

Reverse Linear Neuro Periodization Model for Rehabilitation After Arthroscopic Rotator Cuff Repair: A Narrative Review

 ,
,  , , and
, , and 
Abstract
1. Introduction
2. Methodology for Conducting the Narrative Review
3. Postoperative Rehabilitation Periodization Models
4. Neurocognitive Approach in Postoperative Rotator Cuff Repair Rehabilitation
5. Application of Reverse Linear Neuro Periodization Model in Postoperative Rotator Cuff Repair Rehabilitation
6. Clinical Practices of Reverse Linear Neuro Periodization Model in Postoperative Rotator Cuff Repair Rehabilitation
6.1. Phase 1: Immediate Postoperative Phase (Weeks 1–2)
- -
- Passive Range of Motion (ROM): Gentle passive movements, such as pendulums and assisted shoulder elevation, can prevent stiffness and maintain initial joint mobility. Clinicians should guide patients to perform pendulum exercises by letting the arm hang and gently swinging it in small circular motions, ensuring no active muscle engagement around the shoulder.
- -
- Mental Visualization and Cognitive Interference Tasks: Neurocognitive engagement can start with guided mental visualization. Patients visualize moving their shoulder in specific patterns, such as flexion or rotation, engaging motor planning areas in the brain. Cognitive interference tasks, like responding to sounds while mentally focusing on shoulder stability, can reinforce neural connections. For example, a clinician may ask the patient to focus on shoulder stabilization while listening for specific auditory cues, initiating early neural adaptation.
6.2. Criteria to Progress to Phase 2
- Pain and inflammation are controlled or significantly reduced.
- The patient demonstrates the ability to perform passive range-of-motion exercises (e.g., pendulum exercises) without exacerbating symptoms.
- No signs of complications, such as infection or increased swelling.
- Maintenance of joint integrity without signs of repair compromise.
6.3. Phase 2: Intermediate Postoperative Phase (Weeks 3–6)
- -
