Health Risks in Our Environment: Urban Slum Youth’ Perspectives Using Photovoice in Kampala, Uganda



Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Study Area and Setting
2.3. Selection of Study Participants
2.4. Training Workshop
2.5. Photography Assignment
2.6. Discussing Photos and Data Analysis
2.7. Ethical Considerations
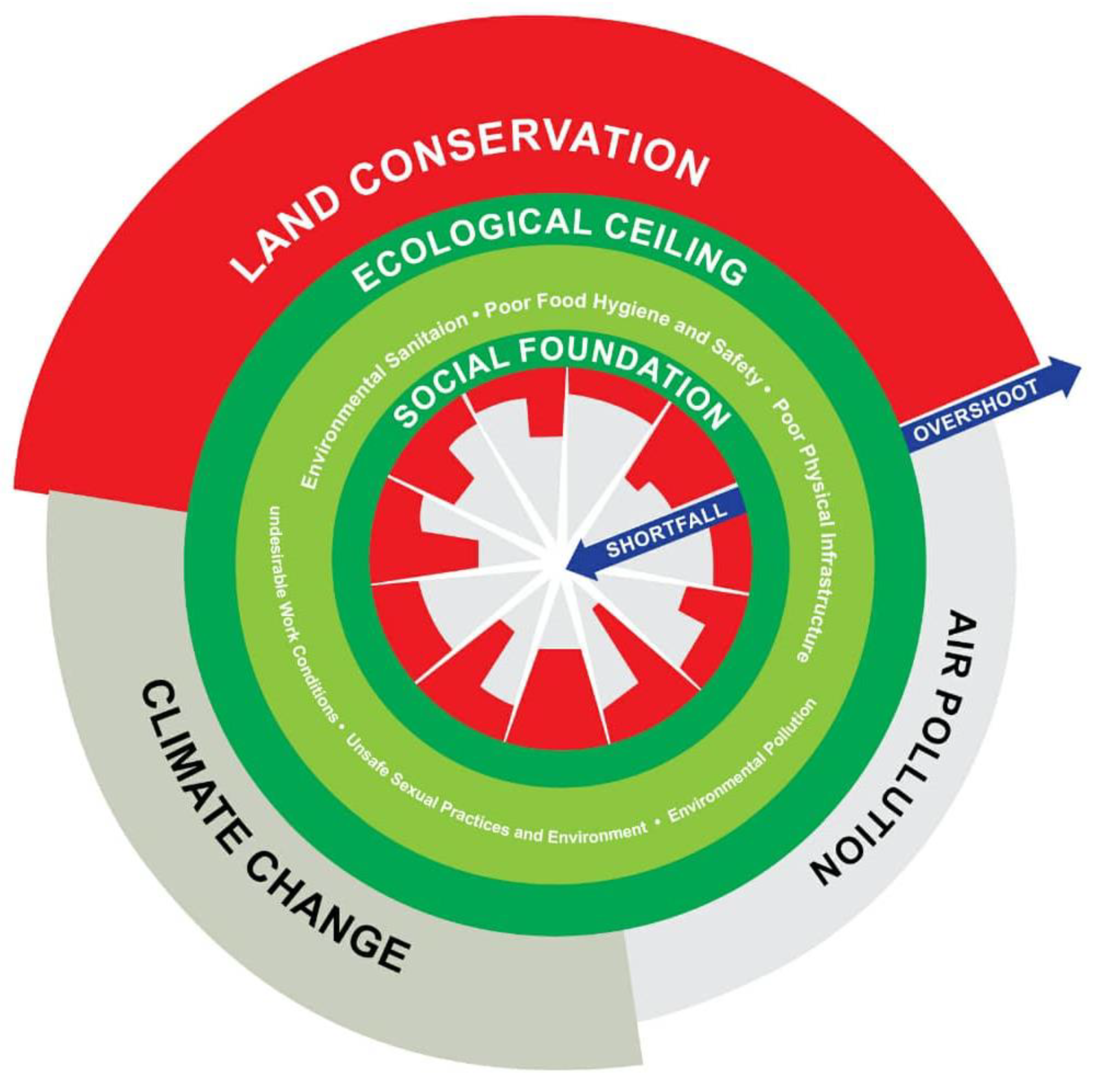
3. Results
3.1. Social Foundation Shortfalls
3.1.1. Environmental Sanitation
“Garbage is collected at one point as people wait for the garbage truck to pick it. The truck often delays for days and the garbage accumulates all over the place while attracting flies. It makes the place unhygienic and spreads diseases.”(Photographer 4, Female, 23 years)
“Someone was bathing in the bathroom, but the wastewater is moving straight into the stormwater channels. The wastewater is stagnated in the stormwater channel and thus could cause diarrheal diseases, cholera especially if children play in that kind of water”(Photographer 6, male, age 22)
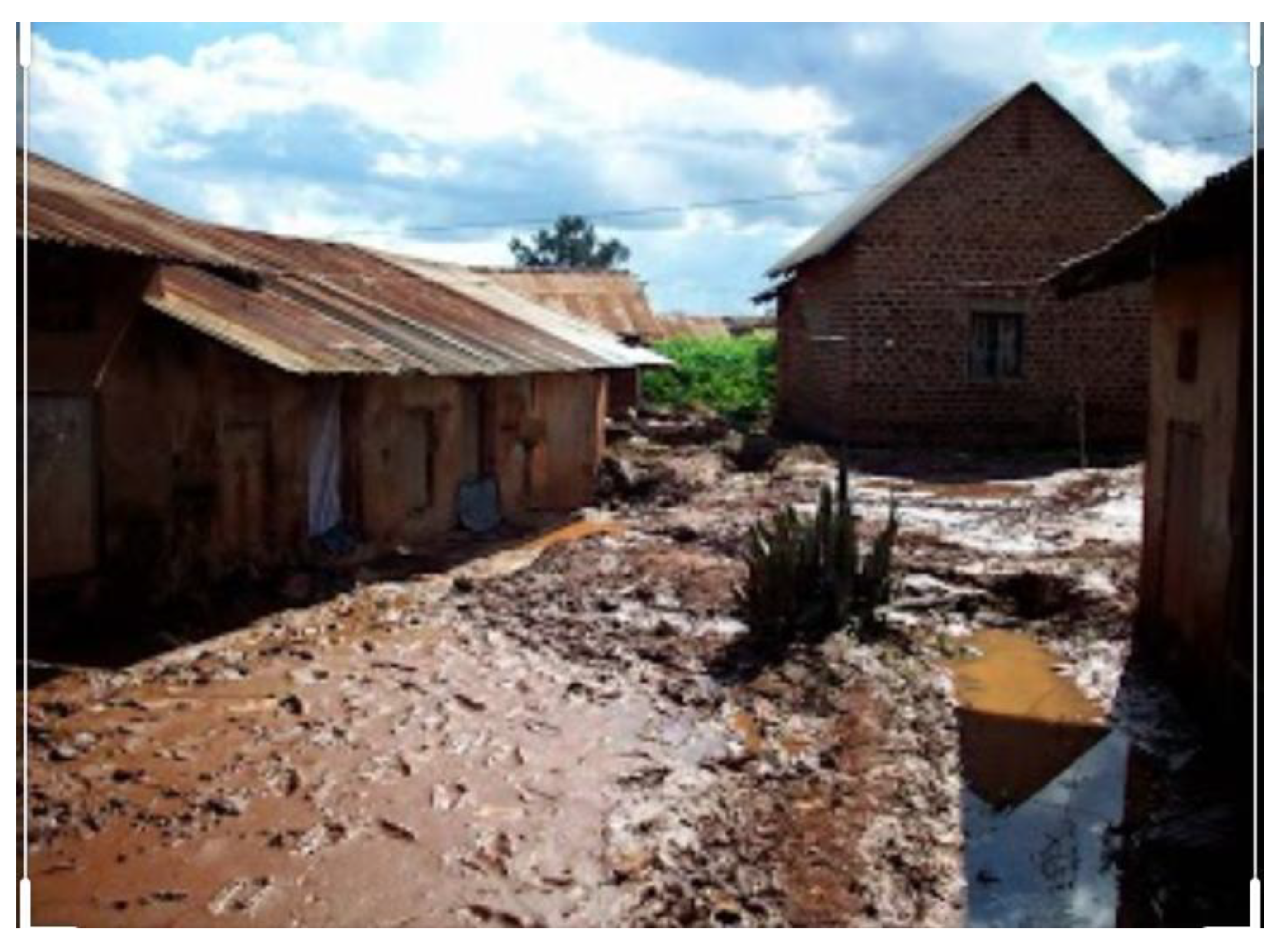
3.1.2. Poor Physical Infrastructure (Housing)
“If the responsible persons/owners of these house do not either remove or renovate them. These houses are a nuisance. In fact, at night, a person can hide there and attack you. There are a unforeseen danger”(Photographer 7, male, 27 years)
3.1.3. Undesirable Work Conditions
