1. Introduction
Medical tourism is seen as a vacation that entails travelling into foreign countries to access a wide range of health services [
1]. Patients who feel that they are spending more than required to access their medical care in their various countries always seek an alternative in other to reduce their medical expenditure [
2,
3]. Such individuals do this by travelling to other countries where they find it cheaper to obtain the same medical services such as dental, medical, and surgical services than the ones obtained in their home or residence countries. Most patients from both developing and developed countries have had the reason to visit some emerging countries such as the United Arab Emirate (UAE), India, and others to seek medical attention. This is because health services in the aforementioned countries are relatively cheaper, and of better quality than that which is obtained in their countries [
3]. In the tourism sectors, health tourism is among the fastest growing section of tourism internationally. The list of countries that are working towards dominating and championing this market legally and practically is fast increasing. This new wave of engagement in the international trade in medical services also has great economic potential for the world economy [
4]. Investment in the medical industry is a way to increase the gross domestic product (GDP), improve services, generate foreign exchange, create a more favorable balance of trade, and boost tourism [
5]. Health tourism is currently a US
$100 billion global business and this aspect of tourism is currently experiencing an average growth rate of 25%. As such, the stakeholders are continually relying on income from medical tourism because of the perceived growth in medical tourism [
6,
7,
8].
The business opportunities that are attached to medical tourism have been identified in many countries [
9]. The United Nations Economic and Social Commission for Asia and the Pacific (UNESCAP) identified a list of countries that have started experiencing an increase in tourism travelers to their destination in 2005. An estimation of about 2.5 million people was expected to have travelled to the countries—India, Malaysia, Singapore, and Thailand (United Nations Economic and Social Commission for Asia and the Pacific (UNESCAP). Countries such as UAE, India, and the Philippines are leading, emerging major health-care destinations. According to Singh et al. [
10], many other countries such as Turkey, Colombia, Argentina, Bolivia, and Brazil are equally on track towards making themselves attractive medical service destinations. Despite the increasing possibilities of this aspect of tourism globally, especially among the emerging economies such as UAE, there is sparse extant literature on the dynamics of medical tourism. Until now, researchers have not really delved into studying this trend, thus only a few academic studies have focused on this sector. Most accessible studies only focus on some aspect of the sector such as economic or marketing aspects of health industry [
