
Effectiveness of a Cucumber Extract Supplement on Articular Pain in Patients with Knee Osteoarthritis: A Randomized Double-Blind Controlled Clinical Trial

 ,
,  ,
,  ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
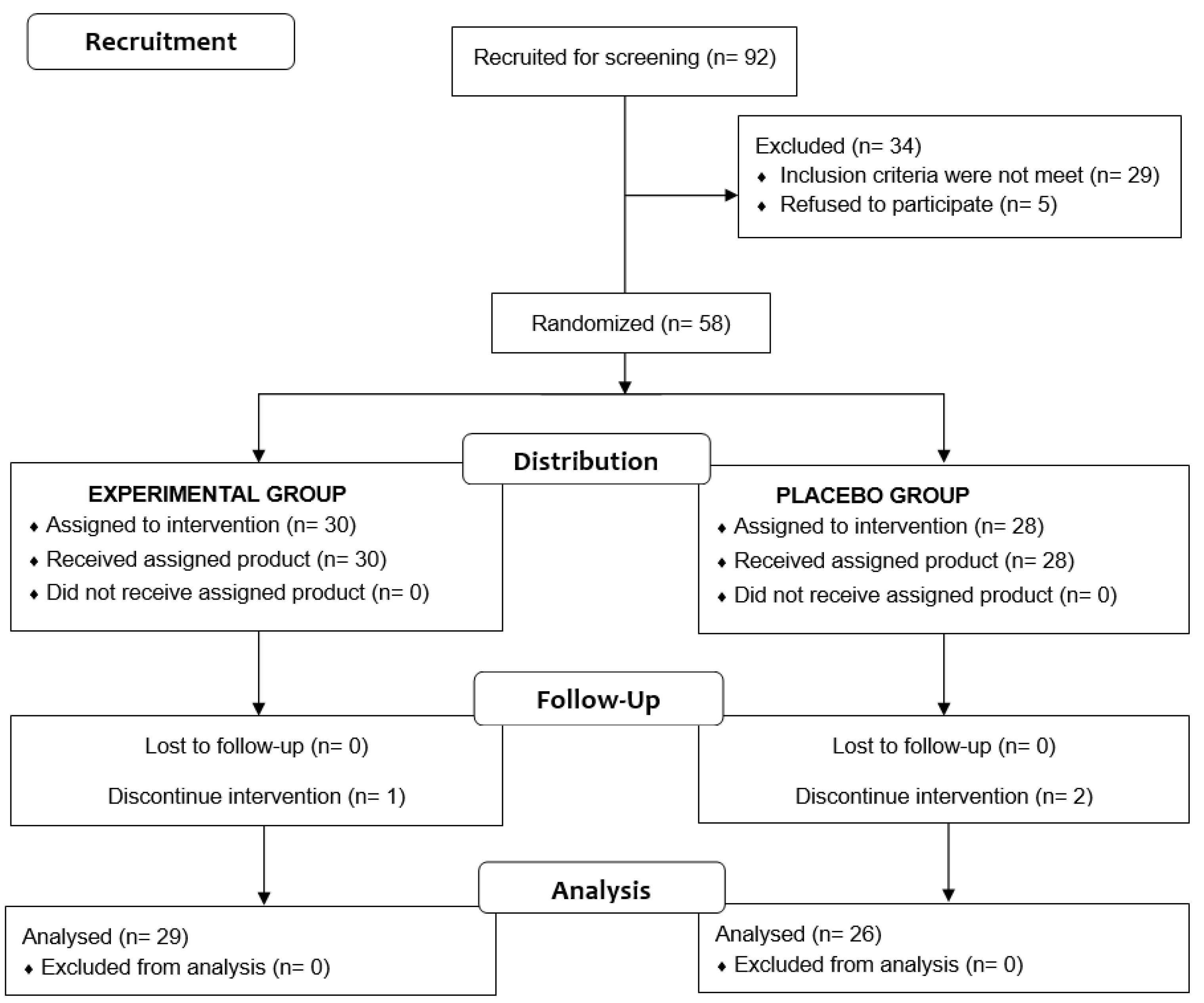
2.1. Design of the Study and Patients
2.2. Intervention and Study Procedures
2.3. Study Variables
2.4. Study Endpoints
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Changes in the Intensity of Knee Pain
3.3. Quality of Life Assessed by the WOMAC Index
3.4. Function Tests
3.4.1. Timed Up and Go (TUG)
3.4.2. Knee Isokinetic and Isometric Dynamometry
3.5. Body Composition
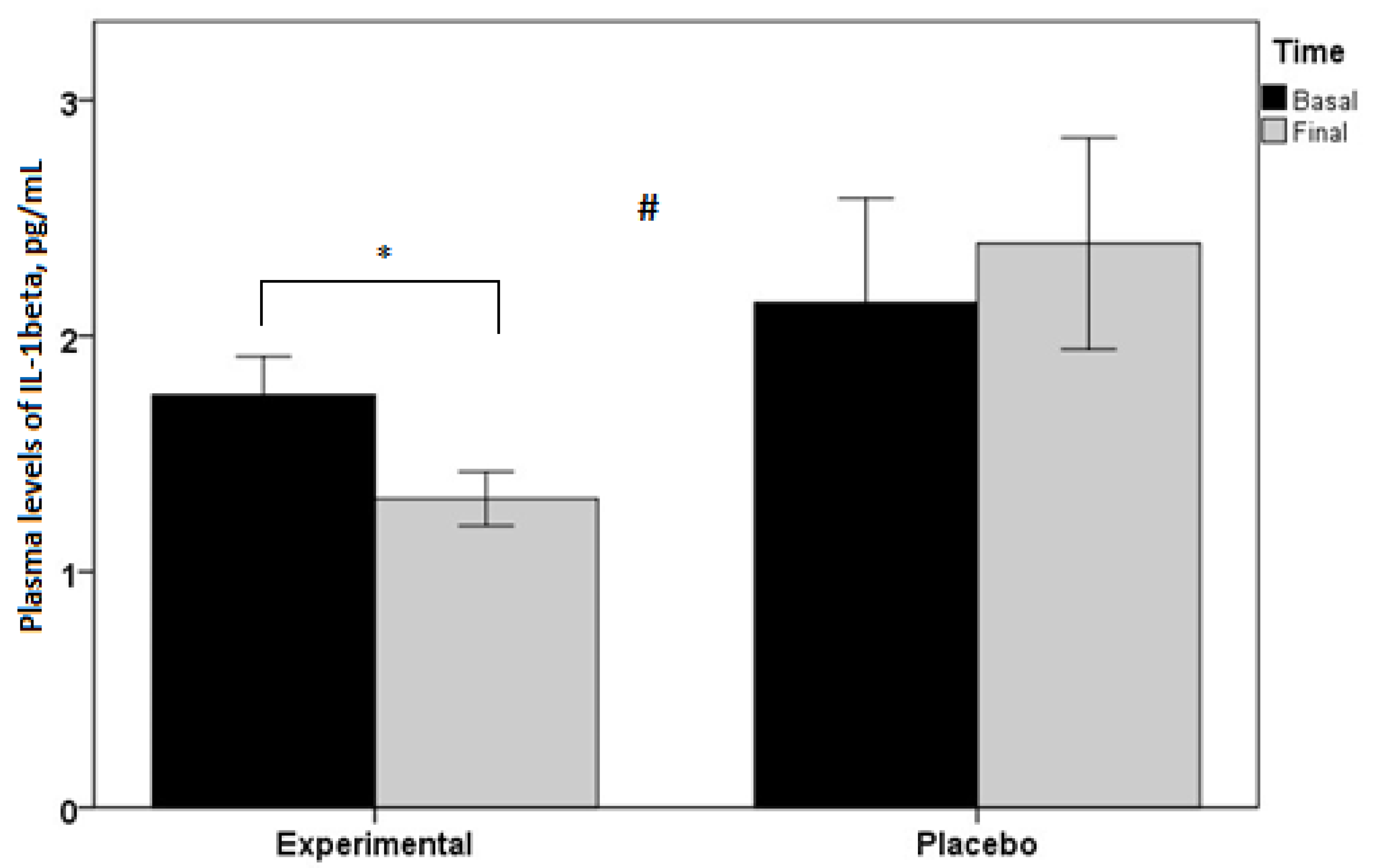
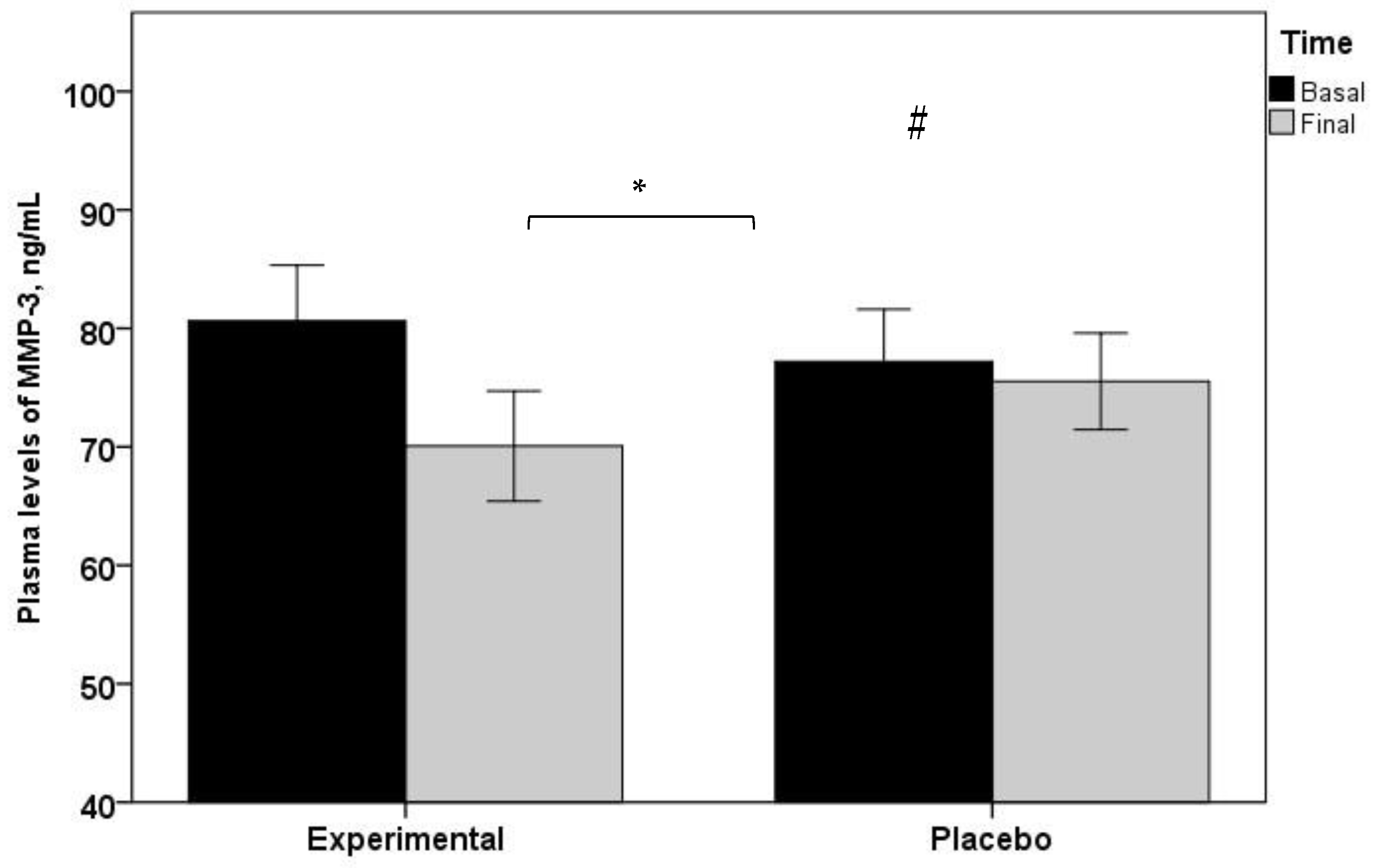
3.6. Biomarkers of Inflammation and Cartilage Degradation
3.7. Dietary Composition, Concomitant Medication and Safety Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, D.; Shen, J.; Zhao, W.; Wang, T.; Hamilton, J.L.; Im, H.J. Osteoarthritis: Toward a comprehensive understanding of pathological mechanism. Bone Res. 2017, 5, 16044. [Google Scholar] [CrossRef] [PubMed]
- Nelson, A.E.; Jordan, J.M. Defining osteoarthritis: A moving target. Osteoarthr. Cartil. 2012, 20, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Moskowitz, R.W. The burden of osteoarthritis: Clinical and quality-of-life issues. Am. J. Manag. Care 2009, 15 (Suppl. 8), S223–S229. [Google Scholar] [PubMed]
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; Bridgett, L.; Williams, S.; Guillemin, F.; Hill, C.L.; et al. The global burden of hip and knee osteoarthritis: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1323–1330. [Google Scholar] [CrossRef] [PubMed]
- Michon, M.; Maheu, E.; Berenbaum, F. Assessing health-related quality of life in hand osteoarthritis: A literature review. Ann. Rheum. Dis. 2011, 70, 921–928. [Google Scholar] [CrossRef]
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine 2020, 29, 100587. [Google Scholar] [CrossRef]
- Zhang, Y.; Jordan, J.M. Epidemiology of osteoarthritis. Clin. Geriatr. Med. 2010, 26, 355–369. [Google Scholar] [CrossRef]
- Osteoarthritis Action Alliance, Arthritis Foundation and Centers for Disease Control and Prevention. A National Publish Health Agenda for Osteoarthritis: 2022 Update. Available online: https://www.cdc.gov/arthritis/docs/oaagenda2020.pdf (accessed on 7 June 2022).
- Jordan, K.M.; Arden, N.K.; Doherty, M.; Bannwarth, B.; Bijlsma, J.W.; Dieppe, P.; Gunther, K.; Hauselmann, H.; Herrero-Beaumont, G.; Kaklamanis, P.; et al. EULAR Recommendations 2003: An evidence based approach to the management of knee osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann. Rheum. Dis. 2003, 62, 1145–1155. [Google Scholar] [CrossRef]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. 2020, 72, 149–162. [Google Scholar] [CrossRef]
- Kloppenburg, M.; Kroon, F.P.; Blanco, F.J.; Doherty, M.; Dziedzic, K.S.; Greibrokk, E.; Haugen, I.K.; Herrero-Beaumont, G.; Jonsson, H.; Kjeken, I.; et al. 2018 update of the EULAR recommendations for the management of hand osteoarthritis. Ann. Rheum. Dis. 2019, 78, 16–24. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE). Osteoarthritis in over 16s: Diagnosis and management. NICE guideline [NG226]. Available online: https://www.nice.org.uk/guidance/ng226 (accessed on 26 October 2022).