- Active-Assisted Movements: Active-assisted exercises, like wall slides, involve the patient using their non-affected arm or a therapist’s assistance to guide the shoulder through gentle motions without full muscle engagement. Wall slides encourage patients to slowly slide their hand up a wall, promoting gradual shoulder elevation in a controlled manner.
- -
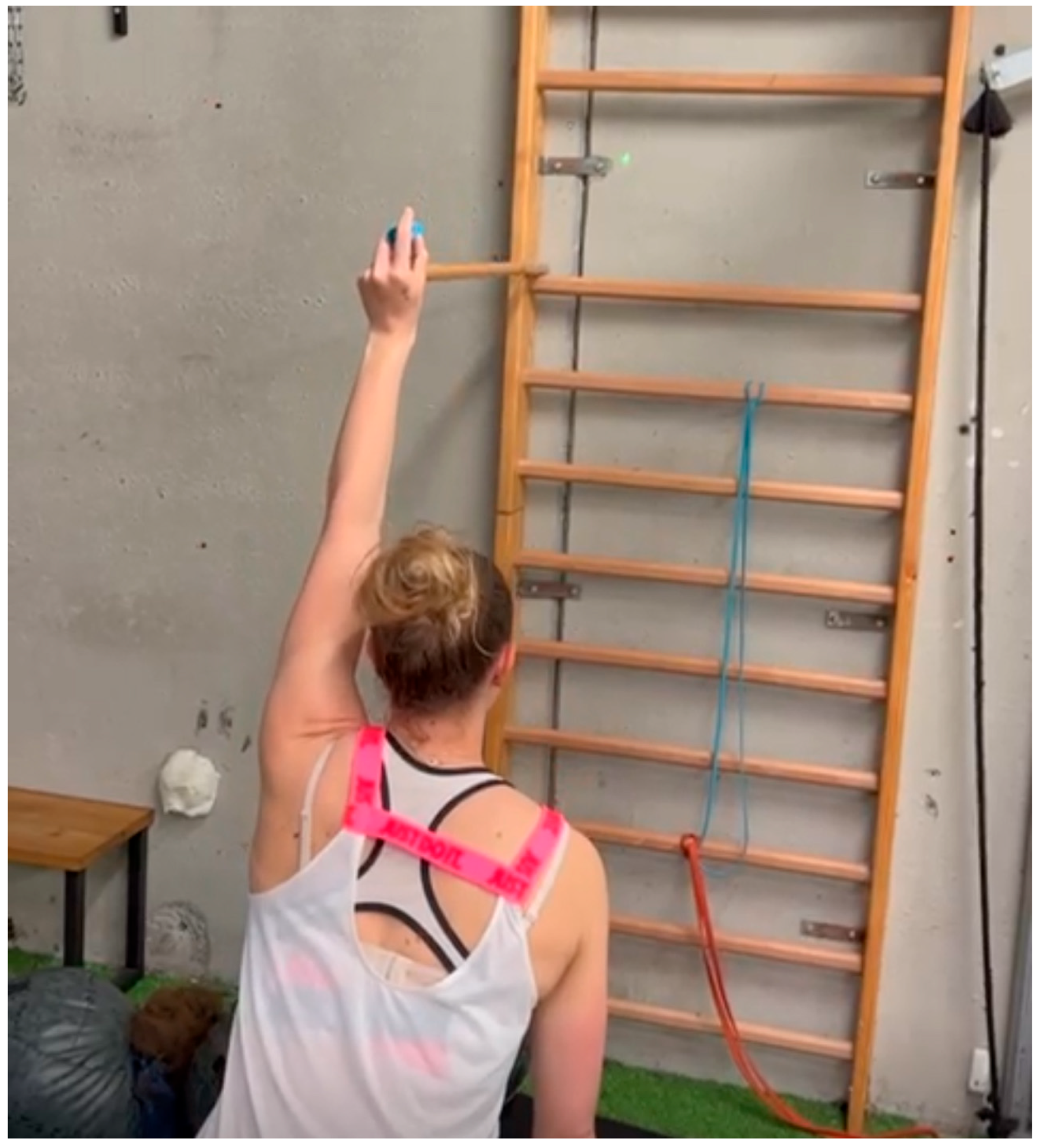
- Laser Pointer Exercises for Proprioception: Clinicians can attach a laser pointer to the patient’s hand and ask them to trace shapes or follow a target on the wall. For example, the patient can practice drawing circles or squares with the laser, enhancing their spatial awareness, control, and proprioceptive feedback as they refine movements (Figure 1).
- -
- Stroboscopic Glasses for Reaction and Balance: Stroboscopic glasses intermittently block vision, forcing the patient to rely on proprioceptive feedback. Patients wearing these glasses can perform seated or standing shoulder exercises, like shoulder flexion or holding a position against light resistance, while managing the visual disruption, and improving sensory processing and coordination.
6.4. Criteria to Progress to Phase 3
- The patient demonstrates tolerance for active-assisted movements with minimal or no pain.
- Improved proprioception and neuromuscular control during basic tasks (e.g., wall slides and laser pointer exercises).
- Full passive range of motion achieved within safe limits for the surgical repair.
- No swelling or irritation following exercises, indicating stability of healing tissue.
6.5. Phase 3: Active Range of Motion and Strengthening Phase (Weeks 6–12)
- -
- Active Shoulder Elevation and Rotation: Patients begin active movements such as shoulder elevation, external rotation, and gentle abduction within a pain-free range. Exercises are typically performed in a supported or supine position initially (e.g., lying down to avoid gravity’s impact), then progressing to seated or standing as tolerance improves.
