Abstract
Background: Cardiovascular diseases (CVDs) and associated risk factors are a growing concern in Cameroon. Physiotherapists (PTs) can play a crucial role in prevention and management. However, the extent of Cameroonian PT involvement in health promotion (HP) activities remains unclear. This study assessed Cameroonian physiotherapists’ current HP practices for people at risk of or with CVDs (pwCVDs). Methods: A cross-sectional survey was administered online to PTs practising in Cameroon. Results: Out of 181 PT responses, 95% reported providing a variety of HP activities, including weight management (74%), dietary advice (73%), physical activity (69%), smoking cessation (69%), stress management (61%), and sleep promotion (48%). While PTs were confident in lifestyle assessments, they felt less confident about sleep interventions. Strong beliefs, confidence, team support, and time allocation enhanced HP practice. However, preference for passive modalities, patient adherence issues, organisational challenges, role ambiguity among healthcare providers, inadequate training opportunities, and the absence of established guidelines for CVD prevention negatively affect HP practice. Conclusions: These findings highlight the challenges and opportunities for enhancing HP delivery within the physiotherapy profession in Cameroon. The findings are useful for future strategies by clinical practitioners and policy makers to address barriers and leverage facilitators effectively for scaling up HP initiatives in Cameroon.
1. Introduction
More than two-thirds of all global deaths are attributed to four chronic non-communicable diseases (CNCDs): cardiovascular disease (CVD), cancer, chronic lung diseases, and diabetes [1]. CVD is the leading cause of death globally, with an estimated 20.5 million deaths in 2021 [2], and accounts for 38% of all global premature deaths [1,3]. The burden of CVD is increasing, with over 80% of all global cases and deaths in low- and medium-income countries (LMICs) [3,4]. Although risk factors are similar globally, CVDs are increasing in LMICs due to changing lifestyles (Westernisation) and health behaviours, including physical inactivity, increased use of tobacco, poor nutrition, obesity, and harmful use of alcohol [5]. These, together with other medical risk factors such as hypertension, dyslipidaemia, and diabetes associated with limited resources for effective prevention and management, contribute to the escalating prevalence and mortality of CVDs in LMICs like Cameroon [6].
In Cameroon, CVDs and associated risk factors are on the rise. According to 2015 estimates, 30.8% of Cameroonian women lived with hypertension, compared with 27.0% for both genders in Africa and 20.1% globally [7], accounting for 41.3–54.5% of heart diseases in Cameroon [8,9]. CVD accounted for 10–16% of hospital admissions, with heart failure (38.5%), stroke (33.3%), and uncontrolled hypertension (22.4%) being the most common [9]. In 2012, 12% of total deaths in Cameroon were attributed to CVD [10]. On average, 43.8% of adult Cameroonian males use tobacco, compared to 36.1% globally. Additionally, 28.5% of adults are physically inactive compared to 27.5% globally [11]. A community-based cross-sectional study among adults reported poor awareness of CVDs and associated risk factors among participants [12]. The fragile health system, limited health promotion (HP), disease prevention policies, and implementation might contribute to the increasing prevalence of CVD risk factors [13]. In this work, we defined HP as any proactive measures to improve patients’ quality of life and health.
Most CVD risk factors are modifiable and can be prevented by addressing lifestyle changes such as tobacco use, unhealthy diet and obesity, harmful use of alcohol, poor stress management, physical inactivity, and poor sleep quality [14]. These risk factors can be reduced and prevented through relevant HP practices that enable people to increase control over and improve their health [15,16]. Physiotherapists (PTs) support patients with different conditions, including people at risk of developing or living with CVDs (pwCVDs) [17]. We defined pwCVDs as PT clients with lifestyle risk factors (smokers, alcohol use, and physical inactivity), medical risk factors (diabetes and hypertension), and diagnosed CVD (coronary artery disease and heart failure) [5]. PTs have regular/frequent opportunities to provide their clients with HP advice. As an informed non-medical profession, with health education, physical interventions, and exercise at the core of their practice [18,19], PTs can support management of these lifestyle-related conditions [20,21] using biopsychosocial and holistic approaches [22]. PTs may be an untapped resource for addressing the CVD epidemic in Cameroon, especially with the absence of specialised units and CVD prevention programmes [23]. PT-led health promotion (PLHP) refers to the involvement of PTs in designing, implementing, and guiding strategies and interventions that promote overall health, prevent injuries, and enhance well-being [24]. Personal, professional, institutional, and community policies and clinical guidelines have been shown to influence PT HP practice elsewhere [25,26,27]. The extent to which HP is covered in the curriculum and training of PTs and their HP practice in Cameroon is not known.
This study aimed to evaluate current PLHP practices and factors affecting PLHP for pwCVDs in Cameroon. The results may help develop and propose strategies and guidelines to improve PLHP practices and health outcomes for pwCVDs in the country.
2. Materials and Methods
2.1. Study Design
This study was designed as an online cross-sectional survey to assess HP practice by PTs and factors affecting PLHP activities in Cameroon.
2.2. Study Area
The study area included all private and public health facilities in Cameroon where PTs practise. Most PTs are concentrated in urban areas, with very few physiotherapy services delivered in rural areas [17].
