
Surgical Treatment of Saphenous Nerve Injury Assisted by Plasma Rich in Growth Factors (PRGF): Lessons from a Case Report

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Report
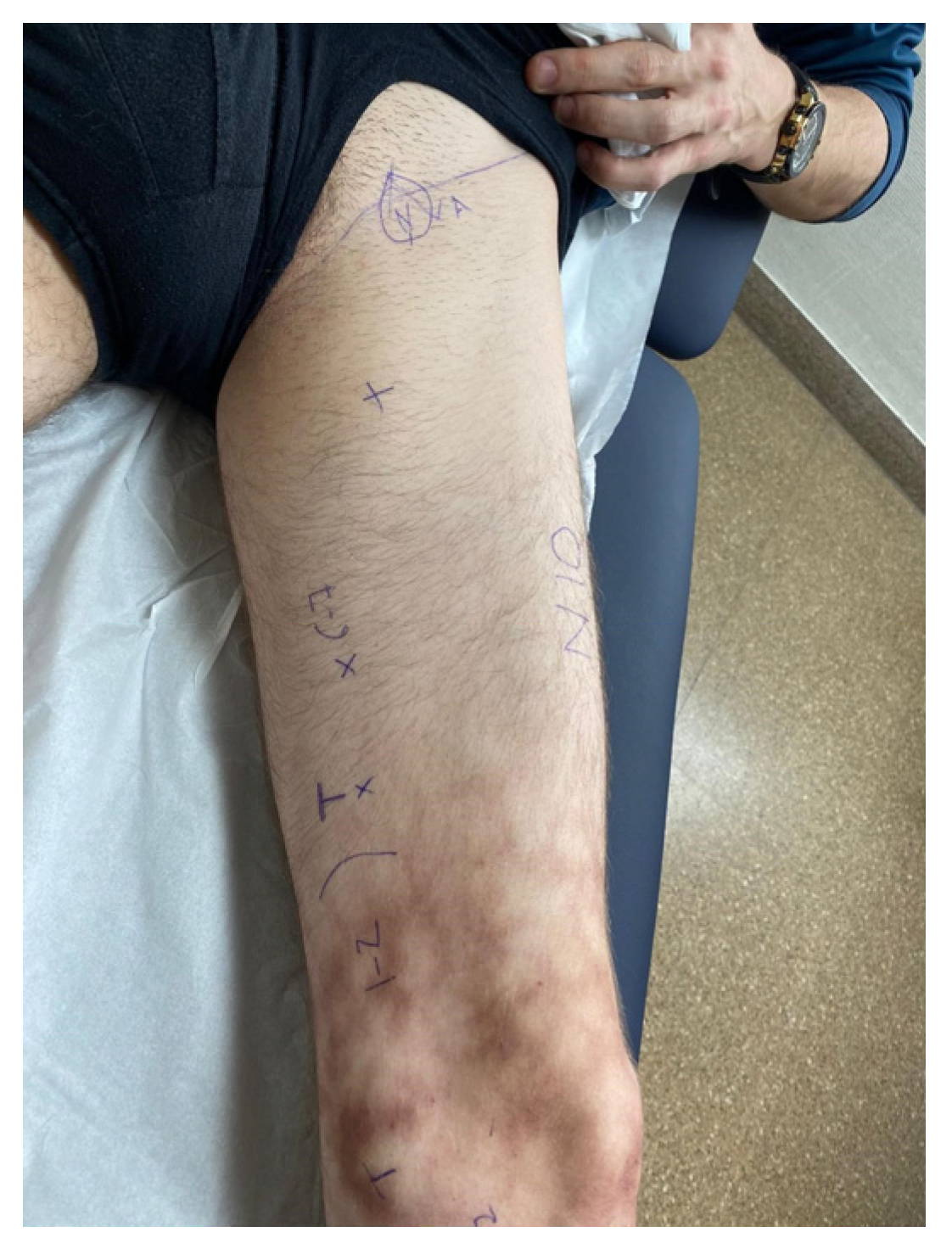
2.1. Patient Presentation
2.2. Diagnostics
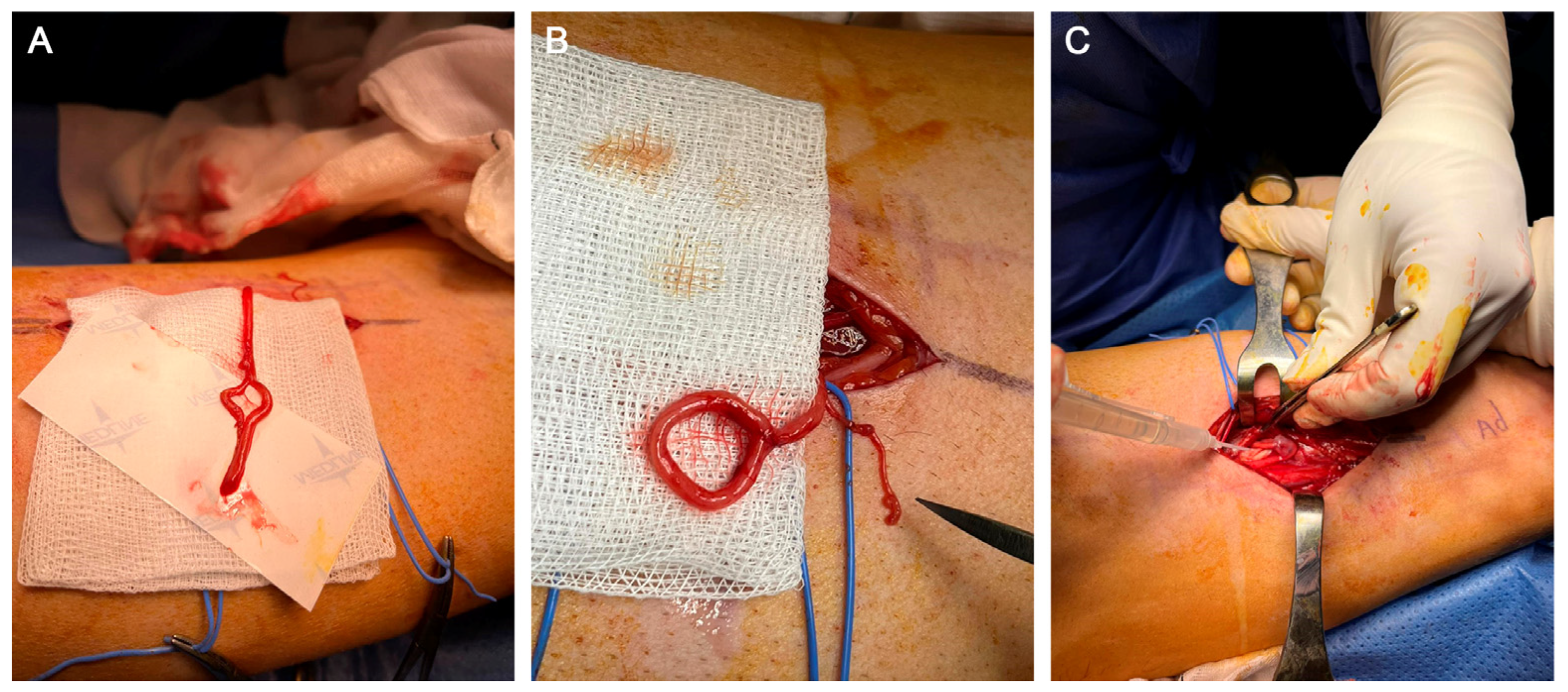
2.3. Surgical Technique
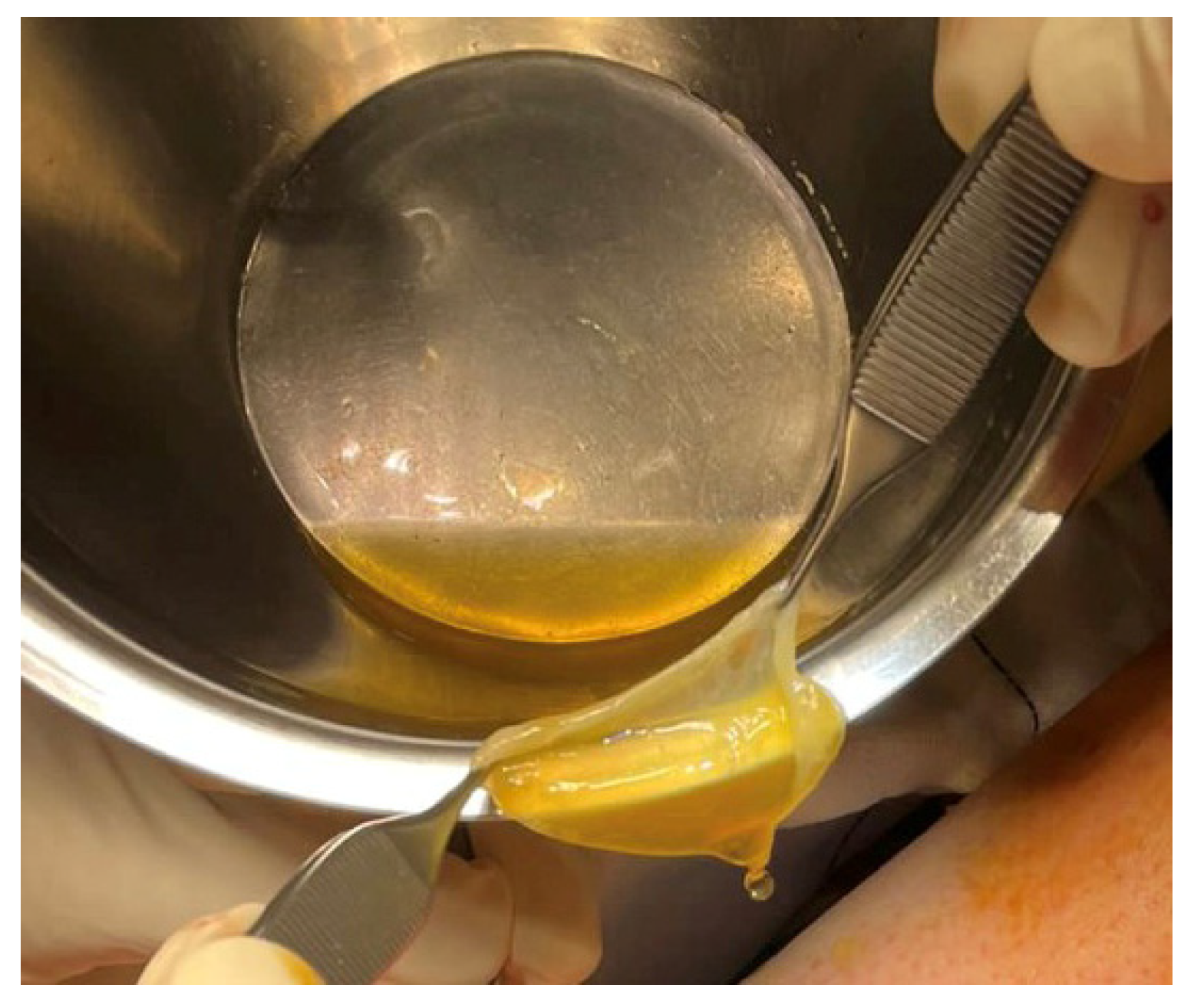
2.4. Plasma Rich in Growth Factors (PRGF) Preparation and Application
2.5. Postoperative and Evolution
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| IBSN | Infrapatellar branch of the saphenous nerve |
| PRGF | Plasma rich in growth factors |
| PRP | Platelet-rich plasma |
| SN | Saphenous nerve |
| US | Ultrasound |
References
- Dayan, V.; Cura, L.; Cubas, S.; Carriquiry, G. Surgical anatomy of the saphenous nerve. Ann. Thorac. Surg. 2008, 85, 896–900. [Google Scholar] [CrossRef] [PubMed]
- Dunaway, D.J.; Steensen, R.N.; Wiand, W.; Dopirak, R.M. The sartorial branch of the saphenous nerve: Its anatomy at the Jt. line of the knee. Arthroscopy 2005, 21, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Ebraheim, N.A.; Mekhail, A.O. The infrapatellar branch of the saphenous nerve: An anatomic study. J. Orthop. Trauma 1997, 11, 195–199. [Google Scholar] [CrossRef]
- Kerver, A.L.; Leliveld, M.S.; den Hartog, D.; Verhofstad, M.H.; Kleinrensink, G.J. The surgical anatomy of the infrapatellar branch of the saphenous nerve in relation to incisions for anteromedial knee surgery. J. Bone Jt. Surg. Am. 2013, 95, 2119–2125. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; Yu, J.-K.; Ao, Y.-F.; Yu, C.-L.; Peng, L.-B.; Lin, C.-Y.; Zhang, J.-Y.; Fu, X. Relationship between different skin incisions and the injury of the infrapatellar branch of the saphenous nerve during anterior cruciate ligament reconstruction. Chin. Med. J. 2007, 120, 1127–1130. [Google Scholar] [CrossRef] [PubMed]
