Acceptance and Influencing Factors of Social Virtual Reality in the Urban Elderly

Abstract
1. Introduction
1.1. The Living Problems and Social Needs of Urban Elderly
1.2. Social Networks and Applications Can Effectively Reduce Social Loneliness
1.3. Virtual Reality (VR) Technology Can Promote Social Networks within the Elderly Population
2. Related Works
2.1. Social Service Provided by VR Technology
2.2. Advantages of VR Technology in Social Development
2.3. Innovation and Contributions of this Study
2.4. Gaps in Previous Studies
- (1)
- (2)
- In addition, studies on the elderly centers on the design of the virtual avatar [36], with no comprehensive consideration of multiple dimensions and variable factors, and no guidance based on them.
- (3)
- This study aims at the elderly group in the metropolitan areas, which is also different from the broad elderly group targeted by previous studies. Since they are more familiar with technology and urban life, these urban elderly people are more likely to be the key customers of social VR investment over the next 10 years.
- (4)
- In the end, the related social VR is mostly aimed at using the screen as an interactive carrier or mobile games. To compensate for it, this study is mainly focused on the construction of social VR under remote service, which is mainly designed under the application of immersive VR devices according to the coherent service content and situational design, instead of a single game use or entertainment needs.
- (5)
- Previous studies have focused on the design of physical therapeutic products, such as the use of therapeutic sea dog robots to accompany the elderly and provide services of therapeutic interaction, but few studies have focused on the relationship between virtual and real world. In the framework of social VR, such studies have highlighted the particularities and uses of virtual situations, and activated the potential of services and study.
2.5. Summary
3. Methods
3.1. Participants
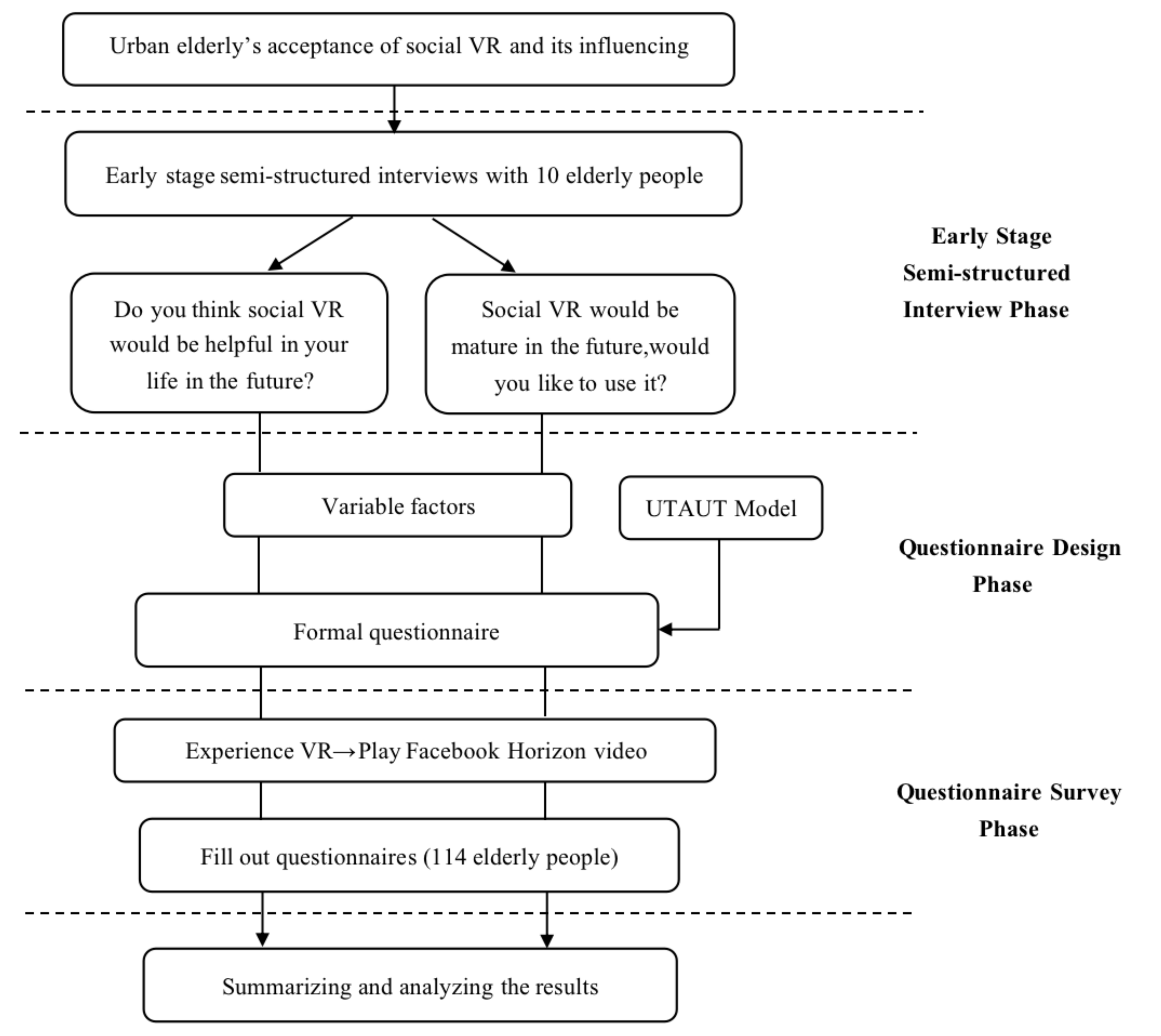
3.2. Procedure
3.2.1. Early Stage Semi-Structured Interviews
3.2.2. Questionnaire Design
3.3. Research Hypothesis
4. Results
4.1. Early Stage Semi-Structured Interviews
4.2. Questionnaire Results
4.2.1. Participants
4.2.2. Descriptive Statistical Analysis of the Research Dimensions
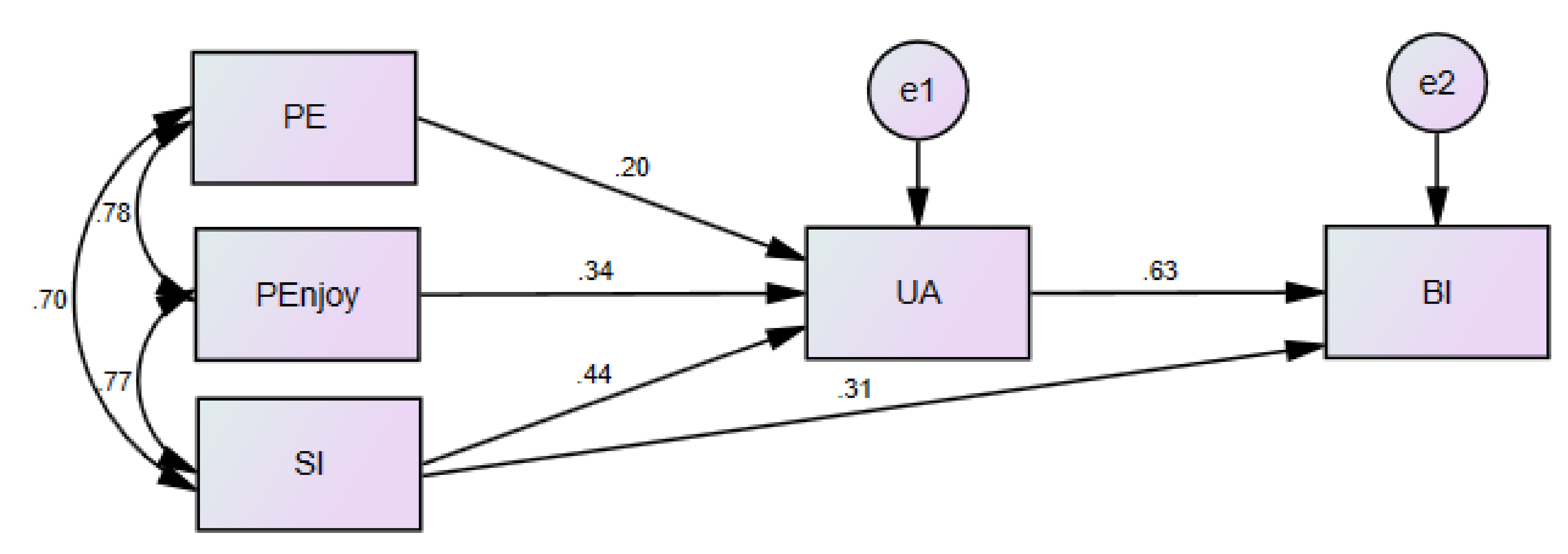
4.2.3. Urban Elderly Acceptance Models of Social VR
5. Discussion
6. Research Limitations
7. Conclusions
- (1)
- The social VR solves the social constraints and self-esteem issues among the elderly.