- Zhang, W.; Moskowitz, R.W.; Nuki, G.; Abramson, S.; Altman, R.D.; Arden, N.; Bierma-Zeinstra, S.; Brandt, K.D.; Croft, P.; Doherty, M.; et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthr. Cartil. 2008, 16, 137–162. [Google Scholar] [CrossRef] [PubMed]
- Laufer, S. Osteoarthritis therapy—Are there still unmet needs? Rheumatology 2004, 43 (Suppl. 1), i9–i15. [Google Scholar] [CrossRef][Green Version]
- Da Costa, B.R.; Pereira, T.V.; Saadat, P.; Rudnicki, M.; Iskander, S.M.; Bodmer, N.S.; Bobos, P.; Gao, L.; Kiyomoto, H.D.; Montezuma, T.; et al. Effectiveness and safety of non-steroidal anti-inflammatory drugs and opioid treatment for knee and hip osteoarthritis: Network meta-analysis. BMJ 2021, 375, n2321. [Google Scholar] [CrossRef] [PubMed]
- Gregori, D.; Giacovelli, G.; Minto, C.; Barbetta, B.; Gualtieri, F.; Azzolina, D.; Vaghi, P.; Rovati, L.C. Association of pharmacological treatments with long-term pain control in patients with knee osteoarthritis: A systematic review and meta-analysis. JAMA 2018, 320, 2564–2579. [Google Scholar] [CrossRef] [PubMed]
- Conaghan, P.G.; Peloso, P.M.; Everett, S.V.; Rajagopalan, S.; Black, C.M.; Mavros, P.; Arden, N.K.; Phillips, C.J.; Rannou, F.; van de Laar, M.A.; et al. Inadequate pain relief and large functional loss among patients with knee osteoarthritis: Evidence from a prospective multinational longitudinal study of osteoarthritis real-world therapies. Rheumatology 2015, 54, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Vitaloni, M.; Botto-van Bemden, A.; Sciortino, R.; Carné, X.; Quintero, M.; Santos-Moreno, P.; Espinosa, R.; Rillo, O.; Monfort, J.; de Abajo, F.; et al. A patients’ view of OA: The Global Osteoarthritis Patient Perception Survey (GOAPPS), a pilot study. BMC Musculoskelet. Disord. 2020, 21, 727. [Google Scholar] [CrossRef] [PubMed]
- Conaghan, P.G.; Porcheret, M.; Kingsbury, S.R.; Gammon, A.; Soni, A.; Hurley, M.; Rayman, M.P.; Barlow, J.; Hull, R.G.; Cumming, J.; et al. Impact and therapy of osteoarthritis: The Arthritis Care OA Nation 2012 survey. Clin. Rheumatol. 2015, 34, 1581–1588. [Google Scholar] [CrossRef]
- Castro-Domínguez, F.; Vargas-Negrín, F.; Pérez, C.; Gutiérrez-Prieto, H.; Rebollo, P. Unmet needs in the osteoarthritis chronic moderate to severe pain management in Spain: A real word data study. Rheumatol. Ther. 2021, 8, 1113–1127. [Google Scholar] [CrossRef]
- Wang, A.; Leong, D.J.; Cardoso, L.; Sun, H.B. Nutraceuticals and osteoarthritis pain. Pharmacol. Ther. 2018, 187, 167–179. [Google Scholar] [CrossRef]
- Castrogiovanni, P.; Trovato, F.M.; Loreto, C.; Nsir, H.; Szychlinska, M.A.; Musumeci, G. Nutraceutical supplements in the management and prevention of osteoarthritis. Int. J. Mol. Sci. 2016, 17, 2042. [Google Scholar] [CrossRef]
