Adding the Mureş River Basin (Transylvania, Romania) to the List of Hotspots with High Contamination with Pharmaceuticals

 , ,
, ,  ,
,  ,
,
Abstract
1. Background
1.1. Pollution Sources and Environmental Hazards of Studied Pharmaceutical Compounds
1.2. Aim
2. Material and Methods
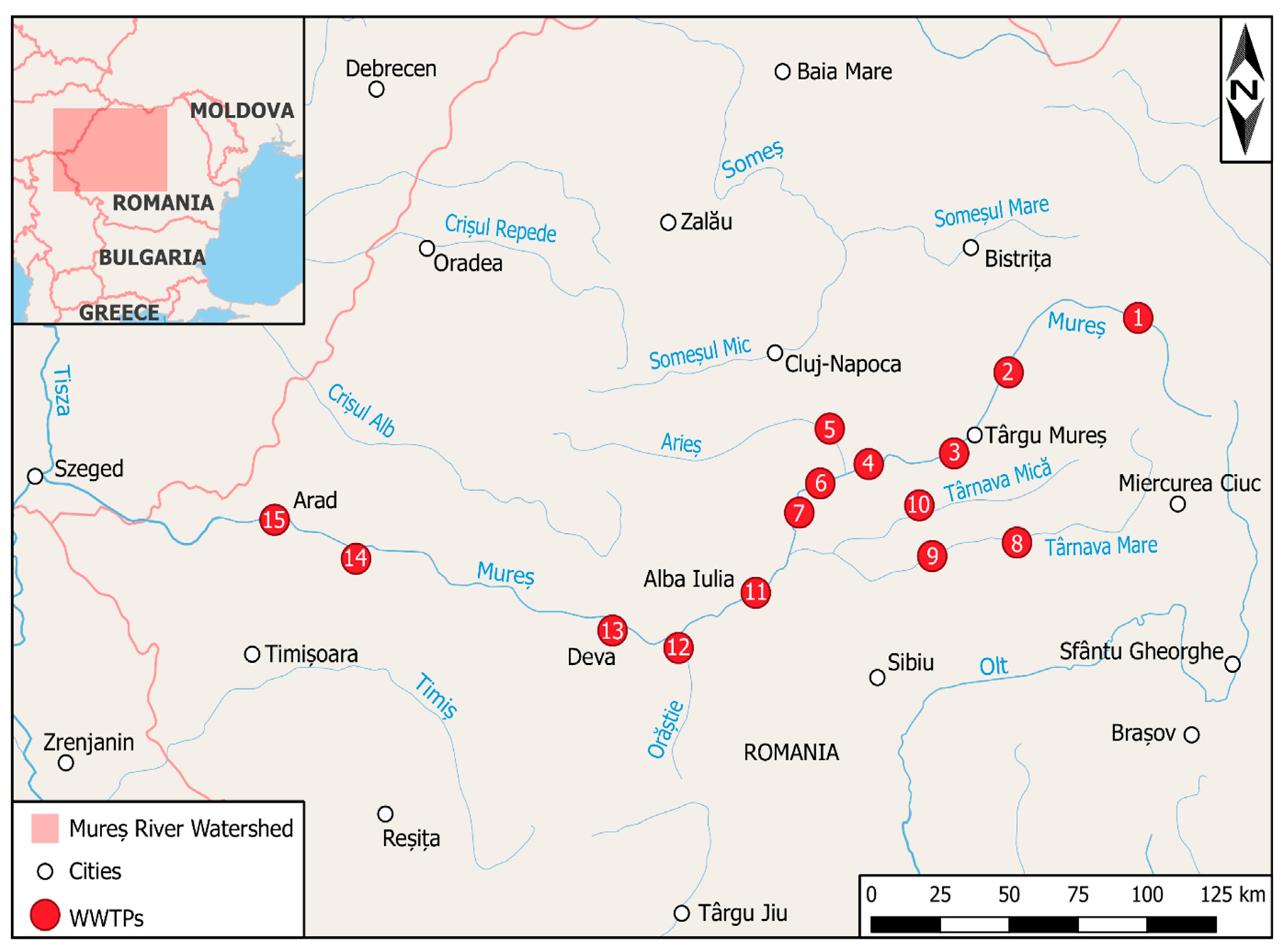
2.1. Sampling
2.2. Reagents
2.3. Sample Extraction
2.4. Liquid Chromatography
2.5. Triple Quadrupole Mass Spectrometry
2.6. Data Analysis
2.7. Method Validation
3. Results
3.1. Concentrations
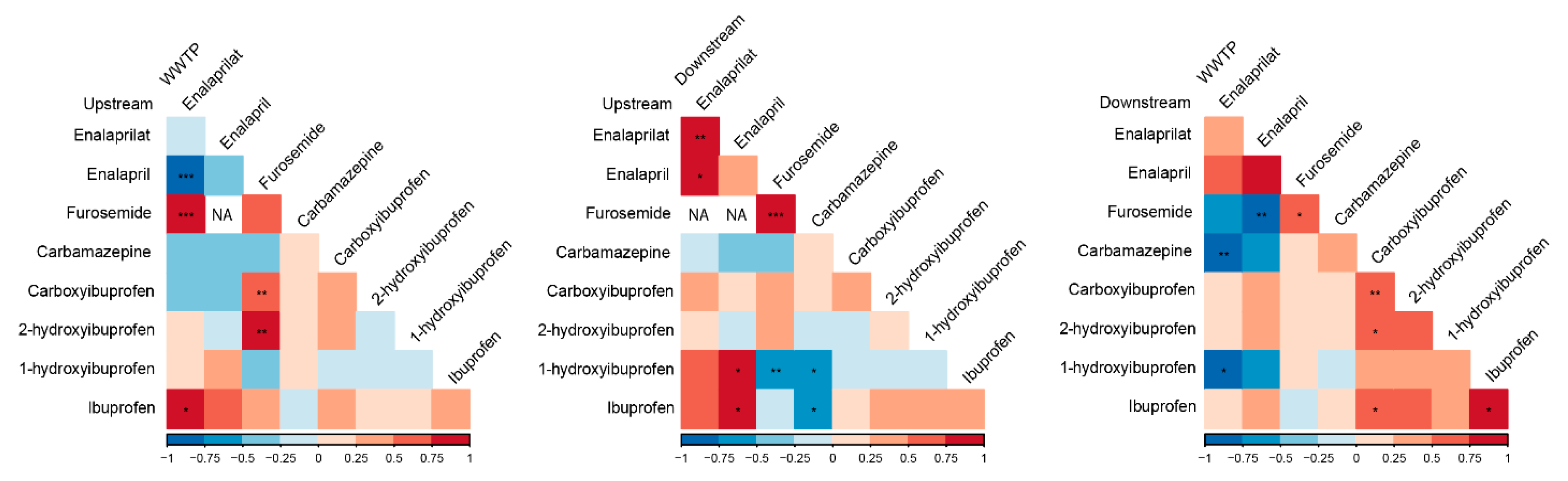
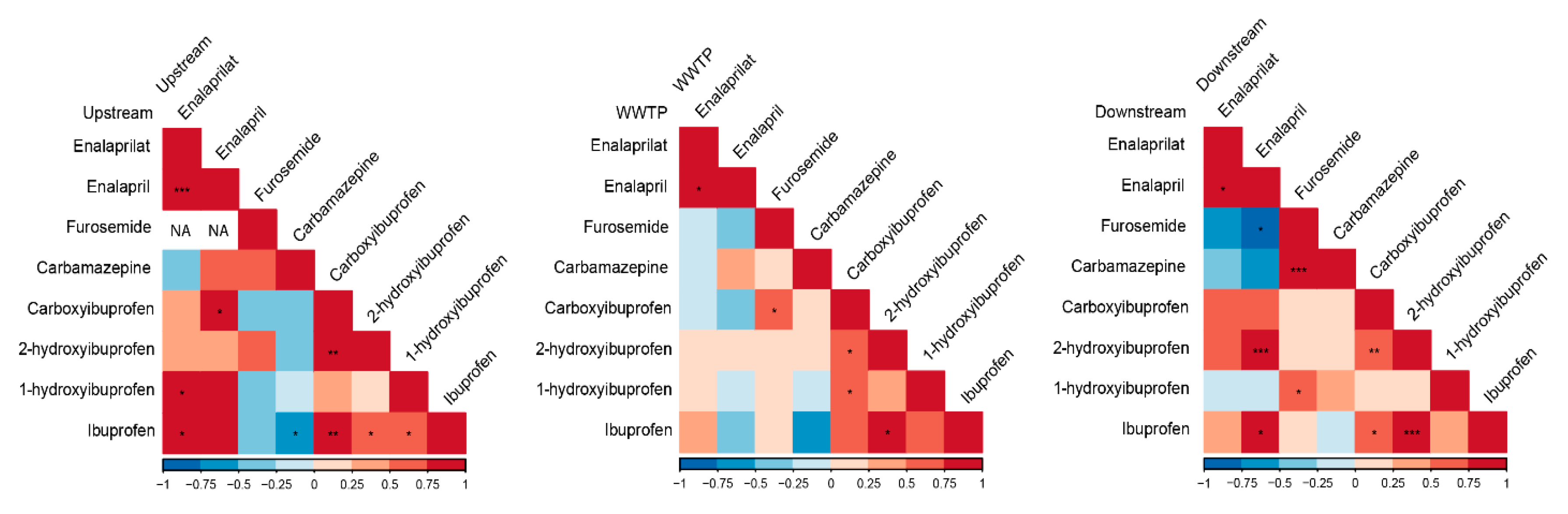
3.2. Correlations
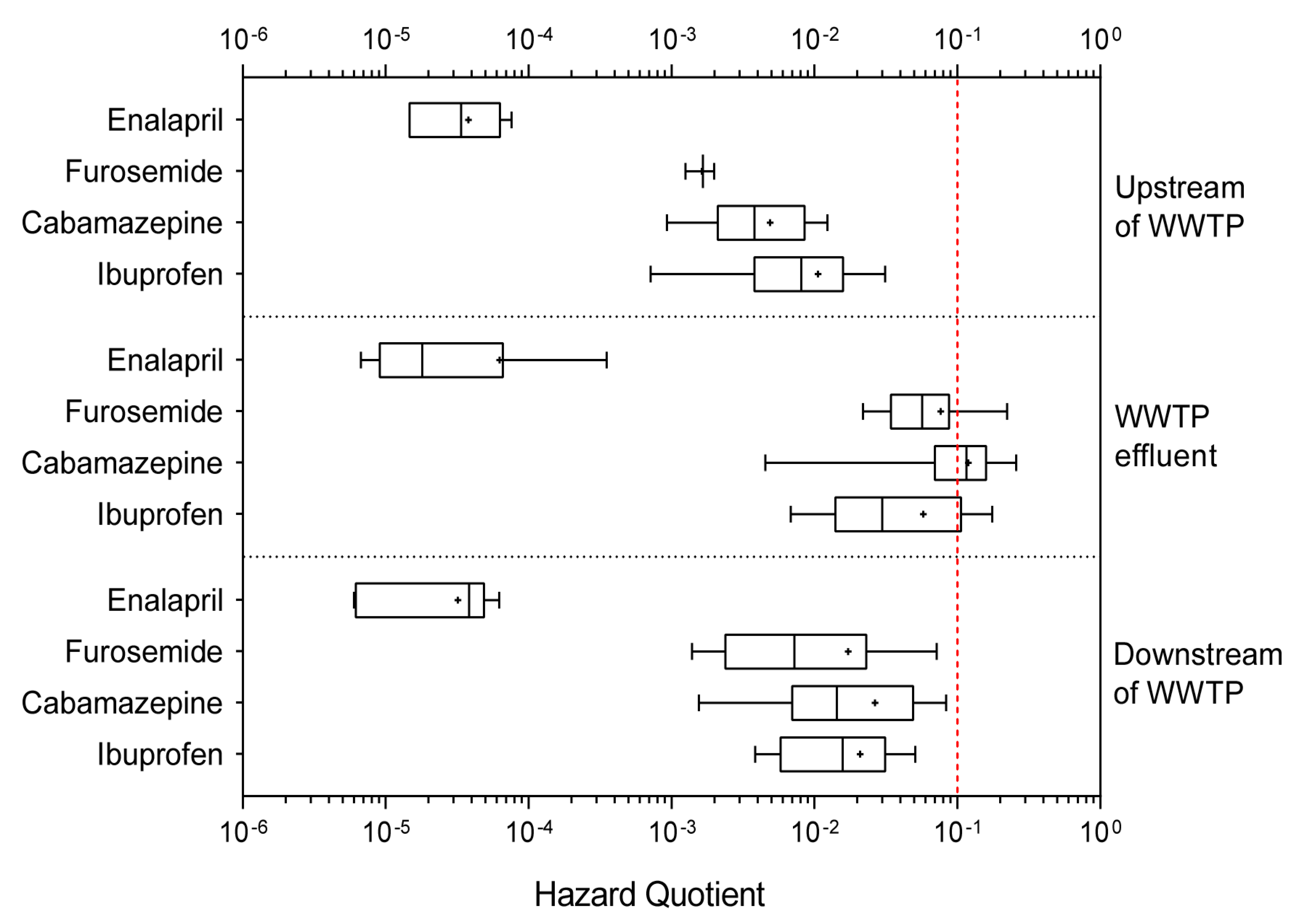
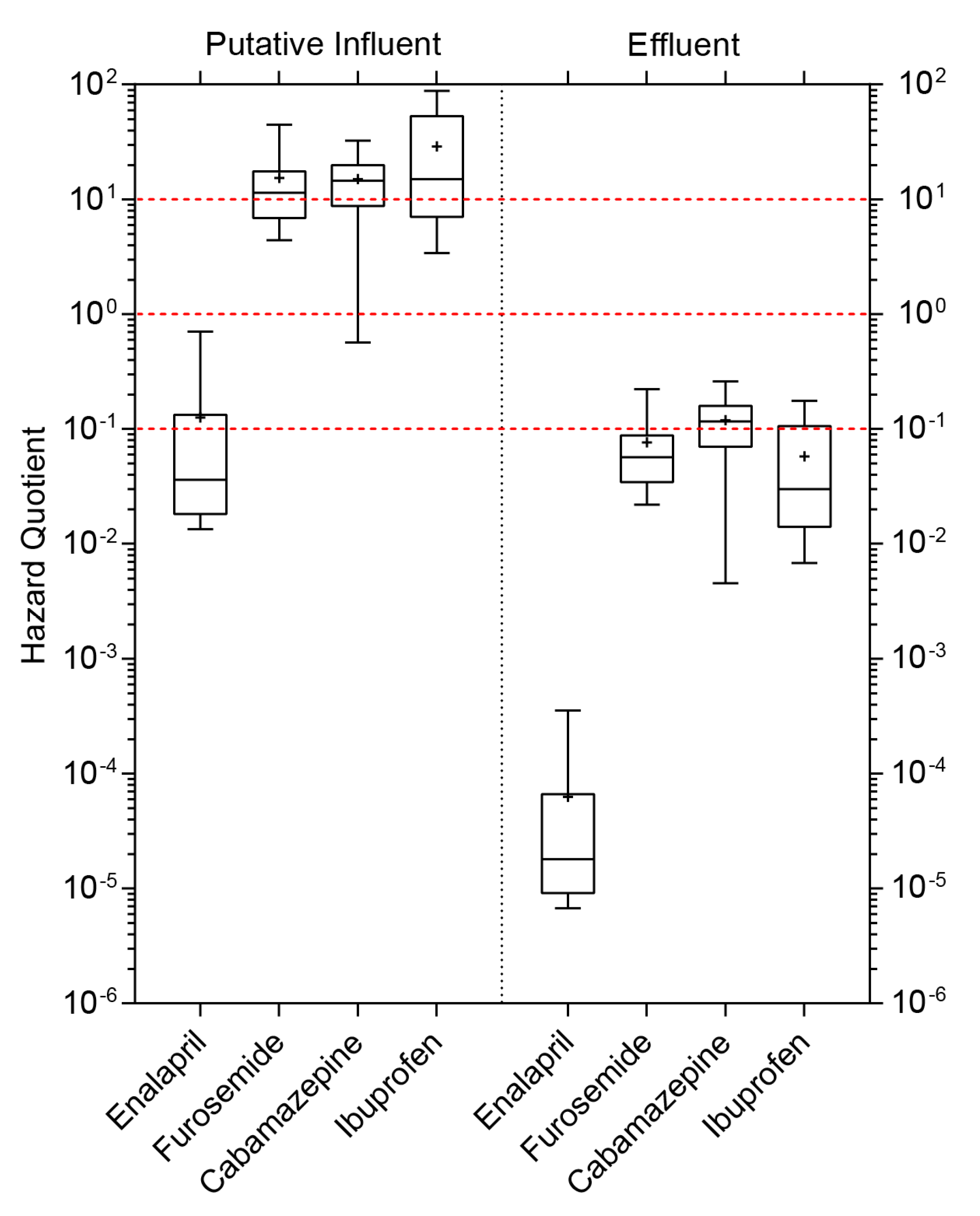
3.3. Hazard Quotient (HQ)
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Declarations
Abbreviations
| HQ | Hazard Quotient |
| WWTP | Wastewater Treatment Plants |
| PNEC | Predicted No Effect Concentration |
| MEC | measured environmental concentration |
| CAS | Chemical Abstracts Service |
| HPLC | High-Performance Liquid Chromatography |
| SPE | Solid Phase Extraction |
| RT | Retention Times |
| QqQ MS | Triple Quadrupole Mass Spectrometry |
| ESI | Electrospray Ionization |
| APCI | Atmospheric Pressure Chemical Ionization |
| CID | Collision Induced Dissociation |
| MRM | Multiple Reaction Monitoring |
| Q | Quantification Ion |
| q | Qualification Ion |
| LOD | Limit of Detection |
| LOQ | Limit of Quantification |
| RSD | Relative Standard Deviation |
| WFD | Water Framework Directive |
| EQS | Environmental Quality Standards |
| AA-EQS | Annual Average Concentration |
| MAC-EQS | Maximum Acceptable Concentration |
| ENA | Enalaprilat |
| ENP | Enalapril |
| FUR | Furosemide |
| CBZ | Carbamazepine |
| IBP | Ibuprofen |
| POPs | Persistent Organic Pollutants |
References
- Danzon, M.P. Price Comparisons for Pharmaceuticals. A Review of U.S. and Cross-National Studies; American Enterprise Institute: Washington, DC, USA, 1999; ISBN 0-8447-7133-3. [Google Scholar]
- Danzon, P.M.; Chao, L.W. Prices, Competition and Regulation in Pharmaceuticals: A Cross-National Comparison; Office of Health Economics: London, UK, 2000. [Google Scholar]
- La Farre, M.; Pérez, S.; Kantiani, L.; Barceló, D. Fate and toxicity of emerging pollutants, their metabolites and transformation products in the aquatic environment. Trends Anal. Chem. 2008, 27, 991–1007. [Google Scholar] [CrossRef]
- Bănăduc, D.; Rey, S.; Trichkova, T.; Lenhardt, M.; Curtean-Bănăduc, A. The Lower Danube River–Danube Delta–North West Black Sea: A pivotal area of major interest for the past, present and future of its fish fauna—A short review. Sci. Total Environ. 2016, 545, 137–151. [Google Scholar] [CrossRef] [PubMed]
- Bănăduc, D.; Joy, M.; Olosutean, H.; Afanasyev, S.; Curtean-Bănăduc, A. Natural and anthropogenic driving forces as key elements in the Lower Danube Basin–South-Eastern Carpathians–North-Western Black Sea coast area lakes, a broken stepping stones for fish in a climatic change scenario? Environ. Sci. Eur. 2020, 32, 14. [Google Scholar] [CrossRef]
- Bănăduc, D.; Curtean-Bănăduc, A.; Pedrotti, F.; Cianfaglione, K.; Akeroyd, J.R. Human Impact on Danube Watershed Biodiversity in the XXI Century; Springer: Berlin, Germany, 2020. [Google Scholar]
- Curtean-Bănăduc, A.; Bănăduc, D. The Transylvanian Water Tower through history. Danube News 2015, 17, 1–4. [Google Scholar]
