Abstract
In the stage of aging society and population aging, the social needs of the elderly are widely discussed by researchers. Especially driven by the demand of tele-medical treatment and tele-rehabilitation therapy, it is vital for the elderly to integrate into virtual communities by combining social virtual reality (VR) with different medical services and entertainment needs. In addition, affected by the COVID-19 epidemic, it is more difficult for people to have face-to-face contacts. With more remote consultation, entertainment and virtual social connectivity, the application of social VR is more urgent and valuable. However, there is little discussion on the acceptability and influencing factors of social VR among the elderly at present. Therefore, in order to get further data, we used (1) early stage semi-structured interviews and then (2) Unified Theory of Acceptance and Use of Technology (UTAUT) questionnaires for investigation. One hundred fourteen elderly people aged 60–89 living in the metropolitan area of Taipei were taken as the subjects. To help them understand the situation and state of using social VR, these elderly people were asked to use a head-mounted display (HMD) to experience social VR games. The preliminary results showed that the elderly had obvious preference for entertainment (32.4%) and medical treatment (31.3%). The interview showed that this was related to the physiological condition or medical needs of the age range. In order to further understand how social VR would affect the social life of the elderly, we proposed the further demand structure of UTAUT Model based on the interview of both experts and the elderly. The model structures include (1) Performance Expectancy, (2) Perceived Enjoyment, (3) Social Influence, (4) User Attitude, (5) Behavioral Intention, and so on. These structures were applied to conduct interviews and questionnaires to find out the influence extent and relevance of the elderly on different structural needs, and suggestions were given accordingly. The results of the above interviews showed that (1) the elderly thought that the functions of entertaining and interacting of social VR could increase their social opportunities, and also meet medical needs (teleconference, cognitive decline, etc.), (2) the closeness of social relations (between family members, friends, doctors, and places), and also affect the relevance of Perceived Enjoyment (β = 0.77, p = 0.000 < 0.05). The results of these phenomena and interviews showed the interplay between the demand structures and their special relevance. They also indicated that as to social VR technologies, various demands and functional issues of the elderly need to be considered, and these demands would appear in the subtle usage, and different social VR interfaces and functions would emerge based on their special living ways and physical and psychological demands.
1. Introduction
1.1. The Living Problems and Social Needs of Urban Elderly
The aging population presents challenges to all aspects of society. By 2050, it is predicted that human life expectancy will increase by another 10 years [1]. As the aging of the population continues to increase, problems related to the physical and mental health and social relations of the elderly are emerging. Numerous studies have shown that isolation or loneliness has a negative effect on the physical and mental health of the elderly [2]. However, elderly individuals often feel socially lonely as a result of their narrow social circle, retirement [3,4], loss of relatives and friends, and decline in physical health, leading to a reduced willingness and opportunity to socialize [5].
Yang and Victor showed that the urban elderly aged over 65 years old experienced the highest levels of loneliness [6]. Although family and social support are helpful to overcome loneliness in the elderly [7], as children go out to work and changes in the family structure occur, the frequency of communication declines, making them prone to loneliness and social issues. To help the elderly to age healthily and improve their quality of life, it has been proposed that enhancing the social participation of the elderly can improve their physical and mental health [8,9]. Methods to attract the elderly to actively participate in social interactions, strengthen their health and mobility, and live safely have also emerged as a key issue within global society.
1.2. Social Networks and Applications Can Effectively Reduce Social Loneliness
Social network assistance and social applications can effectively reduce the loneliness of the elderly [10,11]. Hagan et al. [12] analyzed 17 studies related to loneliness interventions and found that network communication technology could significantly reduce loneliness. Further studies confirmed a positive and significant relationship between social networks and quality of life of the elderly [13,14,15,16,17]. The size of the social network and the satisfaction of social interactions have also been shown to be associated with autism and depression in the elderly [18,19,20]. Ali et al. verified the relationship between network diversity and the risk of death, indicating that increasing the diversity of social networks was essential to improve the health and survival of the elderly [21,22].
1.3. Virtual Reality (VR) Technology Can Promote Social Networks within the Elderly Population
In the era of 5G networks, online social platforms, technology, and hardware, VR can impact the social life of elderly individuals [23]. In particular, the elderly have the experience and ability to use technology. With advancements over the next 5–10 years, elderly users who are familiar with the use of technology products are anticipated to increase. The urban elderly are more aware of current technology and social services, and will be more open to the application of VR technology in their lives. Moreover, related studies highlight how VR technology can improve the quality of life of the elderly [24] by reducing social isolation and loneliness.
2. Related Works
2.1. Social Service Provided by VR Technology
The physical health of the elderly and the fear of falling can affect how frequently elderly members of the population go shopping [25]. The possibility of the elderly using VR for virtual shopping is significant, accordingly. Claudia et al. discussed the positive impact of VR experience on elderly individuals from the perspective of travelling [26] and confirmed that VR technology could provide users with travel services and help improve their experience. Shabbir et al. showed that the social influence and perceived enjoyment of the elderly played an important role in the intention of using VR [27]. Roberts et al. also certified that usefulness was a key factor influencing the acceptance of VR by the elderly, and suggested that increasing interactivity could maximize the advantages of VR to promote social interaction with family and friends. The expected categories include travel, continued education, reminiscence, and self-care [28]. In addition, the behavioral intentions of the elderly when experiencing VR leisure activities highlight enjoyment as the major aspect, indicating that when the elderly find an activity that is interesting and relaxing, it helps to improve health [29,30]. Based on the limitations of subjective and objective conditions, the elderly need more convenient and effective methods in their daily life activities to meet these diversified needs.
2.2. Advantages of VR Technology in Social Development
Social VR allows users from different locations to simultaneously interact and share 3D scenes in an immersive virtual environment (IVE). They can also enjoy real-time face-to-face communication. voices, facial expressions, and actions [23,31,32,33,34], without being affected by the natural environment and region. This can realize realistic social participation and improve safety. Moreover, Jie Li et al. compared the photo sharing experience under social VR with Skype and Facebook spaces, and found that social VR was closer to face-to-face (F2F) sharing [32,35]. Baker et al. [36] studied 22 elderly individuals to obtain their views on social VR in the form of a workshop, and suggested that social VR virtual items could trigger memories that could be shared with others, meeting their social needs [33]. These functions of VR are beyond the reach of other social applications, and provide a virtual public space that can improve the sense of social participation, ensure safety, and enhance mobility. These benefits highlight the potential of these channels to generate social behavior within the elderly population.
