1. Introduction
In dentistry, three main techniques are used to manufacture indirect composite restorations: direct, semi-direct, and indirect. Within these techniques, three production methods are available: conventional (CRC), milled (MRC), and printed (PRC). The quantity, scope, and location of the restoration determine the most appropriate technique for a given case [
1]. The use of direct composite resin as a permanent dental restorative material has significantly increased in recent years due to its aesthetic appeal, conservative preparation, and ability to bond to tooth structure [
2]. However, polymerization shrinkage during light curing is a known cause of adhesive and cohesive failures [
3,
4].
The indirect technique offers excellent occlusal and interproximal anatomy in large cavities. Additionally, due to the indirect nature of their production process, the polymerization shrinkage is restricted to the thin layer of resin cement, leading to reduced polymerization stress between the restoration and the tooth in comparison with direct techniques [
5]. However, indirect restorations require at least two appointments: one for preparation and another for final placement. The semi-direct technique combines elements of both direct and indirect approaches, where the resin is shaped in a model, light-cured, removed for extra-oral finishing and polishing, and then adhesively cemented [
6].
Although composite resin materials used for semi-direct and indirect techniques may share similar components and behavior, they can be processed differently. Today, it is possible to produce permanent indirect composite restorations using the traditional incremental technique or digital workflow with the aid of Computer-Aided Design/Computer-Aided Manufacturing (CAD/CAM) through milling or three-dimensional (3D) printing.
Tetric CAD (Ivoclar, Schaan, Liechtenstein) is an example of a CAD/CAM resin block used for permanent milled resin composite (MRC) restorations. Unlike conventional resin composites, MRCs do not undergo polymerization shrinkage within the tooth, reducing stress and the potential for leakage [
7]. Indirect restorations in MRC offer better contouring of proximal surfaces, improved fracture resistance, and enhanced biocompatibility. However, these benefits come with increased costs and time, and MRCs also present a low potential for repair [
7]. In contrast, Formlabs GmbH (Berlin, Germany) produces a 3D-printable composite resin (PRC) for manufacturing permanent restorations (Permanent Crown Resin). Since MRC production can result in up to 70% of material waste, 3D printing might represent a more sustainable method for producing indirect composite restorations (ICRs) [
8]. However, information about the mechanical properties of PRCs is limited, raising concerns about their long-term durability and reliability compared to materials used in established techniques [
8,
9].
Clearfill AP-X (Kuraray Noritake Dental Inc., Tokyo, Japan) is an example of a conventional micro-hybrid resin composite (CRC) used for direct and semi-direct restorations via the incremental technique. It is known for its aesthetic and acceptable mechanical properties, such as wear resistance and the ability to bond to tooth structure [
10,
11]. Due to the presence of bisphenol A-glycidyl methacrylate in its composition, Clearfill AP-X exhibits high viscosity, low volatility, and reduced polymerization shrinkage [
12]. However, low-certainty evidence suggests a much higher risk of secondary caries and almost double the failure rate compared to amalgam restorations [
13].
One important factor for the longevity of composite restorations is their ability to withstand masticatory forces [
14]. In particular, the fracture load of restoration is a critical measure of its strength and ability to resist stress [
14]. Previous studies have investigated the mechanical properties of composite resins, including their flexural strength, hardness, and wear resistance [
8,
15,
16,
17], and long-term clinical studies have shown acceptable performance [
15]. Despite that, the mechanical response of the bonded restoration is not always predictable solely based on the restoration stiffness, as the processing method and aging can also play a significant role [
18].
While numerous studies have evaluated the fracture load of milled composite resin restorations, limited research has focused on the fracture load of 3D-printed restorations [
19,
20,
21]. Given the increasing use of indirect composite restorations in clinical practice, it is essential to understand how different manufacturing methods contribute to the bonded fracture load and to identify potential areas for improvement. Therefore, this study aimed to evaluate the impact of manufacturing techniques on the fracture load of composite resin restorations after aging. The null hypothesis adopted was that there would be no difference in the fracture load of indirect resin composite restorations manufactured using different techniques, regardless of the aging procedure.