Cameroon Society of Physiotherapy (CASP) assumes the governing and regulatory professional role for PTs in Cameroon [28]. CASP does not have complete data for PTs, but previous studies estimate between 250 and 400 PTs are practising in Cameroon [29,30].
2.3. Study Population
The study population included PTs who are 21 years and above, practising in Cameroon in any region, including public, private, or mission health facilities, and have at least two years of physiotherapy training and one year of clinical practice. Eligible participants had to be able to read and understand English.
2.4. Sample Size
A non-probability (convenience) sampling method was used for this survey due to challenges in determining the number of potential participants. CASP data on the number and characteristics of PTs in Cameroon is incomplete, with only 44 PTs having complete data. The existing literature estimates the number of PTs in Cameroon to vary between 250 and 400 [29,30]. Consequently, the minimum sample size estimated for this study was based on the sample size of 141 study participants used in a similar study in Nigeria [31].
2.5. Survey Instrument
The survey development was informed by previous studies [27,32] and guidelines in survey development [33]. The survey was designed to capture data in three main areas: Section A: demographics; Section B: current health promotion practice; and Section C: factors affecting HP practice at four ecological levels [27]. Demographic variables included age, gender, training, duration of training and clinical experience, health sector, and region of practice. Data on current practice included exercise and physical activity promotion, dietary advice, weight management, smoking cessation, sleep, stress management, and level of confidence in promoting them. In Section C, a four-level ecological model was used to assess factors affecting HP practice, and data on intrapersonal, interpersonal, institutional, and community influences were collected. Closed questions were used to enable management and analysis of responses following guidelines for development and reporting of the survey [33,34]. The developed survey instrument was pilot-tested on a sample of 5 PTs practising in Cameroon who were not included in the study. All feedback was integrated to improve the survey instrument.
2.6. Recruitment and Data Collection
The recruitment of the study participants and data collection was conducted from 1 November 2023 to 31 January 2024. For recruitment, we used the CASP register or mailing list to identify eligible PTs for the study. This group of PTs was asked to promote the survey through their physiotherapy social media networks and community of practice groups at regional and national levels to facilitate recruitment of other PTs practising in Cameroon but who have yet to register with CASP (snowballing) [33]. The survey instrument was administered online using Qualtrics. Participants were able to complete the survey online using electronic devices such as laptops, iPads, and cell phones [33]. Reminders were sent every two weeks during the period the survey was live to ensure maximum response.
2.7. Data Analysis
The web-based data collected were screened for complete responses and downloaded in a Microsoft Excel 2021 document format by the lead author. The data were then transferred to SPSS (IBM SPSS Statistical Software, version 23.0) for statistical analysis. Descriptive statistics (frequencies, central tendency, dispersion/variation, and percentages) were used to present the demographic information and pattern of practice among participants. All missing data (either due to omitted responses or the ‘not applicable’ option) were considered in the analysis.
3. Results
3.1. Participant Characteristics
Responses to the survey questionnaire were obtained from a total of 230 participants. Of these, 38 (16.5.%) were incomplete or poorly completed, and 11 (4.7%) respondents did not meet the inclusion criteria and therefore were not included in the analysis. Table 1 presents the general characteristics of the study participants. Of the 181 respondents included in the analysis, 53% (n = 96) were male and 47% (n = 85) female, with a mean age of 34.43 ± 9.0 years and a mean working experience of 8.96 ± 6.0 years. The mean number of PTs per service was 4.31 ± 4.60, with the highest responses coming from the central region of Cameroon (37.6%, n = 68). Most respondents were trained in Cameroon (95.6%, n = 173) and based in urban settlements (86.7%, n = 157). Of the total sample, 19.3% (n = 35) had a clinical speciality, with the highest being sport (n = 11). Most respondents practised in the private sector, 40.3% (n = 73), with 28.2% working in both the public and private sectors.

Table 1.
Socio-demographic characteristics of the 181 physiotherapists enrolled in the study.
3.2. PT Practice and Levels of Confidence of HP for PwCVDs
PT HP practice is reported in Table 2. Overall, 95% (n = 172) of participants reported that they provide HP to pwCVDs. Most respondents reported that they always conduct HP around weight management (74%, n = 123), dietary advice to increase fruit intake (73%, n = 127), and exercise and physical activity (69%, n = 118). Fewer PTs deliver education around BMI (58%, n = 98) and sleep (48%, n = 83).
Table 2.
Health promotion practices of 172 physiotherapists for people at risk of or with cardiovascular disease in Cameroon.
The majority of respondents were aware of public and clinical guidelines for physical activity (76%, n = 130), exercise (73%, n = 124), and weight management (71%, n = 121), compared to sleep at 53% (n = 91) (see Figure 1). Most PTs deliver HP advice verbally (80%), with apps (69%, n = 118) and websites (63%, n = 109) never used (Figure 2).
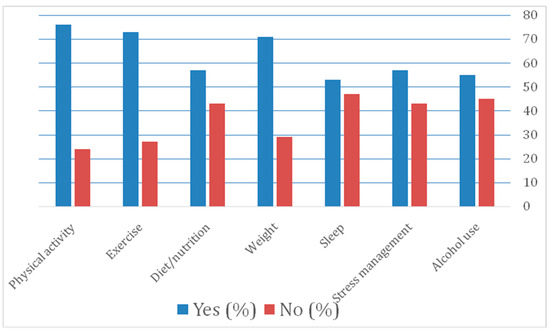
Figure 1.