2.3. Innovation and Contributions of this Study
The main innovation and contributions of this study are to propose a new direction and guidance for the social contact solutions of the elderly, and in addition to the differences in users, the innovation also lies in the usage of devices and situations. As has been described many times in previous sections, the social VR used in this study is designed to help the elderly create different social content and services in terms of visual immersion and perception, unlike previous studies that were focused only on single-product betterment or community services for social interaction in the elderly. Meanwhile, this study is of a regional character, including the issue of the elderly living alone caused by changing life state of urban population, or the gap between people by COVID-19, the situation which never happened in the past.
However, this new situation offers a new possibility and opportunity in the study, and also contributes to the use of social VR in the elderly population, so this study tries to make a difference in the study and provide different ideas and innovation available to the readers.
2.4. Gaps in Previous Studies
Previous studies have discussed and proposed improvement to address loneliness of the elderly, but most have focused only on “physical products,” such as home robots for the elderly (i.e., the use of sea dog robots to accompany the elderly) to address social loneliness and the need for virtual companionship [37]. Other studies also showed that the loneliness of the elderly would be dispelled via home care services. However, most are beneficial for alleviating the loneliness [38,39], but rarely explore or really solve their social dilemmas.
Compared with the above-mentioned solutions, social VR enables a person to quickly blend into different situations and needs due to its ability to immerse and transform the state of perception. In such situations, social interaction could go beyond the “distance” and “space-time.” The elderly thus have more social possibilities, including changing their self-impersonation to become another young face [40], or interacting without the constraints of time or space, even discussing remote issues [41]. All of these can be attributed to the usage of social VR, which results in differences distinctly from the previous studies.
The differences and strengths between this study and previous studies:
- (1)
- Most of the current literature on social VR is aimed at the young, with few designed for the needs of the elderly [35,42,43].
- (2)
- In addition, studies on the elderly centers on the design of the virtual avatar [36], with no comprehensive consideration of multiple dimensions and variable factors, and no guidance based on them.
- (3)
- This study aims at the elderly group in the metropolitan areas, which is also different from the broad elderly group targeted by previous studies. Since they are more familiar with technology and urban life, these urban elderly people are more likely to be the key customers of social VR investment over the next 10 years.
- (4)
- In the end, the related social VR is mostly aimed at using the screen as an interactive carrier or mobile games. To compensate for it, this study is mainly focused on the construction of social VR under remote service, which is mainly designed under the application of immersive VR devices according to the coherent service content and situational design, instead of a single game use or entertainment needs.
- (5)
- Previous studies have focused on the design of physical therapeutic products, such as the use of therapeutic sea dog robots to accompany the elderly and provide services of therapeutic interaction, but few studies have focused on the relationship between virtual and real world. In the framework of social VR, such studies have highlighted the particularities and uses of virtual situations, and activated the potential of services and study.
2.5. Summary
Due to the increase in the proportion of the elderly population in the Metropolitan Area of Taiwan, especially in the aging society, the social needs of the elderly are particularly concerned. Coupled with the changes in urban living conditions, a growing body of the elderly live alone, highlighting the urgent demand of the elderly for social VR over the next decade.
Therefore, this study investigated the demand structure of the elderly, and constructed the Unified Theory of Acceptance and Use of Technology (UTAUT) Model and its structure factor according to the preliminary opinion of 10 extra elderly objects recruited in the earlier stage of the study. More than that, these structures have been developed into the UTAUT Model’s demand structure questionnaire, which was distributed to 114 elderly aged 60–89 living in the urban area of Taipei. The purpose of this study was to conduct questionnaires and interviews in order to solve the social contact of the elderly in the metropolitan areas, so as to identify the status and related factors of these demand factors by the elderly. However, the elderly suffer from social barriers due to their solitary form, children’s separation from their homes, inter-generational relations, and social isolation in the current epidemic situation. This study could shed light on the connections and associations between the services that the elderly want in different structures, rather than on the interaction between games and body. They are more eager to reach medical or entertainment assistance through social VR, and to access the service and conveniences of the technology in a simpler way. In order to obtain more authentic and representative data, the study team conducted a long-term observational and participatory design study in the elderly nursing home.
3. Methods
A questionnaire survey was performed on 114 elderly individuals aged 60–89. Prior to filling out the questionnaire, the researcher asked the participants to try on the Memo VR Headset as a virtual reality experience (Figure 1). The elderly’s understanding of social VR was improved by playing a Facebook Horizon [44] video. During the video, the researcher explained the video content and related services.

Figure 1.
Use of the Memo virtual reality (VR) headset to experience virtual reality.
3.1. Participants
In total, 114 elderly participants completed the questionnaire, including 79 women and 35 men, with an average age of 68.6 years. The survey was conducted at the Taipei Elderly Activity Center.
3.2. Procedure
We focused on the generalization and application of VR technology to social development in the elderly using the UTAUT Model to understand the user’s acceptance of new information. The UTAUT Model adopted in this study is the acceptance and evaluation tool widely used in the application of science and technology to the users, and the calculation method and evaluation data adopted in this study are in accordance with the standard framework of UTAUT Model [45,46], and there is no difference. The UTAUT Model used in this study is only adjusted according to the elements of the structure, and uses the experimental procedures and methods set by the previous researchers [47,48]. The sample population of the experts and the elderly are required to master the reliability and validity to improve the performance of the study.
Through early stage semi-structured interviews, we assessed the factors related to social VR video content and old age, the elderly’s acceptance of science and technology, and summarized the factors influencing the acceptance of technology. This analysis stage was divided into two stages (Figure 2).
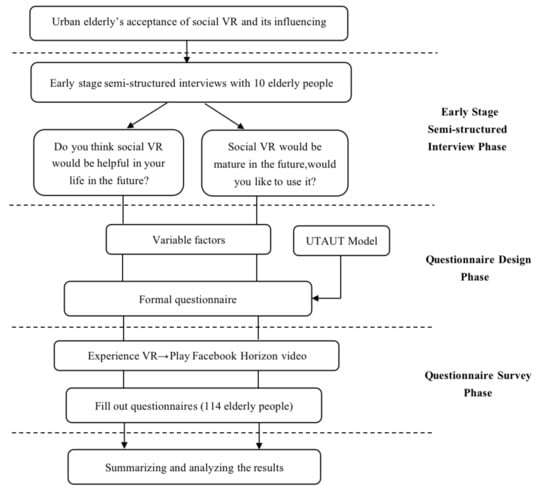
Figure 2.
Specific implementation process.