- (2)
- The social VR clears the hindrance of social restriction and interaction caused by spatial distance.
- (3)
- The social VR needs to take into account the relationship between different needs and properly arrange the social context and interface design.
- (4)
- In the future hardware interface design, more consideration should be given to social VR in its convenience the possibility of service needs.
- (5)
- The social VR will still require interaction with the physical world to provide diversified services.
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Miori, V.; Russo, D. Improving life quality for the elderly through the Social Internet of Things (SIoT). In Proceedings of the 2017 Global Internet of Things Summit (GIoTS), Geneva, Switzerland, 6–9 June 2017; IEEE Press: Piscataway, NJ, USA, 2017; pp. 1–6. [Google Scholar] [CrossRef]
- Courtin, E.; Knapp, M. Social isolation, loneliness and health in old age: A scoping review. Health Soc. Care Community 2017, 25, 799–812. [Google Scholar] [CrossRef]
- Bekhet, A.K.; Zauszniewski, J.A. Mental health of elders in retirement communities: Is loneliness a key factor? Arch. Psychiat. Nurs. 2012, 26, 214–224. [Google Scholar] [CrossRef] [PubMed]
- Segel-Karpas, D.; Ayalon, L.; Lachman, M.E. Loneliness and depressive symptoms: The moderating role of the transition into retirement. Aging Ment. Health 2018, 22, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Gray, A.; Worlledge, G. Addressing loneliness and isolation in retirement housing. Ageing Soc. 2018, 38, 615–664. [Google Scholar] [CrossRef]
- Yang, K.; Victor, C. Age and loneliness in 25 European nations. Ageing Soc. 2011, 31, 1368–1388. [Google Scholar] [CrossRef]
- Zhou, G.; Wang, Y.; Yu, X. Direct and Indirect Effects of Family Functioning on Loneliness of Elderly Chinese Individuals. Curr. Psychol. 2016, 37, 1–7. [Google Scholar] [CrossRef]
- Carver, L.F.; Beamish, R.; Phillips, S.P.; Villeneuve, M. A Scoping Review: Social Participation as a Cornerstone of Successful Aging in Place among Rural Older Adults. Geriatrics 2018, 3, 75. [Google Scholar] [CrossRef]
- Herzog, A.R.; Ofstedal, M.B.; Wheeler, L. Social Engagement and Its Relationship to Health. Clin. Geriatr. Med. 2002, 18, 593–609. [Google Scholar] [CrossRef]
- Khosravi, P.; Rezvani, A.; Wiewiora, A. The impact of technology on older adults’ social isolation. Comput. Hum. Behav. 2016, 63, 594–603. [Google Scholar] [CrossRef]
- Baecker, R.M.; Moffatt, K.; Massimi, M. Technologies for aging gracefully. Interactions 2012, 19, 32–36. [Google Scholar] [CrossRef]
- Hagan, R.; Manktelow, R.; Taylor, B.J.; Mallett, J. Reducing loneliness amongst older people: A systematic search and narrative review. Aging Ment. Health 2014, 18, 683–693. [Google Scholar] [CrossRef] [PubMed]
- Bahramnezhad, F.; Chalik, R.; Bastani, F.; Taherpour, M.; Navab, E. The social network among the elderly and its relationship with quality of life. Electron. Physician 2017, 9, 4306–4311. [Google Scholar] [CrossRef] [PubMed]
- Klimova, B. Social Network Sites and Older Generation. In Applied Physics, System Science and Computers, 3rd ed.; Ntalianis, K., Vachtsevanos, G., Borne, P., Croitoru, A., Eds.; Springer International Publishing: Cham, Switzerland, 27 June 2019; pp. 99–104. [Google Scholar] [CrossRef]