- Colletti, A.; Cicero, A.F.G. Nutraceutical approach to chronic osteoarthritis: From molecular research to clinical evidence. Int. J. Mol. Sci. 2021, 22, 12920. [Google Scholar] [CrossRef] [PubMed]
- Ghoochani, N.; Karandish, M.; Mowla, K.; Haghighizadeh, M.H.; Jalali, M.T. The effect of pomegranate juice on clinical signs, matrix metalloproteinases and antioxidant status in patients with knee osteoarthritis. J. Sci. Food Agric. 2016, 96, 4377–4381. [Google Scholar] [CrossRef] [PubMed]
- Chin, K.Y.; Pang, K.L. Therapeutic effects of olive and its derivatives on osteoarthritis: From bench to bedside. Nutrients 2017, 9, 1060. [Google Scholar] [CrossRef]
- Salehi, B.; Rescigno, A.; Dettori, T.; Calina, D.; Docea, A.O.; Singh, L.; Cebeci, F.; Özçelik, B.; Bhia, M.; Dowlati Beirami, A.; et al. Avocado-soybean unsaponifiables: A panoply of potentialities to be exploited. Biomolecules 2020, 10, 130. [Google Scholar] [CrossRef]
- Simental-Mendía, M.; Sánchez-García, A.; Acosta-Olivo, C.A.; Vilchez-Cavazos, F.; Osuna-Garate, J.; Peña-Martínez, V.M.; Simental-Mendía, L.E. Efficacy and safety of avocado-soybean unsaponifiables for the treatment of hip and knee osteoarthritis: A systematic review and meta-analysis of randomized placebo-controlled trials. Int. J. Rheum. Dis. 2019, 22, 1607–1615. [Google Scholar] [CrossRef]
- Yu, G.; Xiang, W.; Zhang, T.; Zeng, L.; Yang, K.; Li, J. Effectiveness of Boswellia and Boswellia extract for osteoarthritis patients: A systematic review and meta-analysis. BMC Complement. Med. Ther. 2010, 20, 225. [Google Scholar] [CrossRef]
- Laslett, L.L.; Jones, G. Capsaicin for osteoarthritis pain. Prog. Drug Res. 2014, 68, 277–291. [Google Scholar] [PubMed]
- Luk, H.Y.; Appell, C.; Chyu, M.C.; Chen, C.H.; Wang, C.Y.; Yang, R.S.; Shen, C.L. Impacts of green tea on joint and skeletal muscle health: Prospects of translational nutrition. Antioxidants 2020, 9, 1050. [Google Scholar] [CrossRef] [PubMed]
- Bartels, E.M.; Folmer, V.N.; Bliddal, H.; Altman, R.D.; Juhl, C.; Tarp, S.; Zhang, W.; Christensen, R. Efficacy and safety of ginger in osteoarthritis patients: A meta-analysis of randomized placebo-controlled trials. Osteoarthr. Cartil. 2015, 23, 13–21. [Google Scholar] [CrossRef]
- Kuptniratsaikul, V.; Thanakhumtorn, S.; Chinswangwatanakul, P.; Wattanamongkonsil, L.; Thamlikitkul, V. Efficacy and safety of Curcuma domestica extracts in patients with knee osteoarthritis. J. Altern. Complement. Med. 2009, 15, 891–897. [Google Scholar] [CrossRef]
- Kuptniratsaikul, V.; Dajpratham, P.; Taechaarpornkul, W.; Buntragulpoontawee, M.; Lukkanapichonchut, P.; Chootip, C.; Saengsuwan, J.; Tantayakom, K.; Laongpech, S. Efficacy and safety of Curcuma domestica extracts compared with ibuprofen in patients with knee osteoarthritis: A multicenter study. Clin. Interv. Aging 2014, 9, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, P.K.; Nema, N.K.; Maity, N.; Sarkar, B.K. Phytochemical and therapeutic potential of cucumber. Fitoterapia 2013, 84, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Nash, R.J.; Kato, A.; Yu, C.Y.; Fleet, G.W. Iminosugars as therapeutic agents: Recent advances and promising trends. Future Med. Chem. 2011, 3, 1513–1521. [Google Scholar] [CrossRef] [PubMed]
