Salmon Intake Intervention in the Vulnerable Group of Young Polish Women to Maintain Vitamin D Status during the Autumn Season



Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Statement
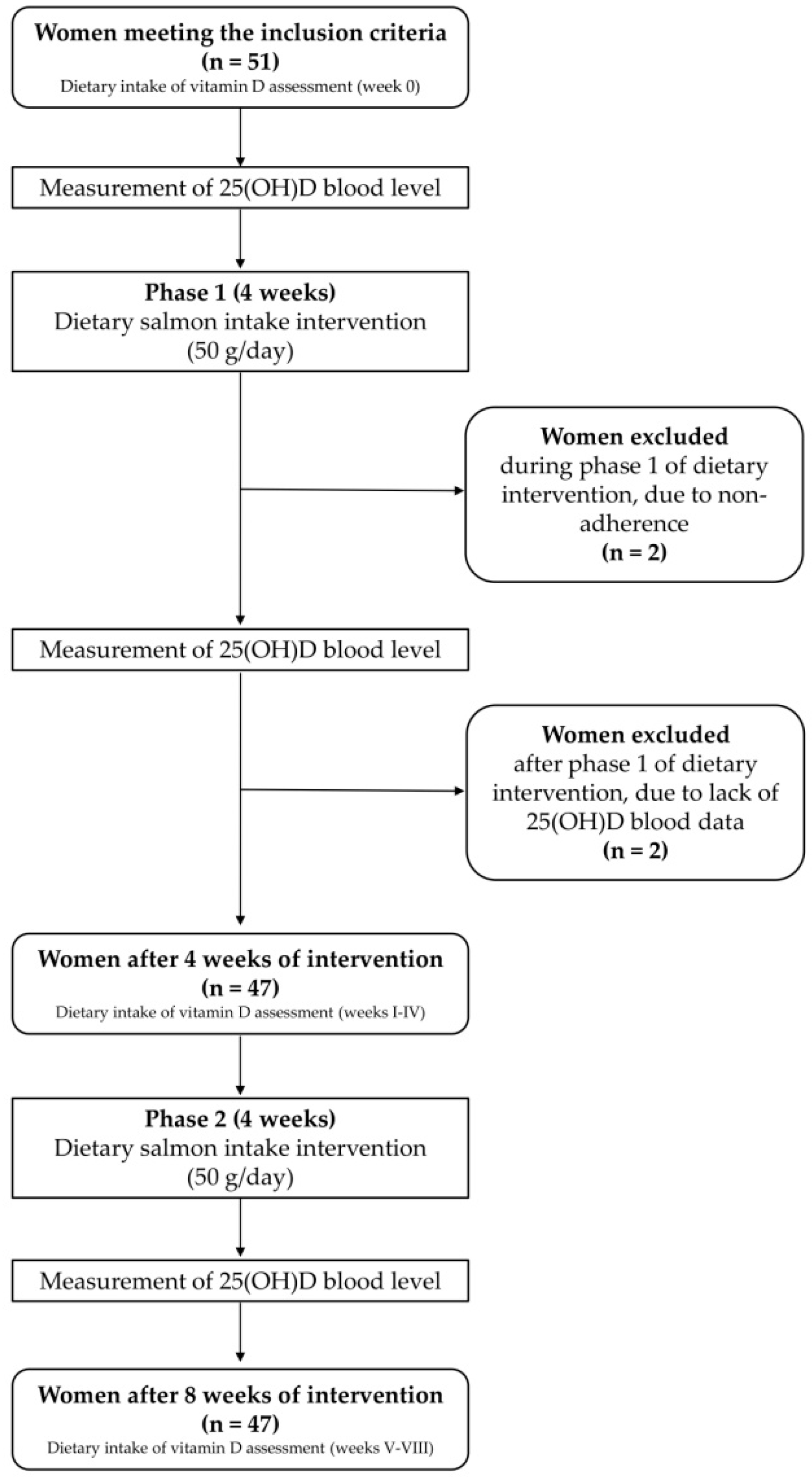
2.2. Studied Group
- −
- females,
- −
- Caucasian,
- −
- aged 20–30 years,
- −
- living in Warsaw or its surroundings (necessary to visit Dietetic Outpatient Clinic of the Department of Dietetics, Warsaw University of Life Sciences (WULS-SGGW) once a week for 8 weeks of the study duration),
- −
- providing written informed consent to participate in the study.
