
Epidemiology of Hepatocellular Carcinoma in Taiwan


Abstract
1. Introduction
2. Materials and Methods
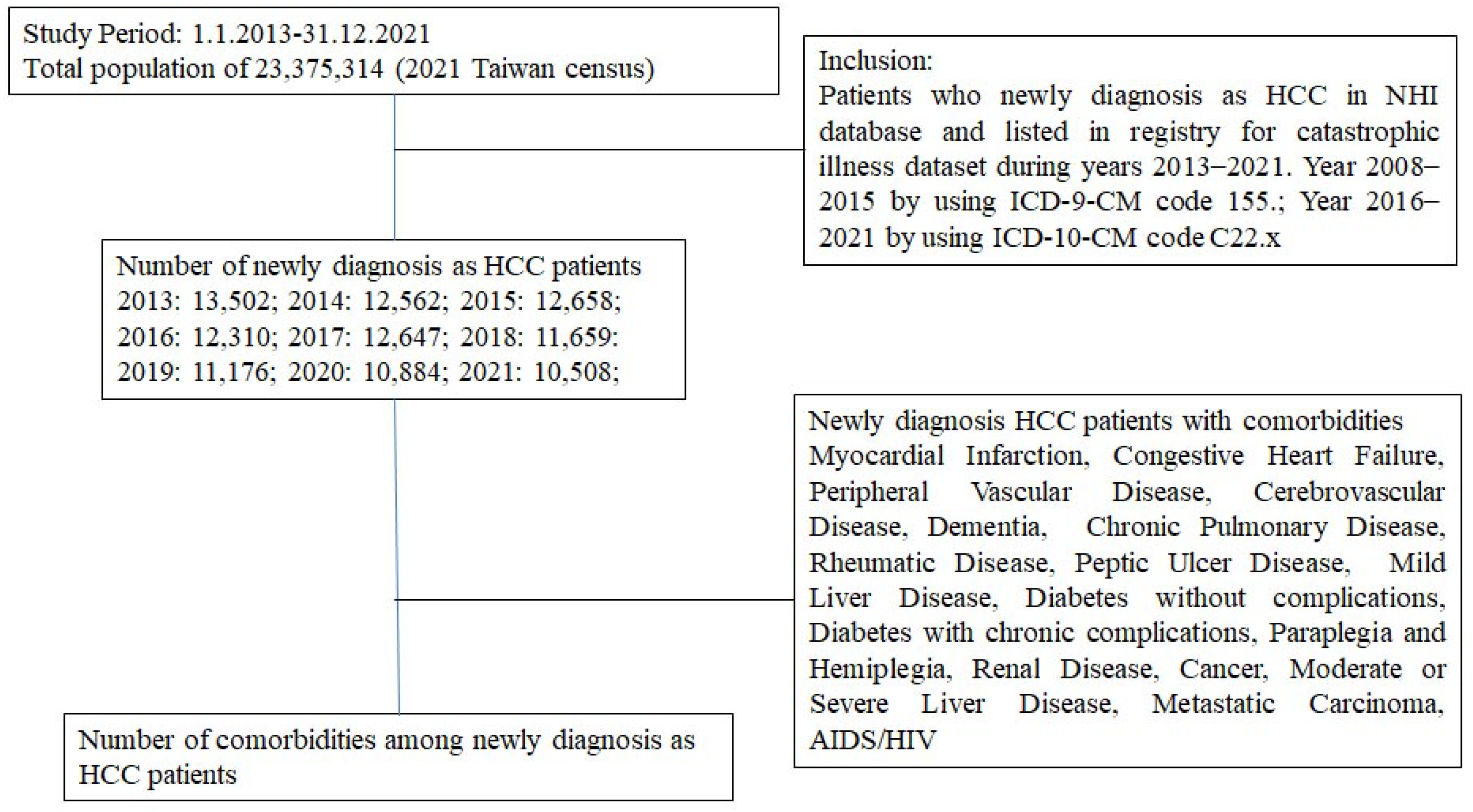
2.1. Data Source
2.2. Study Inclusion
2.3. Data Analyses
3. Results
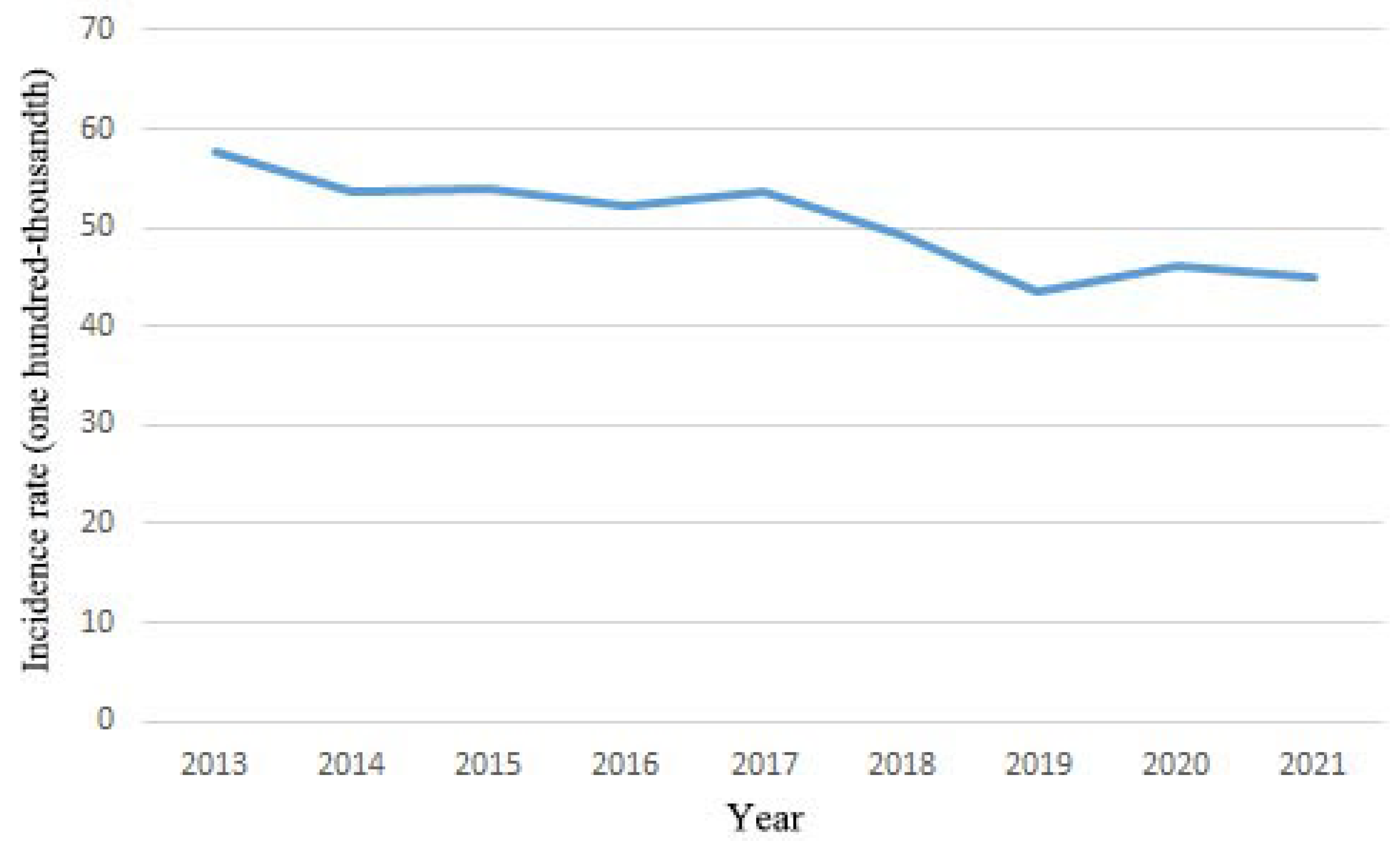
3.1. Annual Incidence of HCC
3.2. Baseline Characteristics and Antineoplastic Agent Usage
3.3. Underlying Diseases in Newly Diagnosed HCC Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef] [PubMed]
- Mittal, S.; El-Serag, H.B. Epidemiology of hepatocellular carcinoma: Consider the population. J. Clin. Gastroenterol. 2013, 47, S2–S6. [Google Scholar] [CrossRef] [PubMed]
- Motta, B.M.; Masarone, M.; Torre, P.; Persico, M. From Non-Alcoholic Steatohepatitis (NASH) to Hepatocellular Carcinoma (HCC): Epidemiology, Incidence, Predictions, Risk Factors, and Prevention. Cancers 2023, 15, 5458. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.Q.; El-Serag, H.B.; Loomba, R. Global epidemiology of NAFLD-related HCC: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 223–238. [Google Scholar] [CrossRef] [PubMed]
- Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; et al.; Global Burden of Disease Cancer Collaboration Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Yang, L.; Ma, L.; Lu, Q.; Luo, Y. Diagnostic Accuracy of Contrast-Enhanced Ultrasound Liver Imaging Reporting and Data System (CEUS LI-RADS) for Differentiating Between Hepatocellular Carcinoma and Other Hepatic Malignancies in High-Risk Patients: A Meta-Analysis. Ultraschall Med. 2021, 42, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.D.; Hainaut, P.; Gores, G.J.; Amadou, A.; Plymoth, A.; Roberts, L.R. A global view of hepatocellular carcinoma: Trends, risk, prevention and management. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Valery, P.C.; Laversanne, M.; Clark, P.J.; Petrick, J.L.; McGlynn, K.A.; Bray, F. Projections of primary liver cancer to 2030 in 30 countries worldwide. Hepatology 2018, 67, 600–611. [Google Scholar] [CrossRef]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Yu, N.C.; Chaudhari, V.; Raman, S.S.; Lassman, C.; Tong, M.J.; Busuttil, R.W.; Lu, D.S. CT and MRI improve detection of hepatocellular carcinoma, compared with ultrasound alone, in patients with cirrhosis. Clin. Gastroenterol. Hepatol. 2011, 9, 161–167. [Google Scholar] [CrossRef]