“This man was carrying building materials from a ground to first floor on that building site. He was carrying three heavy blocks every round, which were too much weight for him. He is likely to develop chest complications that could result in death”(Photographer 7, male, aged 27)
“This man had attacked a neighbor to rob them and they cut him with a panga. Immediately, a mob beat him to death. It is not a good thing for people to take justice into their hands, especially when the court has not participated”(Photographer 9, male, aged 27)
3.1.4. Poor Food Hygiene and Safety
3.1.5. Unsafe Sexual Practices and Environments
“While drinking “malwa”, many people use one pot with many straws and yet some people have poor drinking habits. They put back saliva into the pot, and these days, we have hepatitis B on the rise, which is transmitted through saliva and sweat. Yet, you can’t know how is infected or they can also get Tuberculosis (TB)”(Photographer 8, female, aged 30)
“This man was trying to save this child who had fallen into the drainage channel. If this man wasn’t fast enough, this child would have died due to the surface runoff just like the other child who was hit by the house”(Photographer 1, male, aged 28)
“This man was beaten because he was a thief. He had attacked a neighbor who had a panga and he cut him. Immediately there was mob justice and they beat him to death. It is not good for people to take justice into their hands yet there are courts of law”(Photographer 9, male, age 27)
“The youth drink alcohol during the day. This man was so dirty and his trouser had changed color from black to brown. He was drinking alcohol on his way back home and fell into a trench. He hit his mouth and lost his teeth but also suffered other injuries”(Photographer 6, male, age 22)
3.2. Ecological Ceiling Overshoot
3.2.1. Land Conversion
“This house was built in a swampy area where there is a lot of stagnant water. So, whether it rains or not, there is water. In case the people who reside in the house don’t use mosquito nets they will contact malaria given that the area has good breeding ground for the mosquitos”(Photographer 3, female, aged 22)
3.2.2. Environmental Pollution
“She uses firewood to cook cassava. She will inhale the smoke that comes from the firewood. These inhaled air pollutants can affect her lungs”(Photographer 1, male, aged 28)
“This spring is in the valley while settlements are above it. All the contaminated water flowing from the houses such as the bathroom wastewater ends up into the spring making the spring water unfit for human consumption”(Photographer 7, male, age 27)
“This is a storey building. The whole of the lower level are rentals, and the upper level is a church. Churches have overnights, which exposes the people on the lower floors to noise depriving them of sleep”(Photographer 10, female, age 22)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations Department of Economic and Social Affairs, Population Division. World Urbanisation Prospects; United Nations: New York, NY, USA, 2018.
