Drinking Water Security Challenges in Rohingya Refugee Camps of Cox’s Bazar, Bangladesh

 ,
,  ,
,  and
and
Abstract
1. Introduction
1.1. Status and Conditions of Rohingya Refugees
1.2. Water Quality and Access
1.2.1. Water Source and Collection
1.2.2. Source to Storage Contamination
1.2.3. Groundwater Contamination by Latrine
1.2.4. Storage Container Material
1.3. Sanitation
2. Materials and Methods
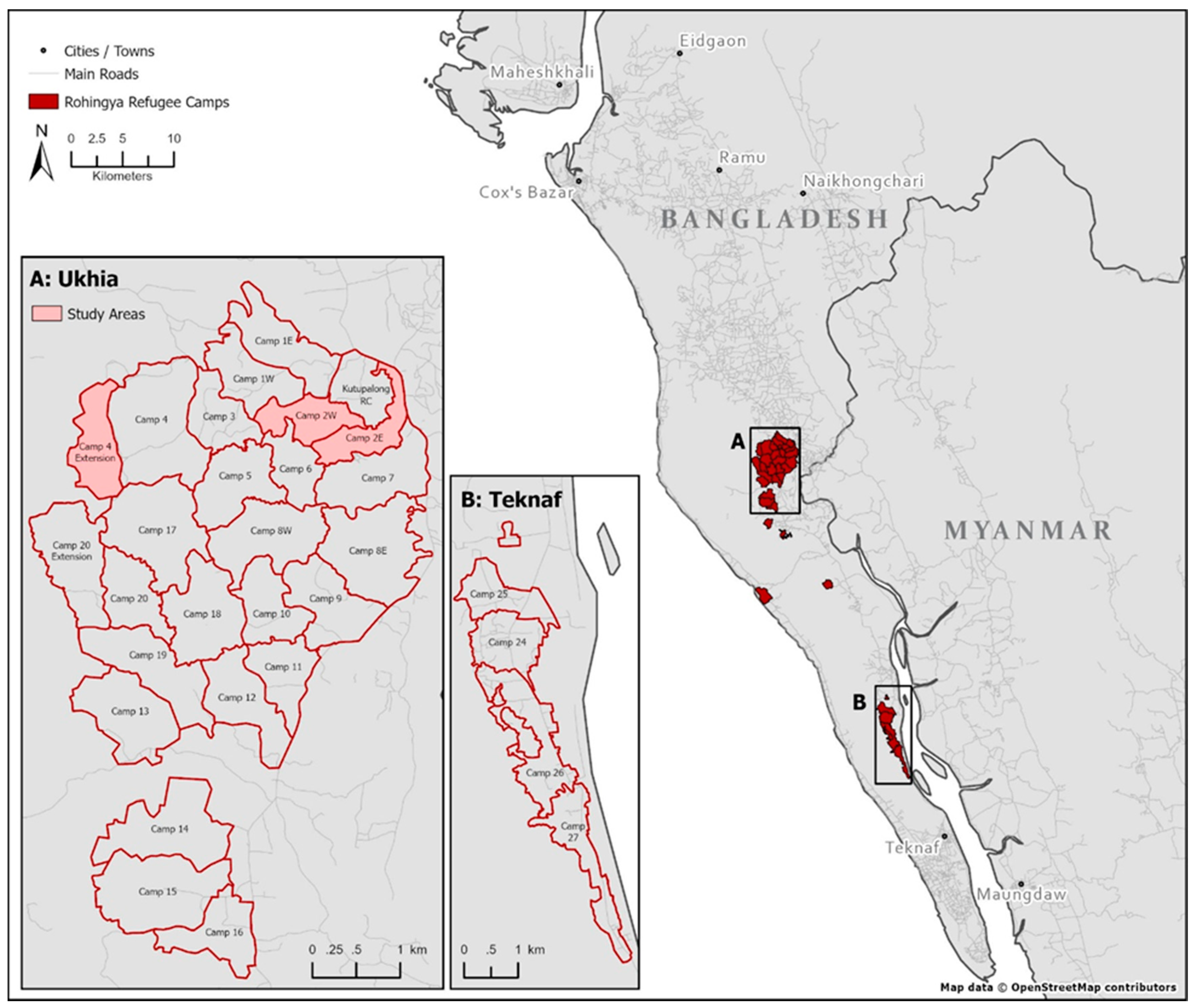
2.1. Study Area
2.2. Primary Data Collection
2.2.1. Quantitative Data: Questionnaire
2.2.2. Quantitative Data: Water Sample Collection and Analysis
Water Quality Analysis: Physical Parameters
Water Quality Analysis: Biological Parameters
2.2.3. Qualitative Data: Focus Group Discussions (FGD)
2.2.4. Qualitative Data: Key Informant Interviews (KII)
2.3. Secondary Data Collection
2.4. Data Analysis
2.5. Limitation
3. Results and Discussion
3.1. Water
3.1.1. Water Quality Assessment
3.1.2. Water Source
3.1.3. Water Source Availability