- Kim, S.Y.; An, J.; Lim, Y.S.; Han, S.; Lee, J.Y.; Byun, J.H.; Won, H.J.; Lee, S.J.; Lee, H.C.; Lee, Y.S. MRI With Liver-Specific Contrast for Surveillance of Patients with Cirrhosis at High Risk of Hepatocellular Carcinoma. JAMA Oncol. 2017, 3, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Tzartzeva, K.; Obi, J.; Rich, N.E.; Parikh, N.D.; Marrero, J.A.; Yopp, A.; Waljee, A.K.; Singal, A.G. Surveillance Imaging and Alpha Fetoprotein for Early Detection of Hepatocellular Carcinoma in Patients with Cirrhosis: A Meta-analysis. Gastroenterology 2018, 154, 1706–1718.e1. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, A.H.; Sadikova, E.; Cheetham, C.; Chiang, K.M.; Shi, J.X.; Caparosa, S.; Younossi, Z.M.; Nyberg, L.M. Increased cancer rates in patients with chronic hepatitis C. Liver Int. 2020, 40, 685–693. [Google Scholar] [CrossRef]
- Saitta, C.; Pollicino, T.; Raimondo, G. Obesity and liver cancer. Ann. Hepatol. 2019, 18, 810–815. [Google Scholar] [CrossRef] [PubMed]
- Ninio, L.; Nissani, A.; Meirson, T.; Domovitz, T.; Genna, A.; Twafra, S.; Srikanth, K.D.; Dabour, R.; Avraham, E.; Davidovich, A.; et al. Hepatitis C Virus Enhances the Invasiveness of Hepatocellular Carcinoma via EGFR-Mediated Invadopodia Formation and Activation. Cells 2019, 8, 1395. [Google Scholar] [CrossRef]
- Khan, A.; Qazi, J. Risk factors and molecular epidemiology of HBV and HCV in internally displaced persons (IDPs) of North Waziristan Agency, Pakistan. J. Pak. Med. Assoc. 2018, 68, 165–169. [Google Scholar]
- Shen, C.; Jiang, X.; Li, M.; Luo, Y. Hepatitis Virus and Hepatocellular Carcinoma: Recent Advances. Cancers 2023, 15, 533. [Google Scholar] [CrossRef]
- Zeng, H.; Li, L.; Hou, Z.; Zhang, Y.; Tang, Z.; Liu, S. Direct-acting Antiviral in the Treatment of Chronic Hepatitis C: Bonuses and Challenges. Int. J. Med. Sci. 2020, 17, 892–902. [Google Scholar] [CrossRef] [PubMed]