- UBOS. National Population and Housing Census 2014 Provisional Results; Uganda Bureau of Statistics Kampala: Kampala, Uganda, 2014.
- Kjellstrom, T.; Friel, S.; Dixon, J.; Corvalan, C.; Rehfuess, E.; Campbell-Lendrum, D.; Gore, F.; Bartram, J. Urban Environmental Health Hazards and Health Equity. J. Urban Health Bull. N. Y. Acad. Med. 2007, 84, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Ssemugabo, C.; Mukama, T.; Halage, A.A.; Paichadze, N.; Gibson, D.G.; Kobusingye, O. Incidence and characteristics of unintentional injuries among children in a resource limited setting in Kampala, Uganda. Int. J. Inj. Control Saf. Promot. 2018, 25, 449–457. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Millenium Development Goals Indicators: The Official United Nations Site for MDGs Indicatprs. Available online: http://mdgs.un.org/unsd/mdg/Metadata.aspx?IndicatorId=32 (accessed on 20 December 2018).
- Isunju, J.B.; Christopher Garimoi, O.; Jaco, K. Hazards and vulnerabilities among informal wetland communities in Kampala, Uganda. Environ. Urban. 2015, 28, 275–293. [Google Scholar] [CrossRef]
- David, S.; Sheridan, B. Editorial: The full spectrum of risk in urban centres: Changing perceptions, changing priorities. Environ. Urban. 2017, 29, 3–14. [Google Scholar] [CrossRef]
- Myers, S.S. Land Use Change and Human Health. In Integrating Ecology and Poverty Reduction: Ecological Dimensions; Ingram, J.C., DeClerck, F., Rumbaitis del Rio, C., Eds.; Springer: New York, NY, USA, 2012; pp. 167–186. [Google Scholar]
- Legros, D.; McCormick, M.; Mugero, C.; Skinnider, M.; Bek’Obita, D.D.; Okware, S.I. Epidemiology of cholera outbreak in Kampala, Uganda. East Afr. Med. J. 2000, 77, 347–349. [Google Scholar] [CrossRef][Green Version]
- WHO. Typhoid fever—Uganda. In Global Alert Response—Disease Outbreak News; World Health Organisation: Geneva, Switzerland, 2015. [Google Scholar]
- Raworth, K. A Safe and Just Space for Humanity. Can We Live within the Doughnut? 2012. Available online: https://www.oxfam.org/en/research/safe-and-just-space-humanity (accessed on 20 December 2018).
- Hossain, M.S.; Ifejika Speranza, C. Challenges and opportunities for operationalizing the safe and just operating space concept at regional scale. Int. J. Sustain. Dev. World Ecol. 2020, 27, 40–54. [Google Scholar] [CrossRef]
- Ross, F. Kate Raworth-Doughnut Economics: Seven Ways to Think Like a 21st Century Economist (2017). Reg. Bus. Stud. 2019, 11, 81–86. [Google Scholar] [CrossRef]
- Schokkaert, E. Review of Kate Raworth’s Doughnut Economics. London: Random House, 2017, 373 pp. Erasmus J. Philos. Econ. 2019, 12, 125–132. [Google Scholar] [CrossRef]
- Castleden, H.; Garvin, T. Modifying Photovoice for community-based participatory Indigenous research. Soc. Sci. Med. 2008, 66, 1393–1405. [Google Scholar] [CrossRef]
- Wang, C.; Burris, M.A. Photovoice: Concept, methodology, and use for participatory needs assessment. Health Educ. Behav. Off. Publ. Soc. Public Health Educ. 1997, 24, 369–387. [Google Scholar] [CrossRef]