- −
- pregnancy,
- −
- lactation,
- −
- obesity, defined based on the criteria of the World Health Organization [30] as body mass index (BMI) ≥ 30 kg/m2,
- −
- fish and/or seafood allergy,
- −
- following any diet with fish consumption restriction (e.g., vegetarian diet),
- −
- vitamin D supplementation use up to 3 weeks before beginning of study and/or planned during study time,
- −
- diseases and/or use of medicines changing vitamin D metabolism,
- −
- planned travels to countries below the 40th parallel (countries with adequate sun exposure to obtain cutaneous vitamin D synthesis during study time),
- −
- planned solarium use during study time.
2.3. Dietary Intervention
2.4. Measurements
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lips, P.; van Schoor, N.M. The effect of vitamin D on bone and osteoporosis. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 585–591. [Google Scholar] [PubMed]
- Gao, Q.; Kou, T.; Zhuang, B.; Ren, Y.; Dong, X.; Wang, Q. The Association between Vitamin D Deficiency and Sleep Disorders: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 1395. [Google Scholar]
- Wang, J.; Lv, S.; Chen, G.; Gao, C.; He, J.; Zhong, H.; Xu, Y. Meta-analysis of the association between vitamin D and autoimmune thyroid disease. Nutrients 2015, 7, 2485–2498. [Google Scholar] [PubMed]
- Estébanez, N.; Gómez-Acebo, I.; Palazuelos, C.; Llorca, J.; Dierssen-Sotos, T. Vitamin D exposure and Risk of Breast Cancer: A meta-analysis. Sci. Rep. 2018, 8, 9039. [Google Scholar]
- Keum, N.; Lee, D.H.; Greenwood, D.C.; Manson, J.E.; Giovannucci, E. Vitamin D supplementation and total cancer incidence and mortality: A meta-analysis of randomized controlled trials. Ann. Oncol. 2019, 30, 733–743. [Google Scholar]
- Wang, M.; Liu, M.; Wang, C.; Xiao, Y.; An, T.; Zou, M.; Cheng, G. Association between vitamin D status and asthma control: A meta-analysis of randomized trials. Respir. Med. 2019, 150, 85–94. [Google Scholar]
- Christakos, S.; Dhawan, P.; Verstuyf, A.; Verlinden, L.; Carmeliet, G. Vitamin D: Metabolism, Molecular Mechanism of Action, and Pleiotropic Effects. Physiol. Rev. 2016, 96, 365–408. [Google Scholar]
- Caprio, M.; Infante, M.; Calanchini, M.; Mammi, C.; Fabbri, A. Vitamin D: Not just the bone. Evidence for beneficial pleiotropic extraskeletal effects. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2017, 22, 27–41. [Google Scholar] [CrossRef]
- Durazo-Arvizu, R.A.; Tian, L.; Brooks, S.P.J.; Sarafin, K.; Cashman, K.D.; Kiely, M.; Merkel, J.; Myers, G.L.; Coates, P.M.; Sempos, C.T. The Vitamin D Standardization Program (VDSP) Manual for Retrospective Laboratory Standardization of Serum 25-Hydroxyvitamin D Data. J. AOAC Int. 2017, 100, 1234–1243. [Google Scholar] [CrossRef]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef]
- National Academies Press (US). Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. In Dietary Reference Intakes for Calcium and Vitamin D; Ross, A.C., Taylor, C.L., Yaktine, A.L., Del Valle, H.B., Eds.; The National Academies Collection: Reports funded by National Institutes of Health; National Academies Press (US): Washington, DC, USA, 2011. [Google Scholar]