Physiotherapists’ awareness of public and clinical guidelines (n = 172).
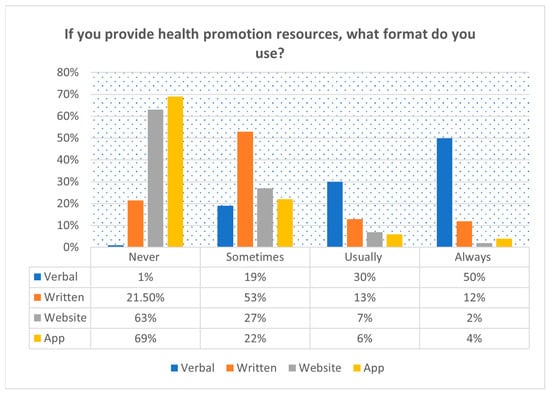
Figure 2.
Format of health promotion practice for people at risk of or with cardiovascular diseases of 172 physiotherapists in Cameroon.
Table 3 provides details on PTs’ confidence level, with the majority confident in assessing lifestyle elements such as weight management (64%, n = 110) and alcohol use (56%, n = 95). PTs reported being slightly confident or lacking confidence in undertaking HP activities involving sleep (61%, n = 102) and diet (50%, n = 85). Overall, 45–69% of the respondents indicated that they assess the level of confidence of pwCVDs to engage in HP in their practice, with 9–20% reporting that they have never assessed the confidence level to improve lifestyle changes for pwCVDs. In addition, 46–61% of the respondents reported that they always address challenges pwCVDs may face across several components of HP and provide them with optimal recommended values in areas such as physical activity, details in Supplementary Table S1.
Table 3.
Physiotherapists’ level of confidence engaging in health promotion practice.
3.3. Factors Affecting HP Practice among PTs in Cameroon for pwCVDs
Factors affecting HP are detailed in Table 4. At the intrapersonal level, professional beliefs about using HP only for those at high risk were held by 64% of respondents (n = 110) and using passive modalities in practice by 30% (n = 53), which may negatively affect HP practice. Participants reported having the relevant skills and knowledge to deliver HP (68%, n = 123) and believe that disease prevention and lifestyle modification are essential for managing chronic conditions (63%, n = 110). At the interpersonal level, the use of personal lifestyle experiences for HP reported by 76% of respondents (n = 131), lack of skills and economic resources (28%, n = 49), and pwCVDs not adhering to HP recommendations (25%, n = 42) may negatively affect HP practice. Interpersonal factors include having confidence in team members, reported by 70% (n = 119), and aligning HP interventions with reasons for consultations, reported by 75% (n = 128) of the respondents. Factors hindering HP practice at the institutional level include lack of organised practice (53%, n = 90), poor role clarification (32%, n = 55), and the absence of regular training opportunities on HP (40%, n = 68). The primary institutional factors include favourable working conditions (52%, n = 89) and having time for HP practice (59%, n = 100) even without financial incentives (59%, n = 100). The lack of existing guidelines on CVD prevention (28%, n = 49) in the Cameroonian setting may hinder HP practice at the community and public levels. Non-interference of religion (61%, n = 104) and culture (59%, n = 102) on HP among respondents may enhance practice.
Table 4.
Factors affecting HP practice based on respondents (n = 172).
4. Discussion
To our knowledge, this is the first study to evaluate practice and factors affecting PLHP for pwCVDs in Cameroon. PTs reported generally high levels of HP practice and confidence to deliver on several components.
4.1. PT Practice of HP for PwCVDs by PTs
The majority of PTs in Cameroon report that they currently deliver several HP components for pwCVDs. Higher proportions of PTs reported delivering on weight management (74%) and dietary advice to eat more fruit (73%) than exercise and physical activities (69%) and sleep (48%). Previous African studies have focused on knowledge, attitudes, and practices towards HP and physical activities among PTs [35]. Studies conducted in Ghana and Nigeria reported that 87% and 92.2% of PTs, respectively, incorporate some aspect of HP in the delivery of care [36,37]. While few studies focused on specific components of HP, some studies have reported similar percentages of integrating HP in practice. Many reported values of HPs were higher than those reported in some African and high-income countries [35,38,39]. For instance, studies conducted in Ghana and Rwanda reported similar values regarding diet and physical activity recommendations [37,38]. Our respondents also reported a higher integration of HP practice in physical activities, smoking cessation, and sleep than in studies conducted in Nigeria, Canada, and Jordan [39,40,41]. Despite 81.5% agreeing that nutritional/dietary counselling is within their scope of practice, less than 50% of Irish and Australian PTs assessed the nutritional status of patients, and even fewer PTs provided nutritional interventions [42,43,44]. The generally lower reported HP activities in previous studies may be due to being conducted in the general patient populations rather than pwCVDs. In pwCVDs, PTs may be more likely to consider the risk and lifestyle factors and what they can do in their role as PTs. It is therefore necessary that studies evaluating the practice of HP for individual components, such as nutritional/dietary counselling, be conducted among PTs in Cameroon to obtain a clearer picture.