- Curtean-Bănăduc, A.; Bănăduc, D.; Bucşa, C. Watersheds management (Transylvania/Romania): Implications, risks, solutions, Strategies to enhance environmental security in transition countries. In NATO Science for Peace and Security Series C: Environmental Security; Springer: Dordrecht, The Netherlands, 2007; p. 225. [Google Scholar]
- Posea, G. Enciclopedia Geografică a României; Editura Ştiinţifică şi Enciclopedică: Bucharest, Romania, 1982. (In Romanian) [Google Scholar]
- Mutihac, V. Structura Geologică a Teritoriului României; Editura Tehnicǎ: Bucharest, Romania, 1990. (In Romanian) [Google Scholar]
- Badea, L.; Bugă, D.; Cioflica, G.; Cucu, V.; Doniţă, I.; Gâştescu, P.; Iordan, I.; Morariu, T.; Niculescu, G.; Oancea, D.; et al. Geografia României, II, Geografia Umană şi Economic; Editura Academiei Republicii Socialiste România: Bucharest, Romania, 1984; p. 543. (In Romanian) [Google Scholar]
- Curtean-Bănăduc, A.; Burcea, A.; Mihuţ, C.-M.; Berg, V.; Lyche, J.L.; Bănăduc, D. Bioaccumulation of persistent organic pollutants in the gonads of Barbus barbus (Linnaeus, 1758). Ecotoxicol. Environ. Saf. 2020, 32, 110852. [Google Scholar] [CrossRef] [PubMed]
- Curtean-Bănăduc, A.; Bănăduc, D. Human impact effects on Târnava River Basin aquatic biodiversity (Transylvania, Romania). In Human Impact on Danube Watershed Biodiversity in the XXI Century; Springer: Cham, Switzerland, 2020; pp. 425–437. [Google Scholar]
- Carvalho, R.N.; Ceriani, L.; Ippolito, A.; Lettieri, T. Development of the first watch list under the environmental quality standards directive. JRC Sci. Hub 2015. [Google Scholar] [CrossRef]
- Schwarzenbach, R.P.; Escher, B.I.; Fenner, K.; Hofstetter, T.B.; Johnson, C.A.; von Gunten, U.; Wehrli, B. The challenge of micropollutants in aquatic systems. Science 2006, 313, 1072–1077. [Google Scholar] [CrossRef]
- Reemtsma, T.; Weiss, S.; Mueller, J.; Petrovic, M.; González, S.; Barcelo, D.; Ventura, F.; Knepper, T.P. Polar pollutants entry into the water cycle by municipal wastewater: A European perspective. Environ. Sci. Technol. 2006, 40, 5451–5458. [Google Scholar] [CrossRef]
- Loftsson, T.; Thorisdottir, S.; Fridriksdóttir, H.; Stefansson, E. Enalaprilat and enalapril maleate eyedrops lower intraocular pressure in rabbits. Acta Ophthalmol. 2010, 88, 337–341. [Google Scholar] [CrossRef]
- McFarland, J.W.; Avdeef, A.; Berger, C.M.; Raevsky, O.A. Estimating the water solubilities of crystalline compounds from their chemical structures alone. J. Chem. Inf. Comput. Sci. 2001, 41, 1355–1359. [Google Scholar] [CrossRef]
- Desbiolles, F.; Malleret, L.; Tiliacos, C.; Wong-Wah-Chung, P.; Laffont-Schwob, I. Occurrence and ecotoxicological assessment of pharmaceuticals: Is there a risk for the Mediterranean aquatic environment? Sci. Total Environ. 2018, 639, 1334–1348. [Google Scholar] [CrossRef] [PubMed]
- Yalkowsky, S.H.; Dannenfelser, R.M. Aquasol Database of Aqueous Solubility; College of Pharmacy, University of Arizona: Tucso, AZ, USA, 1992. [Google Scholar]
- Bushra, R.; Aslam, N. An overview of clinical pharmacology of ibuprofen. Oman Med. J. 2010, 25, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Ferrando-Climent, L.; Collado, N.; Buttiglieri, G.; Gros, M.; Rodriguez-Roda, I.; Rodriguez-Mozaz, S.; Barceló, D. Comprehensive study of ibuprofen and its metabolites in activated sludge batch experiments and aquatic environment. Sci. Total Environ. 2012, 438, 404–413. [Google Scholar] [CrossRef] [PubMed]