4,
11,
12,
13]. Patients have many reasons for visiting overseas for medical attention; the striking ones are the affordability and level of quality of care [
14]. Some developing countries such as India and UAE are known for less expensive and high levels of medical care [
2]. There is high demand for the expansion of this aspect of tourism and for a more comprehensive theoretical framework to show the new dimensions of this sector.
Generally, in the Arabian region, Egypt became medical tourists’ favorite destination in the 1960s. However, the consistent investment in the health sector by the Jordanian government made Jordan overtake Egypt’s position in the 1980s. Currently, UAE is not ranked among the first 10 medical tourism destinations in the world. However, the potential for the development of medical tourism which includes the availability of hot water springs, mineral water, and advanced medical technologies among others are available in the region, most of the countries are yet to maximize the opportunities. Having realized this untapped opportunity, the UAE has suddenly become a global hub and a destination favorite of foreign patients seeking high-quality services [
15]. Accordingly, the partnership of the government of UAE with prestigious health care companies and organizations like the Cleveland Clinic, John Hopkins University-Al Tawam Hospital partnership, and the Mubadala health care are among the new faces of UAE’s health system. In this light, one of the Emirati’s main administrative city—Dubai—is fast becoming a major hub for medical tourism. The city’s health care is reported to currently staff over 35,000 international professionals from more than 100 countries. Going by this pace, the city’s Dubai Health Authority (DHA) is expected to attract over 500,000 medical tourists by 2020.
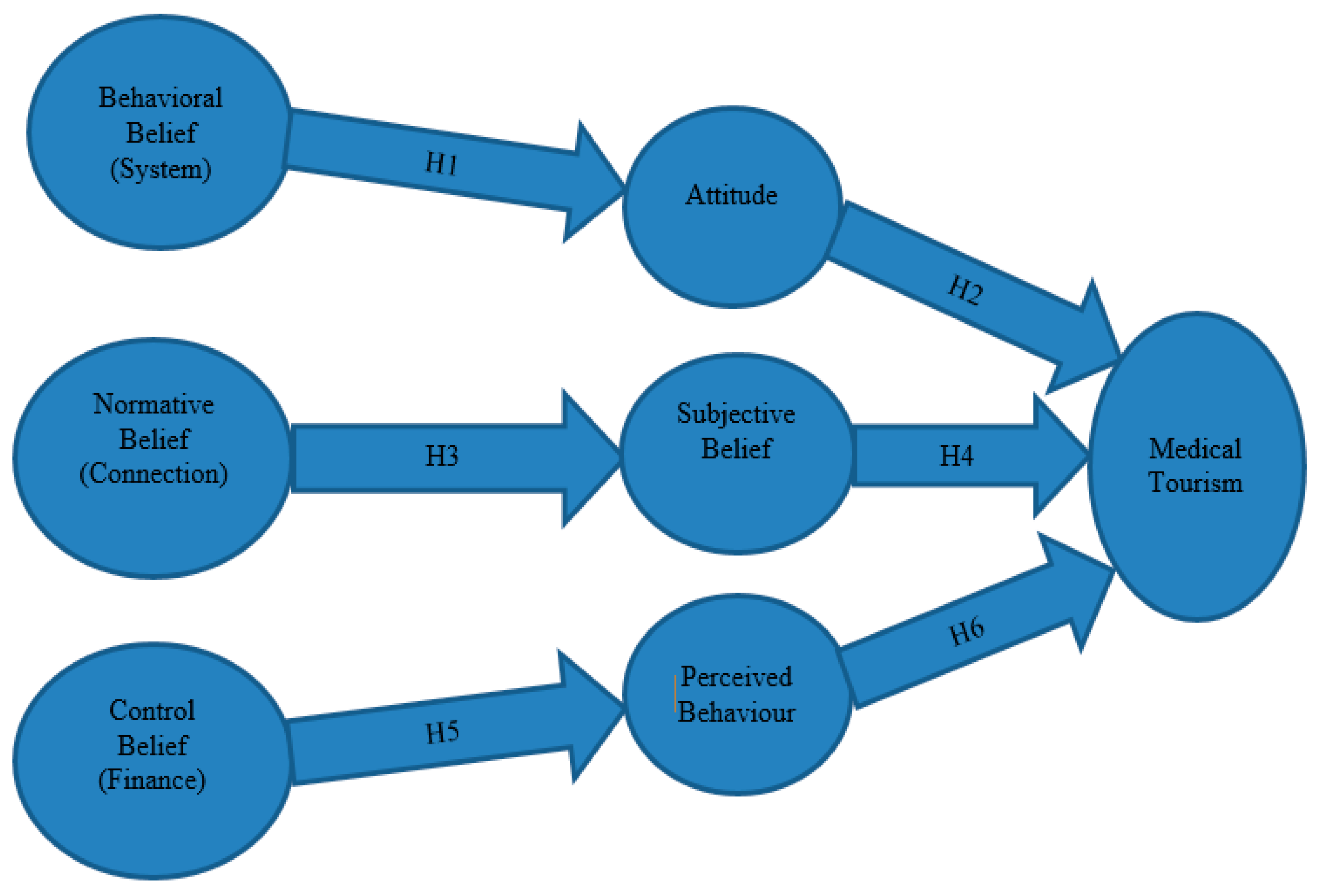
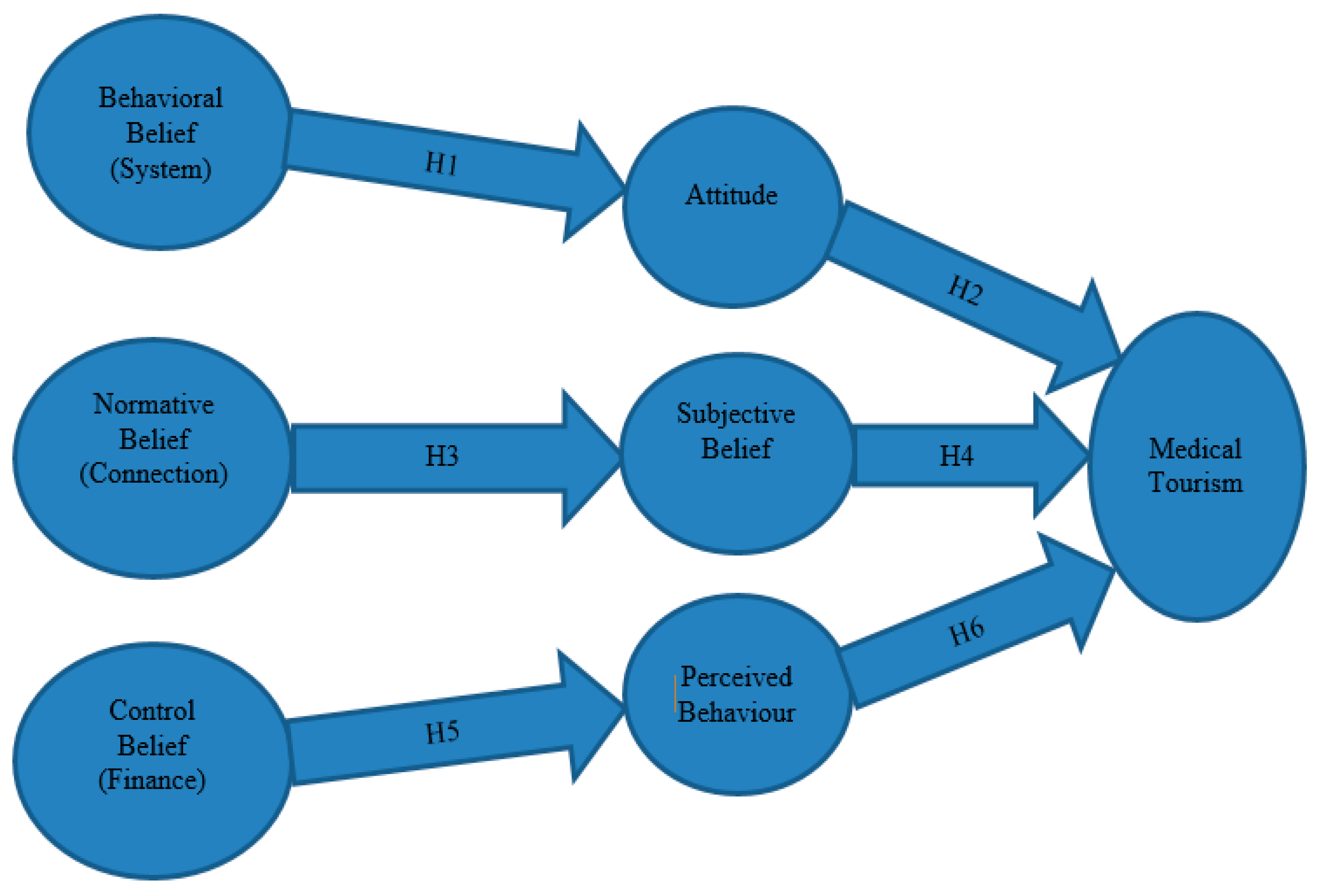
Against this backdrop and the motivations, this study aims to develop an integrated new model that will potentially underpin how to trigger greater expansion and harnessing of the potentials of medical tourism. In addition, such a model is expected to retain and maintain the trend of the medical aspect of tourism in the UAE. The study proposes a novel model developed by the authors which is called the FSC (Finance, System, and Connections) Model (
Figure 1). The model forms a triangular interaction of the factors. The factors are strong Finance (F), strong System (S), and strong Connections (C). This study includes an in-depth definition of the proposed theory and it is exploratory in nature.