4.2. PT Levels of Confidence to Deliver HP for PwCVDs
Consistent with prior research, our data indicate lower confidence levels in delivering HP interventions across all reported behaviours [39,40,41]. We report a similar level of confidence (50%) in delivering dietary advice as in Nigeria (50%) [45] and lower levels of confidence in delivering physical activity (53%) compared to 75% and 93% reported in Nigeria and Australia, respectively [39,43]. The lower level of confidence in physical activity is concerning as this is a primary focus in PT practice. A lack of physical activity policies and implementation in Cameroon may explain this [13]. We reported higher levels of confidence in delivering advice on alcohol use (56%) compared to Nigeria (42.5%) [45] and sleep (39%) compared to reports from Jordan (12%) [41,46]. Conversely, 57% of United States PTs reported routinely assessing their patient’s sleep behaviours [46]. The difference in confidence levels reported across HP components could be accounted for by the different study populations, pwCVDs in our case, and patients in general physiotherapy practice in most previous studies. Also, the purpose and design of data collection instruments in those studies may influence reported outcomes even in a similar context like Nigeria and Cameroon. The focus of our study on pwCVDs might have influenced PTs to think and report their role in modifiable risk factors, not their actual confidence in practice, leading to respondent bias in the study. The PTs in the United States might have access to more formal training, clinical guidelines, and collaborating experts (dieticians/nutritionists, clinical sleep specialists, and psychologists) providing support and increasing confidence in their role in HP practice [46].
Our data align with findings among healthcare students in England; confidence in delivering HP interventions increases in areas of practice with specialists and transparent referral processes [47]. Also, the availability and volume of training in undergraduate physiotherapy courses to deal with a range of HP activities is likely to impact PTs’ confidence in delivering HP activities in practice [47].
Physiotherapy practice is usually centred on physical activity and exercise, and with the bio-psychological model, PTs’ scope of practice has been expanding [19]. Areas such as alcohol use, smoking cessation, stress management, and sleep are still being embraced within the scope of PT practice in Cameroon; confidence and skills to deliver in these areas have been historically low in both high- and low-resource settings [41,46,48]. Confidence is associated with training, but the extent to which HP is integrated into physiotherapy training in Cameroon is not known. Lack of relevant training, including guided counselling and behaviour change techniques such as motivational interviewing, may contribute to low levels of confidence, given behaviour change is required across these lifestyle components [49]. Further studies are warranted to assess factors associated with practices and interventions around specific lifestyle factors in Cameroon. Recent studies demonstrate that PT knowledge and experience are limited in different lifestyle behaviours and conditions, including but not limited to smoking, nutrition, sleep, and stress management, with an increasing need for further education/training to address these behaviours [50,51].
PTs predominantly provide verbal advice to pwCVDs, with relatively little written or printed materials, websites, and apps. This may be associated with the need for more resources, proper educational materials, and expertise on HP, making standard reference material challenging. Even the elderly pwCVDs associate with some form of digital device or that of their carers. Recent trials elsewhere demonstrate the high acceptability of technological-based interventions in rural older adults with obesity [52,53]. Despite contextual barriers in Cameroon, technology-based intervention for HP remains a viable option.
4.3. Factors Affecting HP Practice for pwCVDs
Consistent with the existing literature, respondents in this study reported that intrapersonal factors such as solid professional beliefs, appropriate skill set and knowledge, motivation, positive attitude, and self-confidence towards HP could potentially improve HP practice (Table 4) [37,42,47]. This favours long-term engagement and practice of HP for pwCVDs in Cameroon and influences how HP issues are perceived and addressed. PTs with strong professional beliefs and skills concerning HP are likely to promote their role at different ecological levels (interpersonal, institutional, and public/community). Our findings align well with the global calls to enhance PTs’ contributions to promoting health in daily practice with relevant competencies across different components of HP [19].
Factors potentially limiting HP practice consistent with previous research were identified [35]. These include the lack of regular training, limited resources, lack of specialist referral pathways, and poor role clarification with other clinicians, similar to reports from other Africa-based studies and elsewhere [35,43,44]. Despite time being commonly cited as a barrier in studies from Africa and high-income countries [35,41], the majority of PTs felt that they had the time and working conditions that would allow them to deliver HP activities [35]; this may explain the relatively high level of reported HP activities. This suggests that the priority given to the lack of knowledge, skills, resources, and confidence in improving specific behaviours outweighs the importance of practice time, underscoring the severity of these factors. The situation may vary in other countries that operate under more stringently managed systems. The limited influence of time on HP is encouraging, but it also reveals other challenges related to diverse sectors, healthcare policies, and future practices. For instance, in the private sector, where patients pay for each visit, they may resist follow-up visits due to financial concerns. On the other hand, in the public sector, where services are often free or subsidised, follow-up visits may be constrained by workload and limited contact time per visit [26].
4.4. Implications for Practice
4.4.1. Clinical
The current HP practice and the PTs’ confidence level in Cameroon highlight the need for evidence-based training to design effective interventions and support behaviour change. Advice alone is insufficient for sustained behaviour change, indicating a shift towards health coaching practices [16]. Effective HP acknowledges patients as experts in their situation, with PTs acting as coaches to instil purpose and confidence [54].