- Morita, M.; Hayashi, T.; Ochiai, M.; Maeda, M.; Yamaguchi, T.; Ina, K.; Kuzuya, M. Oral supplementation with a combination of l-citrulline and l-arginine rapidly increases plasma l-arginine concentration and enhances NO bioavailability. Biochem. Biophys. Res. Commun. 2014, 454, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Alderton, W.K.; Cooper, C.E.; Knowles, R.G. Nitric oxide synthases: Structure, function and inhibition. Biochem. J. 2001, 357, 593–615. [Google Scholar] [CrossRef]
- Ostojic, M.; Zevrnja, A.; Vukojevic, K.; Soljic, V. Immunofluorescence Analysis of NF-kB and iNOS expression in different cell populations during early and advanced knee osteoarthritis. Int. J. Mol. Sci. 2021, 22, 6461. [Google Scholar] [CrossRef]
- Víteček, J.; Lojek, A.; Valacchi, G.; Kubala, L. Arginine-based inhibitors of nitric oxide synthase: Therapeutic potential and challenges. Mediators Inflamm. 2012, 2012, 318087. [Google Scholar] [CrossRef]
- Azouz, A.A.; Saleh, E.; Abo-Saif, A.A. Aliskiren, tadalafil, and cinnamaldehyde alleviate joint destruction biomarkers; MMP-3 and RANKL; in complete Freund’s adjuvant arthritis model: Downregulation of IL-6/JAK2/STAT3 signaling pathway. Saudi Pharm. J. 2020, 28, 1101–1111. [Google Scholar] [CrossRef]
- Kumar, D.; Kumar, S.; Singh, J.; Vashistha, B.D.; Singh, N. Free radical scavening and analgesic activities of Cucumis sativus L. fruit extract. J. Young Pharm. 2010, 2, 365–368. [Google Scholar] [CrossRef]
- Wahid, S.; Alqahtani, A.; Alam Khan, R. Analgesic and anti-inflammatory effects and safety profile of Cucurbita maxima and Cucumis sativus seeds. Saudi J. Biol. Sci. 2021, 28, 4334–4341. [Google Scholar] [CrossRef]
- John, S.; Priyadarshini, S.; Sarah, J.M.; Sivaraj, C.; Arumugam, P. In vitro antioxidant and antimicrobial properties of Cucumis sativus L. peel extracts. Int. Res. J. Pharm. 2018, 9, 56–60. [Google Scholar] [CrossRef]
- Mallik, J.; Das, P.; Das, S. Pharmacological activity of Cucumis sativus L.—A complete overview. Asian J. Pharm. Res. Dev. 2013, 1, 2–6. [Google Scholar]
- Heidari, H.; Kamalinejad, M.; Noubarani, M.; Rahmati, M.; Jafarian, I.; Adiban, H.; Eskandari, M.R. Protective mechanisms of Cucumis sativus in diabetes-related models of oxidative stress and carbonyl stress. Bioimpacts 2016, 6, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Nash, R.J.; Azantsa, B.K.; Sharp, H.; Shanmugham, V. Effectiveness of Cucumis sativus extract versus glucosamine-chondroitin in the management of moderate osteoarthritis: A randomized controlled trial. Clin. Interv. Aging 2018, 13, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Hochberg, M.C.; Chang, R.W.; Dwosh, I.; Lindsey, S.; Pincus, T.; Wolfe, F. The American College of Rheumatology 1991 revised criteria for the classification of global functional status in rheumatoid arthritis. Arthritis Rheum. 1992, 35, 498–502. [Google Scholar] [CrossRef]
