos, M. Determinantes ambientais e sociais nos níveis de actividade física dos adolescentes. Utilização de metodologias SIG. Finisterra 2012, 46, 107–118. [Google Scholar] [CrossRef]
- Du, J.; Yagihashi, T. Health capital investment and time spent on health-related activities. Rev. Econ. Househ. 2017, 15, 1215–1248. [Google Scholar] [CrossRef]
- Dumuid, D.; Olds, T.; Sawyer, S.M. Moving beyond more: Towards a healthy balance of daily behaviours. Lancet 2021, 398, 373–374. [Google Scholar] [CrossRef]
- García, J.A. Time use patterns of Spanish people at weekends: In search of what, who and when. Leis. Stud. 2017, 36, 793–810. [Google Scholar] [CrossRef]
- Parent-Thirion, A.; Macías, E.F.; Hurley, J.; Vermeylen, G. Fourth European Working Conditions Survey; Office for Official Publications of the European Communities: Dublin, Ireland, 2007. [Google Scholar]
- Torres, A.; Brites, R.; Lapa, T.; Haas, B.; Steiber, N. First European Quality of Life Survey: Time Use and Work—Life Options over the Life Course; Office for Official Publications of the European Communities: Dublin, Ireland, 2007. [Google Scholar]
- Cerin, E.; Mitáš, J.; Cain, K.L.; Conway, T.L.; Adams, M.A.; Schofield, G.; Sarmiento, O.L.; Reis, R.S.; Schipperijn, J.; Davey, R.; et al. Do associations between objectively-assessed physical activity and neighborhood environment attributes vary by time of the day and day of the week? IPEN adult study. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 34. [Google Scholar] [CrossRef]
- De Sousa, M.; Reeve, C.L.; Peterman, A.H. Development and Initial Validation of the Perceived Scarcity Scale (PScS). Stress Health 2019, 36, 131–146. [Google Scholar] [CrossRef]
- Rudd, M. Feeling short on time: Trends, consequences, and possible remedies. Curr. Opin. Psychol. 2019, 26, 5–10. [Google Scholar] [CrossRef]
- Naegele, G.; Barkholdt, C.; de Vroom, B.; Andersen, J.G.; Krämer, K.; Andersen, J.G.; Krämer, K. A new organization of time over working life—Results from a European Foundation research project of the same name. In Soziale Lebenslaufpolitik; Naegele, G., Ed.; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2010; pp. 110–137. [Google Scholar] [CrossRef]
- Louro, A.; Marques da Costa, N. Indicadores de transporte e mobilidade urbana para cidades saudáveis—Caso da Área Metropolitana de Lisboa, Portugal. GeoUERJ 2017, 30, 99–121. [Google Scholar] [CrossRef][Green Version]
- Yun, H.Y. Neighborhood Built Environments, Walking, and Self-Rated Health among Low-Income Older Adults in St. Paul, Minnesota. Sustainability 2021, 13, 3501. [Google Scholar] [CrossRef]
- Herazo-Beltrán, Y.; Pinillos, Y.; Vidarte, J.; Crissien, E.; Suarez, D.; García, R. Predictors of perceived barriers to physical activity in the general adult population: A cross-sectional study. Braz. J. Phys. Ther 2017, 21, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Cerin, E.; Owen, N.; Oyeyemi, A.L.; Conway, T.L.; Van Dyck, D.; Schipperijn, J.; Macfarlane, D.J.; Salvo, D.; Reis, R.S.; et al. Perceived neighborhood environmental attributes associated with adults[U+05F3] recreational walking: IPEN Adult study in 12 countries. Health Place 2014, 28, 22–30. [Google Scholar] [CrossRef]
- Ou, J.Y.; Levy, J.I.; Peters, J.L.; Bongiovanni, R.; Garcia-Soto, J.; Medina, R.; Scammell, M.K. A walk in the park: The influence of urban parks and community violence on physical activity in Chelsea, MA. Int. J. Environ. Res. Public Health 2016, 13, 97. [Google Scholar] [CrossRef] [PubMed]
- Rees-Punia, E.; Hathaway, E.D.; Gay, J.L. Crime, perceived safety, and physical activity: A meta-analysis. Prev. Med. 2018, 111, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Corburn, J. Equitable and healthy city planning: Towards healthy urban governance in the century of the city. In Healthy Cities: The Theory, Policy, and Practice of Value-Based Urban Planning; de Leeuw, E., Simos, J., Eds.; Springer: New York, NY, USA, 2017; pp. 31–41. [Google Scholar]
- Corburn, J. Urban place and health equity: Critical issues and practices. Int. J. Environ. Res. Public Health 2017, 14, 117. [Google Scholar] [CrossRef] [PubMed]
- Hoehner, C.M.; Brennan, L.K.; Brownson, R.C.; Handy, S.L.; Killingsworth, R. Opportunities for Integrating Public Health and Urban Planning Approaches to Promote Active Community Environments. Am. J. Health Promot. 2003, 18, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Louro, A.; Marques da Costa, N.; Marques da Costa, E. From livable communities to livable metropolis: Challenges for urban mobility in Lisbon Metropolitan Area (Portugal). Int. J. Environ. Res. Public Health 2021, 18, 3525. [Google Scholar] [CrossRef]
- Censos da População—Instituto Nacional de Estatística. Available online: https://censos.ine.pt/xportal/xmain?xpid=CENSOS&xpgid=censos2011_apresentacao (accessed on 12 April 2018).
