Since the beginning of the last century, the relevance of thermal comfort arose in relation to environmental conditions in workplaces and to potential situations of stress for end-users as highlighted by A. Pharo Gagge [
1], where the first principle of thermodynamics was theorized with relation to the human body. However, it is only with the studies of the Danish researcher P.O. Fanger that an index of comfort and well-being, referred to as thermal comfort, was defined years later. Accordingly, ASHRAE 55 [
2] and ISO 7730 [
3] define thermal comfort standard as “that condition of mind that expresses satisfaction with the thermal environment and is assessed by subjective evaluation”. These standards define how to calculate Predicted Mean Vote (PMV) and Predicted Percentage Dissatisfied (PPD) in indoor environments, both applied to healthy people.
During the last decade, a number of studies further developed the above-mentioned definition following different approaches to demonstrate how thermal comfort could be influenced by several factors dealing with the indoor environment and human physical conditions [
4,
5,
6,
7]. Despite the huge efforts spent in this field, there is still a limited attention paid to specific environmental or biophysical conditions such as difference of gender [
8,
9], range of age (children or elderly [
10,
11,
12]), state of health [
13], state of alteration, or particular state as pregnancy that may alter the conventional perception of comfort.
As evidenced by Parsons [
14] the perception of thermal comfort changes if referring to men or women due to natural differences, but also with relation to different behaviours or habits: females tend to be cooler than males in cool conditions because they are physiologically more sensitive to temperature. Similarly, a recent study by Fabbri [
15] on indoor comfort in primary schools, evidenced how children understand thermal comfort differently. These physiological differences may be increased in particular situations or in specific building typologies where pre-defined thermal conditions are set, as happens in schools or hospitals.
Hospitals are extremely complex buildings that have been widely investigated by researchers as reported by Salonen et al. [
16] with a specific focus on the effects of the thermal environment, and many studies tried to systematically rate the comfort perception in different hospital in Sweden [
17], Belgium [
18], Taiwan [
19]. San Josè Alonso et al. [
20] linked the so-called sick building symptoms to three main causes: building characteristics, ventilation, pollution.
Specific studies have been carried out by Balaras [
21], Dascalaki [
22] and Van Gaever [
18] on an operating room (OR) with the purpose to reduce the risk of infection, to improve the design efficiency for space and indoor condition, to assess the well-being of the surgical staff. Melhado [
23] evaluated the thermal risk for the patient in operating rooms directly linking it to thermal conditions. Thermal comfort requirements are consequently set according to the function and the potentially related condition of stress as it is assumed that thermal perception impacts on work performances of medical staff [
24].
1.1. Scientific Literature
The scientific literature offers a dedicated section to patients, whose particular physical conditions are evidenced as a very relevant factor by the World Health Organization (WHO) [
25], assuming that appropriate thermal parameters could improve the healing therapy [
13]. Therefore indoor thermal comfort is widely considered a priority issue in hospitals and related studies. Despite patients’ metabolism being already investigated in the literature, the correlation with thermal comfort especially with reference to pregnant women is still an open field of research. This sounds particularly interesting because pregnancy is not a pathological status even if this temporary condition produces an alteration of normal metabolism due to a number of factors linked to the body’s physiological adaptation, to hormonal variations and psychological aspects. In normal situations, pregnant women spend a couple of days in the hospital before and after the birth to complete the medical protocols and it is expected they consider the thermal comfort perceived in the ward similar to the one of their own house. The perception of comfort is indeed a key element in this specific condition and generally with relation to the users of the hospital typology.
However, performing a literature review in Scopus, using “patient in hospital” as keyword, over a million results dealing with medical issues are obtained and refining the process within the engineering and architectural field, most of the residual papers were focused on the environmental characteristics influencing thermal comfort [
17,
22,
26] and the indoor environmental comfort [
27,
28], rather than on patients as key subject. A limited number of studies are addressed on analysing the perception according to age and gender diversity [
29,
30,
31,
32].