- Rabiet, M.; Togola, A.; Brissaud, F.; Seidel, J.L.; Budzinski, H.; Elbaz-Poulichet, F. Consequences of treated water recycling as regards pharmaceuticals and drugs in surface and ground waters of a medium-sized Mediterranean catchment. Environ. Sci. Technol. 2006, 40, 5282–5288. [Google Scholar] [CrossRef]
- Vieno, N.M.; Härkki, H.; Tuhkanen, T.; Kronberg, L. Occurrence of pharmaceuticals in river water and their elimination in a pilot-scale drinking water treatment plant. Environ. Sci. Technol. 2007, 41, 5077–5084. [Google Scholar] [CrossRef] [PubMed]
- Grzesiuk, M.; Spijkerman, E.; Lachmann, S.C.; Wacker, A. Environmental concentrations of pharmaceuticals directly affect phytoplankton and effects propagate through trophic interactions. Ecotoxicol. Environ. Saf. 2018, 156, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Borgmann, U.; Bennie, D.T.; Ball, A.L.; Palabrica, V. Effect of a mixture of seven pharmaceuticals on Hyalella azteca over multiple generations. Chemosphere 2007, 66, 1278–1283. [Google Scholar] [CrossRef]
- De Lange, H.J.; Noordoven, W.; Murk, A.J.; Lürling, M.F.L.L.W.; Peeters, E.T.H.M. Behavioural responses of Gammarus pulex (Crustacea, Amphipoda) to low concentrations of pharmaceuticals. Aquat. Toxicol. 2006, 78, 209–216. [Google Scholar] [CrossRef]
- Li, Z.H.; Zlabek, V.; Velisek, J.; Grabic, R.; Machova, J.; Kolarova, J.; Li, P.; Randak, T. Acute toxicity of carbamazepine to juvenile rainbow trout (Oncorhynchus mykiss): Effects on antioxidant responses, hematological parameters and hepatic EROD. Ecotoxicol. Environ. Saf. 2011, 74, 319–327. [Google Scholar] [CrossRef]
- Ogueji, E.O.; Nwani, C.D.; Iheanacho, S.C.; Mbah, C.E.; Okeke, C.O.; Yaji, A. Acute toxicity effects of ibuprofen on behaviour and haematological parameters of African catfish Clarias gariepinus (Burchell, 1822). Afr. J. Aquat. Sci. 2018, 43, 293–303. [Google Scholar] [CrossRef]
- Winter, M.J.; Owen, S.F.; Murray-Smith, R.; Panter, G.H.; Hetheridge, M.J.; Kinter, L.B. Using data from drug discovery and development to aid the aquatic environmental risk assessment of human pharmaceuticals: Concepts, considerations, and challenges. Integr. Environ. Assess. Manag. 2010, 6, 38–51. [Google Scholar] [CrossRef] [PubMed]
- Sedlak, D.L.; Gray, J.L.; Pinkston, K.E. Understanding microcontaminants in recycled water. Environ. Sci. Technol. 2000, 34, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Al-Rifai, J.H.; Gabelish, C.L.; Schäfer, A.I. Occurrence of pharmaceutically active and non-steroidal estrogenic compounds in three different wastewater recycling schemes in Australia. Chemosphere 2007, 69, 803–815. [Google Scholar] [CrossRef] [PubMed]
- Barjoveanu, G.; Cojocariu, C.; Robu, B.; Teodosiu, C. Integrated assessment of wastewater treatment plants for sustainable river basin management. Environ. Eng. Manag. J. 2010, 9, 1251–1258. [Google Scholar] [CrossRef]
- Kumar, A.; Chang, B.; Xagoraraki, I. Human health risk assessment of pharmaceuticals in water: Issues and challenges ahead. Int. J. Environ. Res. Public Health 2010, 7, 3929–3953. [Google Scholar] [CrossRef] [PubMed]