The rest of the sections are arranged as follows. An overview of previous models within the context of medical health care is discussed in
Section 2. A brief discussion on the case study—UAE and the research city—Dubai is further discussed in the section. Methodology development, data description and the hypotheses with results are presented in
Section 3, while the estimated results were tested using a structural model and model fit in
Section 4.
Section 5 offers concluding remarks that include policy implications and recommended prospective studies.
3. Research Methodology
In this study, we employed a quantitative experimental approach such that data were collected by using a questionnaire as the statistical instrument. The data was collected online with respondents asked about the quality of services available at medical centers, especially in Dubai. Dubai was chosen for the study, as it is the one of the most popular medical tourism destination hub because of high investment in state of the art medical equipment. The first respondent submitted the online-completed form at 11:52:29 (UAE time) on 7 June 2018 while last returned questionnaire was received at 18:02:52 (UAE time) on 13 June 2018.
The measures in the questionnaire were constructed by adopting from existing valid and reliable sources [
42,
43,
44,
45,
46,
47,
48,
49,
50,
51]. The 320 total questionnaires were distributed among the participants and 303 of the questionnaire copies were considered as completed and reliable. Therefore, the response rate was 94.70%. Translation of the questionnaire was not necessary because the questions were written and administered in English. Prior to the collection of the data, a pilot study was conducted with 25 participants at random in order to verify the quality of the questionnaire. We applied the SMART PLS (partial least square) software package in conducting the structural equation analysis. The objective was to throw more light on model fit and variance of the model construct via the path coefficient analyses. This system is based on an iterative combination of the major component analyses and regression. The advantage of utilizing the PLS technique is its ability to simultaneously incorporate both the path coefficients and other estimates without any bias and inconsistent parameter from the side of the researcher [
15,
52]. This model is prediction oriented which makes it a good parameter for prediction.
4. Findings
The descriptive statistics in
Table 1 shows both the mean and the standard deviations of the variables in question. The variable with the highest mean is the system with 40.43 followed by the finance with 25.69 and the connection with 13.25.
The correlation test results at
Table 2 depicts positive and statistically significant relations with moderate relationship existing among the examined variables. In addition, there is empirical evidence of lesser concern for the presence of the multi-collinearity problem. The assumption here is that the closer the relationship that exists between the variables the greater the multi-collinearity. In addition, from the result of the test, it is observed that the highest number that is up to the average of one is 0.5858.
4.1. Hypotheses Tests
Following the establishment of the above hypotheses, a linear regression of quantitative analysis was employed to estimate the associated empirical evidence. The estimation observes that (see
Table 3) the R-square is 35% which means that 35% of the relationship between the dependent (Medical Tourism) and the independent variables (FSC) can be explained. Although the result of the Durbin Watson (1.7) is close to 2, there is empirical evidence of no serial correlation or autocorrelation.
Moreover, the estimates further show that the three factors (FSC) are all positively related with Medical Tourism as indicated in
Table 4. Except for the relationship between System and Medical Tourism, which is statistically significant at the 5% significance level, the associations of Finance and Connection with Medical Tourism are significant at the 1% significance level. In addition, the impacts of Finance and Connection on Medical Tourism are very similar (0.2065 and 0.2881 respectively), while the System impact on Medical Tourism is lower (0.0699).
Similarly, the H1: BB (SYSTEM) is not a positive predictor of AT for a prospective health tourist’s decision-making process to travel to Dubai for Health Treatment (HT). In addition, H2: AT (Attitude) not is a positive determinant of intention to travel to Dubai for Health Tourism (HT). The outcome of the linear regression (see
Table 4) shows that the null hypothesis is rejected given that the coefficient and the
t-statistics are respectively 0.0699 and 2.4577. Hence, the alternative hypotheses for the two hypotheses above are accepted. The results translate that System is statistically significant and with a positive relationship with Medical Tourism. This is in line with the study expectation and an indicator that better achievement of medical tourism in UAE can be sustainable with the System strategy. This means that there is a need to maintain an attractive and conducive system in the industry. Again, the H3: Normative Belief/Connection (NB) is not a positive determinant of subjective norm (SN) for the prospective tourist’s decision-making process to travel to Dubai for Health Treatment. Additionally, the H4: Subjective Norm (SN) is not a positive determinant of intention to travel to Dubai for Health Treatment (HT). Given the
t-statistic of 3.5141, which is statistically significant at 1%, the above null hypotheses of H3 and H4 are rejected. Therefore, the study accepts the alternative hypotheses. The result shows a positive coefficient of 0.2881 and is statistically significant at the
p-value (0.010). This supports the hypothesis that Connection positively affects or determines the choice of a medical tourist in choosing a medical tourism destination. Lastly, the H5: Control Belief/Finance (CBS) is not a positive predictor of PBC for the prospective tourist’s decision-making process to travel to Dubai for Health Treatment (HT). Additionally, H6: Perceived Behavioral control (PBC) is not a positive determinant of the motivation behind the prospective tourist’s intention to travel to Dubai for Health Treatment (HT). Likewise, the null hypotheses H5 and H6 can be rejected based on the result of the linear regression (see
Table 4) that showed that Finance determines the choice of a medical tourist in regards to the choice of the tourism destination. The result shows that Finance has a positive relationship with medical tourism given that the coefficient and
t-statistics are respectively 0.2065 and 5.3159 with the
p-value of 0.000.