- Portland, G.H.; Martin, D.; Keene, G.; Menz, T. Injury to the infrapatellar branch of the saphenous nerve in anterior cruciate ligament reconstruction: Comparison of horizontal versus vertical harvest site incisions. Arthroscopy 2005, 21, 281–285. [Google Scholar] [CrossRef]
- Song, M.H.; Kim, B.H.; Ahn, S.J.; Yoo, S.H.; Shin, S.H. Preventing lateral skin numbness after medial unicompartmental knee arthroplasty. Clin. Orthop. Surg. 2010, 2, 232–236. [Google Scholar] [CrossRef]
- Wylde, V.; Hewlett, S.; Learmonth, I.D.; Dieppe, P. Persistent pain after Jt. replacement: Prevalence, sensory qualities, and postoperative determinants. Pain 2011, 152, 566–572. [Google Scholar] [CrossRef]
- Sipahioglu, S.; Zehir, S.; Sarikaya, B.; Levent, A. Injury of the infrapatellar branch of the saphenous nerve due to hamstring graft harvest. J. Orthop. Surg. 2017, 25, 2309499017690995. [Google Scholar] [CrossRef]
- Papastergiou, S.G.; Voulgaropoulos, H.; Mikalef, P.; Ziogas, E.; Pappis, G.; Giannakopoulos, I. Injuries to the infrapatellar branch(es) of the saphenous nerve in anterior cruciate ligament reconstruction with four-strand hamstring tendon autograft: Vertical versus horizontal incision for harvest. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 789–793. [Google Scholar] [CrossRef]
- Sabat, D.; Kumar, V. Nerve injury during hamstring graft harvest: A prospective comparative study of three different incisions. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 2089–2095. [Google Scholar] [CrossRef] [PubMed]