Stage 1: Early stage semi-structured interviews. In the process, a head-mounted display (HMD) is used as a tool and experimental carrier to sample the social VR, and the interactive content of the game application program provides the elderly with a preliminary experience to help them quickly grasp the concept of the social VR and the sense of the game. In terms of parameters, before designing the questionnaire, the key words are extracted from the interview responses of 10 elderly as the variable factors in the questionnaire, so as to improve the reliability of the questionnaire.
Stage 2: Questionnaire design and survey. After that, three experts were asked to revise the questionnaire and the preliminary opinions of 10 elderly objects were collected to find out the demand structure that the elderly wanted to obtain in the social VR, in order to verify the validity of the questionnaire. When the questionnaire design was completed, it was used as the structure design of UTAUT Model, and semi-structured interviews and questionnaires with the elderly ensued in order to identify their perceptive problems.
3.2.1. Early Stage Semi-Structured Interviews
During the early stage semi-structured interview process, one-to-one interviews were performed according to topic, with each interview lasting approximately 10 min. The interview topics included the following questions: (1) Do you think social VR would be helpful in your life in the future? (2) Social VR would be mature in the future, would you like to use it?
The preliminary results of the interviews provided a reference for the design of the second-stage questionnaire. Each interview process was recorded, and brief minutes were compiled.
3.2.2. Questionnaire Design
A preliminary questionnaire was formed based on the early stage semi-structured interviews. The relevant questionnaire was then revised by an expert group to ensure it could be easily understood, which could be seen the Questionnaire in Supplementary Materials.
The questionnaire consisted of two parts. Part one focused on basic information of the elderly, including age, gender, education level, living conditions, social tools, and service types.
The second part of the survey focused on the dimensions influencing the elderly’s acceptance of social VR, including: (1) Performance expectancy (PE), (2) Effort expectancy (EE), (3) Perceived enjoyment (PEnjoy), (4) Facilitating conditions (FC), (5) Social influences (SI), (6) User Attitudes (UA), and (7) Behavioral Intentions (BI). Each dimension consisted of four questions, with 28 questions in total. The survey questions were scored using the 7-point Likert scale (from strongly disagree = 1 to strongly agree = 7).
3.3. Research Hypothesis
According to UTAUT Model, the following hypotheses was proposed (see Table 1).

Table 1.
Dimensions and hypotheses of the elderly’s acceptance.
4. Results
4.1. Early Stage Semi-Structured Interviews
As shown in Table 2, after conducting interviews with 10 participants, most had a positive attitude towards social VR. Regarding question 1, “Do you think social VR would be helpful in your life in the future?” The answer was mainly based on the needs of life. For example, one participant mentioned that he likes to ride heavy locomotives, and social VR can provide a group experience that he felt was “quite interesting,” with clear social benefits. In addition, participants also mentioned that the regular tracking of family doctors through social VR can greatly improve the medical “assistance” of daily life. In addition, due to the reduced opportunities of outdoor activities for the elderly, the possibility of “chatting” with peers or others via social VR can help ease loneliness. According to the interview records, keywords such as “quite interesting,” “assistance,” “chatting,” and “family doctors” were extracted. The involved dimensions including PEnjoy, PE, and FC were summarized, and key factors including entertainment, chatting, medical treatment, and shopping were extracted. These were subsequently used as the corresponding variables of the dimensions for the second stage.
Table 2.
Interview topic and main responses.
Regarding the question “Social VR would be mature in the future, would you like to use it?” most participants expressed a positive attitude and willingness to use it, but at the same time considered other limiting factors, including personal and technical factors. The participants confirmed that the technology must be convenient and abundant in content for them to purchase it. Another participant mentioned that he was exposed to these technologies as people around him are frequently using them. According to the second question interview record, the extracted keywords were “acceptable,” “capable of using it,” “convenient,” and “people around are using it.” The dimensions involved in UA, SI, EE, and BI were then summarized to provide an important reference for the questionnaire in the next stage.
4.2. Questionnaire Results
4.2.1. Participants
As shown in Table 3, we collected 114 valid questionnaires from 79 women (69.3%) and 35 men (30.7%). Amongst them, 37% were 65–69 years old and 32.5% were 70–74 years old. In terms of education level, 78 were educated to university or junior college level, accounting for 68.4% of the cohort. In terms of living conditions, the majority (50.9%) lived with family members (referring to living with children or living with a spouse and children), whilst only 12.3% lived alone or lived in a nursing institution. Regarding the use of virtual social tools, the survey was verified using the chi-square goodness-of-fit test to show statistical significance (p = 0.000 < 0.05). The social application most frequently used by the elderly was consistent amongst 94 participants (37.8%), which was significantly higher than all others. A total of 61 participants used Facebook (24.5%), which amongst the service items was considered by the elderly to be comparatively important. The chi-square goodness-of-fit test confirmed statistical significance within the survey (p = 0.000 < 0.05). The most prominent category was entertainment followed by medical treatment, which consisted of 92 (32.4%) and 89 participants (31.3%), respectively.
Table 3.
Demographic of the participants.
4.2.2. Descriptive Statistical Analysis of the Research Dimensions
As shown in Table 4, the Cronbach’s α was used to test the reliability of the self-compiled questionnaire. SPSS 22.0 (IBM, Armonk, N.Y., USA) statistics showed that the reliability coefficients of all variables were higher than 0.7, indicating that the questionnaire showed high reliability. The averages of all dimensions were above 4.6 points (4 = normal), and the averages of PE, PEnjoy, UA, and BI were above 5 points (1–7 points; 7 means strongly agree), indicating the elderly’s acceptance of social VR was positive.
Table 4.
Descriptive statistical analysis of the research dimensions (N = 114).
PE: more than 73% of the elderly believed that medical treatment, entertainment, and chatting functions were helpful to their lives, compared to less than 14% that believed that the applications were useless. Of the participants, less than 20% believed that the shopping function held no value.
EE: more than 60% of the elderly believed that the medical treatment, entertainment, and chatting functions were easy to learn and use, compared to ~23% that found them difficult. In total, 58.7% of the elderly believed that the shopping function was easy to learn and use, whilst ~30% found it challenging.
PEnjoy: approximately 70.3% of the urban elderly thought that the entertainment experience on social VR was interesting, whilst only 15.8% believed it was boring. In total, 62.3% of the elderly thought that the shopping experience was interesting, whilst nearly 20% of the elderly thought it was boring.
FC: more than 60% of the elderly cited the convenience of using social VR (support from family and friends), compared to less than 20% with little-to-no support. In total, 58.8% of the elderly had the knowledge and ability to use social VR, whilst 28.9% lacked the required skillsets. Of the participants, 51.7% had the time and funds to use social VR, whilst over 30% of the elderly did not.