- Catalani, C.; Minkler, M. Photovoice: A review of the literature in health and public health. Health Educ. Behav. Off. Publ. Soc. Public Health Educ. 2010, 37, 424–451. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.C. Youth Participation in Photovoice as a Strategy for Community Change. J. Community Pract. 2006, 14, 147–161. [Google Scholar] [CrossRef]
- Musoke, D.; Ssemugabo, C.; Ndejjo, R.; Molyneux, S.; Ekirapa-Kiracho, E. Ethical practice in my work: Community health workers’ perspectives using photovoice in Wakiso district, Uganda. BMC Med. Ethics 2020, 21, 68. [Google Scholar] [CrossRef] [PubMed]
- Musoke, D.; Ssemugabo, C.; Ndejjo, R.; Ekirapa-Kiracho, E.; George, A.S. Reflecting strategic and conforming gendered experiences of community health workers using photovoice in rural Wakiso district, Uganda. Hum. Resour. Health 2018, 16, 41. [Google Scholar] [CrossRef]
- Musoke, D.; Ekirapa-Kiracho, E.; Ndejjo, R.; George, A. Using photovoice to examine community level barriers affecting maternal health in rural Wakiso district, Uganda. Reprod. Health Matters 2015, 23, 136–147. [Google Scholar] [CrossRef]
- African Union Commission. African Youth Charter; African Union Commission: Addis Ababa, Ethiopia, 2009. [Google Scholar]
- Necheles, J.W.; Chung, E.Q.; Hawes-Dawson, J.; Ryan, G.W.; Williams, S.B.; Holmes, H.N.; Wells, K.B.; Vaiana, M.E.; Schuster, M.A. The Teen Photovoice Project: A pilot study to promote health through advocacy. Prog. Community Health Partnersh. Res. Educ. Action 2007, 1, 221–229. [Google Scholar] [CrossRef]
- Kovacic, M.B.; Stigler, S.; Smith, A.; Kidd, A.; Vaughn, L.M. Beginning a partnership with PhotoVoice to explore environmental health and health inequities in minority communities. Int. J. Environ. Res. Public Health 2014, 11, 11132–11151. [Google Scholar] [CrossRef]
- Kwiringira, J.; Atekyereza, P.; Niwagaba, C.; Günther, I. Descending the sanitation ladder in urban Uganda: Evidence from Kampala Slums. BMC Public Health 2014, 14, 624. [Google Scholar] [CrossRef]
- Ssemugabo, C.; Wafula, S.T.; Ndejjo, R.; Osuret, J.; Musoke, D.; Halage, A.A. Characteristics of sanitation and hygiene facilities in a slum community in Kampala, Uganda. Int. Health 2020. [Google Scholar] [CrossRef]
- Adhiambo, M.; Nyamari, J.; Imungi, J.I. Food Hygiene Conditions and Microbial Contamination of Minimally Processed Fruits in Central Ward, Nairobi County. Int. J. Sci. Res. Publ. 2017, 7, 137. [Google Scholar]
- Wandolo, M.A. Food safety and hygiene practices in the informal outlets (a case study of food kiosks in Kibera slums, Nairobi). In Public Health; Kenyatta University: Nairobi, Kenya, 2011. [Google Scholar]
- Mahabir, R.; Crooks, A.; Croitoru, A.; Agouris, P. The study of slums as social and physical constructs: Challenges and emerging research opportunities. Reg. Stud. Reg. Sci. 2016, 3, 399–419. [Google Scholar] [CrossRef]
- Unger, A.; Riley, L.W. Slum health: From understanding to action. PLoS Med. 2007, 4, e295. [Google Scholar] [CrossRef] [PubMed]
- UBOS. Statistical Abstract 2018; Uganda Bureau of Statistics Kampala: Kampala, Uganda, 2018.