4.2. Structural Model
In addition to the above regression analysis, we expanded our research by adding some structural analysis such as;
- (i)
Alpha reliability
- (ii)
Estimated composite reliability
- (iii)
Average Variance Extracted
- (iv)
Model Fit and R2
- (v)
Estimated path coefficients estimations and its bootstrap confidence intervals.
The three figures below display the results of the structural model, and all were done in consistency PLS Bootstrapping. The arrows included in the model show the path coefficients for only path coefficient, path coefficient with t-values, and path coefficient with p-values that are listed in the path coefficient as estimates. We adopted the 1000 sub by default to estimate the path coefficient, t-test, and p-values to determine and decide whether each causal order was significant. All the path coefficients were found to be significant at the 0.001 level with the expected signs and direction. In addition, all the t-values are above 1.96 which is the 5% significant level. It then shows that all the coefficients are statistically significant. Furthermore, the p-values are all significant, even at 0.001 (1% significant level).
4.2.1. Proposed Measurement Scales with Smart PLS
Table 5 below represents the alpha coefficients for the items within each construct and this shows that all of them are above 0.70, which is the threshold. In this case, the minimum is 0.662 which is the exact threshold if approximated to 070. The composite reliability also conforms to the values obtained from the alpha that shows that it avoided the assumption of equal weighting of the items. The average variance extraction seems to be before the threshold of 0.5, but this could be attributed the nature of the Average Variance Extracted (AVE) that most times seems to be the tougher analyses of the reliability. With the Alpha and the composite reliability values, the reliability of the model is robust.
4.2.2. Model Fit
Table 6 below displayed a model fit with the overall fit at 74.5. The model fit is good at the overall goodness of fit (GFI) which falls into the index according to Tenenhaus et al. [
53] (GFI = 0.77). The quality of the model is good and falls into the proposed overall fit. Our model shows a good and high level of forecasting power with 74.5% of the variance in satisfaction. The model has a good fit and is a good model.
4.2.3. The Models
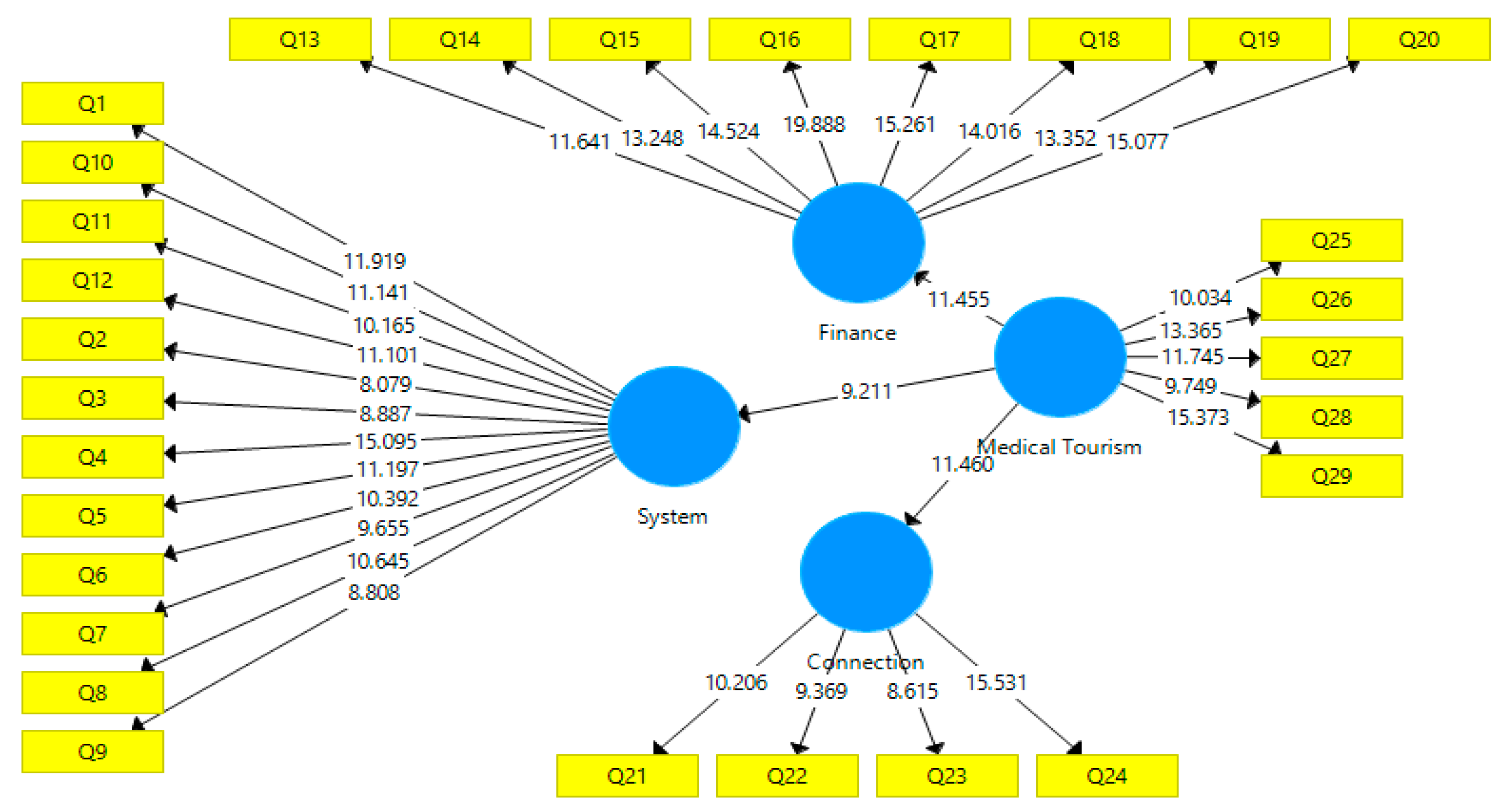
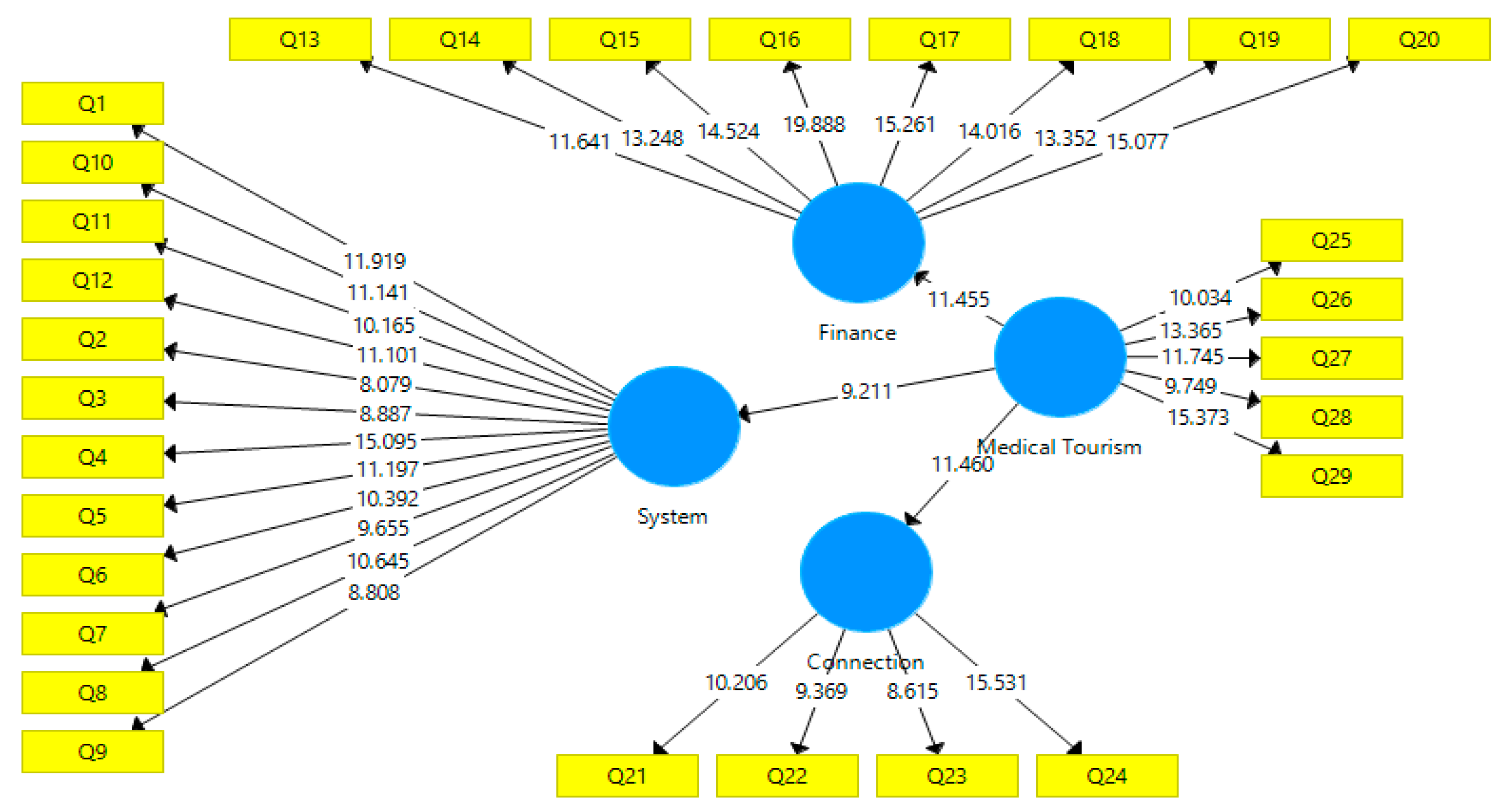
From the model structure below, the path coefficients of the variables are highly significant with the
t-values on the path coefficient arrows (
Figure 2). The
t-statistics of all the coefficients of the variables are highly significant because they are above the threshold of 1.96; this is a great pointer that the model is free from the collinearity problem.