- Spicer, D.D.; Blagg, S.E.; Unwin, A.J.; Allum, R.L. Anterior knee symptoms after four-strand hamstring tendon anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2000, 8, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Mochizuki, T.; Akita, K.; Muneta, T.; Sato, T. Anatomical bases for minimizing sensory disturbance after arthroscopically-assisted anterior cruciate ligament reconstruction using medial hamstring tendons. Surg. Radiol. Anat. 2003, 25, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Katsoulis, E.; Court-Brown, C.; Giannoudis, P.V. Incidence and aetiology of anterior knee pain after intramedullary nailing of the femur and tibia. J. Bone Jt. Surg. Br. 2006, 88, 576–580. [Google Scholar] [CrossRef] [PubMed]
- Leliveld, M.S.; Verhofstad, M.H. Injury to the infrapatellar branch of the saphenous nerve, a possible cause for anterior knee pain after tibial nailing? Injury 2012, 43, 779–783. [Google Scholar] [CrossRef] [PubMed]
- Shi, G.G.; Kumar, A.R.; Ledford, C.K.; Ortiguera, C.J.; Wilke, B.K. Infrapatellar Saphenous Nerve Is at Risk During Tibial Nailing: An Anatomic Study. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2021, 5, e21.00007. [Google Scholar] [CrossRef] [PubMed]
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D. The CARE guidelines: Consensus-based clinical case reporting guideline development. BMJ Case Rep. 2013, 2013, 38–43. [Google Scholar] [CrossRef]
- Anitua, E.; Prado, R.; Nurden, A.T.; Nurden, P. Characterization of Plasma Rich in Growth Factors (PRGF): Components and formulations. In Platelet Rich Plasma in Orthopaedics and Sports Medicine; Anitua, E., Cugat, R., Sánchez, M., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 29–45. [Google Scholar]