- Aspray, T.J.; Bowring, C.; Fraser, W.; Gittoes, N.; Javaid, M.K.; Macdonald, H.; Patl, S.; Selby, P.; Tanna, N.; Francis, R.M. National Osteoporosis Society Vitamin D Guideline Summary. Age Ageing 2014, 43, 592–595. [Google Scholar] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar]
- EFSA Panel on Dietetic Products. N. and A. (NDA) Dietary reference values for vitamin D. EFSA J. 2016, 14, e04547. [Google Scholar] [CrossRef]
- Rusińska, A.; Płudowski, P.; Walczak, M.; Borszewska-Kornacka, M.K.; Bossowski, A.; Chlebna-Sokół, D.; Czech-Kowalska, J.; Dobrzańska, A.; Franek, E.; Helwich, E.; et al. Vitamin D Supplementation Guidelines for General Population and Groups at Risk of Vitamin D Deficiency in Poland-Recommendations of the Polish Society of Pediatric Endocrinology and Diabetes and the Expert Panel with Participation of National Specialist Consultants and Representatives of Scientific Societies-2018 Update. Front. Endocrinol. 2018, 9, 246. [Google Scholar]
- Gordon, C.M.; DePeter, K.C.; Feldman, H.A.; Grace, E.; Emans, S.J. Prevalence of Vitamin D Deficiency among Healthy Adolescents. Arch. Pediatr. Adolesc. Med. 2004, 158, 531–537. [Google Scholar]
- Andersen, R.; Mølgaard, C.; Skovgaard, L.T.; Brot, C.; Cashman, K.D.; Chabros, E.; Charzewska, J.; Flynn, A.; Jakobsen, J.; Kärkkäinen, M.; et al. Teenage girls and elderly women living in northern Europe have low winter vitamin D status. Eur. J. Clin. Nutr. 2005, 59, 533–541. [Google Scholar]
- ENNS: Étude Nationale Nutrition Santé /Enquêtes et Etudes /Nutrition et Santé /Maladies Chroniques et Traumatismes /Dossiers Thématiques /Accueil. Available online: http://invs.santepubliquefrance.fr/Dossiers-thematiques/Maladies-chroniques-et-traumatismes/Nutrition-et-sante/Enquetes-et-etudes/ENNS-etude-nationale-nutrition-sante (accessed on 25 June 2019).
- Calvo, M.S.; Whiting, S.J.; Barton, C.N. Vitamin D Intake: A Global Perspective of Current Status. J. Nutr. 2005, 135, 310–316. [Google Scholar]
- Webb, A.R.; Kline, L.; Holick, M.F. Influence of season and latitude on the cutaneous synthesis of vitamin D3: Exposure to winter sunlight in Boston and Edmonton will not promote vitamin D3 synthesis in human skin. J. Clin. Endocrinol. Metab. 1988, 67, 373–378. [Google Scholar]
- Schmid, A.; Walther, B. Natural Vitamin D Content in Animal Products. Adv. Nutr. 2013, 4, 453–462. [Google Scholar] [PubMed]
- Kunachowicz, H.; Przygoda, B.; Nadolna, I.; Iwanow, K. Tabele Składu i Wartości Odżywczej Żywności; Wydawnictwo Lekarskie PZWL: Warsaw, Poland, 2017. [Google Scholar]
- National Food Institute. European Nutrition and Health Report 2009; Elmadfa, I., Ed.; Karger: Basel, Switzerland; New York, NY, USA, 2009. [Google Scholar]
- Flynn, A.; Hirvonen, T.; Mensink, G.B. Intake of selected nutrients from foods, from fortification and from supplements in various European countries. Food Nutr. Res. 2009, 12, 2038. [Google Scholar]
- Nordiska Ministerrådet. Nordic Nutrition Recommendations 2012. Part 3: Vitamins A, D, E, K, Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Biotin, Pantothenic acid and Vitamin C; Nordisk Ministerråd: Copenhagen, Denmark, 2014. [Google Scholar]
- SACN Vitamin D and Health Report. Available online: https://www.gov.uk/government/publications/sacn-vitamin-d-and-health-report (accessed on 20 May 2019).