- Küster, A.; Adler, N. Pharmaceuticals in the environment: Scientific evidence of risks and its regulation. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2014, 369, 20130587. [Google Scholar] [CrossRef]
- Gheorghe, S.; Lucaciu, I.; Paun, I.; Stoica, C.; Stanescu, E. Environmental exposure and effects of some micropollutants found in the Romanian surface water. J. Environ. Prot. Ecol. 2014, 15, 878–888. [Google Scholar]
- Gheorghe, S.; Petre, J.; Lucaciu, I.; Stoica, C.; Nita-Lazar, M. Risk screening of pharmaceutical compounds in Romanian aquatic environment. Environ. Monit. Assess. 2016, 188, 379. [Google Scholar] [CrossRef]
- Iancu, V.I.; Petre, J.; Gabriel, R.L. Chromatographic method for the analysis of some pharmaceutical compounds from river water. Environ. Eng. Manag. J. 2017, 16, 67–76. [Google Scholar] [CrossRef]
- Jjemba, P.K. Excretion and ecotoxicity of pharmaceutical and personal care products in the environment. Ecotoxicol. Environ. Saf. 2006, 63, 113–130. [Google Scholar] [CrossRef]
- Lienert, J.; Bürki, T.; Escher, B.I. Reducing micropollutants with source control: Substance flow analysis of 212 pharmaceuticals in faeces and urine. Water Sci. Technol. 2007, 56, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Al Aukidy, M.; Verlicchi, P.; Jelic, A.; Petrovic, M.; Barcelò, D. Monitoring release of pharmaceutical compounds: Occurrence and environmental risk assessment of two WWTP effluents and their receiving bodies in the Po Valley, Italy. Sci. Total Environ. 2012, 438, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Gros, M.; Rodríguez-Mozaz, S.; Barceló, D. Rapid analysis of multiclass antibiotic residues and some of their metabolites in hospital, urban wastewater and river water by ultra-high-performance liquid chromatography coupled to quadrupole-linear ion trap tandem mass spectrometry. J. Chromatogr. A 2013, 1292, 173–188. [Google Scholar] [CrossRef] [PubMed]
- Gaw, S.; Thomas, K.V.; Hutchinson, T.H. Sources, impacts and trends of pharmaceuticals in the marine and coastal environment. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2014, 369, 20130572. [Google Scholar] [CrossRef]
- Chen, M.; Cooper, V.I.; Deng, J.; Amatya, P.L.; Ambrus, D.; Dong, S.; Stalker, N.; Nadeau-Bonilla, C.; Patel, J. Occurrence of pharmaceuticals in Calgary’s wastewater and related surface water. Water Environ. Res. 2015, 87, 414–424. [Google Scholar] [CrossRef]
- Ali, A.M.; Rønning, H.T.; Alarif, W.; Kallenborn, R.; Al-Lihaibi, S.S. Occurrence of pharmaceuticals and personal care products in effluent-dominated Saudi Arabian coastal waters of the Red Sea. Chemosphere 2017, 175, 505–513. [Google Scholar] [CrossRef]
- Bendz, D.; Paxéus, N.A.; Ginn, T.R.; Loge, F.J. Occurrence and fate of pharmaceutically active compounds in the environment, a case study: Höje River in Sweden. J. Hazard. Mater. 2005, 122, 195–204. [Google Scholar] [CrossRef]
- Joss, A.; Keller, E.; Alder, A.C.; Göbel, A.; McArdell, C.S.; Ternes, T.; Siegrist, H. Removal of pharmaceuticals and fragrances in biological wastewater treatment. Water Res. 2005, 39, 3139–3152. [Google Scholar] [CrossRef]
- Petrović, M.; Hernando, M.D.; Díaz-Cruz, M.S.; Barceló, D. Liquid chromatography–tandem mass spectrometry for the analysis of pharmaceutical residues in environmental samples: A review. J. Chromatogr. A 2005, 1067, 1–14. [Google Scholar] [CrossRef]