Despite it dates back to 2012, the paper from Khodakarami and Nasroallhi [
33] is still one of the best in providing a quite good picture of the available scientific literature in this field. Surprisingly, the relevance of this topic was clearly highlighted in a work developed in 1977 [
34], where the relation between the patient comfort and the effect of radiant ceiling heating in a hospital ward was investigated. This paper is still a milestone in the field and can be quoted in the history of this research branch.
As evidenced by Sattayakorn et al. [
35], thermal comfort in hospitals is particularly analysed in Asian countries and tropical regions such as in Malaysia [
28], Singapore [
26], Taiwan [
19], while the main source of reports across Europe come from Belgium [
36], Greece [
37] and Italy [
38,
39]. Other studies are connected to age or gender [
14], role (e.g., nurse) [
24] and some hospital-specific functions such as operating rooms [
40]. The other key topic of the proposed study, dealing with Adaptive thermal comfort, is reported in some previous research works by R. De Dear [
31,
41,
42,
43], F. Nicol [
44], Humphreys [
45] and others [
7].
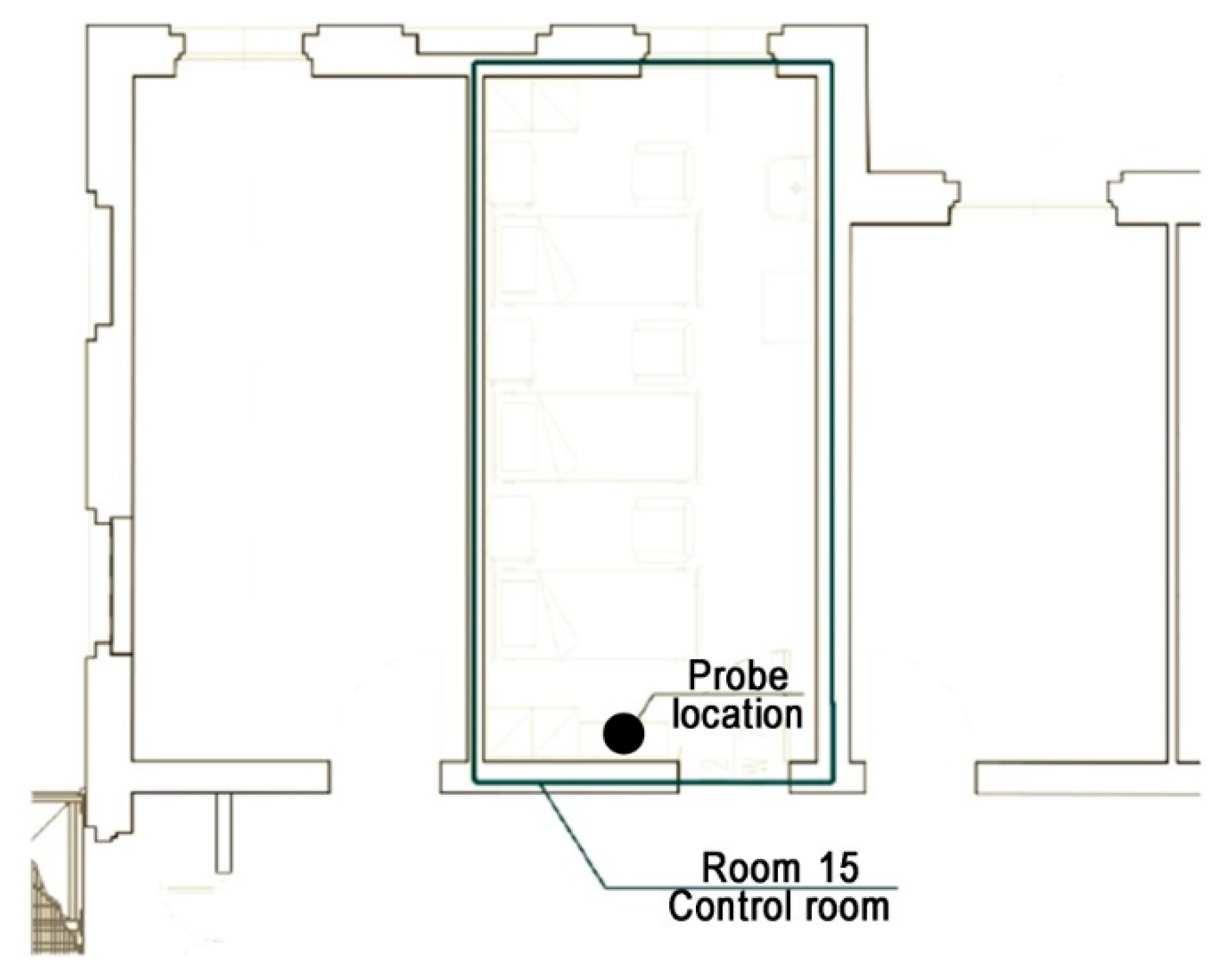
The main subject of the research reported in this paper is strictly connected with rating thermal sensation of pregnant women comparing in situ monitoring data by a probe with the perceived one by a pool of testing patients. This approach has already been tested in a study performed to investigate the level of thermal comfort understanding by very young end-users in a kindergarten [
15]. Unlike young children, who required a guided activity for completing the proposed survey, pregnant women are able to be independent in understanding the survey questions and to properly express their peculiar condition and sensations when filling the proposed form. The survey revealed that the patients do not consider architectural and behavioural features (such as bedding, clothes, services, room shape, etc.) too much relevant or at least able to influence the final outcomes.