- Mushtaq, S.; Mansoor, A.; Umar, M.; Khan, A.; Siddiqi, S.; Manzoor, S. Direct-acting antiviral agents in the treatment of chronic hepatitis C-Real-life experience from clinical practices in Pakistan. J. Med. Virol. 2020, 92, 3475–3487. [Google Scholar] [CrossRef] [PubMed]
- Chien, R.N.; Lu, S.N.; Pwu, R.F.; Wu, G.H.; Yang, W.W.; Liu, C.L. Taiwan accelerates its efforts to eliminate hepatitis C. Glob. Health Med. 2021, 3, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Hsu, J.Y.; Liu, P.P.; Liu, A.B.; Huang, H.K.; Loh, C.H. High 1-year risk of stroke in patients with hepatocellular carcinoma: A nationwide registry-based cohort study. Sci. Rep. 2021, 11, 10444. [Google Scholar] [CrossRef] [PubMed]
- Lazo, M.; Hernaez, R.; Bonekamp, S.; Kamel, I.R.; Brancati, F.L.; Guallar, E.; Clark, J.M. Non-alcoholic fatty liver disease and mortality among US adults: Prospective cohort study. BMJ 2011, 343, d6891. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Ridker, P.M.; Hansson, G.K.; Leducq Transatlantic Network on Atherothrombosis. Inflammation in atherosclerosis: From pathophysiology to practice. J. Am. Coll. Cardiol. 2009, 54, 2129–2138. [Google Scholar] [CrossRef] [PubMed]
- Donato, F.; Tagger, A.; Gelatti, U.; Parrinello, G.; Boffetta, P.; Albertini, A.; Decarli, A.; Trevisi, P.; Ribero, M.L.; Martelli, C.; et al. Alcohol and hepatocellular carcinoma: The effect of lifetime intake and hepatitis virus infections in men and women. Am. J. Epidemiol. 2002, 155, 323–331. [Google Scholar] [CrossRef]
- Goel, S.; Sharma, A.; Garg, A. Effect of Alcohol Consumption on Cardiovascular Health. Curr. Cardiol. Rep. 2018, 20, 19. [Google Scholar] [CrossRef]
- Li, X.; Xu, H.; Gao, P. Diabetes Mellitus is a Risk Factor for Hepatocellular Carcinoma in Patients with Chronic Hepatitis B Virus Infection in China. Med. Sci. Monit. 2018, 24, 6729–6734. [Google Scholar] [CrossRef]