- Ha, T.V.; Hoang, D.B. An assistive healthcare platform for both social and service networking for engaging elderly people. In Proceedings of the 2017 23rd Asia-Pacific Conference on Communications (APCC), Perth, Australia, 11–13 December 2017; pp. 1–6. [Google Scholar] [CrossRef]
- van Ingen, E.; Rains, S.A.; Wright, K.B. Does social network site use buffer against well-being loss when older adults face reduced functional ability? Comput. Hum. Behav. 2017, 70, 168–177. [Google Scholar] [CrossRef]
- Quinn, D.; Chen, L.; Mulvenna, M.; Bond, R. Exploring the Relationship Between Online Social Network Site Usage and the Impact on Quality of Life for Older and Younger Users: An Interaction Analysis. J. Med. Internet Res. 2016, 18, e245. [Google Scholar] [CrossRef]
- Domènech-Abella, J.; Lara, E.; Rubio-Valera, M.; Olaya, B.; Moneta, M.V.; Rico-Uribe, L.A.; Ayuso-Mateos, J.L.; Mundó, J.; Haro, J.M. Loneliness and depression in the elderly: The role of social network. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 381–390. [Google Scholar] [CrossRef]
- Domènech-Abella, J.; Mundó, J.; Haro, J.M.; Rubio-Valera, M. Anxiety, depression, loneliness and social network in the elderly: Longitudinal associations from The Irish Longitudinal Study on Ageing (TILDA). J. Affect. Disord. 2019, 246, 82–88. [Google Scholar] [CrossRef]
- Holmén, K.; Furukawa, H. Loneliness, health and social network among elderly people—A follow-up study. Arch. Gerontol. Geriat. 2002, 35, 261–274. [Google Scholar] [CrossRef]
- Ali, T.; Nilsson, C.J.; Weuve, J.; Rajan, K.B.; Mendes de Leon, C.F. Effects of social network diversity on mortality, cognition and physical function in the elderly: A longitudinal analysis of the Chicago Health and Aging Project (CHAP). J. Epidemiol. Commun. Health 2018, 72, 990–996. [Google Scholar] [CrossRef]
- Bianchetti, L.; Squazzoni, F.; Casnici, N.; Bianchini, D.; Garrafa, E.; Archetti, C.; Romano, V.; Rozzini, L.; Melchiori, M.; Fiorentini, C.; et al. Social networks and health status in the elderly: The ‘ANZIANI IN-RETE’ population-based study. Aging Clin. Exp. Res. 2017, 29, 1173–1179. [Google Scholar] [CrossRef]
- Gunkel, S.N.B.; Prins, M.; Stokking, H.; Niamut, O. Social VR Platform: Building 360-degree Shared VR Spaces. In Adjunct Publication of the 2017 ACM International Conference on Interactive Experiences for TV and Online Video; Association for Computing Machinery: Hilversum, The Netherlands, 2017; pp. 83–84. [Google Scholar] [CrossRef]
- Lin, C.X.; Lee, C.; Lally, D.; Coughlin, J.F. Impact of Virtual Reality (VR) Experience on Older Adults’ Well-Being. In Human Aspects of IT for the Aged Population. Applications in Health, Assistance, and Entertainment; Zhou, J., Salvendy, G., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 89–100. [Google Scholar] [CrossRef]
- Johnson, C.S.; McLeod, K.M. Relationship between Fear of Falling and Preceived Difficulty with Grocery Shopping. J. Frailty Aging 2016, 6, 33–36. [Google Scholar] [CrossRef]