- Bailey, R.L.; Dodd, K.W.; Goldman, J.A.; Gahche, J.J.; Dwyer, J.T.; Moshfegh, A.J.; Sempos, C.T.; Picciano, M.F. Estimation of Total Usual Calcium and Vitamin D Intakes in the United States. J. Nutr. 2010, 140, 817–822. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, R.M. Bone health: Preventing osteoporosis. J. Am. Diet. Assoc. 2010, 110, 498. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lehmann, U.; Gjessing, H.R.; Hirche, F.; Mueller-Belecke, A.; Gudbrandsen, O.A.; Ueland, P.M.; Mellgren, G.; Lauritzen, L.; Lindqvist, H.; Hansen, A.L.; et al. Efficacy of fish intake on vitamin D status: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2015, 102, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Body Mass Index—BMI. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 24 July 2019).
- United States Department of Agriculture, Agricultural Research Service. Available online: https://fdc.nal.usda.gov/fdc-app.html#/food-details/337771/nutrients (accessed on 24 March 2020).
- Fish and Seafood Market in Poland. 2018. Available online: https://gain.fas.usda.gov/Recent%20GAIN%20Publications/2017%20Fish%20and%20Seafood%20Market%20in%20Poland_Warsaw_Poland_2-21-2018.pdf (accessed on 19 August 2019).
- FAO/WHO. Report of the Joint FAO/WHO Expert Consultation on the Risks and Benefits of Fish Consumption: Rome, 25–29 January 2010; FAO: Rome, Italy, 2011. [Google Scholar]
- Jakobsen, J.; Smith, C.; Bysted, A.; Cashman, K.D. Vitamin D in Wild and Farmed Atlantic Salmon (Salmo Salar)—What Do We Know? Nutrients 2019, 11, 982. [Google Scholar] [CrossRef] [PubMed]
- International Society for Advancement of Kinanthropometry. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Potchefstroom, South Africa, 2001. [Google Scholar]
- Reference Values DACH-Referenzwerte. Available online: http://www.sge-ssn.ch/grundlagen/lebensmittel-und-naehrstoffe/naehrstoffempfehlungen/dachreferenzwerte/ (accessed on 2 August 2019).
- Jarosz, M.; Rychlik, E.; Stoś, K.; Wierzejska, R.; Wojtasik, A.; Charzewska, J.; Mojska, H.; Szponar, L.; Sajór, I.; Kłosiewicz-Latoszek, L.; et al. Normy Żywienia dla Populacji Polski; Instytut Żywności i Żywienia: Warszawa, Poland, 2017. [Google Scholar]
- Głąbska, D.; Guzek, D.; Sidor, P.; Włodarek, D. Vitamin D Dietary Intake Questionnaire Validation Conducted among Young Polish Women. Nutrients 2016, 8, 36. [Google Scholar] [CrossRef]
- Ogedegbe, G.; Pickering, T. Principles and techniques of blood pressure measurement. Cardiol. Clin. 2010, 28, 571–586. [Google Scholar] [CrossRef]
- Lucey, A.J.; Paschos, G.K.; Cashman, K.D.; Martínéz, J.A.; Thorsdottir, I.; Kiely, M. Influence of moderate energy restriction and seafood consumption on bone turnover in overweight young adults. Am. J. Clin. Nutr. 2008, 87, 1045–1052. [Google Scholar] [CrossRef][Green Version]