- -
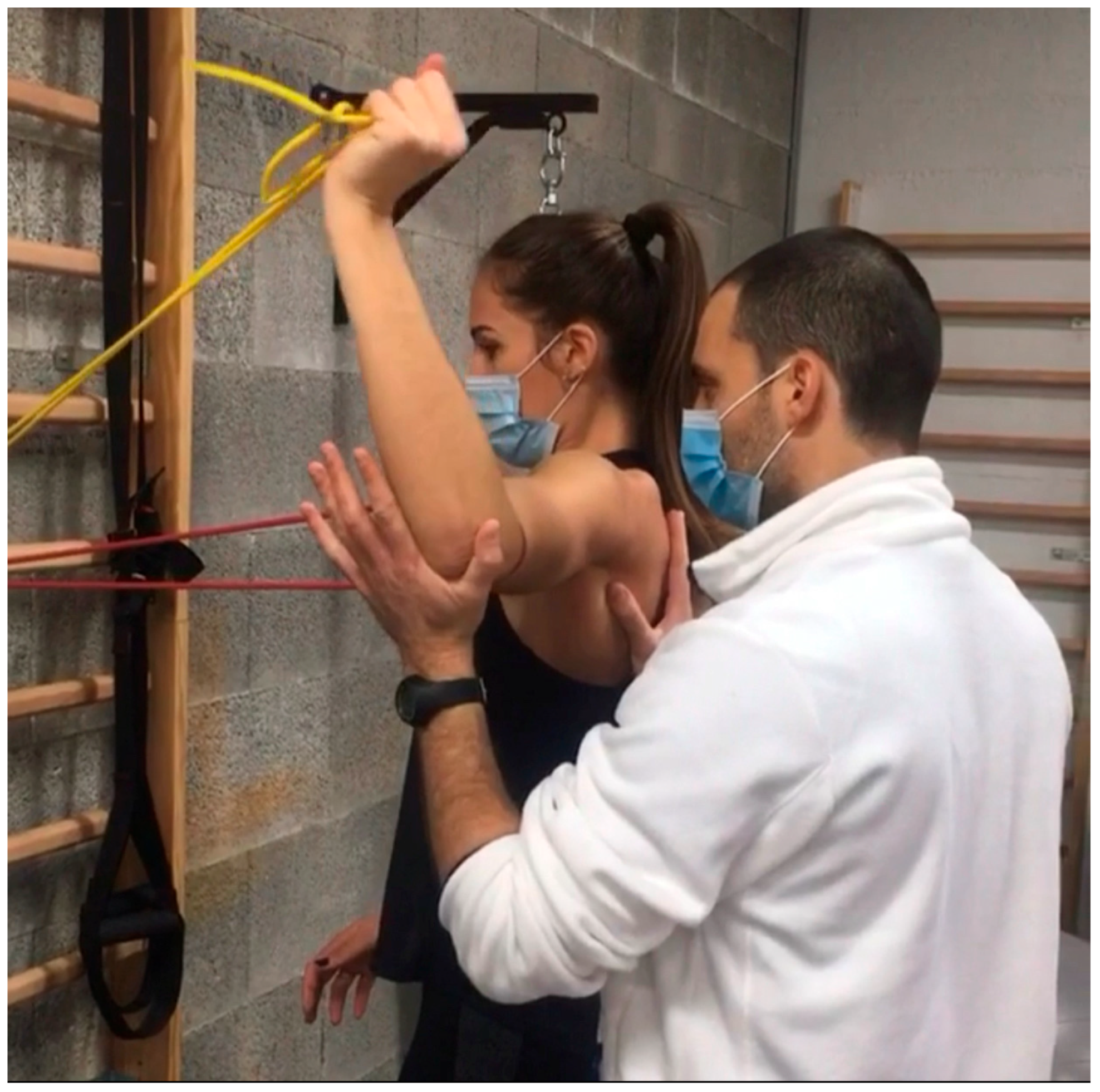
- Resistance Band Exercises: Introducing low-resistance bands provides safe, gradual strengthening. Patients can perform seated rows, external rotations, or internal rotations with light bands, allowing for incremental load. For instance, a clinician might start with a resistance band around the hands, guiding the patient through a controlled external rotation against mild resistance to strengthen stabilizing muscles (Figure 2).
- -
- VR-Based Neurocognitive Drills: Virtual reality can simulate interactive environments that promote shoulder engagement while challenging reaction times and hand–eye coordination. For example, a VR scenario could involve a virtual game where patients use small shoulder movements to “catch” or “block” objects on the screen, requiring accurate control and reaction to dynamic stimuli.
6.6. Criteria to Progress to Phase 4
- The patient achieves a full active range of motion without compensatory movements or pain.
- Ability to perform light resistance exercises (e.g., resistance bands) with proper form and control.
- Demonstrates stable shoulder movement during VR drills or other proprioceptive tasks.
- Improved functional use of the shoulder in daily activities without discomfort.