- Zerbo, A.; Delgado, R.C.; González, P.A. Vulnerability and everyday health risks of urban informal settlements in Sub-Saharan Africa. Glob. Health J. 2020, 4, 46–50. [Google Scholar] [CrossRef]
- Elsey, H.; Manandah, S.; Sah, D.; Khanal, S.; MacGuire, F.; King, R.; Wallace, H.; Baral, S.C. Public Health Risks in Urban Slums: Findings of the Qualitative ‘Healthy Kitchens Healthy Cities’ Study in Kathmandu, Nepal. PLoS ONE 2016, 11, e0163798. [Google Scholar] [CrossRef] [PubMed]
- Corburn, J.; Vlahov, D.; Mberu, B.; Riley, L.; Caiaffa, W.T.; Rashid, S.F.; Ko, A.; Patel, S.; Jukur, S.; Martínez-Herrera, E.; et al. Slum Health: Arresting COVID-19 and Improving Well-Being in Urban Informal Settlements. J. Urban Health 2020, 97, 348–357. [Google Scholar] [CrossRef] [PubMed]
- Bird, J.; Montebruno, P.; Regan, T. Life in a slum: Understanding living conditions in Nairobi’s slums across time and space. Oxf. Rev. Econ. Policy 2017, 33, 496–520. [Google Scholar] [CrossRef]
- Singleton, G.; Rola-Rubzen, M.F.; Muir, K.; Muir, D.; McGregor, M. Youth empowerment and information and communication technologies: A case study of a remote Australian Aboriginal community. GeoJournal 2009, 74, 403. [Google Scholar] [CrossRef]
- Lofton, S.; Norr, K.F.; Jere, D.; Patil, C.; Banda, C. Developing Action Plans in Youth Photovoice to Address Community-Level HIV Risk in Rural Malawi. Int. J. Qual. Methods 2020, 19, 1609406920920139. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant Number | Zone | Age | Gender | Education Level | Occupation | Marital Status |
|---|---|---|---|---|---|---|
| 1 | Kawaala I | 28 | Male | Tertiary (University) | Accountant | Single |
| 2 | Kasubi II | 18 | Female | Secondary (advanced level) | Student | Single |
| 3 | Kawaala I | 22 | Female | Tertiary (Diploma) | Student | Single |
| 4 | Kasubi I | 23 | Female | Secondary (advanced level) | Unemployed | Single |
| 5 | Kasubi II | 29 | Male | Tertiary (University) | Business | Engaged |
| 6 | Kasubi II | 22 | Male | Secondary (advanced level) | Business | Single |
| 7 | Kasubi I | 27 | Male | Tertiary (University) | Electrician | Single |
| 8 | Kasubi I | 30 | Female | Secondary (advanced level) | Unemployed | Single |
| 9 | Kasubi II | 27 | Male | Secondary (advanced level) | Business | Single |
| 10 | Kasubi IV | 35 | Female | Secondary (ordinary level) | Business | Single |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ssemugabo, C.; Nalinya, S.; Lubega, G.B.; Ndejjo, R.; Musoke, D. Health Risks in Our Environment: Urban Slum Youth’ Perspectives Using Photovoice in Kampala, Uganda. Sustainability 2021, 13, 248. https://doi.org/10.3390/su13010248
Ssemugabo C, Nalinya S, Lubega GB, Ndejjo R, Musoke D. Health Risks in Our Environment: Urban Slum Youth’ Perspectives Using Photovoice in Kampala, Uganda. Sustainability. 2021; 13(1):248. https://doi.org/10.3390/su13010248
Chicago/Turabian StyleSsemugabo, Charles, Sarah Nalinya, Grace Biyinzika Lubega, Rawlance Ndejjo, and David Musoke. 2021. "Health Risks in Our Environment: Urban Slum Youth’ Perspectives Using Photovoice in Kampala, Uganda" Sustainability 13, no. 1: 248. https://doi.org/10.3390/su13010248
APA StyleSsemugabo, C., Nalinya, S., Lubega, G. B., Ndejjo, R., & Musoke, D. (2021). Health Risks in Our Environment: Urban Slum Youth’ Perspectives Using Photovoice in Kampala, Uganda. Sustainability, 13(1), 248. https://doi.org/10.3390/su13010248