- Erkkilä, A.T.; Schwab, U.S.; de Mello, V.D.F.; Lappalainen, T.; Mussalo, H.; Lehto, S.; Kemi, V.; Lamberg-Allardt, C.; Uusitupa, M.I.J. Effects of fatty and lean fish intake on blood pressure in subjects with coronary heart disease using multiple medications. Eur. J. Nutr. 2008, 47, 319–328. [Google Scholar] [CrossRef]
- Bratlie, M.; Hagen, I.V.; Helland, A.; Midttun, Ø.; Ulvik, A.; Rosenlund, G.; Sveier, H.; Mellgren, G.; Ueland, P.M.; Gudbrandsen, O.A. Five salmon dinners per week was not sufficient to prevent the reduction in serum vitamin D in autumn at 60° north latitude: A randomised trial. Br. J. Nutr. 2019, 123, 1–21. [Google Scholar] [CrossRef]
- Smyczyńska, J.; Smyczyńska, U.; Stawerska, R.; Domagalska-Nalewajek, H.; Lewiński, A.; Hilczer, M. Seasonality of vitamin D concentrations and the incidence of vitamin D deficiency in children and adolescents from central Poland. Pediatr. Endocrinol. Diabetes Metab. 2019, 25, 54–59. [Google Scholar] [CrossRef]
- Diffey, B.L. Modelling vitamin D status due to oral intake and sun exposure in an adult British population. Br. J. Nutr. 2013, 110, 569–577. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, H.M.; Mavroeidi, A.; Barr, R.J.; Black, A.J.; Fraser, W.D.; Reid, D.M. Vitamin D status in postmenopausal women living at higher latitudes in the UK in relation to bone health, overweight, sunlight exposure and dietary vitamin D. Bone 2008, 42, 996–1003. [Google Scholar] [CrossRef] [PubMed]
- Dale, M.M.; Haylett, D.G. Rang and Dale’s Pharmacology Flashcards; Churchill Livingstone Elsevier: London, UK, 2014. [Google Scholar]
- Kumar, R. The metabolism and mechanism of action of 1,25-dihydroxyvitamin D3. Kidney Int. 1986, 30, 793–803. [Google Scholar] [CrossRef]
- Rynek Ryb [Fish Market]. Available online: https://www.ierigz.waw.pl/publikacje/analizy-rynkowe/rynek-ryb/20873,3,3,0,nr-26-2017-rynek-ryb.html (accessed on 16 August 2019).
- Scheers, N.; Lindqvist, H.; Langkilde, A.M.; Undeland, I.; Sandberg, A.-S. Vitamin B12 as a potential compliance marker for fish intake. Eur. J. Nutr. 2014, 53, 1327–1333. [Google Scholar] [CrossRef] [PubMed]
- Fish and Omega-3 Fatty Acids. Available online: https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/fats/fish-and-omega-3-fatty-acids (accessed on 19 August 2019).
- Piramida Zdrowego Żywienia i Aktywności Fizycznej [Food and Physical Activity Pyramid]. Available online: http://www.izz.waw.pl/attachments/article/7/Piramida%20Zdrowego%20%C5%BBywienia%20i%20Aktywno%C5%9Bci%20Fizycznej%20Broszura.pdf (accessed on 19 August 2019).
- Becker, W.; Pearson, M.; Metod Och Resultatanalys. Livsmedelsverket, Uppsala, Sverige, Riksmaten 1997–1998. Available online: https://www.livsmedelsverket.se/globalassets/matvanor-halsa-miljo/kostrad-matvanor/matvaneundersokningar/riksmaten-1997-1998-resultat-och-metodrapport.pdf (accessed on 19 August 2019).