- Batlle-Gualda, E.; Esteve-Vives, M.C.; Riera, P.; Hargreaves, R.; Cutts, J. Translation and adaptation of the WOMAC questionnaire specific for knee and hip osteoarthritis. Rev. Esp. Reumatol. 1999, 26, 38–45. [Google Scholar]
- Barry, E.; Galvin, R.; Keogh, C.; Horgan, F.; Fahey, T. Is the Timed Up and Go test a useful predictor of risk of falls in community dwelling older adults: A systematic review and meta-analysis. BMC Geriatr. 2014, 14, 14. [Google Scholar] [CrossRef]
- Ruff, K.J.; DeVore, D.P.; Leu, M.D.; Robinson, M.A. Eggshell membrane: A possible new natural therapeutic for joint and connective tissue disorders. Results from two open-label human clinical studies. Clin. Interv. Aging 2009, 4, 235–240. [Google Scholar] [CrossRef]
- Kingsbury, S.R.; Gross, H.J.; Isherwood, G.; Conaghan, P.G. Osteoarthritis in Europe: Impact on health status, work productivity and use of pharmacotherapies in five European countries. Rheumatology 2014, 53, 937–947. [Google Scholar] [CrossRef]
- Berend, K.R.; Berend, M.E.; Dalury, D.F.; Argenson, J.N.; Dodd, C.A.; Scott, R.D. Consensus statement on indications and contraindications for medial unicompartmental knee arthroplasty. J. Surg. Orthop. Adv. 2015, 24, 252–256. [Google Scholar]
- Rodriguez-Merchan, E.C.; Delgado-Martinez, A.D. Risk factors for periprosthetic joint infection after primary total knee arthroplasty. J. Clin. Med. 2022, 11, 6128. [Google Scholar] [CrossRef] [PubMed]
- Vitaloni, M.; Botto-van Bemden, A.; Sciortino Contreras, R.M.; Scotton, D.; Bibas, M.; Quintero, M.; Monfort, J.; Carné, X.; de Abajo, F.; Oswald, E.; et al. Global management of patients with knee osteoarthritis begins with quality of life assessment: A systematic review. BMC Musculoskelet. Disord. 2019, 20, 493. [Google Scholar] [CrossRef]
- Ueda, K.; Sasaki, N.; Goren, A.; Calhoun, S.R.; Shinjo, K.; Enomoto, H.; Muneta, T. Treatment satisfaction with pharmaceutical interventions in Japanese adults with osteoarthritis and chronic knee pain: An analysis of a web-based survey. Clin. Interv. Aging 2018, 13, 2179–2191. [Google Scholar] [CrossRef]
- Xue, Q.; Long, H.; Lin, J.; Du, D.; Zhou, J.; Chen, J.; Zhang, Y.; Cheng, Y.; Ma, X.; Zhang, Z. Quality of life and treatment satisfaction with pharmacological interventions in Chinese adults with chronic pain due to osteoarthritis. BMC Musculoskelet. Disord. 2021, 22, 178. [Google Scholar] [CrossRef]
- Fisher, N.M.; Pendergast, D.R.; Gresham, G.E.; Calkins, E. Muscle rehabilitation: Its effect on muscular and functional performance of patients with knee osteoarthritis. Arch. Phys. Med. Rehabil. 1991, 72, 367–374. [Google Scholar] [PubMed]
- Zacharias, A.; Green, R.A.; Semciw, A.I.; Kingsley, M.I.; Pizzari, T. Efficacy of rehabilitation programs for improving muscle strength in people with hip or knee osteoarthritis: A systematic review with meta-analysis. Osteoarthr. Cartil. 2014, 22, 1752–1773. [Google Scholar] [CrossRef] [PubMed]
- Ziypak, T.; Halici, Z.; Alkan, E.; Akpinar, E.; Polat, B.; Adanur, S.; Cadirci, E.; Ferah, I.; Bayir, Y.; Karakus, E.; et al. Renoprotective effect of aliskiren on renal ischemia/reperfusion injury in rats: Electron microscopy and molecular study. Ren. Fail. 2015, 37, 343–354. [Google Scholar] [CrossRef]