3.1.4. Water Collection Time
3.1.5. Water Collection Responsibility
3.1.6. Maintenance of Water Containers
3.1.7. Water Container Material
3.1.8. Water Treatment
3.2. Sanitation
3.2.1. Latrine Use, Desludging and Waste Disposal
3.2.2. Distance between Water Source and Latrine
3.3. Health Hazards and Disease Prevalence
3.4. Key Threats in the Future
3.4.1. Perceptions of Key Threats in the Future
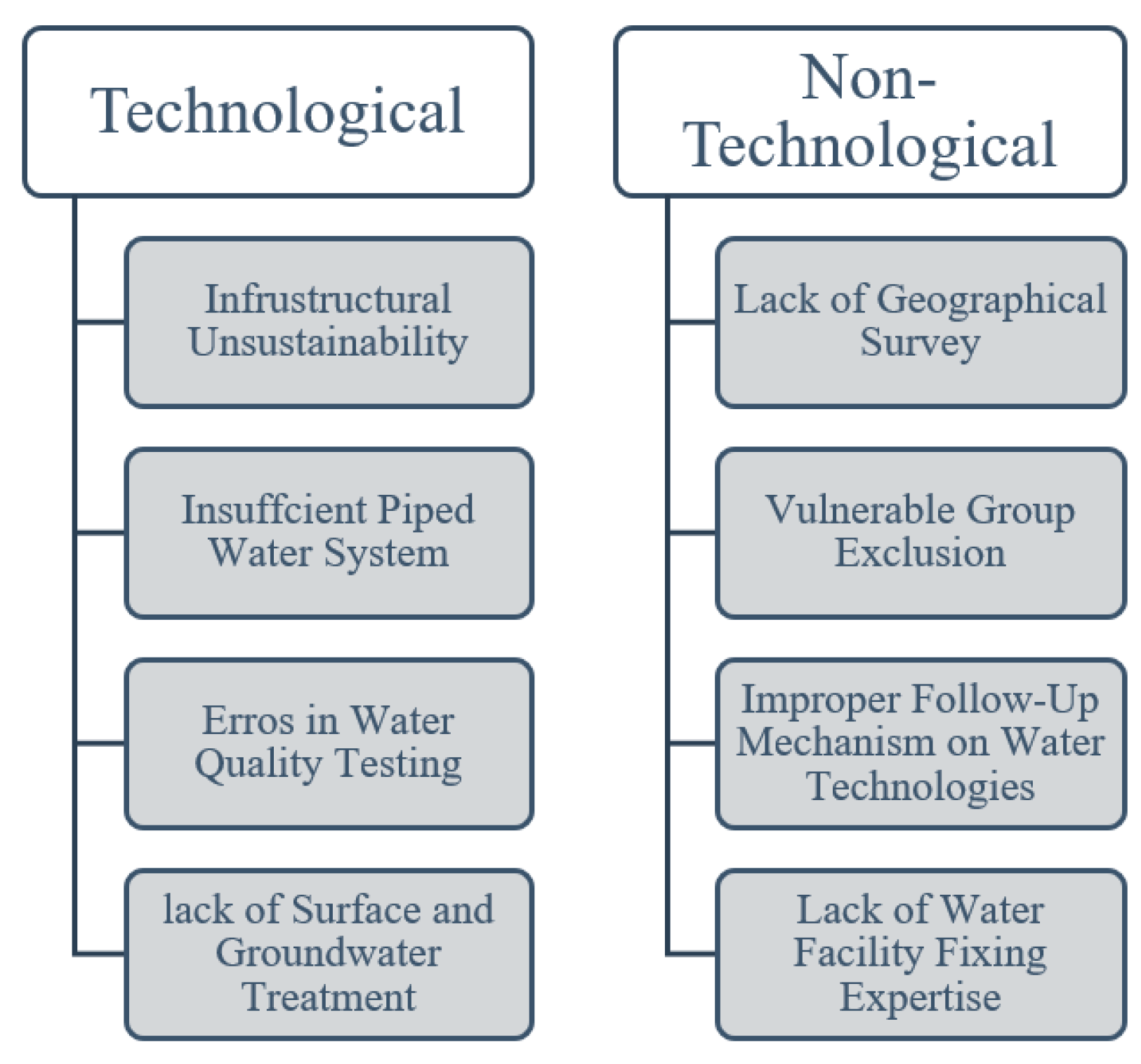
3.4.2. Key Threats that could emerge as a Result of Gaps in Water Programming
3.4.3. COVID-19 and Water Security: A New Threat?
4. Conclusions and Recommendations
4.1. Conclusions
4.2. Recommendations
- The current approach is providing basic humanitarian support to refugees, but it is not sufficient in the long-term. Given the uncertainties in Rohingya refugees returning to Myanmar, the government of Bangladesh should consider implementing projects to design and build water infrastructure that ensure the long-term water supply to the camps.