Thermal comfort represents a key topic in several studies on building energy performance and energy efficiency with relation to standards and regulations. Accordingly, heating and cooling systems (HVAC) conventionally work using indoor thermal comfort set-point defined by the local controller. However, recent studies investigated the relationship between HVAC activation and human behaviour in influencing energy consumption.
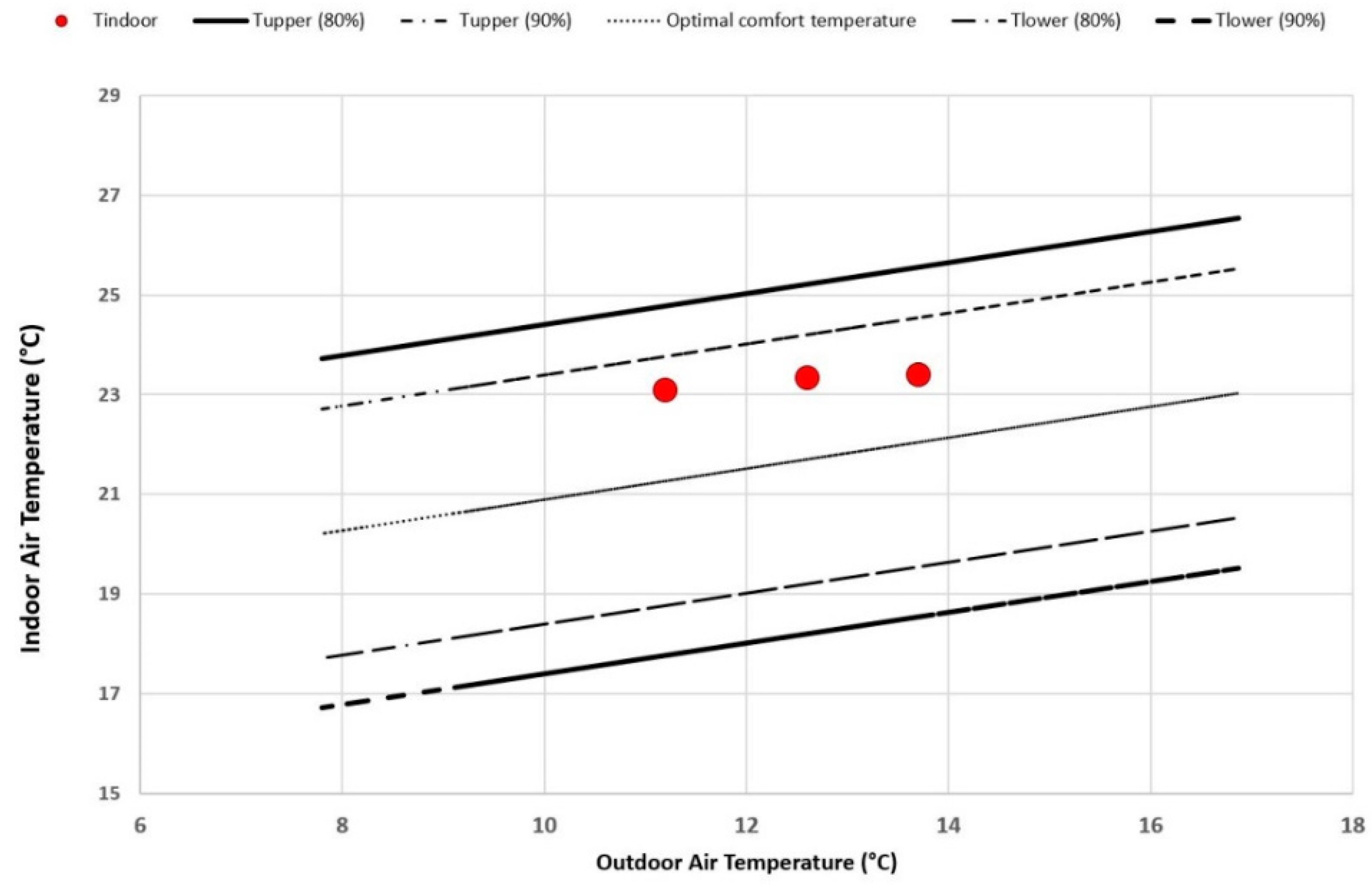
With relation to public buildings, the analysis and evaluation of indoor thermal comfort usually considered the average value of indoor temperature (even if in some typologies and functions, such as schools and hospitals, it is harder to properly consider a unique average value as the users require very specific thermal comfort conditions). This paper assumes a specific background in the scientific literature review by Yang et al. [
46] reporting the implications of thermal comfort standards in energy consumption. It includes studies of thermal comfort and adaptive models in office, school and residential buildings. Conclusions highlight the relevant influence of human behaviour with relation to perceived comfort conditions and consequent impact on energy demand without providing figures or simulations. A 1999 research from Bond et al. [
47] correlates thermal and lighting comfort level with energy consumption. Two decades later, the excellent review of Jung e Jazizadeh [
48] includes the relevant role of users in occupancy and comfort with relation to building energy efficiency. The work of Krokas et al [