6.7. Phase 4: Initial Strengthening Phase (Weeks 12–18)
- -
- Strengthening with Resistance: More resistance is gradually added through exercises like shoulder flexion, side-lying external rotation, and wall push-ups. Side-lying external rotation, performed with a light dumbbell, helps activate the rotator cuff muscles. Wall push-ups with hands at shoulder height allow patients to engage core stability and shoulder strength while reducing load compared to standard push-ups [38].
- -
- Dual-Task Training for Coordination: Patients perform physical tasks, such as catching a ball, while engaging in a mental task like counting backward or solving simple math problems. For instance, a clinician may toss a ball to the patient at intervals while asking them to count by sevens, enhancing coordination and cognitive processing under simultaneous tasks [39].
- -
- Perturbation Training: In perturbation exercises, the clinician applies gentle, unpredictable forces to the patient’s arm while they hold it in a specific position (e.g., shoulder at 90 degrees of abduction). This helps the patient develop reflexive stability and quick adjustments, essential for joint control in daily and athletic activities (Figure 3).
6.8. Criteria to Progress to Phase 5
- The patient consistently performs resistance and strengthening exercises without signs of fatigue, instability, or pain.
- Demonstrates adequate strength and endurance to engage in dual-task and perturbation training with coordination and stability.
- Full participation in daily activities and non-strenuous physical tasks without limitations.
- Sufficient neuromuscular control to handle increased load and dynamic exercises safely.
6.9. Phase 5: Advanced Strengthening and Return-to-Sport Phase (Weeks 18–26)
- -
- Dynamic Strength Training: Using resistance bands, free weights, and Proprioceptive Neuromuscular Facilitation patterns, clinicians guide patients through complex movements, like diagonal shoulder patterns, that activate multiple muscle groups. Push-up progressions can advance from wall push-ups to floor push-ups, depending on the patient’s strength (Figure 3).
- -
- Advanced VR Simulations for Sport-Specific Drills: For athletes, VR can simulate sport-specific scenarios, like a tennis serve or basketball shot. For example, a tennis player may practice the mechanics of a serve in a VR environment, reacting to virtual cues and simulating real-time decisions. This helps train sport-specific coordination and cognitive engagement (Figure 4).
- -
- Stroboscopic and Dual-Task Challenges: Stroboscopic glasses and dual-task training can be combined for agility and neurocognitive adaptability. For instance, patients can perform a Fitlight reaction drill, using the glasses to create intermittent vision while touching lights that appear randomly. This exercise strengthens focus, reaction speed, and adaptability, key elements for athletic performance (Figure 5).
6.10. Criteria to Progress to Unrestricted Activity
- Symmetrical shoulder strength and range of motion compared to the non-injured side.
- Successful execution of sport-specific or work-specific tasks in controlled environments (e.g., VR simulations, agility drills).
- Demonstrates confidence and readiness for unrestricted activity based on clinical evaluation and patient-reported outcomes.
- Absence of pain, instability, or functional limitations during simulated real-life movements or high-intensity tasks.
7. Future Perspectives