- tom Dieck, M.C.; Jung, T.; Michopoulou, E. Experiencing Virtual Reality in Heritage Attractions: Perceptions of Elderly Users. In Augmented Reality and Virtual Reality: The Power of AR and VR for Business; tom Dieck, M.C., Jung, T., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 89–98. [Google Scholar] [CrossRef]
- Syed-Abdul, S.; Malwade, S.; Nursetyo, A.A.; Sood, M.; Bhatia, M.; Barsasella, D.; Liu, M.F.; Chang, C.-C.; Srinivasan, K.; Raja, M.; et al. Virtual reality among the elderly: A usefulness and acceptance study from Taiwan. BMC Geriatr. 2019, 19, 223. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A.R.; De Schutter, B.; Franks, K.; Radina, M.E. Older Adults’ Experiences with Audiovisual Virtual Reality: Perceived Usefulness and Other Factors Influencing Technology Acceptance. Clin. Gerontol. 2019, 42, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Jeng, M.-Y.; Pai, F.-Y.; Yeh, T.-M. The virtual reality leisure activities experience on elderly people. Appl. Res. Qual. Life 2017, 12, 49–65. [Google Scholar] [CrossRef]
- Lin, C.-S.; Jeng, M.-Y.; Yeh, T.-M. The Elderly Perceived Meanings and Values of Virtual Reality Leisure Activities: A Means-End Chain Approach. Int. J. Environ. Res. Public Health 2018, 15, 663. [Google Scholar] [CrossRef]
- Gunkel, S.; Stokking, H.; Prins, M.; Niamut, O.; Siahaan, E.; Cesar, P. Experiencing Virtual Reality Together: Social VR Use Case Study. In Proceedings of the 2018 ACM International Conference on Interactive Experiences for TV and Online Video, Seoul, Korea, 26–28 June 2018; Association for Computing Machinery: New York, NY, USA, 2018; pp. 233–238. [Google Scholar] [CrossRef]
- Zhang, L.; Sun, L.; Wang, W.; Liu, J. Unlocking the Door to Mobile Social VR: Architecture, Experiments and Challenges. IEEE Netw. 2018, 32, 160–165. [Google Scholar] [CrossRef]
- Baker, S.; Waycott, J.; Carrasco, R.; Hoang, T.; Vetere, F. Exploring the Design of Social VR Experiences with Older Adults. In Proceedings of the 2019 on Designing Interactive Systems Conference, San Diego, CA, USA, 23–28 June 2019; Association for Computing Machinery: New York, NY, USA, 2019; pp. 303–315. [Google Scholar] [CrossRef]
- Heidicker, P.; Langbehn, E.; Steinicke, F. Influence of avatar appearance on presence in social VR. In Proceedings of the 2017 IEEE Symposium on 3D User Interfaces (3DUI), Los Angeles, CA, USA, 18–19 March 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 233–234. [Google Scholar] [CrossRef]
- Li, J.; Kong, Y.; Röggla, T.; Simone, F.D.; Ananthanarayan, S.; Ridder, H.d.; Ali, A.E.; Cesar, P. Measuring and Understanding Photo Sharing Experiences in Social Virtual Reality. In Proceedings of the 2019 CHI Conference on Human Factors in Computing Systems, Glasgow, UK, 4–9 May 2019; Association for Computing Machinery: New York, NY, USA, 2019; p. 667. [Google Scholar] [CrossRef]
- Baker, S.; Kelly, R.M.; Waycott, J.; Carrasco, R.; Hoang, T.; Batchelor, F.; Ozanne, E.; Dow, B.; Warburton, J.; Vetere, F. Interrogating Social Virtual Reality as a Communication Medium for Older Adults. Proc. ACM Hum.-Comput. Interact. 2019, 3, 149. [Google Scholar] [CrossRef]