- Lurje, I.; Czigany, Z.; Bednarsch, J.; Roderburg, C.; Isfort, P.; Neumann, U.P.; Lurje, G. Treatment Strategies for Hepatocellular Carcinoma—A Multidisciplinary Approach. Int. J. Mol. Sci. 2019, 20, 1465. [Google Scholar] [CrossRef]
- Yang, G.; Yan, H.; Tang, Y.; Yuan, F.; Cao, M.; Ren, Y.; Li, Y.; He, Z.; Su, X.; Yao, Z.; et al. Advancements in understanding mechanisms of hepatocellular carcinoma radiosensitivity: A comprehensive review. Chin. J. Cancer Res. 2023, 35, 266–282. [Google Scholar] [PubMed]
- Ntellas, P.; Chau, I. Updates on Systemic Therapy for Hepatocellular Carcinoma. Am. Soc. Clin. Oncol. Educ. Book 2024, 44, e430028. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Age | CCI | |||||
|---|---|---|---|---|---|---|
| Year | Mean | Median | 95% CI | Mean | Median | 95% CI |
| 2013 | 65.54 ± 12.59 | 66 | 65.33–65.76 | 4.98 ± 2.62 | 18 | 4.94–5.03 |
| 2014 | 65.88 ± 12.63 | 66 | 65.66–66.10 | 5.42 ± 2.78 | 21 | 5.37–5.47 |
| 2015 | 66.51 ± 12.56 | 66 | 66.29–66.73 | 5.47 ± 2.78 | 19 | 5.42–5.52 |
| 2016 | 66.68 ± 12.45 | 67 | 66.46–66.90 | 5.32 ± 2.83 | 19 | 5.27–5.37 |
| 2017 | 66.84 ± 12.27 | 67 | 66.62–67.05 | 5.25 ± 2.82 | 18 | 5.20–5.30 |
| 2018 | 67.41 ± 12.15 | 67 | 67.19–67.93 | 5.38 ± 2.89 | 19 | 5.33–5.43 |
| 2019 | 67.11 ± 12.25 | 67 | 66.88–67.34 | 5.35 ± 2.87 | 18 | 5.30–5.40 |
| 2020 | 67.9112.24 | 68 | 67.68–68.14 | 5.51 ± 2.96 | 18 | 5.45–5.56 |
| 2021 | 67.92 ± 12.06 | 68 | 67.68–68.15 | 5.49 ± 2.95 | 19 | 5.43–5.55 |
| p for trend | <0.001 | <0.001 | ||||
| 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | p for Trend | |
|---|---|---|---|---|---|---|---|---|---|---|
| Myocardial Infarction | 0.84% | 1.13% | 1.02% | 1.18% | 1.27% | 1.56% | 1.44% | 1.52% | 1.65% | <0.001 |
| Congestive Heart Failure | 5.47% | 6.33% | 6.54% | 6.83% | 7.29% | 7.21% | 7.02% | 8.16% | 7.14% | <0.001 |
| Peripheral Vascular Disease | 2.18% | 2.71% | 2.88% | 2.83% | 2.59% | 2.49% | 3.02% | 2.78% | 2.81% | <0.001 |
| Cerebrovascular Disease | 8.10% | 10.36% | 10.43% | 10.08% | 10.39% | 10.78% | 11.02% | 10.63% | 10.57% | <0.001 |
| Dementia | 2.51% | 3.57% | 3.79% | 3.95% | 4.13% | 4.82% | 4.86% | 5.15% | 4.78% | <0.001 |