49] proposes an algorithm to correlate the cumulative energy costs with the thermal comfort score (in PPD, Predicted Percentage of Dissatisfied) in order to optimize building energy management system. Buratti et al [
50] propose a simple method to correlate PMV (predicted mean vote) with HVAC indoor set-point temperature. It also proposes (Buratti et al., [
51]) a 13-value thermal comfort scale to improve energy efficiency in schools. Jazizadeh and Jung [
52] report a case study where HVAC are activated according to a personalized thermal comfort measurement by an RGB video image. Zhang et al [
53,
54] introduce an algorithm to correlate thermal comfort, indoor airspeed and air conditioning system, while Chaudahuri et al [
55] adopt an artificial neural network within the same scope. Unfortunately, none of the mentioned studies includes the hospital typology as a case study, that still remains a lack in the specific scientific literature.
The closet work to the proposed research is the one from Ugursal and Culp [
56] that considers the effect of temperature and metabolic rate on thermal comfort.
1.2. Thermal Comfort in Hospital: Observation about the Specific Case of Pregnancy
In the case of hospital buildings, energy consumption is strictly correlated to thermal comfort, especially in the case of the hospital ward, where, usually, the indoor temperature set-point is defined by law or national standards and/or following the hospital management rules. Thus, the indoor temperature set-point is not correlated to thermal comfort sensation. The proposed approach suggests that, if a more accurate thermal comfort sensation correlated to the patient (pregnant woman in the specific case) is obtained, HVAC can be set and activated according to more appropriate metering (e.g., with smart sensors) to reduce energy demand while improving the quality of the patients’ stay.