4. Discussion
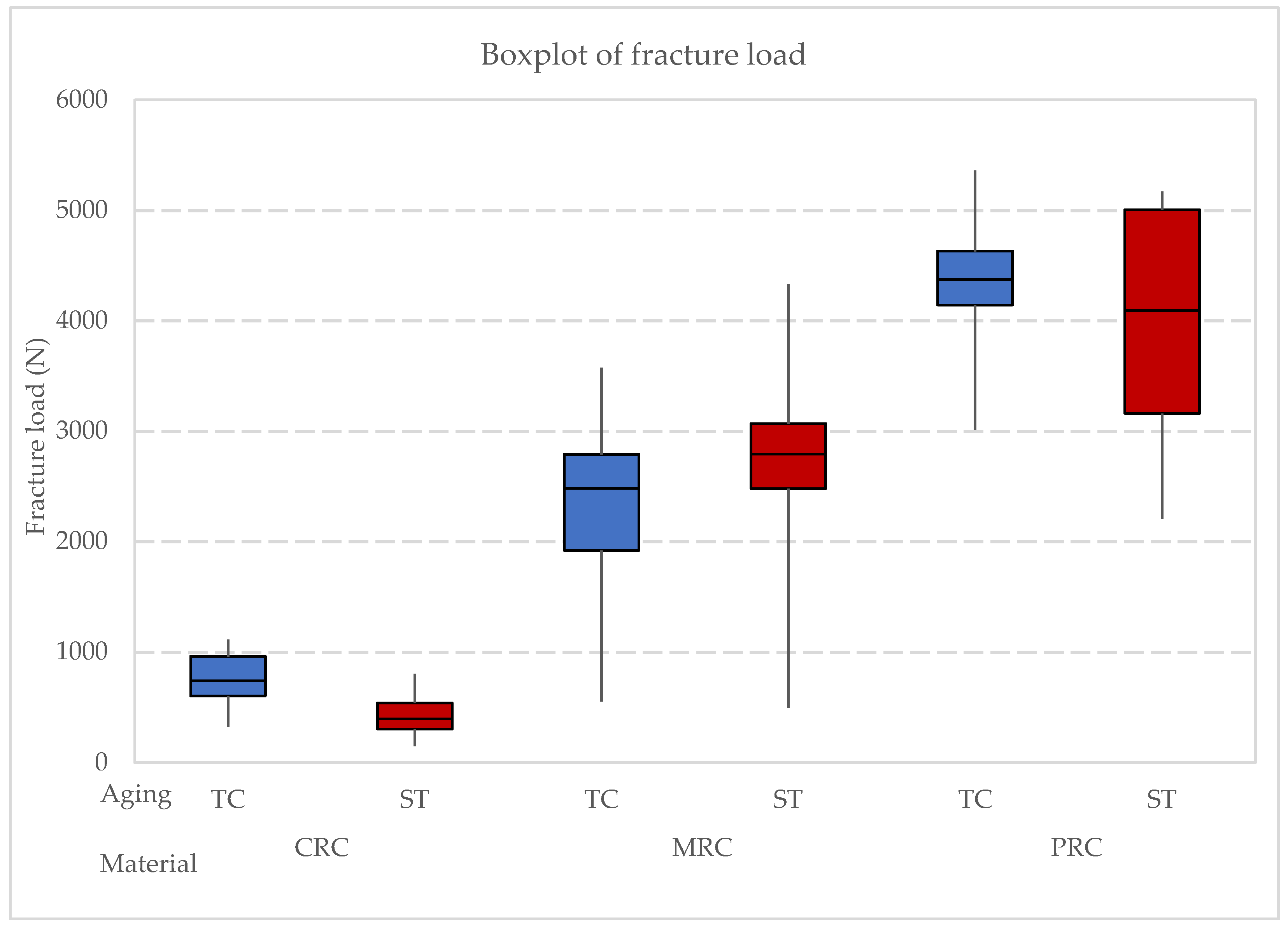
This study evaluated how different manufacturing techniques affect the fracture load of indirect composite restorations after simulated aging. The findings indicate that sandblasting the surface of the specimens as a pre-treatment before cementation increases surface roughness, thereby preparing the surface for bonding. Moreover, significant differences in fracture load among the materials were observed, regardless of the aging protocol, leading to the rejection of the study’s null hypothesis. This finding confirms the different performance between materials and the lack of influence of the aging protocols.