SI: more than 70% of the elderly considered using medical treatment and chatting functions when recommended by a doctor or family member, compared to 16.6% who would not. Approximately 62% of the participants considered using the shopping function when recommended by a friend or important person, but more than 20% declined its use.
UA: more than 70% of the participants thought that medical treatment, entertainment, and chatting functions were worth using. In total, 17.5% (medical treatment), 9.7% (entertainment), and 11.4% (chatting) of the elderly disagreed. Of the participants, 62.3% thought that the shopping function was worth using, compared to 21.9% who disagreed.
BI: more than 70% of the elderly expressed their willingness to use medical treatment, entertainment, and chatting functions in the future. Of the participants, 15.8% (medical treatment), 10.6% (entertainment), and 14% (chatting) expressed their reluctance. In total, 62.3% expressed a willingness to use the shopping function, while 24.5% were unwilling.
4.2.3. Urban Elderly Acceptance Models of Social VR
As shown in Table 5, forced regression analysis showed that PE (p = 0.004 < 0.05), PEnjoy (p = 0.000 < 0.05) and SI (p = 0.000 < 0.05) had a significant positive correlation with UA, whilst SI (β= 0.421) had the greatest impact on UA. SI (p = 0.000 < 0.05) and UA (p = 0.000 < 0.05) also had significant positive effects on BI. However, EE (p = 0.071 > 0.05) and FC (p = 0.348 > 0.05) had no significant effect on UA.
Table 5.
Regression analysis between the research dimensions.
According to regression analysis, PE was verified in the preliminary theoretical hypothesis to positively affect UA (H1). PEnjoy positively affected UA (H3), SI positively affected UA (H5), SI positively affected BI (H6), and UA positively affected BI (H7). The revised model removed EE and FC dimensions, which did not significantly influence UA. The revised model is shown in Figure 3.
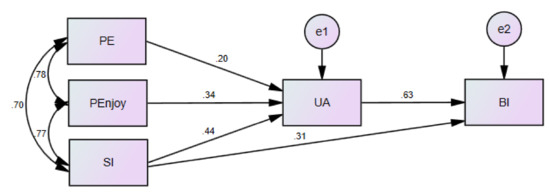
Figure 3.
Unified Theory of Acceptance and Use of Technology (UTAUT) Model of the virtual reality community application for the urban elderly.
5. Discussion
Through the comprehensive consideration of variable factors, we found that most elderly individuals accept social VR but still have concerns. We found that elderly participants were concerned about the stability, security, and reliability of the payment system when using the shopping function [49], and they are particularly sensitive to privacy and property security issues such as information leakage. Secondly, the elderly have long been accustomed to traditional consumption patterns. They believe that physical stores are more credible, and that the urban infrastructure is well-equipped and shopping in physical stores is convenient. In addition, whether the 3D virtual avatar (virtual agent role) can effectively map the users’ actual gestures and facial expressions in real time was raised as a concern.
The elderly participants assessed showed a deep interest in the medical service function. Considering that although the urban structure contains a relatively well-developed medical service system, some shortcomings exist, including time consumption of the patients waiting in line for treatments, or problems with patients returning to the hospital on multiple occasions for treatments, particularly for those with limited physical mobility. The medical service function of social VR can solve these issues and assist the hospital service system. Elderly individuals had fewer concerns in terms of entertainment and chatting functions, which may be related to the experience of using virtual technology, coupled with the limited recreational venues in urban areas. Social VR can however provide users with a large enough space. It was also noteworthy that the elderly’s need to chat is not limited to verbal communication. Social VR can support social behaviors in life activities (such as shopping and entertainment), which is more attractive to the elderly.
From the analysis of the technology acceptance model, SI, PEnjoy, and PE were important indicators that affected the elderly’s acceptance of social VR. We found that for SI, when the individual lacks experience, the social influence on the acceptance of the elderly becomes more important [50]. The decision of the elderly to use social VR is largely determined by surrounding factors such as family, friends, and doctors. During the questionnaire, it was also found that the elderly were susceptible to the influence of their peers to decide whether to take the questionnaire. As such, a one-to-one questionnaire is more authentic and effective. Additionally, most participants mentioned that strong and close ties were important. If friends around them failed to agree with the use of social VR, then they lacked a willingness to use it. This means that encouraging the elderly to use social VR should consider other social groups, social circles, and whether old acquaintances use the platform. These results are consistent with previous studies [51] that showed that social influence is an important factor affecting attitudes and behavioral intentions.
PEnjoy: We increased the explanatory power of the model from 76.7% to 79.6% through the addition of PEnjoy dimensions, indicating that the elderly regard enjoyment as an important factor [52], and that technical staff should consider PEnjoy as an important indicator when developing VR applications [27,53].
PE: although the weight of PE was relatively small, it had a significant impact on the user’s attitude of the elderly [54], which was consistent with Davis et al. [55] and subsequent research on the acceptance of technology. This shows that activities which are helpful to daily life and hobbies will encourage the use of social VR [56]. As such, the future social VR service system must be conceived to meet some functional requirements, including ensuring the safety and trust in social VR [57]. A significant positive correlation was also observed between UA and BI, consistent with previous studies on the technology acceptance model [54]. Although the participants considered that the current hardware was not light enough and that the database was not abundant, they thought that social VR represented the future trend, and that the technology will improve in the future. They were therefore willing to accept and consider its use in the future.
No significant influence of EE, FC, and UA were observed, which differed to the positive influence of EE and FC on technology acceptance reported in previous studies. We found that EE does not significantly impact on UA, as it may require participants to experience social VR in person to accurately explain its difficulty of use. Secondly, most participants believed that if social VR was useful to them, they would try to learn how to use it. Moreover, the vast majority of elderly individuals have experience in technology products and social applications, so the focus on usability does not represent a decisive factor when selecting social VR. In addition, King et al. found that in the technology acceptance model, usability was less predictive of use intention than usefulness [58]. Further studies are now required to investigate whether EE can affect the use attitude of the elderly.
FC also had no significant effect on the acceptance of the elderly, which is consistent with the results of Pal et al. [59] and Hoque et al. [60]. This may be because social VR represents a relatively new method of socializing, and it is not widely used at present. Participants are therefore still unable to realize the convenience of resources such as a fast internet connection, and the assistance from relatives and friends on the impact on the use of social VR. The elderly also rely less on technology in daily life [61].
Feedback from participants of elderly people is described below.
The correlation factor analysis and suggestions are made in the results of the UTAUT Model demand structure questionnaire and the synchronous interview, and the data showed that the application of entertainment and medical needs in social VR content was helpful to social interaction. Moreover, the degree of closeness of social relations and the distance of places also affects the state of social participation (β = 0.77, p = 0.000 < 0.05).