- Lopez-Castejon, G.; Brough, D. Understanding the mechanism of IL-1β secretion. Cytokine Growth Factor Rev. 2011, 22, 189–195. [Google Scholar] [CrossRef]
- Ren, K.; Torres, R. Role of interleukin-1beta during pain and inflammation. Brain Res. Rev. 2009, 60, 57–64. [Google Scholar] [CrossRef]
- Efstathiou, M.; Settas, L. The effect of non-steroidal anti-inflammatory drugs on matrix metalloproteinases levels in patients with osteoarthritis. Mediterr. J. Rheumatol. 2017, 28, 133–141. [Google Scholar] [CrossRef]
- Naito, K.; Takahashi, M.; Kushida, K.; Suzuki, M.; Ohishi, T.; Miura, M.; Inoue, T.; Nagano, A. Measurement of matrix metalloproteinases (MMPs) and tissue inhibitor of metalloproteinases-1 (TIMP-1) in patients with knee osteoarthritis: Comparison with generalized osteoarthritis. Rheumatology 1999, 38, 510–515. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pengas, I.; Eldridge, S.; Assiotis, A.; McNicholas, M.; Mendes, J.E.; Laver, L. MMP-3 in the peripheral serum as a biomarker or knee osteoarthritis, 40 years after open total knee meniscectomy. J. Exp. Orthop. 2018, 5, 21. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Component | Value | Unit |
|---|---|---|
| Energy | 50 (12) | kJ (Kcal) |
| Total lipids | 0.1 | g |
| Total protein | 0.7 | g |
| Water | 95.7 | g |
| Carbohydrates | ||
| Total fiber | 0.8 | g |
| Carbohydrates | 2 | g |
| Vitamins | ||
| Vitamin A | 2 | µg |
| Vitamin D | 0 | µg |
| Vitamin D | 0.09 | mg |
| Folic acid | 13 | µg |
| Riboflavin | 0.02 | mg |
| Niacin | 0.23 | mg |
| Thiamine | 0.02 | mg |
| Vitamin B12 | 0 | µg |
| Vitamin B6 | 0.04 | mg |
| Minerals | ||
| Calcium | 19 | mg |
| Iron | 0.3 | mg |
| Potassium | 150 | mg |
| Magnesium | 12 | mg |
| Sodium | 3 | mg |
| Phosphorus | 23 | mg |
| Iodure | 0.3 | µg |
| Selenium | 0.8 | µg |
| Zinc | 0.1 | mg |
| Variables | Total Subjects (n = 55) | Cucumber Extract (n = 29) | Placebo (n = 26) | p Value |
|---|---|---|---|---|
| Age, years | 50.6 ± 8.6 | 51.4 ± 8.5 | 50.0 ± 8.7 | 0.543 |
| Weight, kg | 76.1 ± 13.6 | 76.4 ± 13.7 | 75.7 ± 13.4 | 0.845 |
| Height, cm | 169.2 ± 8.7 | 169.2 ± 8.7 | 169.2 ± 8.7 | |
| BMI, kg/m2 | 26.5 ± 3.6 | 26.7 ± 3.7 | 26.3 ± 3.6 | 0.737 |
| VAS score | 5.2 ± 1.7 | 5.5 ± 1.5 | 5.2 ± 1.7 | 0.576 |
| VAS Score | Cucumber Extract (n = 29) | Placebo (n = 26) | Between-Group p Value |
|---|---|---|---|
| Baseline | 5.5 ± 1.5 | 5.2 ± 1.7 | 0.013 |
| End of study | 1.7 ± 1.2 | 2.9 ± 2.6 | |
| Study weeks | |||
| Week 1 | 3.7 ± 2.1 | 4.2 ± 2.5 | 0.001 |
| Week 2 | 3.2 ± 2.1 | 3.9 ± 2.5 | |
| Week 3 | 2.8 ± 2.0 | 3.8 ± 2.7 | |
| Week 4 | 2.3 ± 1.5 | 3.5 ± 2.7 | |
| Week 5 | 1.7 ± 1.4 * | 3.4 ± 2.7 * | |
| Week 6 | 1.7 ± 1.4 * | 3.3 ± 2.7 * | |
| Week 7 | 1.8 ± 1.3 * | 2.9 ± 2.4 * | |
| Week 8 | 1.7 ± 1.2 * | 2.9 ± 2.6 * |
| WOMAC Score | Baseline | End of Study | Within-Group p Value | Between-Group p Value |
|---|---|---|---|---|
| Overall | ||||
| Cucumber extract (n = 29) | 32.7 ± 13.6 | 19.3 ± 11.7 | 0.001 | 0.038 |