The novelty and originality of the paper concern two main aspects:
The focus on pregnant women, as the subject with a different metabolic condition, is something that in the scientific literature about thermal comfort is still missing and helps in reflecting on comfort perception with relation to measured values and pre-defined standards,
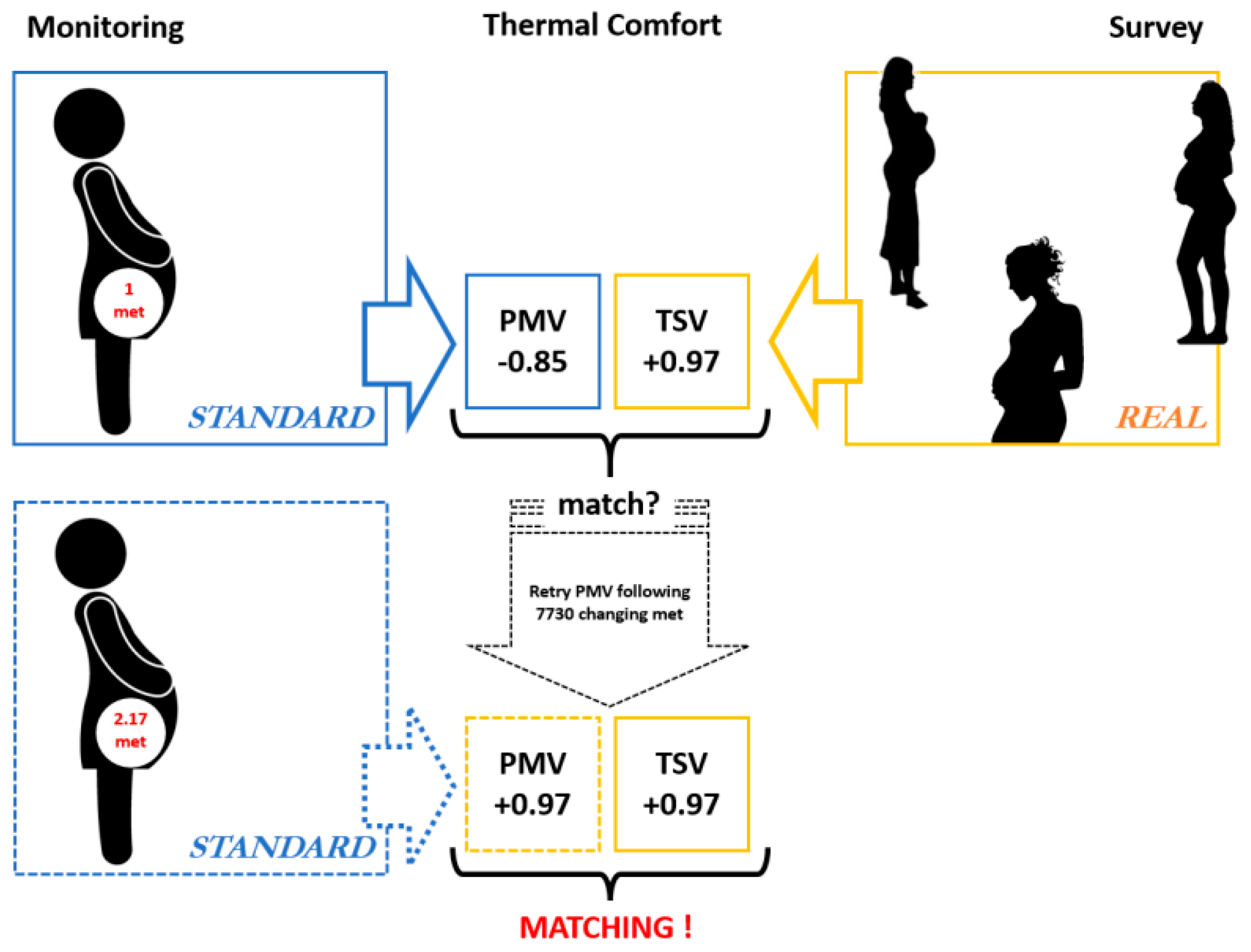
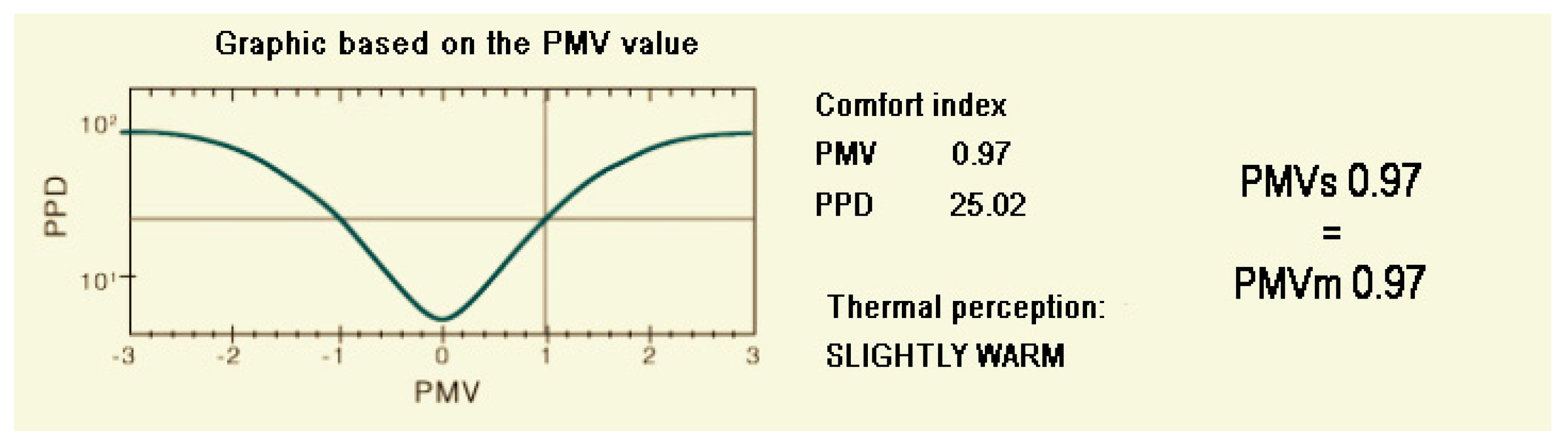
The adopted methodology combines survey and measured data to find an equivalent metabolism (met) that should be used to simulate PMV and thermal comfort following standards ASHRAE 55 [
2] and ISO 7730 [
3] and, consequently, to set HVAC system to improve building energy efficiency.
Additionally, it must be said that the study is not specifically aimed to measure a precise thermal comfort or metabolism value but rather to investigate pregnant woman in a cognitive phase concerning the building features and their perceived level with relation to a thermal comfort status. These outcomes were intended to drive renovation scenario with the purpose to improve the quality of stay as required by the hospital administration in a broader cooperation agreement aimed to address some retrofitting options.
This is the reason why the study was not originally planned to include several hospitals and enlarging the pool of patients for the survey. Thus, the authors are aware that the 55 participants to the survey are not representative from a statistical point of view to extend the validity of outcomes according to a more general perspective (even because the perception can be indirectly influenced by other factors such as the perceived quality of the healthcare system, etc.), however, the authors are also convinced that comparing the in situ measurement with a user-centred survey can be of interest for the scientific community in terms of methodological approach and of potential impacts in re-addressing the standards for very specific categories in further studies. Assuming a generalization of comfort level is not possible for all kind of subjects and some specific categories such as children, elderly and sick people are not included in ISO 7730 and ASHRAE 55 with dedicated standards further studies will be needed and pregnant women might be added as a fourth specific group to be investigated in future studies on thermal comfort.

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}