According to the manufacturer, the evaluated milled composite (MRC) has a fracture load of 2600 N, which aligns with the data from this study. It was anticipated that MRC would exhibit the highest fracture load, followed by conventional resin composite (CRC) and then by printed resin composite (PRC), based on their reported flexural strength values. Contrary to expectations, PRC demonstrated the highest fracture load, followed by MRC and CRC. This might be partially explained by the effects of sandblasting, which increases surface roughness. Laboratory investigations suggest that rough surfaces can negatively impact mechanical characteristics [
35,
36]. Research by Yoshihara et al. [
37] indicates that minor surface imperfections on roughened surfaces may develop into initial cracks under compressive loads, leading to catastrophic failure due to non-uniform stress distribution [
38,
39,
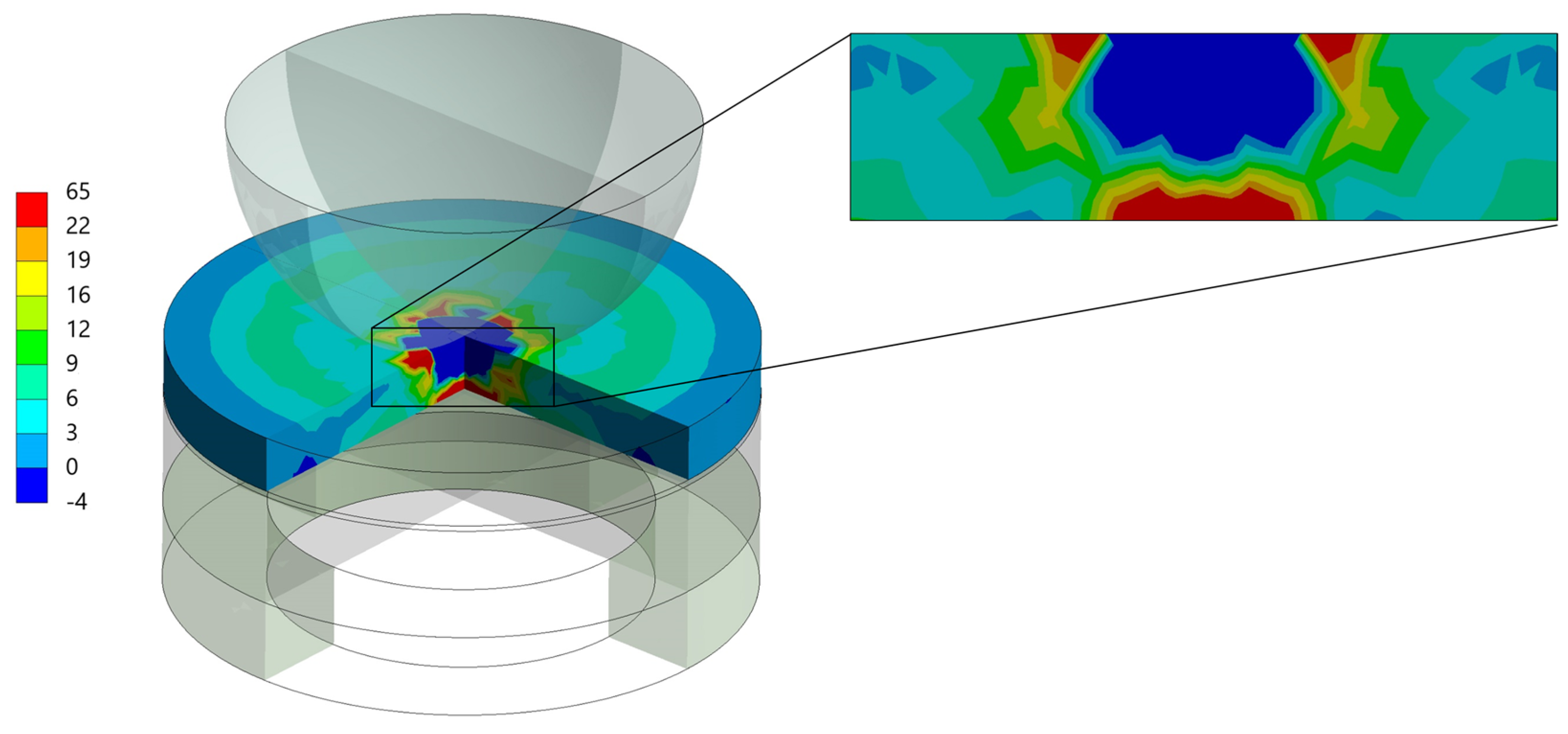
40]. This explains the decreased fracture load observed in CRC and MRC. However, the high fracture load of PRC, despite its increased surface roughness, requires further investigation. In addition, finite element analysis (FEA) suggests that while the stress magnitude in the restoration was close to the manufacturer’s reported strength, the stress in the cement layer was very high in MRC and PRC, indicating potential debonding before material fracture.