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Minagawa, H.; Yamamoto, N.; Abe, H.; Fukuda, M.; Seki, N.; Kikuchi, K.; Kijima, H.; Itoi, E. Prevalence of Symptomatic and Asymptomatic Rotator Cuff Tears in the General Population: From Mass-Screening in One Village. J. Orthop. 2013, 10, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Colvin, A.C.; Egorova, N.; Harrison, A.K.; Moskowitz, A.; Flatow, E.L. National Trends in Rotator Cuff Repair. J. Bone Jt. Surg. 2012, 94, 227–233. [Google Scholar] [CrossRef]
- Longo, U.G.; Risi Ambrogioni, L.; Candela, V.; Berton, A.; Carnevale, A.; Schena, E.; Denaro, V. Conservative versus Surgical Management for Patients with Rotator Cuff Tears: A Systematic Review and META-Analysis. BMC Musculoskelet. Disord. 2021, 22, 50. [Google Scholar] [CrossRef]
- Corban, J.; Shah, S.; Ramappa, A.J. Current Evidence Based Recommendations on Rehabilitation Following Arthroscopic Shoulder Surgery: Rotator Cuff, Instability, Superior Labral Pathology, and Adhesive Capsulitis. Curr. Rev. Musculoskelet. Med. 2024, 17, 247–257. [Google Scholar] [CrossRef]
- Hutchison, M.; Comper, P.; Mainwaring, L.; Richards, D. The Influence of Musculoskeletal Injury on Cognition: Implications for Concussion Research. Am. J. Sports Med. 2011, 39, 2331–2337. [Google Scholar] [CrossRef] [PubMed]
- Kakavas, G.; Forelli, F.; Malliaropoulos, N.; Hewett, T.E.; Tsaklis, P. Periodization in Anterior Cruciate Ligament Rehabilitation: New Framework Versus Old Model? A Clinical Commentary. Int. J. Sports Phys. Ther. 2023, 18, 541–546. [Google Scholar] [CrossRef]
- Killian, S.E.; Cavanaugh, J.T. Rehabilitation Guidelines After Rotator Cuff Repair. Tech. Shoulder Elb. Surg. 2014, 15, 8–12. [Google Scholar] [CrossRef]
- Matlak, S.; Andrews, A.; Looney, A.; Tepper, K.B. Postoperative Rehabilitation of Rotator Cuff Repair: A Systematic Review. Sports Med. Arthrosc. Rev. 2021, 29, 119–129. [Google Scholar] [CrossRef]
- Jung, C.; Tepohl, L.; Tholen, R.; Beitzel, K.; Buchmann, S.; Gottfried, T.; Grim, C.; Mauch, B.; Krischak, G.; Ortmann, H.; et al. Rehabilitation Following Rotator Cuff Repair. Obere Extrem. 2018, 13, 45–61. [Google Scholar] [CrossRef]
- Paoloni, M.; Bernetti, A.; Santilli, V.; Gumina, S. Rehabilitation After Rotator Cuff Repair. In Rotator Cuff Tear; Gumina, S., Ed.; Springer International Publishing: Cham, Switzerland, 2017; pp. 369–380. ISBN 978-3-319-33354-0. [Google Scholar]
- Thigpen, C.A.; Shaffer, M.A.; Gaunt, B.W.; Leggin, B.G.; Williams, G.R.; Wilcox, R.B. The American Society of Shoulder and Elbow Therapists’ Consensus Statement on Rehabilitation Following Arthroscopic Rotator Cuff Repair. J. Shoulder Elb. Surg. 2016, 25, 521–535. [Google Scholar] [CrossRef]
- Kibler, W.B.; Sciascia, A. Rehabilitation Following Rotator Cuff Repair. In Shoulder Surgery Rehabilitation; Di Giacomo, G., Bellachioma, S., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 165–182. ISBN 978-3-319-24854-7. [Google Scholar]
- Belley, A.F.; Mercier, C.; Bastien, M.; Léonard, G.; Gaudreault, N.; Roy, J.-S. Anodal Transcranial Direct-Current Stimulation to Enhance Rehabilitation in Individuals with Rotator Cuff Tendinopathy: A Triple-Blind Randomized Controlled Trial. J. Orthop. Sports Phys. Ther. 2018, 48, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Parel, I.; Candoli, V.; Filippi, M.V.; Padolino, A.; Merolla, G.; Sanniti, S.; Galassi, R.; Paladini, P.; Cutti, A.G. Shoulder Rehabilitation Exercises with Kinematic Biofeedback After Arthroscopic Rotator Cuff Repair: Protocol for a New Integrated Rehabilitation Program. JMIR Res. Protoc. 2023, 12, e35757. [Google Scholar] [CrossRef] [PubMed]
- Myer, G.D.; Paterno, M.V.; Ford, K.R.; Quatman, C.E.; Hewett, T.E. Rehabilitation After Anterior Cruciate Ligament Reconstruction: Criteria-Based Progression Through the Return-to-Sport Phase. J. Orthop. Sports Phys. Ther. 2006, 36, 385–402. [Google Scholar] [CrossRef]