| Chronic Pulmonary Disease | 11.49% | 15.70% | 15.44% | 15.74% | 15.70% | 15.84% | 15.43% | 14.70% | 13.27% | <0.001 |
| Rheumatic Disease | 1.73% | 1.93% | 2.08% | 1.84% | 1.29% | 1.45% | 1.39% | 1.30% | 1.28% | <0.001 |
| Peptic Ulcer Disease | 28.77% | 33.64% | 33.48% | 33.02% | 31.34% | 30.87% | 29.45% | 29.45% | 27.55% | <0.001 |
| Mild Liver Disease | 79.61% | 83.01% | 82.52% | 65.35% | 56.81% | 57.53% | 57.97% | 56.63% | 55.77% | <0.001 |
| Diabetes without complications | 29.93% | 33.53% | 34.22% | 34.72% | 35.27% | 35.98% | 35.92% | 36.51% | 37.30% | <0.001 |
| Diabetes with chronic complications | 8.21% | 10.10% | 11.22% | 12.23% | 13.32% | 14.62% | 14.92% | 15.99% | 15.59% | <0.001 |
| Paraplegia and Hemiplegia | 0.64% | 0.85% | 0.92% | 0.74% | 0.66% | 0.74% | 0.90% | 0.94% | 0.91% | <0.001 |
| Renal Disease | 9.35% | 11.20% | 12.56% | 13.30% | 13.15% | 14.47% | 14.32% | 15.11% | 15.31% | <0.001 |
| Cancer | 96.49% | 96.68% | 96.73% | 96.49% | 96.77% | 96.71% | 96.28% | 96.75% | 96.56% | <0.001 |
| Moderate or Severe Liver Disease | 10.53% | 12.17% | 12.03% | 10.33% | 8.90% | 9.35% | 8.32% | 8.86% | 8.06% | <0.001 |
| Metastatic Carcinoma | 11.06% | 12.54% | 12.47% | 13.26% | 13.91% | 14.49% | 14.81% | 16.47% | 17.43% | <0.001 |
| AIDS/HIV | 0.09% | 0.14% | 0.10% | 0.07% | 0.11% | 0.21% | 0.13% | 0.17% | 0.22% | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, Y.-W.; Chung, C.-H. Epidemiology of Hepatocellular Carcinoma in Taiwan. Clin. Pract. 2024, 14, 570-578. https://doi.org/10.3390/clinpract14020044
Lai Y-W, Chung C-H. Epidemiology of Hepatocellular Carcinoma in Taiwan. Clinics and Practice. 2024; 14(2):570-578. https://doi.org/10.3390/clinpract14020044
Chicago/Turabian StyleLai, Yu-Wei, and Ching-Hu Chung. 2024. "Epidemiology of Hepatocellular Carcinoma in Taiwan" Clinics and Practice 14, no. 2: 570-578. https://doi.org/10.3390/clinpract14020044
APA StyleLai, Y.-W., & Chung, C.-H. (2024). Epidemiology of Hepatocellular Carcinoma in Taiwan. Clinics and Practice, 14(2), 570-578. https://doi.org/10.3390/clinpract14020044