This study demonstrates the complex skill set that is required by PTs to address the multifactorial needs of pwCVDs by identifying different areas of awareness and factors affecting HP practice. These are necessary to provide patient-centred approaches and personalised interventions tailored to individual needs. PTs must appreciate the nuanced ways in which these risk factors affect patients with CVDs, necessitating personalised interventions for optimal outcomes. In line with the global call for PTs to address the increasing global burden of CNCDs [19,20], PTs are challenged to address several risk factors. The World Health Professions Alliance provides resources such as the Health Improvement Card, which can be used to assess and monitor risk factors for pwCVDs [55].
4.4.2. Educational
The findings reveal that PTs conduct HP activities but lack confidence across multiple domains. Cameroonian PTs may need more knowledge or confidence in utilising behaviour change techniques to address lifestyle conditions for pwCVDs. This highlights the need for formal training at entry level into practice and continuous professional development training on HP and behaviour change techniques to effectively equip PTs with the requisite skills and knowledge to address lifestyle-related issues [43,48]. In line with existing evidence and ecological models, efforts should focus on strengthening individual factors and professional beliefs among PTs to positively impact healthcare [21].
4.4.3. Policy
The findings offer valuable insights for the development and implementation of PLHP initiatives not only in Cameroon but also in similar settings in Africa. They underscore the importance of curriculum development that integrates HP strategies to equip PTs to address the CVD pandemic. Entry-level physiotherapy programmes in Cameroon should be assessed to ensure they equip graduates with the skills to address emerging healthcare needs, such as promoting health and preventing illnesses, especially among pwCVDs. The government should invest in producing evidence-based public and clinical guidelines in Cameroon.
4.5. Strengths and Limitations
Strengths include the use of a rigorously developed and validated survey instrument, the use of ecological levels to investigate factors affecting HP practice holistically, the large number of respondents, and the use of recommended guidelines in the conduct and reporting of this study.
The study faced challenges with the representativeness of its sample, which makes generalising the findings difficult. This was mitigated by recruiting a large sample of practising PTs, estimated at 250–400 [29,30]. Secondly, respondent bias is possible, as individuals who completed the survey may have a heightened interest in HP activities [56]. This bias could skew the findings and may not accurately represent the broader population of PTs in Cameroon. Thirdly, the sample was not specific to PTs who manage pwCVDs. PTs with much lower caseloads of pwCVDs may face different realities in their practice, so findings should be considered cautiously. Fourthly, we examine potential factors affecting several components of HP without any solid association with PLHP practice; future studies should examine barriers and facilitators to specific components of PLHP in Cameroon. Finally, while the study utilised a validated survey tool, the reliance on quantitative research methods with closed-ended questions may limit the depth of insights into PTs’ beliefs, attitudes, and perceptions regarding HP for pwCVDs. This limitation underscores the need for complementary qualitative research to explore these aspects comprehensively.
5. Conclusions
Cameroonian PTs reported high levels of practice in some HP activities with consistently lower confidence levels in delivering all activities for pwCVDs. Most respondents delivered HP advice verbally, seldom using print or written advice. Professional beliefs, confidence in interventions, supportive teams, and favourable working conditions potentially enhance HP practice. This highlights the necessity of strong organisational and professional support. However, entrenched beliefs in using passive modalities, patient adherence issues, and systemic challenges, including lack of resources, guidelines, role ambiguity, and limited training opportunities, may limit HP practice.
This study demonstrates the complex skill set that PTs require to effectively address the multifactorial needs of pwCVDs by identifying different areas, awareness, and factors affecting HP practice. In line with existing evidence and ecological models, efforts should focus on strengthening individual factors and professional beliefs among PTs to positively impact the broader healthcare ecosystem. This highlights the importance of curriculum development integrating HP strategies to equip PTs to address the CVD pandemic. Our quantitative research methods with closed-ended questions may limit the depth of insights into Cameroonian PTs’ beliefs, attitudes, and perceptions regarding HP for pwCVDs. This limitation underscores the need for complementary qualitative research to gain an in-depth understanding of HP practices in Cameroon.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/clinpract14050140/s1, Table S1: A Do you ask your patients about their confidence to change or improve their habits in the following areas? B Do you discuss challenges patients may face while trying to improve in any of the following areas? C Do you assist your patient to know the optimal recommended values for? What is most (highest) common type of problems your see on daily basis?—Selected Choice.
Author Contributions
Conceptualisation, E.N.N. and S.M.; methodology, E.N.N. and S.M.; validation, E.N.N., S.M. and C.K.; data curation, E.N.N. and S.M.; formal analysis, E.N.N.; investigation, E.N.N., S.M. and C.K.; supervision, S.M., C.K., R.Y. and J.L.; writing of original draft, E.N.N.; writing—review and editing, all authors; approval of final draft, all authors. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study received approvals from Sheffield Hallam University with Ethics review ID ER43779431 (18 October 2022) and Cameroon National Ethics Committee for Human Health Research #2023/10/1595/CE/CNERSH/SP (18 October 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated during and analysed during the current study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hajat, C.; Stein, E. The Global Burden of Multiple Chronic Conditions: A Narrative Review. Prev. Med. Rep. 2018, 12, 284–293. [Google Scholar] [CrossRef]
- Deaths from Cardiovascular Disease Surged 60% Globally over the Last 30 Years: Report—World Heart Federation. Available online: https://world-heart-federation.org/news/deaths-from-cardiovascular-disease-surged-60-globally-over-the-last-30-years-report/ (accessed on 10 March 2024).