This study further points out that in the future, social VR can support the social behavior training essential in the activities of the elderly through entertainment, even the improvement schemes of rehabilitation. And the service of social VR can extend to the possibility of remote rehabilitation and treatment, such as tele-rehabilitation visits through social VR, or combination with the needs of shopping and entertainment, and to a certain extent, increasing the motivation interest of the elderly in rehabilitation and socializing. And it can also slow down the cognitive deterioration of the elderly, because these behaviors and activities can unremittingly stimulate the judgment and life management ability of the elderly.
In the application of social VR, nostalgic therapy can be implemented as well; the visual and interactive action and other sensory familiarity are prone to stimulate the elderly’s rich associations and memories, thereby enhancing the social will, which is beneficial to the physical and mental health of the elderly with or without cognitive impairment. Moreover, it can give full play to the social VR scene’s plasticity.
In addition, more elderly say that physical behaviors tend to be inept, but in social VR, somatosensory sports can be included in social activities, because the status of social VR changes, the elderly can even engage in more activities that are favored by young people, such as rock climbing or canoeing. For them, these activities cannot be achieved in real life, but while experiencing social VR, it can be accessible despite their physiological deterioration, and thus indirectly promote the social interaction between the elderly and different age groups.
Some findings mentioned above suggest that the elderly’s expectation of social VR is to reduce social disorders they experience out of mental or physical decline. These social disorders concern the lower frequency of participation due to physical inactivity, the less likelihood of outdoor activities due to social isolation caused by distance, or less chances that they will participate in the community due to physical diseases or cognitive decline. As described in the paper, social VR can help the elderly master these abilities by linking different functions, reduce social barriers caused by external factors, and at the same time help them socialize in a positive way. To some extent, social VR will help improve social isolation and loneliness among the elderly, and simultaneously alleviate their problems caused by cognitive impairment or physical inconveniences.
The contribution of this study is to identify the issues and service structures that may be emphasized in the use of social VR in the elderly population over the next 10–15 years. Such products are not yet available at this stage, and most of them are designed for younger populations. Therefore, the discussion combining social VR in the elderly population is more innovative and distinctive. And in the social VR used by the elderly, medical services and social entertainment is a representative service structure. Based on this, the design interface under this demand and the service type on the social VR have become the focus of discussion, and the purpose of this paper is mainly to provide guidance on this information, so that further researchers can continue to develop and conduct social VR application.
6. Research Limitations
Some limitations of the study should be noted. Firstly, the participants’ understanding of social VR was affected by existing VR technology, and they had not used social VR for a prolonged time period. Secondly, the majority of the elderly participants were from Taiwan and those based in other geographical locations should be assessed to improve the scope of the study. Thirdly, the subjects were healthy elderly individuals and those with limited physical mobility should also be assessed. Finally, the main contribution of this paper is to point out the trend of virtual social activities of the future elderly. The data showed that the elderly had obvious preference for entertainment (32.4%) and medical treatment (31.3%). There will be an increase in each other’s sensitivity to social VR. However, at this stage, as a preliminary study, or the beginning of study and the current state of use of the elderly, we have not yet launched a large-scale experimental design and system development to be applied to the real experience of the elderly. But as a tentative study, this paper has its own valuable contents, and it is urgent to make the relevant researchers know this message.
Furthermore, in the study of this age range, the elements of medical rehabilitation and entertainment account for a significant proportion and have a relative effect on the data indicators made by this study, but this element is still one of the keys to be explored and guided, and in order to gain a better understanding of the impact conditions brought about by these structures, we also conducted interviews with 114 elderly aged 60–89 who lived in urban areas of Taipei, and the results of these interviews led to evidence responses related to the structure. The content of the interviews will be presented in a qualitative manner, and these will be the discussion orientation of our interviews with the elderly, which are quite relevant and critical to the use of social VR by the elderly. So we’ll put them into future study and future service system development.
In the future, we will focus on the development of social VR in medical and entertainment service. The virtual social interface will be designed with social characteristics according to the preferences and characteristics of the elderly. Hopefully, the elderly can use the language and non-language combined multi-sensory social ways to promote positive social interaction in a relatively comfortable and safe environment, especially interacting with friends and relatives, thus to help solve their social loneliness and isolation. In addition, we can develop teleconference, social games, group recall, and other systems for social VR in the future to alleviate cognitive decline of the elderly.
7. Conclusions
The main purpose of this study is to explore the structure of social VR in the elderly in the metropolitan areas, and to discuss the results of interviews with 114 elderly aged 60–89 who lived in urban areas of Taipei. Based on the feedback of these structures and the interview of the elderly, UTAUT Model was also used to conduct structured questionnaires and make some relevant conclusions and suggestions.
The final results showed that the structural factors in entertainment and medical treatment were relatively significant, which was related to the demands of specific age. But these structures also showed the eagerness of the elderly for social needs. And in the next 10–15 years, these elderly people will be more likely to utilize social VR. The elderly in the study identified the following characteristics’ recommendations for the development of social VR and the contributions of this study.
- (1)
- The social VR solves the social constraints and self-esteem issues among the elderly.
As for the elderly, there are many sports that they do not dare to try in the past or cannot participate in because of physiological state constraints, but all of them can be achieved through the social VR. The social VR helps break through physical limits; such outdoor activities as rock climbing, tracing the river, and canoeing can be achieved through virtual environment.
In the past, the elderly tended to be less likely to engage in activities because of physiological states or physical conditions, or because of their self-esteem for fear of troubling others. However, the use of social VR today breaks these limits or eliminates worries and gives them the confidence to participate in different social activities. This finding echoes UTAUT Model’s performance on recreational and medical treatment issues, which represent that entertainment and medical susceptibility to the elderly mainly show in how they overcome their physiological state and self-esteem issues to participate in more recreations.
- (2)
- The social VR clears the hindrance of social restriction and interaction caused by spatial distance.
Because of COVID-19, or the lifestyle of the elderly in urban areas, the elderly were forced to cancel the activities for their physical conditions or long distances. For example, their friends lived too far away, or it was inconvenient for them to travel to the place where the activities are held. Even the lack of face-to-face interaction with others as a result of the epidemic can lead to social alienation and estrangement. However, the application of social VR can solve this problem and construct a social interaction state in another virtual space environment, and such an application can also remove the elderly’s problem of space and distance barrier.
This finding was also related to the closeness of the UTAUT Model in social relationships, and such factors may also affect the influence index of the elderly on Perceived Enjoyment, indicating that besides the intimacy of social friends, the influence factor of distance is also one of the opportunities for social VR to develop and highlight its edge. For such, social VR services are indeed an opportunity to address this gap.