- Castiglioni, S.; Bagnati, R.; Fanelli, R.; Pomati, F.; Calamari, D.; Zuccato, E. Removal of pharmaceuticals in sewage treatment plants in Italy. Environ. Sci. Technol. 2006, 40, 357–363. [Google Scholar] [CrossRef]
- Glassmeyer, S.T.; Furlong, E.T.; Kolpin, D.W.; Cahill, J.D.; Zaugg, S.D.; Werner, S.L.; Meyer, M.T.; Kryak, D.D. Transport of chemical and microbial compounds from known wastewater discharges: Potential for use as indicators of human faecal contamination. Environ. Sci. Technol. 2005, 39, 5157–5169. [Google Scholar] [CrossRef] [PubMed]
- Gómez, M.J.; Bueno, M.M.; Lacorte, S.; Fernández-Alba, A.R.; Agüera, A. Pilot survey monitoring pharmaceuticals and related compounds in a sewage treatment plant located on the Mediterranean coast. Chemosphere 2007, 66, 993–1002. [Google Scholar] [CrossRef]
- Verlicchi, P.; Al Aukidy, M.; Zambello, E. Occurrence of pharmaceutical compounds in urban wastewater: Removal, mass load and environmental risk after a secondary treatment—A review. Sci. Total Environ. 2012, 429, 123–155. [Google Scholar] [CrossRef]
- Radjenovic, J.; Petrovic, M.; Barceló, D. Analysis of pharmaceuticals in wastewater and removal using a membrane bioreactor. Anal. Bioanal. Chem. 2007, 387, 1365–1377. [Google Scholar] [CrossRef] [PubMed]
- Pedrouzo, M.; Borrull, F.; Pocurull, E.; Marcé, R.M. Presence of pharmaceuticals and hormones in waters from sewage treatment plants. Water Air Soil Pollut. 2011, 217, 267–281. [Google Scholar] [CrossRef]
- Escher, B.I.; Baumgartner, R.; Koller, M.; Treyer, K.; Lienert, J.; McArdell, C.S. Environmental toxicology and risk assessment of pharmaceuticals from hospital wastewater. Water Res. 2011, 45, 75–92. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, S. Removal of pharmaceuticals and personal care products (PPCPs) from wastewater: A review. J. Environ. Manag. 2016, 182, 620–640. [Google Scholar] [CrossRef]
- Moldovan, Z. Occurrences of pharmaceutical and personal care products as micropollutants in rivers from Romania. Chemosphere 2006, 64, 1808–1817. [Google Scholar] [CrossRef]
- Moldovan, Z.; Schmutzer, G.; Tusa, F.; Calin, R.; Alder, A.C. An overview of pharmaceuticals and personal care products contamination along the river Someş watershed, Romania. J. Environ. Monit. 2007, 9, 986–993. [Google Scholar] [CrossRef]
- Moldovan, Z.; Chira, R.; Alder, A.C. Environmental exposure of pharmaceuticals and musk fragrances in the Somes River before and after upgrading the municipal wastewater treatment plant Cluj-Napoca, Romania. Environ. Sci. Pollut. Res. 2009, 16, 46. [Google Scholar] [CrossRef]
- Chițescu, C.L.; Nicolau, A.I. Preliminary survey of pharmaceutical residues in some important Romanian rivers. Toxicol. Environ. Chem. 2014, 96, 1333–1345. [Google Scholar] [CrossRef]
- Chițescu, C.L.; Kaklamanos, G.; Nicolau, A.I.; Stolker, A.A.M.L. High sensitive multiresidue analysis of pharmaceuticals and antifungals in surface water using U-HPLC-Q-Exactive Orbitrap HRMS. Application to the Danube river basin on the Romanian territory. Sci. Total Environ. 2015, 532, 501–511. [Google Scholar] [CrossRef] [PubMed]
- Ripp, J. Analytical Detection Limit Guidance & Laboratory Guide for Determining Method Detection Limits; PUBL-TS-056-96; Wisconsin Department of Natural Resources, Laboratory Certification Program: Madison, WI, USA, 1996.