- Rainwater harvesting could be adopted as a sustainable solution to water scarcity in the dry seasons. The strategic construction of these systems could also reduce the risk of flooding in the camps.
- Since pit latrines are quick to overflow and pose risks of fecal contamination to nearby water sources, alternative methods for sanitation should be considered. Urine Diversion Dehydration Toilets (UDDTs) are a cost-effective and sustainable sanitation technology introduced in many low-income countries [86], including Bangladesh [87,88], and should be considered in the Rohingya context.
- The absence of residual free chlorine in drinking water samples is a possible health concern for refugees. Responsible agencies should take necessary steps to preserve residual chlorine at distribution points.
- Indiscriminate disposal of waste around the camps leads to reduced hygiene and increases the likelihood of contamination during water collection, transportation, and storage. An additional effort from authorities is required to ensure proper disposal and management of waste.
- Impairments to water quality require a response that integrates hygiene education and improvements to the sources, treatment, and storage of water.
- Basic training on water infrastructure repair and maintenance can be provided to the camp-based community resource volunteers among the Rohingya refugees who can take care of the water infrastructure in the camps and can support their community when needed.
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- UNHCR. Figures at a Glance. Available online: https://www.unhcr.org/figures-at-a-glance.html (accessed on 27 August 2020).
- Council on Foreign Relations (CFR). A World in Flight. Available online: https://www.cfr.org/interactive/refugee-crisis/#!/a-system-under-strain (accessed on 27 August 2020).
- Warziniack, T. The Effects of Water Scarcity and Natural Resources on Refugee Migration. Soc. Nat. Resour. 2013, 26, 1037–1049. [Google Scholar] [CrossRef]
- Black, R. Forced migration and environmental change: The impact of refugees on host environments. J. Environ. Manag. 1994, 42, 261–277. [Google Scholar] [CrossRef]
- Jacobsen, K. Refugees’ environmental impact: The effect of patterns of settlement. J. Refug. Stud. 1997, 10, 19–36. [Google Scholar] [CrossRef]
- Jacobsen, K. Can refugees benefit the state? Refugee resources and African statebuilding. J. Mod. Afr. Stud. 2002, 40, 577–596. [Google Scholar] [CrossRef]
- Jaafar, H.; Ahmad, F.; Holtmeier, L.; King-Okumu, C. Refugees, water balance, and water stress: Lessons learned from Lebanon. Ambio 2019, 49, 1179–1193. [Google Scholar] [CrossRef]
- Farishta, A. The Impact of Syrian Refugees on Jordan’s Water Resources and Water Management Planning. Ph.D. Thesis, Columbia University, New York, NY, USA, 2014. [Google Scholar]
- Abu-Allaban, M.; El-Naqa, A.; Jaber, M.; Hammouri, N. Water scarcity impact of climate change in semi-arid regions: A case study in Mujib basin, Jordan. Arab. J. Geosci. 2015, 8, 951–959. [Google Scholar] [CrossRef]
- UNDP. Rapid Assessment of the Impact of Syrian Refugee Influx on the Environment in Jordan. Available online: https://jordankmportal.com/resources/download?id=rapid-assessment-of-the-impact-of-syrian-refugee-influx-on-the-environment-in-jordan (accessed on 27 August 2020).
- Dar, D.O.; Khan, M. The Dadaab camps—Mitigating the effects of drought in the Horn (perspective). PLoS Curr. 2011, 3, RRN1289. [Google Scholar] [CrossRef]
- UNESCO. Final Report. In Proceedings of the 20th Session of the Intergovernmental Council, Paris, France, 4–7 June 2012. [Google Scholar]
- Young, S.L.; Boateng, G.O.; Jamaluddine, Z.; Miller, J.D.; Frongillo, E.A.; Neilands, T.B.; Collins, S.M.; Wutich, A.; Jepson, W.E.; Stoler, J. The Household Water InSecurity Experiences (HWISE) Scale: Development and validation of a household water insecurity measure for low-income and middle-income countries. BMJ Glob. Health 2019, 4, e001750. [Google Scholar] [CrossRef]
- Milton, A.H.; Rahman, M.; Hussain, S.; Jindal, C.; Choudhury, S.; Akter, S.; Ferdousi, S.; Mouly, T.A.; Hall, J.; Efird, J.T. Trapped in statelessness: Rohingya refugees in Bangladesh. Int. J. Environ. Res. Public Health 2017, 14, 942. [Google Scholar] [CrossRef]
- Reid, K. Rohingya Refugees in Bangladesh: Facts, FAQs, and How to Help. Available online: https://www.worldvision.org/refugees-news-stories/rohingya-refugees-bangladesh-facts (accessed on 27 August 2020).