- Jerosch, J.; Wüstner, P. Effekt Eines Sensomotorischen Trainingsprogramms bei Patienten mit Subakromialem Schmerzsyndrom. Der Unfallchirurg 2002, 105, 36–43. [Google Scholar] [CrossRef]
- Forelli, F.; Riera, J.; Marine, P.; Gaspar, M.; Memain, G.; Miraglia, N.; Nielsen-Le Roux, M.; Bouzekraoui Alaoui, I.; Kakavas, G.; Hewett, T.E.; et al. Implementing Velocity-Based Training to Optimize Return to Sprint After Anterior Cruciate Ligament Reconstruction in Soccer Players: A Clinical Commentary. Int. J. Sports Phys. Ther. 2024, 19, 355–365. [Google Scholar] [CrossRef]
- Forelli, F.; Moiroux-Sahraoui, A.; Nielsen-Le Roux, M.; Miraglia, N.; Gaspar, M.; Stergiou, M.; Bjerregaard, A.; Mazeas, J.; Douryang, M. Stay in the Game: Comprehensive Approaches to Decrease the Risk of Sports Injuries. Cureus 2024, 16, e76461. [Google Scholar] [CrossRef]
- Stergiou, M.; Calvo, A.L.; Forelli, F. Effectiveness of Neuromuscular Training in Preventing Lower Limb Soccer Injuries: A Systematic Review and Meta-Analysis. J. Clin. Med. 2025, 14, 1714. [Google Scholar] [CrossRef]
- Paolucci, T.; Agostini, F.; Conti, M.; Cazzolla, S.; Mussomeli, E.; Santilli, G.; Poso, F.; Bernetti, A.; Paoloni, M.; Mangone, M. Comparison of Early versus Traditional Rehabilitation Protocol after Rotator Cuff Repair: An Umbrella-Review. J. Clin. Med. 2023, 12, 6743. [Google Scholar] [CrossRef] [PubMed]
- Nikolaidou, O.; Migkou, S.; Karampalis, C. Rehabilitation after Rotator Cuff Repair. Open Orthop. J. 2017, 11, 154–162. [Google Scholar] [CrossRef]
- Moiroux-Sahraoui, A.; Forelli, F.; Mazeas, J.; Rambaud, A.J.; Bjerregaard, A.; Riera, J. Quadriceps Activation After Anterior Cruciate Ligament Reconstruction: The Early Bird Gets the Worm! Int. J. Sports Phys. Ther. 2024, 19, 1044–1051. [Google Scholar] [CrossRef]
- Williams, T.D.; Tolusso, D.V.; Fedewa, M.V.; Esco, M.R. Comparison of Periodized and Non-Periodized Resistance Training on Maximal Strength: A Meta-Analysis. Sports Med. 2017, 47, 2083–2100. [Google Scholar] [CrossRef] [PubMed]
- Turner, A. The Science and Practice of Periodization: A Brief Review. Strength Cond. J. 2011, 33, 34–46. [Google Scholar] [CrossRef]
- Grgic, J.; Mikulic, P.; Podnar, H.; Pedisic, Z. Effects of Linear and Daily Undulating Periodized Resistance Training Programs on Measures of Muscle Hypertrophy: A Systematic Review and Meta-Analysis. PeerJ 2017, 5, e3695. [Google Scholar] [CrossRef]
- Rhea, M.R.; Alderman, B.L. A Meta-Analysis of Periodized versus Nonperiodized Strength and Power Training Programs. Res. Q. Exerc. Sport 2004, 75, 413–422. [Google Scholar] [CrossRef]
- Harries, S.K.; Lubans, D.R.; Callister, R. Systematic Review and Meta-Analysis of Linear and Undulating Periodized Resistance Training Programs on Muscular Strength. J. Strength Cond. Res. 2015, 29, 1113–1125. [Google Scholar] [CrossRef] [PubMed]
- Moesgaard, L.; Beck, M.M.; Christiansen, L.; Aagaard, P.; Lundbye-Jensen, J. Effects of Periodization on Strength and Muscle Hypertrophy in Volume-Equated Resistance Training Programs: A Systematic Review and Meta-Analysis. Sports Med. 2022, 52, 1647–1666. [Google Scholar] [CrossRef]
- Baumeister, J.; Reinecke, K.; Weiss, M. Changed Cortical Activity after Anterior Cruciate Ligament Reconstruction in a Joint Position Paradigm: An EEG Study: ACL and Cortical Activity. Scand. J. Med. Sci. Sports 2007, 18, 473–484. [Google Scholar] [CrossRef]
- Houck, D.A.; Kraeutler, M.J.; Schuette, H.B.; McCarty, E.C.; Bravman, J.T. Early Versus Delayed Motion After Rotator Cuff Repair: A Systematic Review of Overlapping Meta-Analyses. Am. J. Sports Med. 2017, 45, 2911–2915. [Google Scholar] [CrossRef]
- Kakavas, G.; Malliaropoulos, N.; Bikos, G.; Pruna, R.; Valle, X.; Tsaklis, P.; Maffulli, N. Periodization in Anterior Cruciate Ligament Rehabilitation: A Novel Framework. Med. Princ. Pract. 2021, 30, 101–108. [Google Scholar] [CrossRef]