- USEPA (U.S. Environmental Protection Agency). Protocol for EPA Approval of New Methods for Organic and Inorganic Analytes in Wastewater and Drinking Water; U.S. Environmental Protection Agency: Washington, DC, USA, 1999.
- Taiyun, W.; Viliam, S. R Package “Corrplot”: Visualization of a Correlation Matrix, Version 0.84. 2017. Available online: https://github.com/taiyun/corrplot (accessed on 31 May 2020).
- QGIS Development Team. QGIS Geographic Information System; Open Source Geospatial Foundation: Chicago, IL, USA, 2019. [Google Scholar]
- Water Framework Directive (WFD)—Directive 2000/60/EC of the European Parliament and of the Council of 23 October 2000 Establishing a Framework for Community Action in the Field of Water Policy. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:32000L0060 (accessed on 28 November 2020).
- Moermond, C.T.A. Environmental Risk Limits for Pharmaceuticals: Derivation of WFD Water Quality Standards for Carbamazepine, Metoprolol, Metformin and Amidotrizoic Acid; RIVM Report 27000602; National Institute for Public Health and the Environment: Utrecht, The Netherlands, 2014.
- WCA (World Cargo Alliance). Derivation of Proposed Environmental Quality Standards for Ibuprofen, Draft Report to DG Environment from WCA; WCA: Oxon, UK, 2014. [Google Scholar]
- Hernando, M.D.; Mezcua, M.; Fernández-Alba, A.R.; Barceló, D. Environmental risk assessment of pharmaceutical residues in wastewater effluents, surface waters and sediments. Talanta 2006, 69, 334–342. [Google Scholar] [CrossRef] [PubMed]
- European Communities (EC). Technical Guidance Documents in Support of the Commission Directive 93/667/EEC on Risk Assessment for New Notified Substances and the Commission Regulation (EC) 1488/94 on Risk Substances. (Part 1, 2 and 3); European Communities (EC): Ispra, Italy, 1996; Available online: https://publications.europa.eu/en/publication-detail/-/publication/9aebb292-39c5-4b9c-b4cb-97fb02d9bea2 (accessed on 31 May 2020).
- Miege, C.; Choubert, J.M.; Ribeiro, L.; Eusebe, M.; Coquery, M. Fate of pharmaceuticals and personal care products in wastewater treatment plants—Conception of a database and first results. Environ. Pollut. 2009, 157, 1721–1726. [Google Scholar] [CrossRef] [PubMed]
- Al-Janabi, A.A.H.S. In vitro antibacterial activity of ibuprofen and acetaminophen. J. Global Infect. Dis. 2010, 2, 105–108. [Google Scholar] [CrossRef]
- Quintana, J.B.; Weiss, S.; Reemtsma, T. Pathways and metabolites of microbial degradation of selected acidic pharmaceutical and their occurrence in municipal wastewater treated by a membrane bioreactor. Water Res. 2005, 39, 2654–2664. [Google Scholar] [CrossRef]
- Tixier, C.; Singer, H.P.; Oellers, S.; Müller, S.R. Occurrence and fate of carbamazepine, clofibric acid, diclofenac, ibuprofen, ketoprofen, and naproxen in surface waters. Environ. Sci. Technol. 2003, 37, 1061–1068. [Google Scholar] [CrossRef]
- Lin, A.Y.C.; Reinhard, M. Photodegradation of common environmental pharmaceuticals and estrogens in river water. Environ. Toxicol. Chem. 2005, 24, 1303–1309. [Google Scholar] [CrossRef]
- Andreozzi, R.; Marotta, R.; Pinto, G.; Pollio, A. Carbamazepine in water: Persistence in the environment, ozonation treatment and preliminary assessment on algal toxicity. Water Res. 2002, 36, 2869–2877. [Google Scholar] [CrossRef]
- Joint Danube Survey (JDS) 3-2013. A Comprehensive Analysis of Danube Water Quality. Final Report. International Commission for the Protection of the Danube River, Vienna. 2015. Available online: https://www.icpdr.org/main/sites/default/files/nodes/documents/jds3_final_scientific_report_2.pdf (accessed on 31 May 2020).