- Inter Sector Coordination Group (ISCG), Bangladesh. 2020 Joint Response Plan for Rohingya Humanitarian Crisis. Available online: https://www.humanitarianresponse.info/sites/www.humanitarianresponse.info/files/documents/files/jrp_2020_final_in-design_200422_12.2mb.pdf (accessed on 27 August 2020).
- Islam, M.M.; Jarna, R.N.; Khan, D.H.; Nayeem, M.; Rushmi, Z.T.; Rahman, M.M.; Reza, H.M. Prevalence of Diseases among Rohingya Refugees in Bangladesh: A Comprehensive Study. IOSR J. Nurs. Health Sci. 2019, 8, 14–21. [Google Scholar]
- Inter Sector Coordination Group (ISCG), Bangladesh. 2019 Joint Response Plan for Rohingya Humanitarian Crisis. Available online: https://www.humanitarianresponse.info/sites/www.humanitarianresponse.info/files/documents/files/2019_jrp_for_rohingya_humanitarian_crisis_compressed.pdf (accessed on 27 August 2020).
- Rahman, M.D. Rohingya Refugee and Humanitarian Crisis: Synergies within Bangladesh Government and Humanitarian Community (Case Study: WASH for Rohingya Refugees); TVVR-19/5007; Division of Water Resources Engineering, Lund University: Lund, Sweden, 2019. [Google Scholar]
- Banerjee, S. The Rohingya Crisis: A Health Situation Analysis of Refugee Camps in Bangladesh. Available online: https://www.orfonline.org/research/the-rohingya-crisis-a-health-situation-analysis-of-refugee-camps-in-bangladesh-53011/ (accessed on 27 August 2020).
- You, J.; Staddon, C.; Cook, A.; Walker, J.; Boulton, J.; Powell, W.; Ieropoulos, I. Multidimensional benefits of improved sanitation: Evaluating ‘PEE POWER®’ in Kisoro, Uganda. Int. J. Environ. Res. Public Health 2020, 17, 2175. [Google Scholar] [CrossRef] [PubMed]
- Hsan, K.; Naher, S.; Griffiths, M.D.; Shamol, H.H.; Rahman, M.A. Factors associated with the practice of water, sanitation, and hygiene (WASH) among the Rohingya refugees in Bangladesh. J. Watersanitation Hyg. Dev. 2019, 9, 794–800. [Google Scholar] [CrossRef]
- Shrestha, D.; Cronin, A.A. The right to water and protecting refugees. Waterlines 2006, 24, 12. [Google Scholar] [CrossRef]
- Cronin, A.A.; Shrestha, D.; Cornier, N.; Abdalla, F.; Ezard, N.; Aramburu, C. A review of water and sanitation provision in refugee camps in association with selected health and nutrition indicators—The need for integrated service provision. J. Water Health 2007, 6, 1–13. [Google Scholar] [CrossRef]
- REACH; UNICEF. Water, Sanitation and Hygiene Assessment—Monsoon Follow-Up, Cox’s Bazar—Rohingya Refugee Response Report. Available online: https://reliefweb.int/report/bangladesh/water-sanitation-and-hygiene-assessment-monsoon-follow-cox-s-bazar-rohingya (accessed on 27 August 2020).
- Inter Sector Coordination Group (ISCG), Bangladesh. 2018 Joint Response Plan for Rohingya Humanitarian Crisis March–December 2018. Available online: https://www.humanitarianresponse.info/sites/www.humanitarianresponse.info/files/documents/files/jrp_for_rohingya_humanitarian_crisis_-_for_distribution_0.pdf (accessed on 27 August 2020).
- UNDP. Impacts of Rohingya Refugee Influx on Host Communities. Available online: https://www.humanitarianresponse.info/sites/www.humanitarianresponse.info/files/2019/08/UNDP_Impacts-of-the-Rohingya-Refugee-Influx-on-Host-Communities_Nov2018.pdf (accessed on 27 August 2020).
- Molla, M.A.M. WATER Scarcity Hits Rohingya Camp Areas. Available online: https://www.thedailystar.net/frontpage/water-scarcity-hits-rohingya-camp-areas-1585102 (accessed on 27 August 2020).