- Yu, R.; Hui, E.; Lee, J.; Poon, D.; Ng, A.; Sit, K.; Ip, K.; Yeung, F.; Wong, M.; Shibata, T.; et al. Use of a Therapeutic, Socially Assistive Pet Robot (PARO) in Improving Mood and Stimulating Social Interaction and Communication for People with Dementia: Study Protocol for a Randomized Controlled Trial. JMIR Res. Protoc. 2015, 4, e45. [Google Scholar] [CrossRef]
- Li, S.; Yu, F.; Peng, K. Effect of State Loneliness on Robot Anthropomorphism: Potential Edge of Social Robots Compared to Common Nonhumans. J. Phys. Conf. Ser. 2020, 1631, 012024. [Google Scholar] [CrossRef]
- Hudson, J.; Ungar, R.; Albright, L.; Tkatch, R.; Schaeffer, J.; Wicker, E.R. Robotic Pet Use Among Community-Dwelling Older Adults. J. Gerontol. Ser. B 2020, 75, 2018–2028. [Google Scholar] [CrossRef]
- Reed, D.J.; Fitzpatrick, G. Acting Your Age in Second Life. In Proceedings of the International Conference on Fun and Games, Eindhoven, The Netherlands, 20–21 October 2008; Springer: Berlin/Heidelberg, Germany, 2008; pp. 158–169. [Google Scholar] [CrossRef]
- Korsgaard, D.; Bjørner, T.; Sørensen, P.K.; Bruun-Pedersen, J.R. Older adults eating together in a virtual living room: Opportunities and limitations of eating in augmented virtuality. In Proceedings of the 31st European Conference on Cognitive Ergonomics, Belfast, UK, 10–13 September 2019; Association for Computing Machinery: New York, NY, USA, 2019; pp. 168–176. [Google Scholar] [CrossRef]
- Zamanifard, S.; Freeman, G. “The Togetherness that We Crave”: Experiencing Social VR in Long Distance Relationships. In Proceedings of the Conference Companion Publication of the 2019 on Computer Supported Cooperative Work and Social Computing, Austin, TX, USA, 9–13 November 2019; Association for Computing Machinery: New York, NY, USA, 2019; pp. 438–442. [Google Scholar] [CrossRef]
- Pedro, A.; Le, Q.T.; Park, C.S. Framework for Integrating Safety into Construction Methods Education through Interactive Virtual Reality. J. Prof. Issues Eng. Educ. Pract. 2016, 142, 04015011. [Google Scholar] [CrossRef]
- Welcome to Facebook Horizon. Available online: https://www.youtube.com/watch?v=Is8eXZco46Q (accessed on 25 September 2019).
- Im, I.; Hong, S.; Kang, M.S. An international comparison of technology adoption: Testing the UTAUT model. Inform. Manag. 2011, 48, 1–8. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User Acceptance of Information Technology: Toward a Unified View. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef]
- Huang, T.; Huang, C. Elderly’s acceptance of companion robots from the perspective of user factors. Univ. Access Inf. Soc. 2020, 19, 935–948. [Google Scholar] [CrossRef]
- Petersen, F.; Jacobs, M.; Pather, S. Barriers for User Acceptance of Mobile Health Applications for Diabetic Patients: Applying the UTAUT Model. In Proceedings of the Conference on e-Business, e-Services and e-Society, Skukuza, South Africa, 6–8 April 2020; Springer International Publishing: Berlin/Heidelberg, Germany, 2020; pp. 61–72. [Google Scholar] [CrossRef]
- Ruangkana, V.; Kessuvan, A. Factors Affecting the Elderly’s Adoption of Online Purchasing. In Proceedings of the 2019 International Conference on Engineering, Science, and Industrial Applications (ICESI), Tokyo, Japan, 22–24 August 2019; pp. 1–5. [Google Scholar] [CrossRef]