Despite not showing a significant difference between aging protocols, it is noteworthy that 96.7% of CRC specimens survived water storage, and 90% of specimens subjected to thermocycling also survived. CRC did not experience any bonding failures after thermocycling, while MRC and PRC had one and three debonded specimens, respectively. The debonding in PRCs could be attributed to polymerization stress or lack of sufficient bond strength. However, no literature is available on the polymerization rate of this or similar PRC materials, suggesting a need for further research.
Temperature fluctuations and complex chewing pressures in the oral cavity significantly impact the flexural stress in composite restorations, leading to material fatigue [
41,
42]. This underscores the importance of simulating fatigue in studies of dental restoration materials. Water storage and thermocycling are standard procedures in dental research to simulate aging. Thermocycling, which involves exposing materials to extreme temperature changes over many cycles, is more indicative of real-life conditions than water storage [
43]. Studies have shown that thermocycling can reduce flexural strength and microhardness [
16,
44,
45], although some research, like that by de Oliveira et al. [
46], suggests that micro-hybrid resin composites maintain their hardness value despite thermocycling. This study did not observe significant changes in fracture load after water storage and 10,000 thermal cycles. According to Henderson et al. [
47], further research is needed to fully understand the effects of thermocycling on fracture load.
A recent scoping review highlighted that while 3D-printed composites hold promise, they currently fall short in hardness, flexural strength, and overall mechanical durability compared to traditional materials. Their performance as long-term permanent restorations remains inadequate [
18,
48]. Nevertheless, this study shows that 3D-printed composites can be viable for indirect restorations when properly cemented. Rosentritt et al. [
49] found that printed and milled permanent crowns exhibited acceptable mid-term performance and wear stability, with similar fracture forces. However, their study did not confirm that PRC had superior fracture forces compared to MRC.
Considering the dentin analog used in this study, it is important to acknowledge that no material perfectly replicates natural dentin. Epoxy filled with glass fibers (NEMA grade 10) is considered a suitable dentin analog, although it may have some differences [
50]. These differences are generally minor and may not significantly impact the performance of dental restorations [
50]. Thus, further exploration of factors such as flexural strength, water sorption, and material wear is essential for improving the longevity and reliability of indirect resin composite restorations. Enhanced understanding of fracture load can lead to the development of more effective materials and techniques for testing dental restorations.
In summary, the present study demonstrates the significant influence of manufacturing techniques on the fracture load of indirect composite restorations (ICRs), with 3D-printed resin composites (PRC) exhibiting adequate behavior. These findings align with previous research on the mechanical properties of 3D-printed dental materials, which highlighted the promising performance of high-filled 3D-printed resins [
51]. Interestingly, aging protocols, such as thermocycling and water storage, did not significantly impact fracture load in any group, suggesting the resilience of PRC under simulated oral conditions. These findings are consistent with studies evaluating the durability of 3D-printed restorations, which have shown that post-processing conditions like thermal aging may not critically compromise their mechanical integrity [
52,
53]. Additionally, finite element analysis reinforced the superior stress distribution in PRC, possibly contributing to its higher load-bearing capacity. These results suggest that 3D printing offers a viable alternative to conventional and milled methods, justifying further investigation into bond strength and surface treatment optimization for long-term clinical success [
52,
53,
54].



 ,
, 




{kind=link}
{kind=link}
{kind=link}