- Mahmud, Z.H.; Islam, M.S.; Imran, K.M.; Hakim, S.A.; Worth, M.; Ahmed, A.; Hossan, S.; Haider, M.; Islam, M.R.; Hossain, F.; et al. Occurrence of Escherichia coli and faecal coliforms in drinking water at source and household point-of-use in Rohingya camps, Bangladesh. Gut Pathog. 2019, 11, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Clasen, T.F.; Bastable, A. Faecal contamination of drinking water during collection and household storage: The need to extend protection to the point of use. J. Water Health 2003, 1, 109–115. [Google Scholar] [CrossRef]
- Wright, J.; Gundry, S.; Conroy, R. Household drinking water in developing countries: A systematic review of microbiological contamination between source and point-of-use. Trop. Med. Int. Health 2004, 9, 106–117. [Google Scholar] [CrossRef]
- Gundry, S.W.; Wright, J.A.; Conroy, R.; Du Preez, M.; Genthe, B.; Moyo, S.; Mutisi, C.; Ndamba, J.; Potgieter, N. Contamination of drinking water between source and point-of-use in rural households of South Africa and Zimbabwe: Implications for monitoring the Millennium Development Goal for water. Water Pract. Technol. 2006, 1, wpt2006032. [Google Scholar] [CrossRef]
- Rufener, S.; Mäusezahl, D.; Mosler, H.J.; Weingartner, R. Quality of drinking-water at source and point-of-consumption—Drinking cup as a high potential recontamination risk: A field study in Bolivia. J. Healthpopulationand Nutr. 2010, 28, 34. [Google Scholar] [CrossRef]
- Mushi, M.F.; Mpelasoka, O.E.; Mazigo, H.D.; McLeod, L.; Moremi, N.; Mirambo, M.M.; Mshana, S.E. High rate of drinking water contamination due to poor storage in squatter settlements in Mwanza, Tanzania. Tanzan. J. Health Res. 2018, 20. [Google Scholar] [CrossRef]
- Ngasala, T.M.; Gasteyer, S.P.; Masten, S.J.; Phanikumar, M.S. Linking Cross Contamination of Domestic Water with Storage Practices at the Point of Use in Urban Areas of Dar es Salaam, Tanzania. J. Environ. Eng. 2019, 145, 04019017. [Google Scholar] [CrossRef]
- Van Ryneveld, M.B.; Fourie, A.B. A strategy for evaluating the environmental impact of on-site sanitation systems. Water SA 1997, 23, 279–291. [Google Scholar]
- Graham, J.P.; Polizzotto, M.L. Pit latrines and their impacts on groundwater quality: A systematic review. Environ. Health Perspect. 2013, 121, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.H.; Ahmed, S.; Jakariya, M. Investigation of shallow tube-well water quality considering the influence of nearby latrines in a rural village of Bangladesh. IAHS Publ. 2009, 20, 299. [Google Scholar]
- Howard, G.; Pedley, S.; Barrett, M.; Nalubega, M.; Johal, K. Risk factors contributing to microbiological contamination of shallow groundwater in Kampala, Uganda. Water Res. 2003, 37, 3421–3429. [Google Scholar] [CrossRef]
- Banks, D.; Karnachuk, O.V.; Parnachev, V.P.; Holden, W.; Frengstad, B. Groundwater contamination from rural pit latrines: Examples from Siberia and Kosova. Water Environ. J. 2002, 16, 147–152. [Google Scholar] [CrossRef]
- Dzwairo, B.; Hoko, Z.; Love, D.; Guzha, E. Assessment of the impacts of pit latrines on groundwater quality in rural areas: A case study from Marondera district, Zimbabwe. Phys. Chem. Earth Parts A/B/C 2006, 31, 779–788. [Google Scholar] [CrossRef]
- Wright, J.A.; Cronin, A.; Okotto-Okotto, J.; Yang, H.; Pedley, S.; Gundry, S.W. A spatial analysis of pit latrine density and groundwater source contamination. Environ. Monit. Assess. 2013, 185, 4261–4272. [Google Scholar] [CrossRef]
- Ahaneku, I.E.; Adeoye, P.A. Impact of pit latrines on groundwater quality of Fokoslum, Ibadan, southwestern Nigeria. Br. J. Appl. Sci. Technol. 2014, 4, 440. [Google Scholar] [CrossRef]
- Mills, J.E.; Cumming, O. The Impact of Water, Sanitation and Hygiene on Key Health and Social Outcomes: Review of Evidence. June 2016. Available online: https://www.researchgate.net/profile/Joanna_Esteves_Mills/publication/319503296_The_impact_of_water_sanitation_and_hygiene_on_key_health_and_social_outcomes_review_of_evidence/links/59afa924458515150e4b0a73/The-impact-of-water-sanitation-and-hygiene-on-key-health-and-social-outcomes-review-of-evidence.pdf (accessed on 27 August 2020).