- Anand, S.; Bradshaw, C.; Prabhakaran, D. Prevention and Management of CVD in LMICs: Why Do Ethnicity, Culture, and Context Matter? BMC Med. 2020, 18, 7. [Google Scholar] [CrossRef] [PubMed]
- Bowry, A.D.K.; Lewey, J.; Dugani, S.B.; Choudhry, N.K. The Burden of Cardiovascular Disease in Low- and Middle-Income Countries: Epidemiology and Management. Can. J. Cardiol. 2015, 31, 1151–1159. [Google Scholar] [CrossRef] [PubMed]
- Peiris, D.; Ghosh, A.; Manne-Goehler, J.; Jaacks, L.M.; Theilmann, M.; Marcus, M.E.; Zhumadilov, Z.; Tsabedze, L.; Supiyev, A.; Silver, B.K.; et al. Cardiovascular Disease Risk Profile and Management Practices in 45 Low-Income and Middle-Income Countries: A Cross-Sectional Study of Nationally Representative Individual-Level Survey Data. PLoS Med. 2021, 18, e1003485. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Sun, Y.; Jiang, D.; Wang, C.; Liu, S. Risk-Attributable Burden of Ischemic Heart Disease in 137 Low- and Middle-Income Countries From 2000 to 2019. J. Am. Heart Assoc. 2021, 10, e021024. [Google Scholar] [CrossRef] [PubMed]
- Dzudie, A.; Fourie, J.M.; Scholtz, W.; Scarlatescu, O.; Nel, G.; Kingue, S. PASCAR and WHF Cardiovascular Diseases Scorecard Project. Cardiovasc. J. Afr. 2020, 31, 8. [Google Scholar] [CrossRef] [PubMed]
- Akono, M.N.; Simo, L.P.; Agbor, V.N.; Njoyo, S.L.; Mbanya, D. The Spectrum of Heart Disease among Adults at the Bamenda Regional Hospital, North West Cameroon: A Semi Urban Setting. BMC Res. Notes 2019, 12, 761. [Google Scholar] [CrossRef] [PubMed]
- Nkoke, C.; Jingi, A.M.; Makoge, C.; Teuwafeu, D.; Nkouonlack, C.; Dzudie, A. Epidemiology of Cardiovascular Diseases Related Admissions in a Referral Hospital in the South West Region of Cameroon: A Cross-Sectional Study in Sub-Saharan Africa. PLoS ONE 2019, 14, e0226644. [Google Scholar] [CrossRef]
- About the CVD World Monitor | CVD World Monitor. Available online: http://cvdworldmonitor.org/about/ (accessed on 22 November 2021).
- World Health Statistics. Available online: https://www.who.int/data/gho/data/themes/topics/topic-details/GHO/world-health-statistics (accessed on 22 November 2021).
- Aminde, L.N.; Takah, N.; Ngwasiri, C.; Noubiap, J.J.; Tindong, M.; Dzudie, A.; Veerman, J.L. Population Awareness of Cardiovascular Disease and Its Risk Factors in Buea, Cameroon. BMC Public Health 2017, 17, 545. [Google Scholar] [CrossRef]
- Tatah, L.; Mapa-Tassou, C.; Shung-King, M.; Oni, T.; Woodcock, J.; Weimann, A.; McCreedy, N.; Muzenda, T.; Govia, I.; Mbanya, J.C.; et al. Analysis of Cameroon’s Sectoral Policies on Physical Activity for Noncommunicable Disease Prevention. Int. J. Environ. Res. Public Health 2021, 18, 12713. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Bezner, J.R. Promoting Health and Wellness: Implications for Physical Therapist Practice. Phys Ther. 2015;95:1433–1444. Phys. Ther. 2016, 96, 123. [Google Scholar] [CrossRef][Green Version]
- Malik, S.H.; Blake, H.; Suggs, L.S. A Systematic Review of Workplace Health Promotion Interventions for Increasing Physical Activity. Br. J. Health Psychol. 2014, 19, 149–180. [Google Scholar] [CrossRef] [PubMed]
- Physiotherapy Practice Start up, Cameroon. Available online: https://www.indiegogo.com/projects/1307213 (accessed on 8 July 2022).