- Loos, R.; Gawlik, B.M.; Locoro, G.; Rimaviciute, E.; Contini, S.; Bidoglio, G. EU-wide survey of polar organic persistent pollutants in European river waters. Environ. Pollut. 2009, 157, 561–568. [Google Scholar] [CrossRef]
- Ho, K.T.; Konovets, I.M.; Terletskaya, A.; Milyukin, M.V.; Lyashenko, A.V.; Shitikova, L.I.; Shevchuk, L.I.; Afanasyev, S.; Krot, Y.G.; Ye, K.; et al. Contaminants, mutagenicity and toxicity in the surface waters of Kyiv, Ukraine. Mar. Pollut. Bull. 2020, 155, 111153. [Google Scholar] [CrossRef] [PubMed]
- Barinova, S.; Krassilov, V.A. Algal diversity and bio-indication of water resources in Israel. Int. J. Environ. Resour. 2012, 1, 62–72. [Google Scholar]
- Wepener, V. Statement of world aquatic scientific societies on the need to take urgent action against human-caused climate change, based on scientific evidence. Afr. J. Aquat. Sci. 2020, 45, 383–385. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Substance | CAS Number | Molecular Weight | Water Solubility | pKa | Log Kow | PNEC |
|---|---|---|---|---|---|---|
| Enalaprilat | 76420-72-9 | 348.399 g/mol | 0.876 mg/mL | 3.13 | −0.94 [17] | NA |
| Enalapril | 75847-73-3 | 376.453 g/mol | 16.4 g/L [18] | 3.67 | 4.22 | 184 µg/L [19] |
| Furosemide | 54-31-9 | 330.739 g/mol | 73.1 mg/L [20] | 4.25 | 2.03 | 6.2 µg/L [19] |
| Carbamazepine | 298-46-4 | 236.274 g/mol | 0.152 mg/mL | 15.96 | 2.45 | 7.7 µg/L [19] |
| Ibuprofen | 15687-27-1 | 206.285 g/mol | 21 mg/L [20] | 5.3 [21] | 3.97 | 2.3 µg/L [19] |
| Carboxyibuprofen | 15935-54-3 | 236.267 g/mol | 0.3 g/L | 3.97 | 2.78 [22] | NA |
| 1-hydroxyibuprofen | 53949-53-4 | 222.284 g/mol | 0.51 g/L | 4.55 | 2.69 [22] | NA |
| 2-hydroxyibuprofen | 51146-55-5 | 222.284 g/mol | 0.3 g/L | 4.63 | 2.37 [22] | NA |
| Substance | RT | Ion Mode | Ion Transition | Fragmentor (V) | Collision Energy (V) |
|---|---|---|---|---|---|
| Enalaprilat | 3.808 | Positive | Q 349.2→206.2 | 135 | 15 |
| Positive | q 349→303.2 | 135 | 12 | ||
| Enalapril | 7.201 | Positive | Q 377.3→234.2 | 70 | 17 |
| Positive | q 377.3→303.3 | 70 | 12 | ||
| Furosemide | 7.593 | Negative | Q 329→285.1 | 120 | 10 |
| Negative | q 329→204.7 | 110 | 20 | ||
| Carbamazepine | 7.917 | Positive | Q 237→194 | 110 | 15 |
| Positive | q 237→191.9 | 110 | 35 | ||
| * 10,11-dihydrocarbamazepine | 8.052 | Positive | Q 239.1→196 | 110 | 25 |
| Positive | q 239.1→180.1 | 110 | 25 | ||
| Ibuprofen | 7.240 | Negative | Q 205→161 | 75 | 5 |
| Carboxyibuprofen | 5.516 | Negative | Q 235→191 | 75 | 5 |
| 1-hydroxyibuprofen | 5.811 | Negative | Q 221→159 | 75 | 5 |
| 2-hydroxyibuprofen | 5.526 | Negative | Q 221→177 | 75 | 0 |
| * Ibuprofen-d3 | 7.239 | Negative | Q 208→164 | 75 | 0 |
| Substance | Quantification Transition | LOD ppb | LOQ ppb |
|---|---|---|---|
| Enalaprilat | 349.2→206.2 | 0.592 | 1.972 |
| Enalapril | 377.3→234.2 | 0.625 | 2.084 |
| Furosemide | 329→285.1 | 0.868 | 2.894 |
| Carbamazepine | 237→194 | 0.355 | 1.183 |
| Ibuprofen | 205→161 | 0.806 | 2.687 |
| Carboxyibuprofen | 235→191 | 0.795 | 2.648 |
| 1-hydroxyibuprofen | 221→159 | 0.736 | 2.453 |
| 2-hydroxyibuprofen | 221→177 | 0.686 | 2.287 |
| Location | Substance | Min (ng/L) | Max (ng/L) | Median (ng/L) | Average (ng/L) | N | F |
|---|---|---|---|---|---|---|---|
| Upstream | Enalaprilat | 1.19 | 23.16 | 7.66 | 9.02 | 6 | 40% |
| Enalapril | 2.70 | 14.00 | 6.22 | 6.96 | 5 | 33% | |
| Furosemide | 7.78 | 12.30 | 10.27 | 10.12 | 3 | 20% | |
| Carbamazepine | 7.16 | 95.11 | 29.38 | 37.72 | 14 | 93% | |
| Carboxyibuprofen | 6.74 | 111.61 | 26.30 | 31.30 | 13 | 87% | |
| 2-hydroxyibuprofen | 2.27 | 49.49 | 2.27 | 2.27 | 15 | 100% | |
| 1-hydroxyibuprofen | 0.28 | 4.66 | 2.19 | 2.39 | 13 | 87% | |
| Ibuprofen | 1.65 | 71.85 | 18.59 | 24.39 | 12 | 80% | |
| WWTP effluent | Enalaprilat | 2.54 | 146.66 | 7.93 | 24.82 | 9 | 60% |
| Enalapril | 1.24 | 64.93 | 3.31 | 11.54 | 9 | 60% | |
| Furosemide | 135.92 | 1379.37 | 352.43 | 473.62 | 14 | 93% | |
| Carbamazepine | 34.95 | 1992.43 | 893.94 | 918.99 | 14 | 93% | |
| Carboxyibuprofen | 17.84 | 2036.70 | 91.36 | 431.01 | 12 | 80% | |
| 2-hydroxyibuprofen | 15.94 | 826.16 | 85.29 | 221.64 | 12 | 80% | |
| 1-hydroxyibuprofen | 1.30 | 84.22 | 7.82 | 22.85 | 13 | 87% | |
| Ibuprofen | 15.68 | 403.06 | 68.66 | 132.62 | 8 | 53% | |
| Downstream | Enalaprilat | 1.83 | 19.07 | 8.83 | 8.90 | 8 | 53% |
| Enalapril | 1.11 | 11.50 | 7.07 | 5.90 | 7 | 47% | |
| Furosemide | 8.63 | 444.63 | 44.84 | 106.81 | 12 | 80% | |
| Carbamazepine | 11.99 | 643.31 | 110.26 | 204.15 | 15 | 100% | |
| Carboxyibuprofen | 6.76 | 166.28 | 22.38 | 51.74 | 15 | 100% | |
| 2-hydroxyibuprofen | 11.92 | 85.68 | 33.23 | 43.28 | 15 | 100% | |
| 1-hydroxyibuprofen | 0.16 | 11.24 | 2.80 | 4.14 | 14 | 93% | |