- AlAwadhi, S.; Morris, A. In The Use of the UTAUT Model in the Adoption of E-Government Services in Kuwait. In Proceedings of the the 41st Hawaii International International Conference on Systems Science (HICSS-41 2008), Waikoloa, HI, USA, 7–10 January 2008; IEEE Computer Society: Piscataway, NJ, USA, 2008; p. 219. [Google Scholar] [CrossRef]
- Briz-Ponce, L.; Pereira, A.; Carvalho, L.; Juanes-Méndez, J.A.; García-Peñalvo, F.J. Learning with mobile technologies–Students’ behavior. Comput. Hum. Behav. 2017, 72, 612–620. [Google Scholar] [CrossRef]
- Dogruel, L.; Joeckel, S.; Bowman, N.D. The use and acceptance of new media entertainment technology by elderly users: Development of an expanded technology acceptance model. Behav. Inform. Technol. 2015, 34, 1052–1063. [Google Scholar] [CrossRef]
- El Shamy, N.; Hassanein, K. A Meta-Analysis of Enjoyment Effect on Technology Acceptance: The Moderating Role of Technology Conventionality. In Proceedings of the 50th Hawaii International Conference on System Sciences, Hilton Waikoloa Village, HI, USA, 4–7 January 2017. [Google Scholar] [CrossRef]
- Guner, H.; Acarturk, C. The use and acceptance of ICT by senior citizens: A comparison of technology acceptance model (TAM) for elderly and young adults. Univ. Access Inf. Soc. 2020, 19, 311–330. [Google Scholar] [CrossRef]
- Davis, F.D. Perceived Usefulness, Perceived Ease of Use, and User Acceptance of Information Technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef]
- Weatherall, J.W.A. A Grounded Theory Analysis of Older Adults and Information Technology. Educ. Gerontol. 2000, 26, 371–386. [Google Scholar] [CrossRef]
- Li, R.; Chung, T.-L.; Fiore, A.M. Factors affecting current users’ attitude towards e-auctions in China: An extended TAM study. J. Retail. Consum. Serv. 2017, 34, 19–29. [Google Scholar] [CrossRef]
- King, W.R.; He, J. A meta-analysis of the technology acceptance model. Inform. Manag. 2006, 43, 740–755. [Google Scholar] [CrossRef]
- Pal, D.; Funilkul, S.; Charoenkitkarn, N.; Kanthamanon, P. Internet-of-Things and Smart Homes for Elderly Healthcare: An End User Perspective. IEEE Access 2018, 6, 10483–10496. [Google Scholar] [CrossRef]
- Hoque, R.; Sorwar, G. Understanding factors influencing the adoption of mHealth by the elderly: An extension of the UTAUT model. Int. J. Med. Inform. 2017, 101, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Coughlin, J.F. PERSPECTIVE: Older Adults’ Adoption of Technology: An Integrated Approach to Identifying Determinants and Barriers. J. Prod. Innov. Manag. 2015, 32, 747–759. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Hypothesis | Research Hypothesis |
|---|---|
| H1 | Performance Expectancy (PE) will positively affect User Attitude (UA) |
| H2 | Effort Expectancy (EE) will positively affect User Attitude (UA) |
| H3 | Perceived Enjoyment (PEnjoy) will positively affect User Attitude (UA) |
| H4 | Facilitating Conditions (FC) will positively affect User Attitude (UA) |
| H5 | Social Influence (SI) will positively affect User Attitude (UA) |
| H6 | Social Influence (SI) will positively affect User Attitude (UA) |