- Dean, E.; Dornelas de Andrade, A.; O’Donoghue, G.; Skinner, M.; Umereh, G.; Beenen, P.; Cleaver, S.; Afzalzada, D.; Fran Delaune, M.; Footer, C.; et al. The Second Physical Therapy Summit on Global Health: Developing an Action Plan to Promote Health in Daily Practice and Reduce the Burden of Non-Communicable Diseases. Physiother. Theory Pract. 2014, 30, 261–275. [Google Scholar] [CrossRef] [PubMed]
- Dean, E.; Umerah, G.; Dornelas de Andrade, A.; Söderlund, A.; Skinner, M. The Third Physical Therapy Summit on Global Health: Health-Based Competencies. Physiotherapy 2015, 101, e13–e14. [Google Scholar] [CrossRef]
- Dean, E. Physical Therapy in the 21st Century (Part I): Toward Practice Informed by Epidemiology and the Crisis of Lifestyle Conditions. Physiother. Theory Pract. 2009, 25, 330–353. [Google Scholar] [CrossRef]
- Frerichs, W.; Kaltenbacher, E.; van de Leur, J.P.; Dean, E. Can Physical Therapists Counsel Patients with Lifestyle-Related Health Conditions Effectively? A Systematic Review and Implications. Physiother. Theory Pract. 2012, 28, 571–587. [Google Scholar] [CrossRef]
- Bezner, J.R.; Lloyd, L.; Crixell, S.; Franklin, K. Health Behaviour Change Coaching in Physical Therapy: Improving Physical Fitness and Related Psychological Constructs of Employees in a University Setting. Eur. J. Physiother. 2017, 19, 1–2. [Google Scholar] [CrossRef]
- Ragupathi, L.; Stribling, J.; Yakunina, Y.; Fuster, V.; McLaughlin, M.A.; Vedanthan, R. Availability, Use, and Barriers to Cardiac Rehabilitation in LMIC. Glob. Heart 2017, 12, 323–334.e10. [Google Scholar] [CrossRef]
- Ontario Physiotherapy Leadership Consortium Physiotherapists in Health Promotion: Findings of a Forum. Physiother. Can. 2011, 63, 391–392. [CrossRef]
- Higgins, R.; Gray, H. Barriers and Facilitators to Student Physiotherapists’ Use of Psychological Interventions in Physiotherapy Practice. Physiotherapy 2020, 107, e154. [Google Scholar] [CrossRef]
- Rogers, H.L.; Pablo Hernando, S.; Núñez-Fernández, S.; Sanchez, A.; Martos, C.; Moreno, M.; Grandes, G. Barriers and Facilitators in the Implementation of an Evidence-Based Health Promotion Intervention in a Primary Care Setting: A Qualitative Study. J. Health Organ. Manag. 2021, 35, 349–367. [Google Scholar] [CrossRef]
- Rubio-Valera, M.; Pons-Vigués, M.; Martínez-Andrés, M.; Moreno-Peral, P.; Berenguera, A.; Fernández, A. Barriers and Facilitators for the Implementation of Primary Prevention and Health Promotion Activities in Primary Care: A Synthesis through Meta-Ethnography. PLoS ONE 2014, 9, e89554. [Google Scholar] [CrossRef]
- Cameroon Society of Physiotherapy. Available online: https://world.physio/membership/cameroon (accessed on 16 March 2022).
- Sharma, K.N. Evidence of Barriers to Evidence-Based Physiotherapy Practice in Central Africa. Int. J. Health Sci. Res. 2022, 12, 299–302. [Google Scholar] [CrossRef]
- Kossi, O. Training, Care Delivery, and Research in Physiotherapy in Sub-Saharan French-Speaking Africa. S. Afr. J. Physiother. 2023, 79, 1932. [Google Scholar] [CrossRef]
- Abaraogu, U.O.; Edeonuh, J.C.; Frantz, J. Promoting Physical Activity and Exercise in Daily Practice: Current Practices, Barriers, and Training Needs of Physiotherapists in Eastern Nigeria. Physiother. Can. 2016, 68, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Ngeh, E.N.; Lowe, A.; Garcia, C.; McLean, S. Physiotherapy-Led Health Promotion Strategies for People with or at Risk of Cardiovascular Diseases: A Scoping Review. Int. J. Environ. Res. Public Health 2023, 20, 7073. [Google Scholar] [CrossRef]
- Kelley, K. Good Practice in the Conduct and Reporting of Survey Research. Int. J. Qual. Health Care 2003, 15, 261–266. [Google Scholar] [CrossRef]
- Sharma, A.; Minh Duc, N.T.; Luu Lam Thang, T.; Nam, N.H.; Ng, S.J.; Abbas, K.S.; Huy, N.T.; Marušić, A.; Paul, C.L.; Kwok, J.; et al. A Consensus-Based Checklist for Reporting of Survey Studies (CROSS). J. Gen. Intern. Med. 2021, 36, 3179–3187. [Google Scholar] [CrossRef]
- Musonda, N.; Simpamba, M.M. A Review of Health Promotion Practices Among Physiotherapists in Africa. J. Prev. Rehabil. Med. 2021, 3, 14–19. [Google Scholar] [CrossRef]
- Abaraogu, U.O.; Onah, U.; Abaraogu, O.D.; Fawole, H.O.; Kalu, M.E.; Seenan, C.A. Knowledge, Attitudes, and the Practice of Health Promotion among Physiotherapists in Nigeria. Physiother. Can. 2019, 71, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Boakye, H.; Quartey, J.; Baidoo, N.A.B.; Ahenkorah, J. Knowledge, Attitude and Practice of Physiotherapists towards Health Promotion in Ghana. S. Afr. J. Physiother. 2018, 74, 443. [Google Scholar] [CrossRef]