| Ibuprofen | 8.84 | 117.14 | 36.17 | 47.88 | 11 | 73% |
| Location | ENA | ENP | FUR | CBZ | CarboxyIBP | 2-hydroxyiIBP | 1-hydroxyIBP | IBP | |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Upstream | 4.88 | NA | NA | 20.32 | 6.74 | 21.57 | NA | NA |
| Downstream | 7.13 | NA | NA | 22.45 | 6.79 | 27.56 | NA | NA | |
| Effluent | 10.55 | 3.31 | 150.26 | 444.73 | 25.19 | 548.05 | 6.99 | 271.60 | |
| 2 | Upstream | NA | NA | NA | 17.47 | NA | 2.89 | 2.86 | NA |
| Downstream | NA | NA | 68.65 | 477.26 | 14.90 | 29.04 | 2.84 | NA | |
| Effluent | 4.32 | NA | 135.92 | 1224.15 | 25.20 | 69.87 | 3.07 | NA | |
| 3 | Upstream | NA | NA | NA | 30.25 | NA | 32.10 | 0.28 | 1.65 |
| Downstream | NA | NA | 143.36 | 377.68 | 93.31 | 74.65 | 0.16 | NA | |
| Effluent | NA | NA | 441.74 | 1230.86 | 254.44 | 226.54 | 1.30 | NA | |
| 4 | Upstream | NA | NA | 12.30 | 95.11 | 13.24 | 22.09 | 2.47 | 9.93 |
| Downstream | NA | NA | 21.04 | 146.56 | 14.18 | 27.44 | 2.79 | 14.07 | |
| Effluent | NA | NA | 298.53 | 1079.31 | 391.16 | 320.95 | 27.08 | 43.14 | |
| 5 | Upstream | 1.73 | 2.71 | NA | 8.97 | 27.96 | 43.24 | 1.77 | 24.00 |
| Downstream | 1.83 | 2.61 | 294.59 | 254.64 | 6.76 | 56.40 | 11.24 | 63.69 | |
| Effluent | NA | 3.20 | 847.10 | 568.59 | 37.55 | 84.94 | 21.94 | 92.47 | |
| 6 | Upstream | NA | NA | 7.78 | 71.37 | 15.34 | 21.97 | 2.78 | 15.63 |
| Downstream | NA | NA | 8.63 | 85.65 | 13.57 | 17.85 | 2.44 | 16.35 | |
| Effluent | 6.51 | NA | 214.79 | 1701.62 | 22.72 | 15.94 | 3.98 | 15.68 | |
| 7 | Upstream | NA | NA | NA | 71.23 | 7.57 | 15.77 | 2.16 | 8.32 |
| Downstream | NA | NA | 14.44 | 110.26 | 8.39 | 16.81 | 2.54 | 8.84 | |
| Effluent | NA | NA | 241.95 | 876.52 | 17.84 | 32.34 | 8.53 | 28.67 | |
| 8 | Upstream | 23.16 | 14.00 | NA | 12.59 | 53.54 | 30.13 | 2.55 | 44.05 |
| Downstream | 19.07 | 11.50 | NA | 94.46 | 166.28 | 85.68 | 9.02 | 107.35 | |
| Effluent | NA | NA | NA | NA | 1646.56 | NA | 84.22 | 403.06 | |
| 9 | Upstream | 12.73 | 9.17 | 10.27 | 28.52 | 48.25 | 49.49 | 4.23 | 71.85 |
| Downstream | 13.34 | 8.93 | 15.91 | 88.20 | 50.50 | 65.68 | 4.55 | 64.87 | |
| Effluent | 7.93 | 7.29 | 325.29 | 1194.42 | NA | 85.64 | 2.22 | 44.84 | |
| 10 | Upstream | 10.45 | 6.22 | NA | 7.16 | 26.30 | 37.13 | 2.19 | 36.95 |
| Downstream | 13.25 | 7.07 | 17.11 | 53.88 | 22.38 | 42.91 | 2.68 | 36.17 | |
| Effluent | 31.17 | 17.04 | 1379.37 | 1992.43 | 542.88 | 321.89 | 61.52 | NA | |
| 11 | Upstream | NA | NA | NA | 63.70 | 33.74 | 31.19 | 1.62 | 15.26 |
| Downstream | 3.15 | 1.14 | 444.63 | 643.31 | 25.60 | 33.23 | 7.00 | NA | |
| Effluent | 3.65 | 1.24 | 439.93 | 663.75 | NA | NA | NA | NA | |
| 12 | Upstream | NA | 2.70 | NA | NA | 8.10 | 2.27 | NA | NA |
| Downstream | 10.52 | 8.97 | 11.21 | 11.99 | 161.05 | 68.29 | 1.39 | 117.14 | |
| Effluent | 146.6 | 64.93 | 207.04 | 225.99 | NA | NA | NA | NA | |
| 13 | Upstream | 1.19 | NA | NA | 38.64 | 45.85 | 26.10 | 1.66 | 21.54 |
| Downstream | 2.93 | 1.11 | 101.57 | 234.56 | 29.76 | 11.92 | 2.81 | 13.33 | |
| Effluent | 10.04 | 3.49 | 414.28 | 717.23 | 26.65 | 61.82 | 7.82 | NA | |
| 14 | Upstream | NA | NA | NA | 25.61 | 111.61 | 40.23 | 4.66 | 35.12 |
| Downstream | NA | NA | NA | 32.43 | 20.47 | 28.60 | 2.26 | 13.09 | |
| Effluent | NA | 1.27 | 1154.93 | 34.95 | 145.17 | 65.59 | 3.97 | NA | |
| 15 | Upstream | NA | NA | NA | 37.14 | 8.64 | 10.74 | 1.80 | 8.34 |
| Downstream | NA | NA | 140.53 | 428.90 | 142.12 | 63.09 | 6.25 | 71.84 | |
| Effluent | 2.54 | 2.08 | 379.57 | 911.36 | 2036.70 | 826.16 | 64.42 | 161.47 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burcea, A.; Boeraş, I.; Mihuţ, C.-M.; Bănăduc, D.; Matei, C.; Curtean-Bănăduc, A. Adding the Mureş River Basin (Transylvania, Romania) to the List of Hotspots with High Contamination with Pharmaceuticals. Sustainability 2020, 12, 10197. https://doi.org/10.3390/su122310197
Burcea A, Boeraş I, Mihuţ C-M, Bănăduc D, Matei C, Curtean-Bănăduc A. Adding the Mureş River Basin (Transylvania, Romania) to the List of Hotspots with High Contamination with Pharmaceuticals. Sustainability. 2020; 12(23):10197. https://doi.org/10.3390/su122310197
Chicago/Turabian StyleBurcea, Alexandru, Ioana Boeraş, Claudia-Maria Mihuţ, Doru Bănăduc, Claudiu Matei, and Angela Curtean-Bănăduc. 2020. "Adding the Mureş River Basin (Transylvania, Romania) to the List of Hotspots with High Contamination with Pharmaceuticals" Sustainability 12, no. 23: 10197. https://doi.org/10.3390/su122310197
APA StyleBurcea, A., Boeraş, I., Mihuţ, C.-M., Bănăduc, D., Matei, C., & Curtean-Bănăduc, A. (2020). Adding the Mureş River Basin (Transylvania, Romania) to the List of Hotspots with High Contamination with Pharmaceuticals. Sustainability, 12(23), 10197. https://doi.org/10.3390/su122310197