| Placebo (n = 26) | 31.4 ± 12.1 | 24.7 ± 13.4 | 0.004 | |
| Pain | ||||
| Cucumber extract (n = 29) | 7.4 ± 3.4 | 4.0 ± 2.2 | 0.001 | 0.114 |
| Placebo (n = 26) | 6.9 ± 3.0 | 5.2 ± 2.8 | 0.021 | |
| Stiffness | ||||
| Cucumber extract (n = 29) | 3.1 ± 1.9 | 1.7 ± 1.5 | 0.001 | 0.034 |
| Placebo (n = 26) | 2.6 ± 1.4 | 2.2 ± 1.3 | 0.207 | |
| Physical function | ||||
| Cucumber extract (n = 29) | 22.2 ± 10.3 | 13.6 ± 9.3 | 0.001 | 0.089 |
| Placebo (n = 26) | 21.9 ± 9.2 | 17.0 ± 10.4 | 0.003 |
| Variables | Experimental Group (n = 29) | Placebo Group (n = 26) | Between-Group p Value | ||||
|---|---|---|---|---|---|---|---|
| Baseline | End of Study | Within-Group p Value | Baseline | End of Study | Within- Group p Value | ||
| Isokinetic dynamometry | |||||||
| At 60°·s−1 knee extension | |||||||
| Peak torque, Nm | 119.0 ± 48.1 | 118.6 ± 48.7 | 0.942 | 108.4 ± 40.8 | 107.5 ± 41.1 | 0.849 | 0.930 |
| Relative peak torque, Nm/Kg | 1.6 ± 0.8 | 1.6 ± 0.8 | 0.943 | 1.5 ± 0.6 | 1.5 ± 0.6 | 0.862 | 0.938 |
| Total work, J | 516.6 ± 212.5 | 493.0 ± 192.3 | 0.164 | 484.7 ± 196.7 | 485.6 ± 188.9 | 0.960 | 0.319 |
| Total work for 1RM, J | 112.1± 45.4 | 106.9 ± 41.2 | 0.167 | 105.2 ± 41.1 | 105.4 ± 40.3 | 0.960 | 0.322 |
| Average power, W | 72.5 ± 28.1 | 75.6 ± 32.8 | 0.157 | 65.6 ± 26.2 | 64.7 ± 25.3 | 0.703 | 0.211 |
| At 60°·s−1 knee flexion | |||||||
| Peak torque, Nm | 60.0 ± 25.0 | 66.4 ± 26.3 | 0.007 | 57.9 ± 22.4 | 56.5 ± 22.7 | 0.542 | 0.021 |
| Relative peak torque, Nm/Kg | 0.8 ± 0.4 | 0.9 ± 0.4 | 0.004 | 0.8 ± 0.3 | 0.8 ± 0.3 | 0.633 | 0.018 |
| Total work, J | 297.3 ± 137.4 | 340.8 ± 156.7 | 0.001 | 294.9 ± 137.1 | 291.7 ± 138.0 | 0.779 | 0.004 |
| Total work for 1RM, J | 67.0 ± 29.7 | 76.5 ± 32.7 | 0.001 | 64.6 ± 28.5 | 64.7 ± 27.7 | 0.979 | 0.004 |
| Average power, W | 39.9 ± 19.2 | 46.9 ± 22.6 | 0.001 | 37.1 ± 17.0 | 36.7 ± 18.4 | 0.825 | 0.008 |
| At 180°·s−1 knee extension | |||||||
| Peak torque, Nm | 78.4 ± 40.2 | 79.4 ± 33.7 | 0.720 | 65.0 ± 24.3 | 66.8 ± 26.1 | 0.547 | 0.848 |
| Relative peak torque, Nm/Kg | 1.1 ± 0.7 | 1.1 ± 0.6 | 0.835 | 0.9 ± 0.3 | 0.9 ± 0.4 | 0.330 | 0.572 |
| Total work, J | 375.1 ± 193.5 | 370.5 ± 180.7 | 0.782 | 338.9 ± 164.0 | 317.8 ± 129.8 | 0.231 | 0.494 |
| Total work for 1RM, J | 82.0 ± 33.5 | 83.8 ± 35.0 | 0.568 | 71.6 ± 28.4 | 72.0 ± 27.9 | 0.925 | 0.746 |
| Average power, W | 118.9 ± 58.7 | 129.3 ± 64.2 | 0.008 | 102.5 ± 46.1 | 100.8 ± 44.9 | 0.655 | 0.031 |
| At 180°·s−1 knee flexion | |||||||
| Peak torque, Nm | 45.2 ± 19.1 | 50.0 ± 22.2 | 0.006 | 40.7 ± 20.8 | 40.8 ± 20.0 | 0.930 | 0.061 |
| Relative peak torque, Nm/Kg | 0.6 ± 0.3 | 0.7 ± 0.4 | 0.002 | 0.5 ± 0.3 | 0.6 ± 0.3 | 0.750 | 0.055 |
| Total work, J | 194.7 ± 143.8 | 224.2 ± 143.2 | 0.004 | 138.7 ± 110.0 | 145.0 ± 114.8 | 0.557 | 0.109 |
| Total work for 1RM, J | 44.2 ± 29.7 | 50.7 ± 30.4 | 0.011 | 32.9 ± 23.3 | 33.1 ± 23.7 | 0.934 | 0.085 |
| Average power, W | 61.5 ± 43.4 | 70.7 ± 41.9 | 0.002 | 38.7 ± 32.5 | 40.6 ± 33.6 | 0.539 | 0.087 |
| Isometric dynamometry | |||||||
| At 90° knee position | |||||||