- AUW, Oxfam and UNHCR. HEAL in WASH: Towards a Roadmap, Project Report, Humanitarian Empowerment through Active Learning (HEAL) in Water, Sanitation and Hygiene; Asian University for Women: Chittagong, Bangladesh, 2020. [Google Scholar]
- Duru, M.; Amadi, C.; Amadi, B.; Nsofor, C.; Nze, H. Effect of different storage vessels on water quality. Glob. Res. J. Sci. 2013, 2, 9–13. [Google Scholar]
- Akuffo, I.; Cobbina, S.J.; Alhassan, E.H.; Nkoom, M. Assessment of the quality of water before and after storage in the Nyankpala community of the Tolon-Kumbungu District, Ghana. Int. J. Sci. Technol. Res. 2013, 2, 270–289. [Google Scholar]
- Packiyam, R.; Kananan, S.; Pachaiyappan, S.; Narayanan, U. Effect of storage containers on coliforms in household drinking water. Int. J. Curr. Microbiol. Appl. Sci. 2016, 5, 461–477. [Google Scholar] [CrossRef]
- Mohanan, N.; Manju, E.K.; Jacob, S. The effect of different types of storage vessels on water quality. Int. J. Innov. Res. Sci. Eng. Technol. 2017, 6, 2347–6710. [Google Scholar]
- Brown, J.; Cavill, S.; Cumming, O.; Jeandron, A. Water, sanitation, and hygiene in emergencies: Summary review and recommendations for further research. Waterlines 2012, 31, 11–29. [Google Scholar] [CrossRef]
- Inter Sector Coordination Group (ISCG), Bangladesh. COVID-19: Preparedness and Response for the Rohingya Refugee Camps and Host Communities in Cox’s Bazar District. Available online: https://www.humanitarianresponse.info/en/operations/bangladesh/document/coxs-bazar-update-8-covid-19-preparedness-and-response-06-may-2020 (accessed on 27 August 2020).
- Karin, S. Status of Rohingya Refugees in Bangladesh: A Comparative Study with Emphasis on Aspects of Women and Girls in Camps of Kutupalong, Cox’s Bazar, Bangladesh. Open Access Libr. J. 2020, 7, 1. [Google Scholar] [CrossRef]
- UNHCR. Rohingya Refugee Response Bangladesh, Camp Profiles. Available online: https://data2.unhcr.org/en/documents/download/71771 (accessed on 27 August 2020).
- Sugden, R.A.; Smith, T.M.F.; Jones, R.P. Cochran’s rule for simple random sampling. J. R. Stat. Soc. Ser. B Stat. Methodol. 2000, 62, 787–793. [Google Scholar] [CrossRef]
- Hennink, M.M. Focus Group Discussions Understanding Qualitative Research; Oxford University Press & Ebooks Corporation: New York, NY, USA, 2014. [Google Scholar]
- Kumar, K. Conducting Key Informant Interviews in Developing Countries; Agency for International Development: Washington, DC, USA, 1989; pp. 1–40. [Google Scholar]
- Thornthwaite, C.W. An approach toward a rational classification of climate. Geogr. Rev. 1948, 38, 55–94. [Google Scholar] [CrossRef]
- Mather, J.R. The Climatic Water Budget in Environmental Analysis; DC Heath and Company: Lexington, MA, USA, 1978. [Google Scholar]
- Rahman, M.J.; Nizame, F.A.; Unicomb, L.; Luby, S.P.; Winch, P.J. Behavioral antecedents for handwashing in a low-income urban setting in Bangladesh: An exploratory study. BMC Public Health 2017, 17, 1–10. [Google Scholar] [CrossRef][Green Version]
- Porter, R. New Clean Water Technology Installed in Rohingya Refugee Camps: The Refugee Crisis as a Water Crisis. Available online: https://savethewater.org/clean-water-technology-rohingya-refugee-camps/ (accessed on 27 August 2020).
- Sharma, R. Water Handling Practices and Level of Contamination between Source and Point-of Use in Kolladiba Town, Ethiopia. Int. J. Environ. Sci. Technol. 2013, 8, 25–35. [Google Scholar]
- IOM, UNHCR & UNICEF. Water Quality Dashboard-Field Agencies (February–December 2019). Available online: https://public.tableau.com/profile/tanvir.ahmed#!/vizhome/WaterQualityDashboard-FieldAgencies/Dashboard (accessed on 27 August 2020).
- IOM, UNHCR & UNICEF. Water Quality Dashboard-Field Agencies (January–June 2020). Available online: https://public.tableau.com/profile/tanvir.ahmed#!/vizhome/WaterQualityDashboard-FieldAgenciesJan-March2020/Dashboard (accessed on 27 August 2020).
- UNHCR. Camp Profiles October 2019—Rohingya Refugee Response Bangladesh. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/72961.pdf (accessed on 27 August 2020).