- Coda, R.G.; Cheema, S.G.; Hermanns, C.A.; Tarakemeh, A.; Vopat, M.L.; Kramer, M.; Schroeppel, J.P.; Mullen, S.; Vopat, B.G. A Review of Online Rehabilitation Protocols Designated for Rotator Cuff Repairs. Arthrosc. Sports Med. Rehabil. 2020, 2, e277–e288. [Google Scholar] [CrossRef]
- Doiron-Cadrin, P.; Lafrance, S.; Saulnier, M.; Cournoyer, É.; Roy, J.-S.; Dyer, J.-O.; Frémont, P.; Dionne, C.; MacDermid, J.C.; Tousignant, M.; et al. Shoulder Rotator Cuff Disorders: A Systematic Review of Clinical Practice Guidelines and Semantic Analyses of Recommendations. Arch. Phys. Med. Rehabil. 2020, 101, 1233–1242. [Google Scholar] [CrossRef] [PubMed]
- Ezell, D.J.; Malcarney, H.L. Rotator Cuff Repair Rehabilitation Considerations and Respective Guidelines: A Narrative Review. JSES Rev. Rep. Tech. 2021, 1, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Risi Ambrogioni, L.; Berton, A.; Candela, V.; Carnevale, A.; Schena, E.; Gugliemelli, E.; Denaro, V. Physical Therapy and Precision Rehabilitation in Shoulder Rotator Cuff Disease. Int. Orthop. 2020, 44, 893–903. [Google Scholar] [CrossRef]
- Longo, U.G.; Risi Ambrogioni, L.; Berton, A.; Candela, V.; Migliorini, F.; Carnevale, A.; Schena, E.; Nazarian, A.; DeAngelis, J.; Denaro, V. Conservative versus Accelerated Rehabilitation after Rotator Cuff Repair: A Systematic Review and Meta-Analysis. BMC Musculoskelet. Disord. 2021, 22, 637. [Google Scholar] [CrossRef]
- Pasculli, R.M.; Bowers, R.L. Evidence-Based Management of Rotator Cuff Tears (Acute and Chronic). Curr. Phys. Med. Rehabil. Rep. 2022, 10, 239–247. [Google Scholar] [CrossRef]
- Jang, J.-H.; Oh, J.-S. Changes in Shoulder External Rotator Muscle Activity during Shoulder External Rotation in Various Arm Positions in the Sagittal Plane. J. Phys. Ther. Sci. 2014, 26, 135–137. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, M.D.M.; Maduro, P.A.; Rios, P.M.B.; Nascimento, L.D.S.; Silva, C.N.; Kliegel, M.; Ihle, A. Effects of 12 Weeks of Physical-Cognitive Dual-Task Training on Executive Functions, Depression, Sleep Quality, and Quality of Life in Older Adult Women: A Randomized Pilot Study. Sustainability 2022, 15, 97. [Google Scholar] [CrossRef]
- van der Meijden, O.A.; Westgard, P.; Chandler, Z.; Gaskill, T.R.; Kokmeyer, D.; Millett, P.J. Rehabilitation after Arthroscopic Rotator Cuff Repair: Current Concepts Review and Evidence-Based Guidelines. Int. J. Sports Phys. Ther. 2012, 7, 197–218. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Objective | Exercises | Description |
|---|---|---|
| Protect the repair, reduce pain and inflammation | Passive Range of Motion | Gentle pendulum exercises, assisted shoulder elevation; passive movements only to prevent stiffness and maintain initial joint mobility without stressing the repair. |
| Neuromuscular re-education | Mental Visualization | Patient visualizes shoulder movements (e.g., flexion, rotation) to engage motor planning and neural pathways, guided by the clinician. |
| Stimulate early neural adaptation | Cognitive Interference Tasks | Patient responds to auditory cues while focusing on shoulder stability, initiating neural connections without active physical movement. |
| Objective | Exercises | Description |
|---|---|---|
| Regain controlled mobility | Active-Assisted Movements | Wall slides and shoulder abduction with assistance; patient uses their non-affected arm or a therapist’s support to maintain gentle motion. |
| Enhance proprioception | Laser Pointer Exercises | Patient traces shapes on a wall using a laser pointer attached to their hand, improving control, proprioception, and spatial awareness. |