- (3)
- The social VR needs to take into account the relationship between different needs and properly arrange the social context and interface design.
In different demands, plenty of related factors are highlighted in social VR. In respect of the life situation and interface design, it needs to be configured in accordance with the conditions required in these states, such as the relevance between medical structure and entertainment structure. How to arrange in the specific situation and shown in the interface design, and present proper scheme design, and in the interface information and operation? How to help the elderly quickly find the appropriate operation plan and the corresponding use state? All of these have become the focus of not only social situation designed by the social VR for the elderly but also the interface design.
- (4)
- In the future hardware interface design, more consideration should be given to social VR in its convenience the possibility of service needs.
The social VR still uses HMD as carrier and tool at this stage, but in the future, different hardware design and software collocation will become possible to create new state service, like the fitting combination of scarf and hat. It may become the hardware modeling of future social VR, and in the future service, these need to be comfortable and sensitive enough for the elderly given their degraded and weakened sensory. And how social VR designs according to their physiological perception needs will become one of the key factors to decide whether the product can be accepted by the elderly.
- (5)
- The social VR will still require interaction with the physical world to provide diversified services.
In the end, although social VR provides more possibilities in a virtual immersive environment, the link to the real world is still the focus that must be considered. How to achieve and better the link between the virtual and the real world by social VR will be the focus to be considered by the future elderly or the social VR. Whether long-distance virtual medical treatment and rehabilitation can be carried out in an immersive environment, or whether further treatment can be carried out in a home environment or in a nearby hospital. After all, physical medical behavior in some conditions or technology has not been overcome, physical conditions and medical behavior are the inevitable activities, and in addition, social VR will have more possibilities and challenges, and these contents need to be considered to strengthen the services of virtual environment and physical state.
Supplementary Materials
The following are available online at https://www.mdpi.com/2071-1050/12/22/9345/s1, Questionnaire.
Author Contributions
All authors contributed to the paper. Conceptualization, D.S. and I-J.L.; methodology, D.S. and I-J.L.; software, D.S.; writing—original draft preparation, D.S.; writing—review and editing, I-J.L.; supervision, I-J.L. All authors read and agreed to the published version of the manuscript.
Funding
This research was funded by Fujian Social Science Planning Project, grant number FJ2018C083.
Acknowledgments
The authors thank Zhenzeng Wu for the helpful conversations and constructive comments during the writing process.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Miori, V.; Russo, D. Improving life quality for the elderly through the Social Internet of Things (SIoT). In Proceedings of the 2017 Global Internet of Things Summit (GIoTS), Geneva, Switzerland, 6–9 June 2017; IEEE Press: Piscataway, NJ, USA, 2017; pp. 1–6. [Google Scholar] [CrossRef]
- Courtin, E.; Knapp, M. Social isolation, loneliness and health in old age: A scoping review. Health Soc. Care Community 2017, 25, 799–812. [Google Scholar] [CrossRef]
- Bekhet, A.K.; Zauszniewski, J.A. Mental health of elders in retirement communities: Is loneliness a key factor? Arch. Psychiat. Nurs. 2012, 26, 214–224. [Google Scholar] [CrossRef] [PubMed]
- Segel-Karpas, D.; Ayalon, L.; Lachman, M.E. Loneliness and depressive symptoms: The moderating role of the transition into retirement. Aging Ment. Health 2018, 22, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Gray, A.; Worlledge, G. Addressing loneliness and isolation in retirement housing. Ageing Soc. 2018, 38, 615–664. [Google Scholar] [CrossRef]
- Yang, K.; Victor, C. Age and loneliness in 25 European nations. Ageing Soc. 2011, 31, 1368–1388. [Google Scholar] [CrossRef]
- Zhou, G.; Wang, Y.; Yu, X. Direct and Indirect Effects of Family Functioning on Loneliness of Elderly Chinese Individuals. Curr. Psychol. 2016, 37, 1–7. [Google Scholar] [CrossRef]
- Carver, L.F.; Beamish, R.; Phillips, S.P.; Villeneuve, M. A Scoping Review: Social Participation as a Cornerstone of Successful Aging in Place among Rural Older Adults. Geriatrics 2018, 3, 75. [Google Scholar] [CrossRef]
- Herzog, A.R.; Ofstedal, M.B.; Wheeler, L. Social Engagement and Its Relationship to Health. Clin. Geriatr. Med. 2002, 18, 593–609. [Google Scholar] [CrossRef]
- Khosravi, P.; Rezvani, A.; Wiewiora, A. The impact of technology on older adults’ social isolation. Comput. Hum. Behav. 2016, 63, 594–603. [Google Scholar] [CrossRef]
- Baecker, R.M.; Moffatt, K.; Massimi, M. Technologies for aging gracefully. Interactions 2012, 19, 32–36. [Google Scholar] [CrossRef]
- Hagan, R.; Manktelow, R.; Taylor, B.J.; Mallett, J. Reducing loneliness amongst older people: A systematic search and narrative review. Aging Ment. Health 2014, 18, 683–693. [Google Scholar] [CrossRef] [PubMed]
- Bahramnezhad, F.; Chalik, R.; Bastani, F.; Taherpour, M.; Navab, E. The social network among the elderly and its relationship with quality of life. Electron. Physician 2017, 9, 4306–4311. [Google Scholar] [CrossRef] [PubMed]
- Klimova, B. Social Network Sites and Older Generation. In Applied Physics, System Science and Computers, 3rd ed.; Ntalianis, K., Vachtsevanos, G., Borne, P., Croitoru, A., Eds.; Springer International Publishing: Cham, Switzerland, 27 June 2019; pp. 99–104. [Google Scholar] [CrossRef]