- Casey, V.; Brown, L.; Carpenter, J.D.; Nekesa, J.; Etti, B. The role of handpump corrosion in the contamination and failure of rural water supplies. Waterlines 2016, 59–77. [Google Scholar] [CrossRef]
- Gurzau, E.S.; Neagu, C.; Gurzau, A.E. Essential metals—Case study on iron. Ecotoxicol. Environ. Saf. 2003, 56, 190–200. [Google Scholar] [CrossRef]
- Almanaseer, N. Rainwater Harvesting for Adaptation to Water Scarcity in Refugees Camps in Jordan. J. Eng. Appl. Sci. 2019, 15. [Google Scholar] [CrossRef]
- Thomas, T.H.; Martinson, D.B. Roofwater Harvesting: A Handbook for Practitioners; Technical Paper Series, 49; IRC International Water and Sanitation Center: Delft, The Netherlands, 2007. [Google Scholar]
- Phillips, R.M.; Vujcic, J.; Boscoe, A.; Handzel, T.; Aninyasi, M.; Cookson, S.T.; Ram, P.K. Soap is not enough: Handwashing practices and knowledge in refugee camps, Maban County, South Sudan. Confl. Health 2015, 9, 39. [Google Scholar] [CrossRef] [PubMed]
- UNDP & UN-Women. Report on Environmental Impact of Rohingya Influx. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwjiutWwjvTpAhVOX30KHQVpBFIQFjADegQIARAB&url=https%3A%2F%2Fwww.undp.org%2Fcontent%2Fdam%2Fbangladesh%2Fdocs%2FPublications%2FPub-2018%2FUpdated%2FREIRI.pdf&usg=AOvVaw1xG_oXi3S_sxxRjXGEAgow (accessed on 27 August 2020).
- WHO. Emergency: Rohingya Crisis, Bi-Weekly Situation Report #12. Available online: http://www.searo.who.int/bangladesh/sitrep12cxbban2019.pdf (accessed on 27 August 2020).
- UNHCR. Longer Dry Season Shrinks Water Supply for Rohingya Refugees to Critical Levels. Available online: https://www.unhcr.org/news/briefing/2019/5/5ce7a8cb4/longer-dry-season-shrinks-water-supply-rohingya-refugees-critical-levels.html (accessed on 27 August 2020).
- Rahman, A.; UNHCR. Fighting Water Scarcity in Cox’s Bazar Refugee Camps. Available online: https://www.unhcr.org/news/latest/2019/1/5c2fc16a4/fighting-water-scarcity-coxs-bazar-refugee-camps.html (accessed on 27 August 2020).
- Ahmed, B.; Orcutt, M.; Sammonds, P.; Burns, R.; Issa, R.; Abubakar, I.; Devakumar, D. Humanitarian disaster for Rohingya refugees: Impending natural hazards and worsening public health crises. Lancet Glob. Health 2018, 6, e487–e488. [Google Scholar] [CrossRef]
- International Organization for Migration (IOM), Bangladesh. Rohingya Humanitarian Crisis Response—External Update (22–28 June 2018). Available online: https://bangladesh.iom.int/sites/default/files/documents/01-07-18/2018-06-28%20-%20IOM%20Rohingya%20Crisis%20Response%20-%20External%20Sitrep.pdf (accessed on 27 August 2020).
- WHO. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 27 August 2020).
- Chulov, M. Fears Realised as First Covid-19 Case Found in Lebanon Refugee Camp. Available online: https://www.theguardian.com/world/2020/apr/22/fears-realised-as-first-covid-19-case-diagnosed-in-lebanon-refugee-camp (accessed on 27 August 2020).
- Fallon, K. Greece: 148 Refugees Test Positive for COVID-19, All Asymptomatic. Available online: https://www.aljazeera.com/news/2020/04/greece-148-refugees-test-positive-covid-19-asymptomatic-200421134039733.html (accessed on 27 August 2020).
- Kelly, A. Covid-19 Spreading Quickly through Refugee Camps, Warn Calais Aid Groups. Available online: https://www.theguardian.com/global-development/2020/apr/09/covid-19-spreading-quickly-though-refugee-camps-warn-calais-aid-groups (accessed on 27 August 2020).
- IEDCR. COVID-19 Status Bangladesh. Available online: https://iedcr.gov.bd/covid-19/covid-19-situation-updates (accessed on 27 August 2020).
- UNHCR. Refugee Health Workers Lead COVID-19 Battle in Bangladesh Camps. Available online: https://www.unhcr.org/news/stories/2020/7/5f198f1f4/refugee-health-workers-lead-covid-19-battle-bangladesh-camps.html (accessed on 27 August 2020).
- Prothom Alo. 1700 Isolation Beds Being Prepared for Rohingyas. Prothom Alo. Available online: https://en.prothomalo.com/bangladesh/1700-isolation-beds-being-prepared-for-rohingyas (accessed on 27 August 2020).
- Prothom Alo. 500 Rohingya Drifting at Sea in Two Trawlers. Prothom Alo. Available online: https://en.prothomalo.com/bangladesh/500-rohingyas-drifting-at-sea-in-two-trawlers (accessed on 27 August 2020).
- Banerjee, S. COVID19 and Displaced Rohingyas in Bangladesh Camps. ORF. Available online: https://www.orfonline.org/expert-speak/covid19-displaced-rohingyas-bangladesh-camps-64800/ (accessed on 27 August 2020).