- Pietinen, P.; Paturi, M.; Reinivuo, H.; Tapanainen, H.; Valsta, L.M. FINDIET 2007 Survey: Energy and nutrient intakes. Public Health Nutr. 2010, 13, 920–924. [Google Scholar] [CrossRef] [PubMed]
- Van der Meer, I.M.; Boeke, A.J.P.; Lips, P.; Grootjans-Geerts, I.; Wuister, J.D.; Devillé, W.L.J.M.; Wielders, J.P.M.; Bouter, L.M.; Middelkoop, B.J.C. Fatty fish and supplements are the greatest modifiable contributors to the serum 25-hydroxyvitamin D concentration in a multiethnic population. Clin. Endocrinol. Oxf. 2008, 68, 466–472. [Google Scholar] [CrossRef]
- Petrenya, N.; Lamberg-Allardt, C.; Melhus, M.; Broderstad, A.R.; Brustad, M. Vitamin D status in a multi-ethnic population of northern Norway: The SAMINOR 2 Clinical Survey. Public Health Nutr. 2019, 1–15. [Google Scholar] [CrossRef]
- Hansen, A.L.; Dahl, L.; Bakke, L.; Frøyland, L.; Thayer, J.F. Fish consumption and heart rate variability: Preliminary results. J. Psychophysiol. 2010, 24, 41–47. [Google Scholar] [CrossRef]
- Hansen, A.L.; Dahl, L.; Olson, G.; Thornton, D.; Graff, I.E.; Frøyland, L.; Thayer, J.F.; Pallesen, S. Fish Consumption, Sleep, Daily Functioning, and Heart Rate Variability. J. Clin. Sleep Med. 2014, 10, 567–575. [Google Scholar] [CrossRef]
- Vuholm, S.; Teisen, M.N.; Buch, N.G.; Stark, K.D.; Jakobsen, J.; Mølgaard, C.; Lauritzen, L.; Damsgaard, C.T. Is high oily fish intake achievable and how does it affect nutrient status in 8-9-year-old children? The FiSK Junior trial. Eur. J. Nutr. 2019, 59, 1205–1218. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Mean ± SD | Median (Min–Max) | |
|---|---|---|---|
| Characteristics | Age (years) | 22.9 ± 1.6 | 23.0 * (20.0–28.0) |
| BMI (kg/m2) | 21.43 ± 2.49 | 21.27 (16.92–27.96) | |
| Serum level | 25(OH)D for t0 (nmol/L) | 58.4 ± 20.2 | 57.1 (19.7–93.1) |
| 25(OH)D for t4 (nmol/L) | 41.2 ± 14.1 | 39.9 * (15.1–90.3) | |
| 25(OH)D for t8 (nmol/L) | 52.5 ± 11.4 | 54.1 (25.6–72.9) | |
| Change of serum level | 25(OH)D change from t0 to t4 (nmol/L) | −17.2 ± 13.9 | −16.7 (−44.5–11.4) |
| 25(OH)D change from t4 to t8 (nmol/L) | 11.3 ± 12.2 | 8,8 * (−18.5–38.8) | |
| 25(OH)D change from t0 to t8 (nmol/L) | −6.0 ± 16.1 | −8.1 (−36.8–24.2) | |
| Variables | Mean ± SD | Median (Min–Max) | p | |
|---|---|---|---|---|
| Intake for t0 (µg) | Total | 3.02 ± 1.36 | 2.79 * (1.04–7.74) | - |
| 25(OH)D < 50 nmol/L | 3.02 ± 1.63 | 2.66 * (1.04–7.74) | 0.7510 | |
| 25(OH)D ≥ 50 nmol/L | 3.02 ± 1.20 | 2.90 * (1.09–5.99) | ||
| Intake for t4 (µg) | Total | 10.08 ± 1.34 | 9.82 * (7.84–13.91) | - |
| 25(OH)D < 50 nmol/L | 9.88 ± 1.26 | 9.73 * (7.84–13.15) | 0.0515 | |
| 25(OH)D ≥ 50 nmol/L | 10.73 ± 1.46 | 10.65 * (8.62–13.91) | ||
| Intake for t8 (µg) | Total | 9.85 ± 1.96 | 9.71 * (1.81–13.82) | - |
| 25(OH)D < 50 nmol/L | 9.44 ± 2.43 | 9.59 * (1.81–13.82) | 0.3411 | |
| 25(OH)D ≥ 50 nmol/L | 10.11 ± 1.60 | 9.89 * (6.77–12.78) | ||
| Serum 25-hydroxyvitamin D level | |||
|---|---|---|---|
| Inadequate (<50 nmol/L) * | Adequate (50–250 nmol/L) * | Potentially Toxic (> 250 nmol/L) * | |