- Ha, T.V.; Hoang, D.B. An assistive healthcare platform for both social and service networking for engaging elderly people. In Proceedings of the 2017 23rd Asia-Pacific Conference on Communications (APCC), Perth, Australia, 11–13 December 2017; pp. 1–6. [Google Scholar] [CrossRef]
- van Ingen, E.; Rains, S.A.; Wright, K.B. Does social network site use buffer against well-being loss when older adults face reduced functional ability? Comput. Hum. Behav. 2017, 70, 168–177. [Google Scholar] [CrossRef]
- Quinn, D.; Chen, L.; Mulvenna, M.; Bond, R. Exploring the Relationship Between Online Social Network Site Usage and the Impact on Quality of Life for Older and Younger Users: An Interaction Analysis. J. Med. Internet Res. 2016, 18, e245. [Google Scholar] [CrossRef]
- Domènech-Abella, J.; Lara, E.; Rubio-Valera, M.; Olaya, B.; Moneta, M.V.; Rico-Uribe, L.A.; Ayuso-Mateos, J.L.; Mundó, J.; Haro, J.M. Loneliness and depression in the elderly: The role of social network. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 381–390. [Google Scholar] [CrossRef]
- Domènech-Abella, J.; Mundó, J.; Haro, J.M.; Rubio-Valera, M. Anxiety, depression, loneliness and social network in the elderly: Longitudinal associations from The Irish Longitudinal Study on Ageing (TILDA). J. Affect. Disord. 2019, 246, 82–88. [Google Scholar] [CrossRef]
- Holmén, K.; Furukawa, H. Loneliness, health and social network among elderly people—A follow-up study. Arch. Gerontol. Geriat. 2002, 35, 261–274. [Google Scholar] [CrossRef]
- Ali, T.; Nilsson, C.J.; Weuve, J.; Rajan, K.B.; Mendes de Leon, C.F. Effects of social network diversity on mortality, cognition and physical function in the elderly: A longitudinal analysis of the Chicago Health and Aging Project (CHAP). J. Epidemiol. Commun. Health 2018, 72, 990–996. [Google Scholar] [CrossRef]
- Bianchetti, L.; Squazzoni, F.; Casnici, N.; Bianchini, D.; Garrafa, E.; Archetti, C.; Romano, V.; Rozzini, L.; Melchiori, M.; Fiorentini, C.; et al. Social networks and health status in the elderly: The ‘ANZIANI IN-RETE’ population-based study. Aging Clin. Exp. Res. 2017, 29, 1173–1179. [Google Scholar] [CrossRef]
- Gunkel, S.N.B.; Prins, M.; Stokking, H.; Niamut, O. Social VR Platform: Building 360-degree Shared VR Spaces. In Adjunct Publication of the 2017 ACM International Conference on Interactive Experiences for TV and Online Video; Association for Computing Machinery: Hilversum, The Netherlands, 2017; pp. 83–84. [Google Scholar] [CrossRef]
- Lin, C.X.; Lee, C.; Lally, D.; Coughlin, J.F. Impact of Virtual Reality (VR) Experience on Older Adults’ Well-Being. In Human Aspects of IT for the Aged Population. Applications in Health, Assistance, and Entertainment; Zhou, J., Salvendy, G., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 89–100. [Google Scholar] [CrossRef]
- Johnson, C.S.; McLeod, K.M. Relationship between Fear of Falling and Preceived Difficulty with Grocery Shopping. J. Frailty Aging 2016, 6, 33–36. [Google Scholar] [CrossRef]
- tom Dieck, M.C.; Jung, T.; Michopoulou, E. Experiencing Virtual Reality in Heritage Attractions: Perceptions of Elderly Users. In Augmented Reality and Virtual Reality: The Power of AR and VR for Business; tom Dieck, M.C., Jung, T., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 89–98. [Google Scholar] [CrossRef]
- Syed-Abdul, S.; Malwade, S.; Nursetyo, A.A.; Sood, M.; Bhatia, M.; Barsasella, D.; Liu, M.F.; Chang, C.-C.; Srinivasan, K.; Raja, M.; et al. Virtual reality among the elderly: A usefulness and acceptance study from Taiwan. BMC Geriatr. 2019, 19, 223. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A.R.; De Schutter, B.; Franks, K.; Radina, M.E. Older Adults’ Experiences with Audiovisual Virtual Reality: Perceived Usefulness and Other Factors Influencing Technology Acceptance. Clin. Gerontol. 2019, 42, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Jeng, M.-Y.; Pai, F.-Y.; Yeh, T.-M. The virtual reality leisure activities experience on elderly people. Appl. Res. Qual. Life 2017, 12, 49–65. [Google Scholar] [CrossRef]
- Lin, C.-S.; Jeng, M.-Y.; Yeh, T.-M. The Elderly Perceived Meanings and Values of Virtual Reality Leisure Activities: A Means-End Chain Approach. Int. J. Environ. Res. Public Health 2018, 15, 663. [Google Scholar] [CrossRef]
- Gunkel, S.; Stokking, H.; Prins, M.; Niamut, O.; Siahaan, E.; Cesar, P. Experiencing Virtual Reality Together: Social VR Use Case Study. In Proceedings of the 2018 ACM International Conference on Interactive Experiences for TV and Online Video, Seoul, Korea, 26–28 June 2018; Association for Computing Machinery: New York, NY, USA, 2018; pp. 233–238. [Google Scholar] [CrossRef]
- Zhang, L.; Sun, L.; Wang, W.; Liu, J. Unlocking the Door to Mobile Social VR: Architecture, Experiments and Challenges. IEEE Netw. 2018, 32, 160–165. [Google Scholar] [CrossRef]
- Baker, S.; Waycott, J.; Carrasco, R.; Hoang, T.; Vetere, F. Exploring the Design of Social VR Experiences with Older Adults. In Proceedings of the 2019 on Designing Interactive Systems Conference, San Diego, CA, USA, 23–28 June 2019; Association for Computing Machinery: New York, NY, USA, 2019; pp. 303–315. [Google Scholar] [CrossRef]
- Heidicker, P.; Langbehn, E.; Steinicke, F. Influence of avatar appearance on presence in social VR. In Proceedings of the 2017 IEEE Symposium on 3D User Interfaces (3DUI), Los Angeles, CA, USA, 18–19 March 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 233–234. [Google Scholar] [CrossRef]
- Li, J.; Kong, Y.; Röggla, T.; Simone, F.D.; Ananthanarayan, S.; Ridder, H.d.; Ali, A.E.; Cesar, P. Measuring and Understanding Photo Sharing Experiences in Social Virtual Reality. In Proceedings of the 2019 CHI Conference on Human Factors in Computing Systems, Glasgow, UK, 4–9 May 2019; Association for Computing Machinery: New York, NY, USA, 2019; p. 667. [Google Scholar] [CrossRef]
- Baker, S.; Kelly, R.M.; Waycott, J.; Carrasco, R.; Hoang, T.; Batchelor, F.; Ozanne, E.; Dow, B.; Warburton, J.; Vetere, F. Interrogating Social Virtual Reality as a Communication Medium for Older Adults. Proc. ACM Hum.-Comput. Interact. 2019, 3, 149. [Google Scholar] [CrossRef]