- Corine Land Cover—Copernicus. Available online: https://land.copernicus.eu/pan-european/corine-land-cover (accessed on 29 May 2021).
- Ferdinand, A.O.; Sen, B.; Rahurkar, S.; Engler, S.; Menachemi, N. The relationship between built environments and physical activity: A systematic review. Am. J. Public Health 2012, 102, e7–e13. [Google Scholar] [CrossRef] [PubMed]
- King, A.C.; Stokols, D.; Talen, E.; Brassington, G.S.; Killingsworth, R. Theoretical approaches to the promotion of physical activity: Forging a transdisciplinary paradigm. Am. J. Prev. Med. 2002, 23, 15–25. [Google Scholar] [CrossRef]
- Pereira Neiva, H.; Brandão Faíl, L.; José Silva, A.; Almeida Marinho, D. Caracterização dos utilizadores de piscinas em Portugal: Práticas usuais e motivações. RIAA 2019, 3, 3–7. [Google Scholar] [CrossRef]
- Almeida, D. A Emergência Low-Cost: Drivers que Influenciam o Comportamento do Consumidor na Escolha do Ginásio. Master’s Thesis, ISCTE Business School, Lisbon, Portugal, 2017. Available online: https://repositorio.iscte-iul.pt/handle/10071/16367 (accessed on 18 May 2021).
- Louro, A.; Marques da Costa, N.; Marques da Costa, E. Sustainable Urban Mobility Policies as a Path to Healthy Cities—The Case Study of LMA, Portugal. Sustainability 2019, 11, 2929. [Google Scholar] [CrossRef]
- Mitten, D.; Overholt, J.R.; Haynes, F.I.; D’Amore, C.C.; Ady, J.C. Hiking: A Low-Cost, Accessible Intervention to Promote Health Benefits. Am. J. Lifestyle Med. 2018, 12, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.L.; Jago, R.; Brockman, R.; Cartwright, K.; Page, A.S.; Fox, K.R. Physically active families—De-bunking the myth? A qualitative study of family participation in physical activity. Child Care Health Dev. 2010, 36, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Yarmohammadi, S.; Mozafar Saadati, H.; Ghaffari, M.; Ramezankhani, A. A systematic review of barriers and motivators to physical activity in elderly adults in Iran and worldwide. Epidemiol. Health 2019, 41, e2019049. [Google Scholar] [CrossRef] [PubMed]
- Sousa, P.; Marques da Costa, N.; Marques da Costa, E.; Ricoca Peixoto, V.; Campos Fernandes, A.; Gaspar, R.; Duarte-Ramos, F.; Abrantes, P.; Leite, A. COMPRIME—COnhecer Mais PaRa Intervir MElhor: Preliminary Mapping of Municipal Level Determinants of COVID-19 Transmission in Portugal at Different Moments of the 1st Epidemic Wave. Port. J. Public Health 2021, 38, 18–25. [Google Scholar] [CrossRef]
- Marques da Costa, E.; Marques da Costa, N. O processo pandémico da COVID-19 em Portugal Continental. Análise geográfica dos primeiros 100 dias. Finisterra 2020, 55, 11–18. [Google Scholar] [CrossRef]
- Long, T.Q. Individual Subjective Well-Being during the COVID-19 Pandemic. Sustainability 2021, 13, 7816. [Google Scholar] [CrossRef]
- Jornal de Negócios. Ginásios e Piscinas Voltam a Funcionar. Saiba Quais as Regras que Terá de Seguir. Available online: https://www.jornaldenegocios.pt/economia/coronavirus/detalhe/ginasios-e-piscinas-voltam-a-funcionar-saiba-quais-as-regras-que-tera-de-seguir (accessed on 27 April 2021).
- Sábado. Covid-19: Lisboetas Saem à Rua Para Passear e Praticar Exercício Físico. Available online: https://www.sabado.pt/portugal/detalhe/covid-19-lisboetas-saem-a-rua-para-passear-e-praticar-exercicio-fisico (accessed on 27 May 2021).