- Frantz, J.; Ngambare, R. Physical Activity and Health Promotion Strategies among Physiotherapists in Rwanda. Afr. Health Sci. 2013, 13, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Aweto, H.A.; Oligbo, C.N.; Fapojuwo, O.A.; Olawale, O.A. Knowledge, Attitude and Practice of Physiotherapists towards Promotion of Physically Active Lifestyles in Patient Management. BMC Health Serv. Res. 2013, 13, 21. [Google Scholar] [CrossRef]
- Bodner, M.E.; Rhodes, R.E.; Miller, W.C.; Dean, E. Smoking Cessation and Counseling. Am. J. Prev. Med. 2012, 43, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Al-Sharman, A.; Aldughmi, M.; Khalil, H.; AlKhawaldeh, H.; Siengsukon, C.F.; El-Salem, K. Knowledge and Attitudes of Physiotherapists toward Sleep: A Survey Study. Work 2022, 73, 739–746. [Google Scholar] [CrossRef]
- Abaraogu, U.O.; Ogaga, M.O.; Odidika, E.; Frantz, J. Promotion of Healthy Nutrition in Clinical Practice: A Cross-Sectional Survey of Practices and Barriers among Physiotherapists in Southeast Nigeria. Hong Kong Physiother. J. 2016, 35, 21–29. [Google Scholar] [CrossRef]
- Snodgrass, S.J.; Carter, A.E.; Guest, M.; Collins, C.E.; James, C.; Kable, A.K.; Ashby, S.E.; Plotnikoff, R.C. Weight Management Including Dietary and Physical Activity Advice Provided by Australian Physiotherapists: A Pilot Cross-Sectional Survey. Physiother. Theory Pract. 2014, 30, 409–420. [Google Scholar] [CrossRef]
- O’Donoghue, G.; Cunningham, C.; Murphy, F.; Woods, C.; Aagaard-Hansen, J. Assessment and Management of Risk Factors for the Prevention of Lifestyle-Related Disease: A Cross-Sectional Survey of Current Activities, Barriers and Perceived Training Needs of Primary Care Physiotherapists in the Republic of Ireland. Physiotherapy 2014, 100, 116–122. [Google Scholar] [CrossRef]
- Abaraogu, U.O.; Ogaga, M.O.; Dean, E. Practices of Nigerian Physiotherapists with Respect to Lifestyle Risk Factor Assessment and Intervention: A National Cross-Sectional Survey. Physiother. Theory Pract. 2017, 33, 497–507. [Google Scholar] [CrossRef]
- Siengsukon, C.F.; Al-dughmi, M.; Sharma, N.K. A Survey of Physical Therapists’ Perception and Attitude About Sleep. J. Allied Health 2015, 44, 41–50. [Google Scholar]
- McLean, S.; Charlesworth, L.; May, S.; Pollard, N. Healthcare Students’ Perceptions about Their Role, Confidence and Competence to Deliver Brief Public Health Interventions and Advice. BMC Med. Educ. 2018, 18, 114. [Google Scholar] [CrossRef] [PubMed]
- Coren, S. Sleep Health and Its Assessment and Management in Physical Therapy Practice: The Evidence. Physiother. Theory Pract. 2009, 25, 442–452. [Google Scholar] [CrossRef] [PubMed]
- Fortune, J.; Breckon, J.; Norris, M.; Eva, G.; Frater, T. Motivational Interviewing Training for Physiotherapy and Occupational Therapy Students: Effect on Confidence, Knowledge and Skills. Patient Educ. Couns. 2019, 102, 694–700. [Google Scholar] [CrossRef]
- Alodaibi, F.A.; Alotaibi, M.A.; Almohiza, M.; Alhowimel, A.S. Physical Therapists’ Role in Health and Wellness Promotion for People with Musculoskeletal Disorders: A Cross-Sectional Description Study Conducted in Saudi Arabia. J. Multidiscip. Healthc. 2022, 15, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Shore, H.; Hebron, C. Musculoskeletal Physiotherapists’ Perceptions of Health Promotion. Musculoskelet. Sci. Pract. 2020, 50, 102260. [Google Scholar] [CrossRef]
- Batsis, J.A.; Petersen, C.L.; Clark, M.M.; Cook, S.B.; Kotz, D.; Gooding, T.L.; Roderka, M.N.; Al-Nimr, R.I.; Pidgeon, D.; Haedrich, A.; et al. Feasibility and Acceptability of a Technology-Based, Rural Weight Management Intervention in Older Adults with Obesity. BMC Geriatr. 2021, 21, 44. [Google Scholar] [CrossRef]
- Batsis, J.A.; Petersen, C.L.; Clark, M.M.; Cook, S.B.; Lopez-Jimenez, F.; Al-Nimr, R.I.; Pidgeon, D.; Kotz, D.; Mackenzie, T.A.; Bartels, S.J. A Weight Loss Intervention Augmented by a Wearable Device in Rural Older Adults With Obesity: A Feasibility Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2021, 76, 95–100. [Google Scholar] [CrossRef]
- Good and Bad Help: How Purpose and Confidence Transform Lives. Available online: http://allcatsrgrey.org.uk/wp/wpfb-file/good_and_bad_help_0-pdf/ (accessed on 19 August 2023).
- WHPA Health Improvement Card—Physiopedia. Available online: https://www.physio-pedia.com/WHPA_Health_Improvement_Card (accessed on 18 April 2024).
- Morrison, C.; Lee, J.P.; Gruenewald, P.J.; Marzell, M. A Critical Assessment of Bias in Survey Studies Using Location-Based Sampling to Recruit Patrons in Bars. Subst. Use Misuse 2015, 50, 1427–1436. [Google Scholar] [CrossRef][Green Version]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).