| Before intervention | 18 (38%) | 29 (62%) | 0 (0%) |
| After 4 weeks of intervention | 36 (77%) | 11 (23%) | 0 (0%) |
| After 8 weeks of intervention | 18 (38%) | 29 (62%) | 0 (0%) |
| Variables | Age | BMI | |||
|---|---|---|---|---|---|
| p | R | p | R | ||
| Serum level | 25(OH)D for t0 (nmol/L) | 0.0880 | −0.2512 | 0.0419 * | −0.2980 |
| 25(OH)D for t4 (nmol/L) | 0.5753 * | −0.0838 | 0.0663 * | −0.2701 | |
| 25(OH)D for t8 (nmol/L) | 0.2300 | −0.1786 | 0.4038 * | −0.1247 | |
| Change of serum level | 25(OH)D change from t0 to t4 (nmol/L) | 0.4630 | 0.1096 | 0.3604 * | 0.1364 |
| 25(OH)D change from t4 to t8 (nmol/L) | 0.4387 * | 0.1157 | 0.4776 * | 0.1062 | |
| 25(OH)D change from t0 to t8 (nmol/L) | 0.2010 | −0.1897 | 0.1362 * | 0.2206 | |
| Variables | p | R | |
|---|---|---|---|
| Serum level | 25(OH)D for t4 (nmol/L) | < 0.0001 * | 0.7474 |
| 25(OH)D for t8 (nmol/L) | < 0.0001 | 0.6089 | |
| Change of serum level | 25(OH)D change from t0 to t4 (nmol/L) | < 0.0001 | −0.7154 |
| 25(OH)D change from t4 to t8 (nmol/L) | 0.1257 * | −0.2265 | |
| 25(OH)D change from t0 to t8 (nmol/L) | < 0.0001 | −0.8274 | |
| Variables | Inadequate 25(OH)D (< 50 nmol/L) | Adequate 25(OH)D (≥ 50 nmol/L) | ||||
|---|---|---|---|---|---|---|
| Mean ± SD | Median (Min–Max) | Mean ± SD | Median (Min–Max) | p ** | ||
| Serum level | 25(OH)D for t0 (nmol/L) | 37.5 ± 10.1 | 36.4 (19.7–48.9) | 71.4 ± 12.4 | 70.4 (53.2–93.1) | <0.0001 |
| 25(OH)D for t4 (nmol/L) | 31.2 ± 8.8 | 29.2 (15.1–51.7) | 47.4 ± 13.3 | 45.4 (28.5–90.3) * | <0.0001 | |
| 25(OH)D for t8 (nmol/L) | 47.1 ± 12.7 | 46.8 (25.6–72.9) * | 55.8 ± 9.2 | 56.8 (39.8–72.1) | 0.0198 | |
| Change of serum level | 25(OH)D change from t0 to t4 (nmol/L) | −5.0 ± 13.0 | −8.5 (−21.2–32.9) | −17.4 ± 24.0 | −16.4 (−53.7–41.3) | 0.0501 |
| 25(OH)D change from t4 to t8 (nmol/L) | 15.9 ± 12.6 | 15.1 (−0.3–37.0) | 8.4 ± 11.2 | 7.1 (−18.5–38.8) | 0.0381 | |
| 25(OH)D change from t0 to t8 (nmol/L) | 10.9 ± 16.0 | 8.2 (−10.3–52.0) | −9.0 ± 23.9 | −6.7 (−52.0–53.0) * | 0.0005 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Utri, Z.; Głąbska, D. Salmon Intake Intervention in the Vulnerable Group of Young Polish Women to Maintain Vitamin D Status during the Autumn Season. Sustainability 2020, 12, 2829. https://doi.org/10.3390/su12072829
Utri Z, Głąbska D. Salmon Intake Intervention in the Vulnerable Group of Young Polish Women to Maintain Vitamin D Status during the Autumn Season. Sustainability. 2020; 12(7):2829. https://doi.org/10.3390/su12072829
Chicago/Turabian StyleUtri, Zofia, and Dominika Głąbska. 2020. "Salmon Intake Intervention in the Vulnerable Group of Young Polish Women to Maintain Vitamin D Status during the Autumn Season" Sustainability 12, no. 7: 2829. https://doi.org/10.3390/su12072829
APA StyleUtri, Z., & Głąbska, D. (2020). Salmon Intake Intervention in the Vulnerable Group of Young Polish Women to Maintain Vitamin D Status during the Autumn Season. Sustainability, 12(7), 2829. https://doi.org/10.3390/su12072829