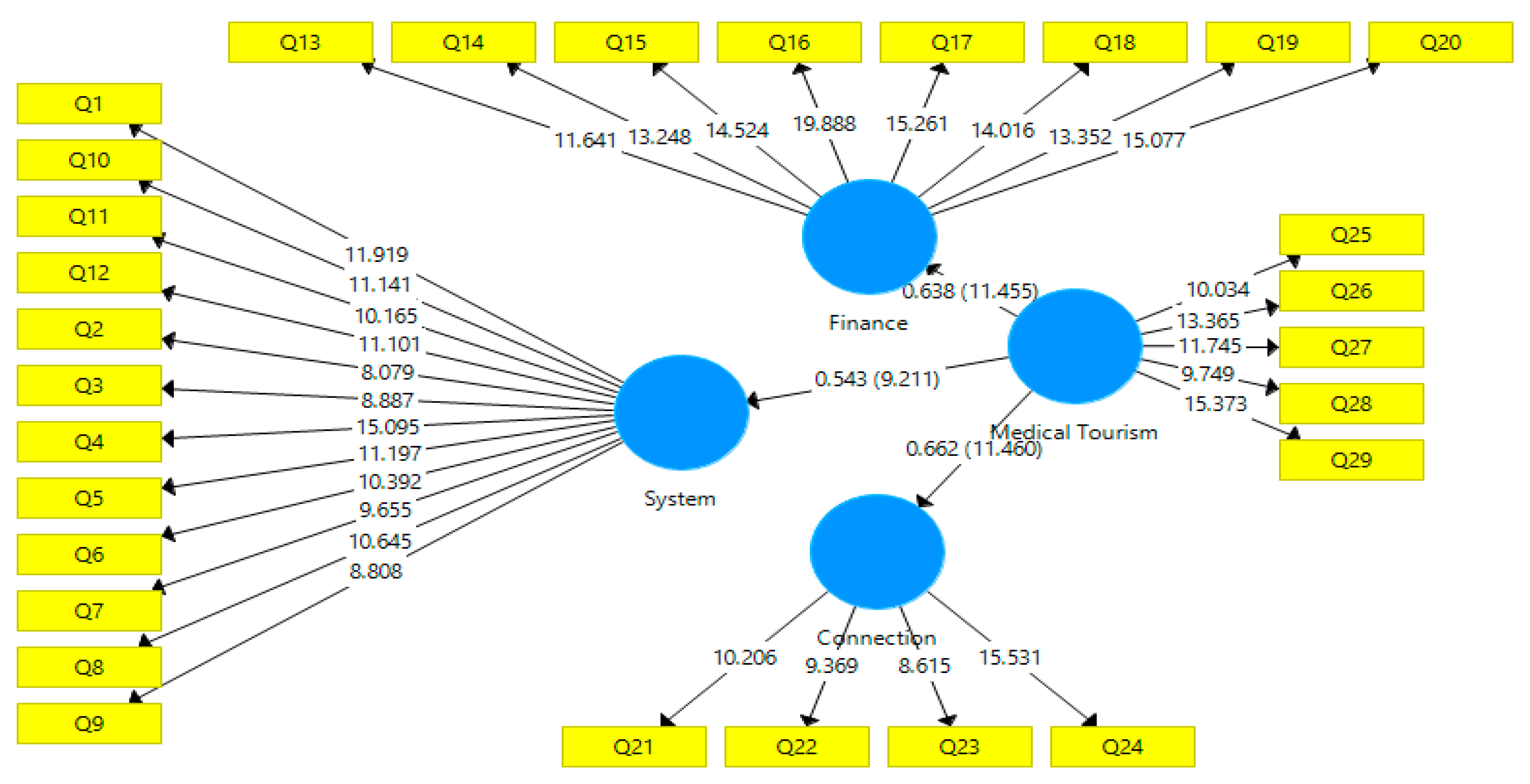
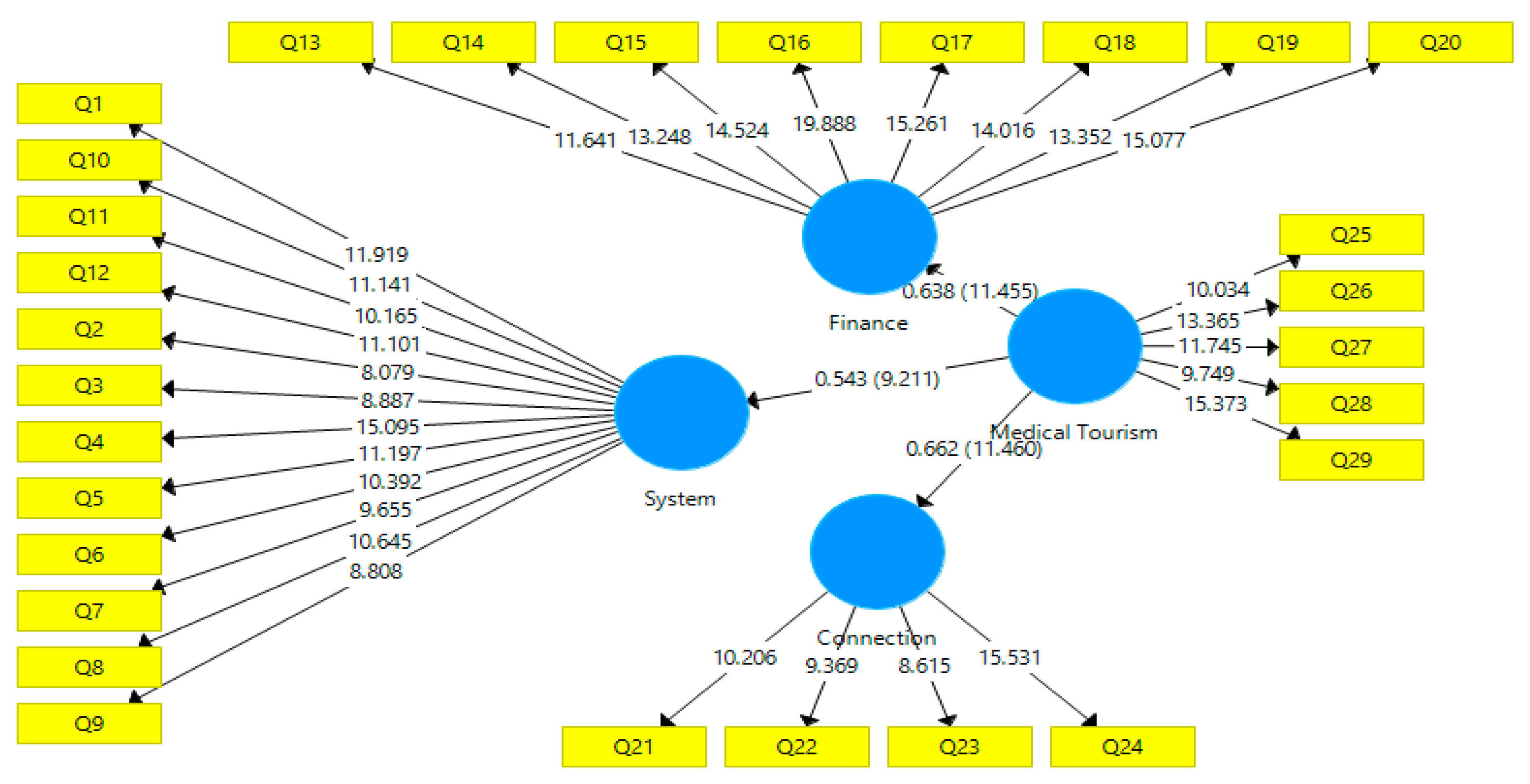
From the model structure below (
Figure 3), the entire path coefficients are significant with the values above or equal to 0.5 at 0.001. All the path coefficients were found to be significant at the 0.001 level with the anticipated signs and direction that show a good structural model fit. This shows that there is an interaction or causality passing through the variables to the targeted variable, Medical Tourism.