- Yu, R.; Hui, E.; Lee, J.; Poon, D.; Ng, A.; Sit, K.; Ip, K.; Yeung, F.; Wong, M.; Shibata, T.; et al. Use of a Therapeutic, Socially Assistive Pet Robot (PARO) in Improving Mood and Stimulating Social Interaction and Communication for People with Dementia: Study Protocol for a Randomized Controlled Trial. JMIR Res. Protoc. 2015, 4, e45. [Google Scholar] [CrossRef]
- Li, S.; Yu, F.; Peng, K. Effect of State Loneliness on Robot Anthropomorphism: Potential Edge of Social Robots Compared to Common Nonhumans. J. Phys. Conf. Ser. 2020, 1631, 012024. [Google Scholar] [CrossRef]
- Hudson, J.; Ungar, R.; Albright, L.; Tkatch, R.; Schaeffer, J.; Wicker, E.R. Robotic Pet Use Among Community-Dwelling Older Adults. J. Gerontol. Ser. B 2020, 75, 2018–2028. [Google Scholar] [CrossRef]
- Reed, D.J.; Fitzpatrick, G. Acting Your Age in Second Life. In Proceedings of the International Conference on Fun and Games, Eindhoven, The Netherlands, 20–21 October 2008; Springer: Berlin/Heidelberg, Germany, 2008; pp. 158–169. [Google Scholar] [CrossRef]
- Korsgaard, D.; Bjørner, T.; Sørensen, P.K.; Bruun-Pedersen, J.R. Older adults eating together in a virtual living room: Opportunities and limitations of eating in augmented virtuality. In Proceedings of the 31st European Conference on Cognitive Ergonomics, Belfast, UK, 10–13 September 2019; Association for Computing Machinery: New York, NY, USA, 2019; pp. 168–176. [Google Scholar] [CrossRef]
- Zamanifard, S.; Freeman, G. “The Togetherness that We Crave”: Experiencing Social VR in Long Distance Relationships. In Proceedings of the Conference Companion Publication of the 2019 on Computer Supported Cooperative Work and Social Computing, Austin, TX, USA, 9–13 November 2019; Association for Computing Machinery: New York, NY, USA, 2019; pp. 438–442. [Google Scholar] [CrossRef]
- Pedro, A.; Le, Q.T.; Park, C.S. Framework for Integrating Safety into Construction Methods Education through Interactive Virtual Reality. J. Prof. Issues Eng. Educ. Pract. 2016, 142, 04015011. [Google Scholar] [CrossRef]
- Welcome to Facebook Horizon. Available online: https://www.youtube.com/watch?v=Is8eXZco46Q (accessed on 25 September 2019).
- Im, I.; Hong, S.; Kang, M.S. An international comparison of technology adoption: Testing the UTAUT model. Inform. Manag. 2011, 48, 1–8. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User Acceptance of Information Technology: Toward a Unified View. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef]
- Huang, T.; Huang, C. Elderly’s acceptance of companion robots from the perspective of user factors. Univ. Access Inf. Soc. 2020, 19, 935–948. [Google Scholar] [CrossRef]
- Petersen, F.; Jacobs, M.; Pather, S. Barriers for User Acceptance of Mobile Health Applications for Diabetic Patients: Applying the UTAUT Model. In Proceedings of the Conference on e-Business, e-Services and e-Society, Skukuza, South Africa, 6–8 April 2020; Springer International Publishing: Berlin/Heidelberg, Germany, 2020; pp. 61–72. [Google Scholar] [CrossRef]
- Ruangkana, V.; Kessuvan, A. Factors Affecting the Elderly’s Adoption of Online Purchasing. In Proceedings of the 2019 International Conference on Engineering, Science, and Industrial Applications (ICESI), Tokyo, Japan, 22–24 August 2019; pp. 1–5. [Google Scholar] [CrossRef]
- AlAwadhi, S.; Morris, A. In The Use of the UTAUT Model in the Adoption of E-Government Services in Kuwait. In Proceedings of the the 41st Hawaii International International Conference on Systems Science (HICSS-41 2008), Waikoloa, HI, USA, 7–10 January 2008; IEEE Computer Society: Piscataway, NJ, USA, 2008; p. 219. [Google Scholar] [CrossRef]
- Briz-Ponce, L.; Pereira, A.; Carvalho, L.; Juanes-Méndez, J.A.; García-Peñalvo, F.J. Learning with mobile technologies–Students’ behavior. Comput. Hum. Behav. 2017, 72, 612–620. [Google Scholar] [CrossRef]
- Dogruel, L.; Joeckel, S.; Bowman, N.D. The use and acceptance of new media entertainment technology by elderly users: Development of an expanded technology acceptance model. Behav. Inform. Technol. 2015, 34, 1052–1063. [Google Scholar] [CrossRef]
- El Shamy, N.; Hassanein, K. A Meta-Analysis of Enjoyment Effect on Technology Acceptance: The Moderating Role of Technology Conventionality. In Proceedings of the 50th Hawaii International Conference on System Sciences, Hilton Waikoloa Village, HI, USA, 4–7 January 2017. [Google Scholar] [CrossRef]
- Guner, H.; Acarturk, C. The use and acceptance of ICT by senior citizens: A comparison of technology acceptance model (TAM) for elderly and young adults. Univ. Access Inf. Soc. 2020, 19, 311–330. [Google Scholar] [CrossRef]
- Davis, F.D. Perceived Usefulness, Perceived Ease of Use, and User Acceptance of Information Technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef]
- Weatherall, J.W.A. A Grounded Theory Analysis of Older Adults and Information Technology. Educ. Gerontol. 2000, 26, 371–386. [Google Scholar] [CrossRef]
- Li, R.; Chung, T.-L.; Fiore, A.M. Factors affecting current users’ attitude towards e-auctions in China: An extended TAM study. J. Retail. Consum. Serv. 2017, 34, 19–29. [Google Scholar] [CrossRef]
- King, W.R.; He, J. A meta-analysis of the technology acceptance model. Inform. Manag. 2006, 43, 740–755. [Google Scholar] [CrossRef]
- Pal, D.; Funilkul, S.; Charoenkitkarn, N.; Kanthamanon, P. Internet-of-Things and Smart Homes for Elderly Healthcare: An End User Perspective. IEEE Access 2018, 6, 10483–10496. [Google Scholar] [CrossRef]
- Hoque, R.; Sorwar, G. Understanding factors influencing the adoption of mHealth by the elderly: An extension of the UTAUT model. Int. J. Med. Inform. 2017, 101, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Coughlin, J.F. PERSPECTIVE: Older Adults’ Adoption of Technology: An Integrated Approach to Identifying Determinants and Barriers. J. Prod. Innov. Manag. 2015, 32, 747–759. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).