| H7 | User Attitude (UA) will positively affect Behavioral Intention (BI) |
| Question | Response | Keywords | Dimension | Variable Factor |
|---|---|---|---|---|
| Do you think social VR would be helpful in your life in the future? |
|
| PEnjoy | Entertainment |
|
|
|
| |
|
| PE |
| |
|
| PE | Medical treatment | |
| Social VR would be mature in the future, would you like to use it? |
|
|
| Personal factors |
|
|
| Technical factors | |
|
|
|
|
| Variable | Description | N | (%) |
|---|---|---|---|
| Age | 60–64 | 29 | 25.4 |
| 65–69 | 37 | 32.5 | |
| 70–74 | 32 | 28.1 | |
| 75–89 | 16 | 14.0 | |
| 114 | 100 | ||
| Gender | Female | 79 | 69.3 |
| Male | 35 | 30.7 | |
| 114 | 100 | ||
| Education level | High school and under | 29 | 25.4 |
| University/Junior college | 78 | 68.4 | |
| Master degree and above | 7 | 6.1 | |
| 114 | 100 | ||
| Living condition | Live alone | 13 | 11.4 |
| Live with spouse | 42 | 36.8 | |
| Live with family | 58 | 50.9 | |
| Live in nursing institution | 1 | 0.9 | |
| 114 | 100 | ||
| Use of virtual social tools | Line | 94 | 37.8 |
| 37 | 14.9 | ||
| 61 | 24.5 | ||
| TencentInstant Messenger (QQ) | 8 | 3.2 | |
| Skype | 25 | 10.0 | |
| VR | 11 | 4.4 | |
| 2 | 0.8 | ||
| Other/none | 11 | 4.4 | |
| 114 | 100 | ||
| Service type | Medical treatment | 89 | 31.3 |
| Entertainment | 92 | 32.4 | |
| Chatting | 60 | 21.1 | |
| Shopping | 43 | 15.1 | |
| 114 | 100 |
| Constructs | No. of Questions | Cronbach’s α | Mean | SD |
|---|---|---|---|---|
| PE | 4 | 0.863 | 5.33 | 1.340 |
| EE | 4 | 0.921 | 4.75 | 1.536 |
| PEnjoy | 4 | 0.883 | 5.02 | 1.355 |
| FC | 4 | 0.915 | 4.61 | 1.596 |
| SI | 4 | 0.906 | 4.95 | 1.511 |
| UA | 4 | 0.896 | 5.15 | 1.372 |
| BI | 4 | 0.897 | 5.17 | 1.384 |
| Independent Variable | Dependent Variable | Unstandardized | Standardized | T | p | Adj-R2 | D-W | VIF | |
|---|---|---|---|---|---|---|---|---|---|
| b | Standard Error | β | |||||||
| PE | UA | 0.219 | 0.074 | 0.214 | 2.963 | 0.004 * | 0.796 | 1.775 | 2.894 |
| EE | −0.125 | 0.069 | −0.140 | −1.823 | 0.071 | 3.286 | |||
| PEnjoy | 0.397 | 0.097 | 0.392 | 4.091 | 0.000 * | 5.108 | |||
| FC | 0.066 | 0.070 | 0.076 | 0.943 | 0.348 | 3.642 | |||
| SI | 0.382 | 0.069 | 0.421 | 5.535 | 0.000 * | 3.215 | |||
| SI | BI | 0.285 | 0.067 | 0.312 | 4.277 | 0.000 * | 0.819 | 1.873 | 3.323 |
| UA | 0.635 | 0.074 | 0.630 | 8.639 | 0.000 * | 3.323 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shao, D.; Lee, I.-J. Acceptance and Influencing Factors of Social Virtual Reality in the Urban Elderly. Sustainability 2020, 12, 9345. https://doi.org/10.3390/su12229345
Shao D, Lee I-J. Acceptance and Influencing Factors of Social Virtual Reality in the Urban Elderly. Sustainability. 2020; 12(22):9345. https://doi.org/10.3390/su12229345
Chicago/Turabian StyleShao, Dan, and I-Jui Lee. 2020. "Acceptance and Influencing Factors of Social Virtual Reality in the Urban Elderly" Sustainability 12, no. 22: 9345. https://doi.org/10.3390/su12229345
APA StyleShao, D., & Lee, I.-J. (2020). Acceptance and Influencing Factors of Social Virtual Reality in the Urban Elderly. Sustainability, 12(22), 9345. https://doi.org/10.3390/su12229345