- Rafa, N.; Uddin, S.M.N.; Staddon, C. Exploring challenges in safe water availability and accessibility in preventing COVID-19 in refugee settlements. Water Int. 2020. [Google Scholar] [CrossRef]
- Uddin, S.M.N.; Muhandiki, V.S.; Fukuda, J.; Nakamura, M.; Sakai, A. Assessment of social acceptance and scope of scaling up urine diversion dehydration toilets in Kenya. J. Watersanitation Hyg. Dev. 2012, 2, 182–189. [Google Scholar] [CrossRef]
- Uddin, S.M.N.; Ronteltap, M.; van Lier, J.B. Assessment of urine diverting dehydrating toilets as a flood-resilient and affordable sanitation technology in the context of Bangladesh. J. Watersanitation Hyg. Dev. 2013, 3, 87–95. [Google Scholar] [CrossRef]
- Uddin, S.M.N.; Muhandiki, V.S.; Sakai, A.; Al Mamun, A.; Hridi, S.M. Socio-cultural acceptance of appropriate technology: Identifying and prioritizing barriers for widespread use of the urine diversion toilets in rural Muslim communities of Bangladesh. Technol. Soc. 2014, 38, 32–39. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primary Water Sources | Drinking Water |
|---|---|
| Improved Water Sources | >99% |
| Tubewells/boreholes/handpumps | 73% |
| Tap stand/piped water | 20% |
| Water tank | 5% |
| Protected dug well | <1% |
| Cart with small tank | <1% |
| Unimproved Water Sources | <1% |
| Unprotected dug well | <1% |
| Camp 2 (N = 70) | Camp 4 (N = 30) | |||
|---|---|---|---|---|
| Variable | n (%) | Mean ± SD | n (%) | Mean ± SD |
| Sex | ||||
| Male | 21 (30) | 8 (26.7) | ||
| Female | 49 (70) | 22 (73.3) | ||
| Age (years) | 31.03 ± 11.69 | 31.18 ± 12.43 | ||
| Education (years) | ||||
| Never Attended School | 8 (11.4) | 4 (13.3) | ||
| Primary School | 42 (60) | 17 (56.7) | ||
| Secondary School | 20 (28.6) | 9 (30) | ||
| Employment Status | ||||
| Employed | 5 (7.1) | 3 (10) | ||
| Unemployed | 65 (92.9) | 27 (90) | ||
| Sl. no | Parameter | Unit | Method/Instrument Used | Result | WHO Limit | |||
|---|---|---|---|---|---|---|---|---|
| Storage 2 | Tubewell 2 | Storage 4Ext | Tubewell 4Ext | |||||
| 1 | pH | – | Hanna HI 8424 pH Meter | 5.38 | 5.43 | 7.12 | 7.06 | 6.5–8.5 |
| 2 | Turbidity | NTU | HF Scientific DRT-100B Turbidity Meter | 0.2 | 0.7 | 1.0 | 4.0 | Max. 5 |
| 3 | Residual Chlorine | mg/L | DPD Colorimetric Method using HACH DR-2000 | Nil | Nil | Nil | Nil | Min 0.2 |
| 4 | Dissolved Oxygen | mg/L | BOYN 820 DO Meter | 5.84 | 5.71 | 6.07 | 6.12 | – |
| 5 | Total Coliform | cfu/100 mL | Membrane Filter Technique | Nil | Nil | Nil | Nil | Nil |
| 6 | Fecal Coliform | cfu/100 mL | Membrane Filter Technique | Nil | Nil | Nil | Nil | Nil |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akhter, M.; Uddin, S.M.N.; Rafa, N.; Hridi, S.M.; Staddon, C.; Powell, W. Drinking Water Security Challenges in Rohingya Refugee Camps of Cox’s Bazar, Bangladesh. Sustainability 2020, 12, 7325. https://doi.org/10.3390/su12187325
Akhter M, Uddin SMN, Rafa N, Hridi SM, Staddon C, Powell W. Drinking Water Security Challenges in Rohingya Refugee Camps of Cox’s Bazar, Bangladesh. Sustainability. 2020; 12(18):7325. https://doi.org/10.3390/su12187325
Chicago/Turabian StyleAkhter, Mehereen, Sayed Mohammad Nazim Uddin, Nazifa Rafa, Sanjida Marium Hridi, Chad Staddon, and Wayne Powell. 2020. "Drinking Water Security Challenges in Rohingya Refugee Camps of Cox’s Bazar, Bangladesh" Sustainability 12, no. 18: 7325. https://doi.org/10.3390/su12187325
APA StyleAkhter, M., Uddin, S. M. N., Rafa, N., Hridi, S. M., Staddon, C., & Powell, W. (2020). Drinking Water Security Challenges in Rohingya Refugee Camps of Cox’s Bazar, Bangladesh. Sustainability, 12(18), 7325. https://doi.org/10.3390/su12187325