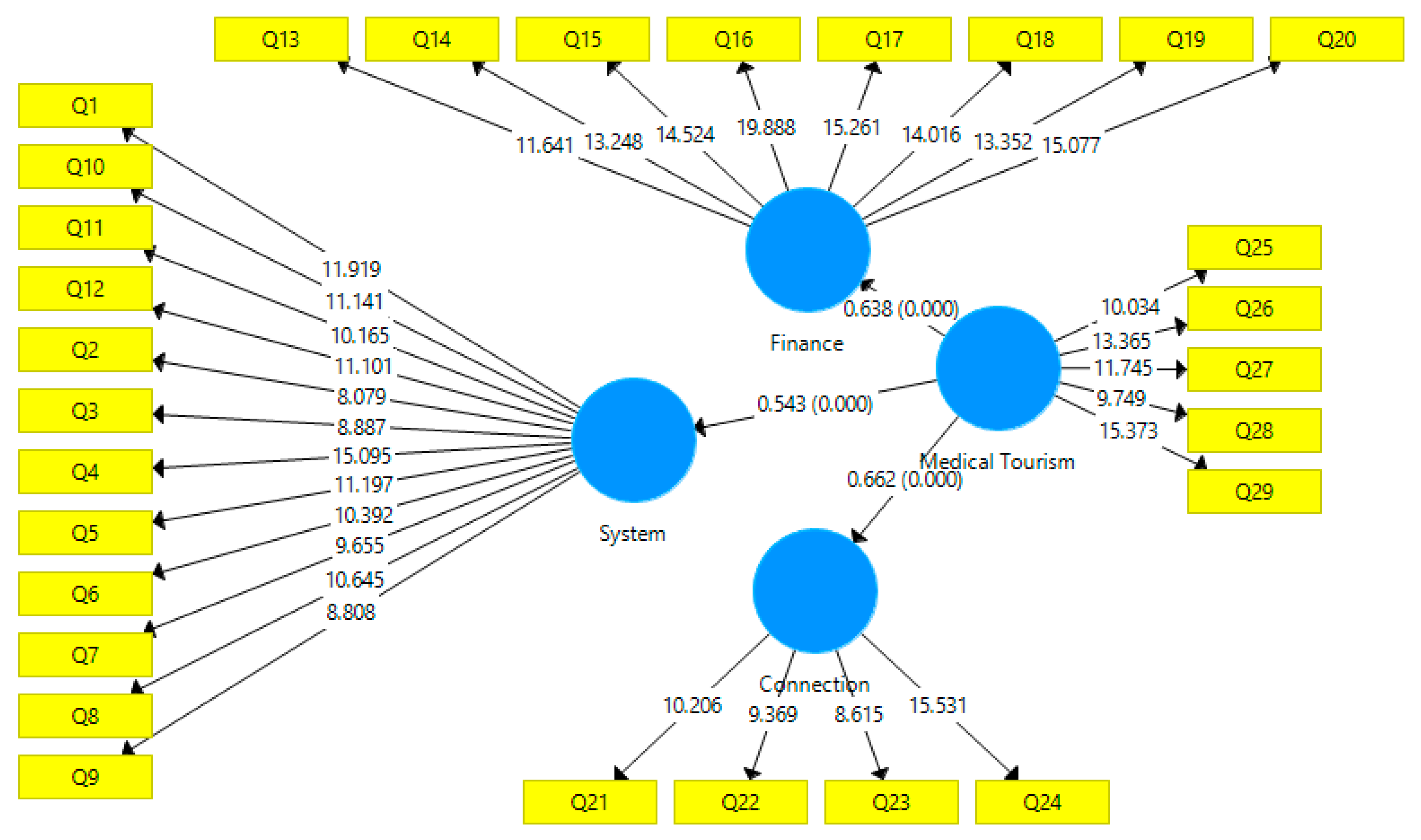
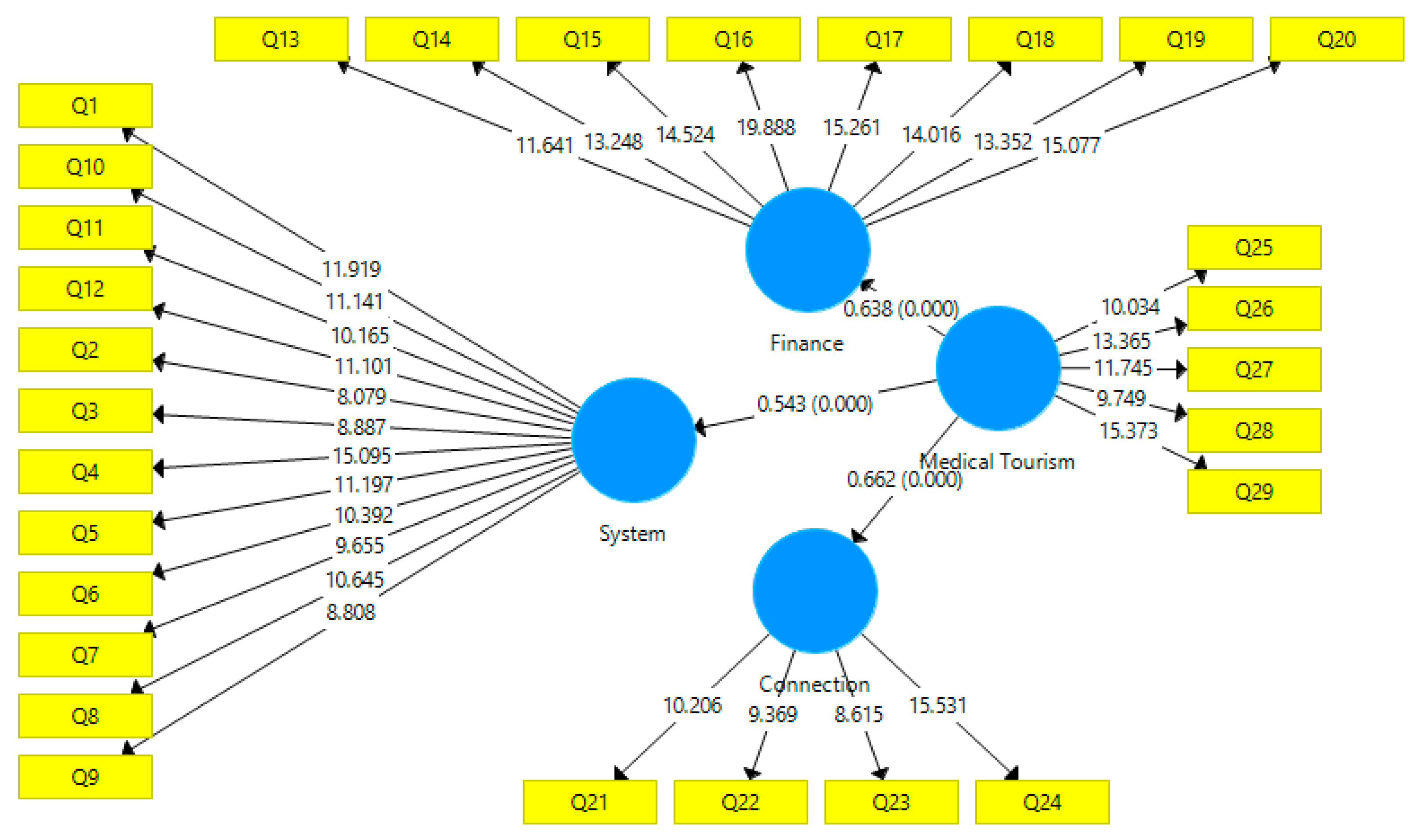
In addition, the path coefficients with
p-values are all well measured (
Figure 4) with the expected signs and level of significant at 0.001. The
p-values are statistically significant, even at 1%.
In
Table 7, the
p-value for each estimated path shows that all path coefficients are significant. In addition, the
t-statistics of all the coefficients of the variables are statistically significant since they are all above the threshold of 1.96. Hence, it is a good indicator that the model is free from the collinearity problem and the estimated coefficients have the same sign that shows that the variables are normally distributed. Additionally, the analysis of R-square coefficients explained the robustness of the finance and connection, thus, the model and its antecedents explain over 30% of the system construct. Other endogenous constructs also displayed the value of the R-square coefficients.
5. Concluding Remarks and Policy Implications
The bedrock of every business is an idea. This idea will definitely not go any longer without the applicability of the three factors studied in our model: Finance, system, and connection. Even from the statistical analyses in this work, it is observed that the chosen factors have a positive relationship with the medical tourism and they are statistically significant in determining the choice of the medical tourist and their tourism destinations. Dubai is considered among the emerging cities with good infrastructures like airlines, hospitals, good roads and hotels, and open for a market in all sectors of the economy, which tourism as a whole and medical tourism in particular, is among them. These three factors characterize the opening up of Dubai to the rest of the world. As such, the study suggests that Dubai possesses the potential to increase the traffic of tourists to come to Dubai, especially for the purpose of health. With the UAE’s desire to meet the country’s vision 2020 and subsequently turning Dubai into a medical tourist destination, evidence suggests that such vision is not far from reach. Hence, the UAE’s medical tourism policy is effectively driving the policy vehicle to meeting the Sustainable Development Goal 2030, especially, through sustainable good health and well-being.