| Peak torque, Nm | 144.7 ± 71.7 | 171.9 ± 81.8 | 0.001 | 145.4 ± 61.1 | 145.0 ± 61.4 | 0.946 | 0.002 |
| Relative peak torque, Nm/Kg | 2.0 ± 1.2 | 2.4 ± 1.4 | 0.001 | 1.9 ± 0.9 | 2.0 ± 0.8 | 0.942 | 0.002 |
| Average peak torque, Nm | 142.5 ± 56.2 | 162.0 ± 75.8 | 0.001 | 138.2 ± 58.3 | 139.2 ± 59.2 | 0.859 | 0.022 |
| Variables | Baseline | End of Study | Within-Group p Value | Between-Group p Value |
|---|---|---|---|---|
| Weight, kg | ||||
| Cucumber extract (n = 29) | 76.4 ± 13.7 | 76.0 ± 13.4 | 0.200 | 0.753 |
| Placebo (n = 26) | 75.7 ± 13.4 | 75.1 ± 12.7 | 0.102 | |
| Fat mass, kg | ||||
| Cucumber extract (n = 29) | 23.4 ± 7.2 | 22.7 ± 7.5 | 0.083 | 0.929 |
| Placebo (n = 26) | 21.6 ± 7.9 | 20.8 ± 7.6 | 0.078 | |
| Fat mass, % | ||||
| Cucumber extract (n = 29) | 30.7 ± 8.0 | 29.8 ± 8.4 | 0.107 | 0.835 |
| Placebo (n = 26) | 28.4 ± 8.3 | 27.7 ± 8.5 | 0.212 | |
| Muscle mass, kg | ||||
| Cucumber extract (n = 29) | 50.3 ± 11.3 | 50.6 ± 10.8 | 0.529 | 0.215 |
| Placebo (n = 26) | 51.5 ± 10.3 | 51.0 ± 10.7 | 0.264 |
| Variables | Baseline | End of Study | Within-Group p Value | Between-Group p Value |
|---|---|---|---|---|
| IL-1β, pg/mL | ||||
| Cucumber extract (n = 29) | 1.8 ± 0.9 | 1.3 ± 0.6 | 0.050 | 0.044 |
| Placebo (n = 26) | 2.1 ± 2.3 | 2.4 ± 2.3 | 0.305 | |
| MMP-3, ng/mL | ||||
| Cucumber extract (n = 29) | 80.6 ± 25.3 | 70.1 ± 25.0 | 0.001 | 0.018 |
| Placebo (n = 26) | 77.2 ± 22.5 | 75.5 ± 20.8 | 0.532 | |
| COMP, ng/mL | ||||
| Cucumber extract (n = 29) | 28.2 ± 17.9 | 31.0 ± 18.7 | 0.493 | 0.896 |
| Placebo (n = 26) | 27.6 ± 12.7 | 29.6 ± 20.0 | 0.638 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Piñero, S.; Muñoz-Carrillo, J.C.; Victoria-Montesinos, D.; García-Muñoz, A.M.; Ávila-Gandía, V.; López-Román, F.J. Effectiveness of a Cucumber Extract Supplement on Articular Pain in Patients with Knee Osteoarthritis: A Randomized Double-Blind Controlled Clinical Trial. Appl. Sci. 2023, 13, 485. https://doi.org/10.3390/app13010485
Pérez-Piñero S, Muñoz-Carrillo JC, Victoria-Montesinos D, García-Muñoz AM, Ávila-Gandía V, López-Román FJ. Effectiveness of a Cucumber Extract Supplement on Articular Pain in Patients with Knee Osteoarthritis: A Randomized Double-Blind Controlled Clinical Trial. Applied Sciences. 2023; 13(1):485. https://doi.org/10.3390/app13010485
Chicago/Turabian StylePérez-Piñero, Silvia, Juan Carlos Muñoz-Carrillo, Desirée Victoria-Montesinos, Ana María García-Muñoz, Vicente Ávila-Gandía, and Francisco Javier López-Román. 2023. "Effectiveness of a Cucumber Extract Supplement on Articular Pain in Patients with Knee Osteoarthritis: A Randomized Double-Blind Controlled Clinical Trial" Applied Sciences 13, no. 1: 485. https://doi.org/10.3390/app13010485
APA StylePérez-Piñero, S., Muñoz-Carrillo, J. C., Victoria-Montesinos, D., García-Muñoz, A. M., Ávila-Gandía, V., & López-Román, F. J. (2023). Effectiveness of a Cucumber Extract Supplement on Articular Pain in Patients with Knee Osteoarthritis: A Randomized Double-Blind Controlled Clinical Trial. Applied Sciences, 13(1), 485. https://doi.org/10.3390/app13010485