| Improve sensory processing | Stroboscopic Glasses Exercises | With stroboscopic glasses, patient performs shoulder flexion or static holds, adapting to intermittent visual disruption to strengthen reaction time and coordination. |
| Objective | Exercises | Description |
|---|---|---|
| Build active ROM and stability | Active Shoulder Elevation and Rotation | Gradual shoulder movements, such as elevation and rotation, in a supported position (e.g., supine), progressing to seated/standing as patient tolerates. |
| Introduce gentle resistance | Resistance Band Exercises | Exercises like seated rows and shoulder external rotation with light resistance bands to safely engage stabilizing shoulder muscles. |
| Enhance hand–eye coordination | VR-Based Neurocognitive Drills | Patient engages with interactive VR scenarios, such as a virtual game requiring small shoulder movements to “catch” or “block” objects, challenging reaction time and control. |
| Objective | Exercises | Description |
|---|---|---|
| Increase strength and endurance | Strengthening with Resistance | Progressive resistance added through exercises like wall push-ups, shoulder flexion with dumbbells, and side-lying external rotation to engage and strengthen shoulder muscles. |
| Enhance cognitive processing | Dual-Task Training | Patient performs a physical task, like catching a ball, while completing a cognitive task, such as counting backward, reinforcing coordination and cognitive focus. |
| Develop reflexive stability | Perturbation Training | Clinician applies unpredictable forces to the patient’s arm while it is in a static position, training the patient to react and stabilize the shoulder quickly. |
| Objective | Exercises | Description |
|---|---|---|
| Maximize functional strength | Dynamic Strength Training | Exercises like diagonal shoulder patterns with resistance bands, free weights, and PNF patterns activate multiple muscle groups in functional movements. |
| Simulate sport-specific movements | Advanced VR Simulations | For athletes, VR simulates a sports environment (e.g., tennis serve or basketball shot), helping the patient practice specific movements and coordination for return to sport. |
| Enhance reaction and agility | Stroboscopic and Dual-Task Challenges | Combining stroboscopic glasses with dual-task drills like Fitlight exercises (touching lights with intermittent vision), reinforces agility, speed, and cognitive adaptability. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kakavas, G.; Brilakis, E.; Papatzikou, M.; Malliaropoulos, N.; Mazeas, J.; Forelli, F. Reverse Linear Neuro Periodization Model for Rehabilitation After Arthroscopic Rotator Cuff Repair: A Narrative Review. Clin. Pract. 2025, 15, 105. https://doi.org/10.3390/clinpract15060105
Kakavas G, Brilakis E, Papatzikou M, Malliaropoulos N, Mazeas J, Forelli F. Reverse Linear Neuro Periodization Model for Rehabilitation After Arthroscopic Rotator Cuff Repair: A Narrative Review. Clinics and Practice. 2025; 15(6):105. https://doi.org/10.3390/clinpract15060105
Chicago/Turabian StyleKakavas, Georgios, Emmanouil Brilakis, Maria Papatzikou, Nikolaos Malliaropoulos, Jean Mazeas, and Florian Forelli. 2025. "Reverse Linear Neuro Periodization Model for Rehabilitation After Arthroscopic Rotator Cuff Repair: A Narrative Review" Clinics and Practice 15, no. 6: 105. https://doi.org/10.3390/clinpract15060105
APA StyleKakavas, G., Brilakis, E., Papatzikou, M., Malliaropoulos, N., Mazeas, J., & Forelli, F. (2025). Reverse Linear Neuro Periodization Model for Rehabilitation After Arthroscopic Rotator Cuff Repair: A Narrative Review. Clinics and Practice, 15(6), 105. https://doi.org/10.3390/clinpract15060105