- Google. COVID-19 Community Mobility Reports (Portugal). Available online: https://www.gstatic.com/covid19/mobility/2021-08-09_PT_Mobility_Report_pt-PT.pdf (accessed on 27 May 2021).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Census (INE, 2011) | Survey (2018) | |||||||
|---|---|---|---|---|---|---|---|---|
| Private Households | Residents | Private Households | Residents | |||||
| n | % | n | % | n | % | n | % | |
| Center | 486,044 | 42.3 | 1,135,343 | 40.3 | 132 | 32.2 | 304 | 30.2 |
| 1st ring | 235,384 | 20.5 | 589,151 | 20.9 | 84 | 20.5 | 214 | 21.3 |
| 2nd ring | 293,784 | 25.6 | 761,306 | 27.0 | 134 | 32.7 | 337 | 33.5 |
| 3rd ring | 132,563 | 11.5 | 330,076 | 11.7 | 60 | 14.6 | 151 | 15.0 |
| Total | 1,147,775 | 100.0 | 2,815,876 | 100.0 | 410 | 100.0 | 1006 | 100.0 |
| Practice of Physical Activity | n | % | |
|---|---|---|---|
| Practice of, at least, one physical activity | No | 200 | 49.0 |
| Yes | 208 | 51.0 | |
| Type of activity 1 | Gym | 76 | 18.6 |
| Swimming | 53 | 13.0 | |
| Walking/hiking/trekking | 93 | 22.8 | |
| Cycling | 67 | 16.4 | |
| Frequency 2 | Daily | 38 | 13.1 |
| 3 to 5 times a week | 51 | 17.6 | |
| 1 to 2 times a week | 120 | 41.5 | |
| 1 to 2 times per month | 37 | 12.8 | |
| Rarely | 43 | 14.9 | |
| Most frequent location 2 | In the parish of residence | 193 | 67.0 |
| In the municipality of residence | 64 | 22.2 | |
| Another municipality | 19 | 6.6 | |
| Don’t know/Don’t answer | 12 | 4.2 | |
| Transport mode used 2 | Soft modes | 173 | 59.9 |
| Collective transports | 12 | 4.2 | |
| Individual transports | 81 | 28.0 | |
| Combination of modes | 8 | 2.8 | |
| Don’t know/Don’t answer | 15 | 5.2 |
| Practice of Physical Activity | Yes | No | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Typology of households | One-person family | 42 | 41.2 | 60 | 58.8 |
| Couple without children | 41 | 46.6 | 47 | 53.4 | |
| Couple with children | 86 | 58.1 | 62 | 41.9 | |
| One-parent family | 16 | 64.0 | 9 | 36.0 | |
| Others | 23 | 51.1 | 22 | 48.9 | |
| Existence of children and youth (until 17 years old) | Yes | 74 | 61.2 | 47 | 38.8 |
| No | 134 | 46.7 | 153 | 53.3 | |
| Existence of elders (65 or more years old) | Yes | 47 | 42.7 | 63 | 57.3 |
| No | 161 | 54.0 | 137 | 46.0 | |
| Practice of Any Physical Activity by Type of Family |  Gym |  Swimming |  Walking/Trekking/Hiking |  Cycling |
|---|---|---|---|---|
One-person family 41.2% 41.2% | 15.7% | 5.9% | 20.6% | 6.9% |
Couple without children 46.6% 46.6% | 17.0% | 5.7% | 26.1% | 4.6% |
Couple with children 58.1% 58.1% | 21.6% | 22.3% | 19.6% | 29.7% |
One-parent family 64.0% 64.0% | 16.0% | 28.0% | 32.9% | 24.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Louro, A.; Franco, P.; Marques da Costa, E. Determinants of Physical Activity Practices in Metropolitan Context: The Case of Lisbon Metropolitan Area, Portugal. Sustainability 2021, 13, 10104. https://doi.org/10.3390/su131810104
Louro A, Franco P, Marques da Costa E. Determinants of Physical Activity Practices in Metropolitan Context: The Case of Lisbon Metropolitan Area, Portugal. Sustainability. 2021; 13(18):10104. https://doi.org/10.3390/su131810104
Chicago/Turabian StyleLouro, Ana, Pedro Franco, and Eduarda Marques da Costa. 2021. "Determinants of Physical Activity Practices in Metropolitan Context: The Case of Lisbon Metropolitan Area, Portugal" Sustainability 13, no. 18: 10104. https://doi.org/10.3390/su131810104
APA StyleLouro, A., Franco, P., & Marques da Costa, E. (2021). Determinants of Physical Activity Practices in Metropolitan Context: The Case of Lisbon Metropolitan Area, Portugal. Sustainability, 13(18), 10104. https://doi.org/10.3390/su131810104