Policy Implications
The findings of the current research present useful policy implications and direction for the stakeholders in the industry. Due to the significance of the FSC, it then suffices an implication for the government to implement policies effectively that are observed to lubricate further directly, or indirectly, the examined factors (FSC). For instance, in the aspect of finance, both the government of UAE and the administrative government of Dubai are expected to create an enabling environment for private investors. The implementation of such policy direction is billed to yield the success report enumerated by the Gulfnews (2018) [
54]. Since the industry is liberalized, the government policies like the tax reduction policy on importation of medical equipment will go a long way at aiding the performance of the privately-owned health outfit. Hence, it suggests that if the above tested factors are efficiently implemented in the business of Medical Tourism in UAE, it will tangibly contribute to the achievement of making these targets of UAE a reality. However, there are some limitations for this study. The main limitation of this study is that there are good medical tourism destinations, such as Turkey, in the region that are well known in the industry [
2]. Another limitation of this study is that the government of UAE should provide proper strategies in order to involve the private sectors to invest in medical tourism. The future research recommendations of this study are that Dubai should design and implement proper strategies, which encourage the local and foreign investors to participate in medical tourism in a way that enables Dubai to compete with the other competitors such as Turkey in the region. Lastly, there are usually two factors that need to be resolved to improve the medical tourism in Dubai, such as the high cost of medical treatment in Dubai and the lack of having elite doctors residing in Dubai. The above-mentioned factors need to be sorted out in a way to build a brand image for Dubai in medical tourism. This is because proper collaboration is required among the policymakers and the travel and tourism sectors of the Dubai [
55].



{kind=link}
{kind=link}
{kind=link}
{kind=link}