- Hunter, L.Y.; Louis, D.S.; Ricciardi, J.R.; O’Connor, G.A. The saphenous nerve: Its course and importance in medial arthrotomy. Am. J. Sports Med. 1979, 7, 227–230. [Google Scholar] [CrossRef]
- Grabowski, R.; Gobbi, A.; Zabierek, S.; Domzalski, M.E. Nonspecific Chronic Anteromedial Knee Pain Neuroma as a Cause of Infrapatellar Pain Syndrome: Case Study and Literature Review. Orthop. J. Sports Med. 2018, 6, 2325967117751042. [Google Scholar] [CrossRef]
- Mochida, H.; Kikuchi, S. Injury to infrapatellar branch of saphenous nerve in arthroscopic knee surgery. Clin. Orthop. Relat. Res. 1995, 320, 88–94. [Google Scholar] [CrossRef]
- Marder, R.A.; Raskind, J.R.; Carroll, M. Prospective evaluation of arthroscopically assisted anterior cruciate ligament reconstruction. Patellar tendon versus semitendinosus and gracilis tendons. Am. J. Sports Med. 1991, 19, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, D.; Calvo, R.; Vaisman, A.; Campero, M.; Moraga, C. Injury to the infrapatellar branch of the saphenous nerve in ACL reconstruction with the hamstrings technique: Clinical and electrophysiological study. Knee 2008, 15, 360–363. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.V.; Mezian, K.; Nanka, O.; Wu, W.T.; Lou, Y.M.; Wang, J.C.; Martinoli, C.; Ozcakar, L. Ultrasound Imaging for the Cutaneous Nerves of the Extremities and Relevant Entrapment Syndromes: From Anatomy to Clinical Implications. J. Clin. Med. 2018, 7, 457. [Google Scholar] [CrossRef]
- Saranteas, T.; Anagnostis, G.; Paraskeuopoulos, T.; Koulalis, D.; Kokkalis, Z.; Nakou, M.; Anagnostopoulou, S.; Kostopanagiotou, G. Anatomy and clinical implications of the ultrasound-guided subsartorial saphenous nerve block. Reg. Anesth. Pain Med. 2011, 36, 399–402. [Google Scholar] [CrossRef] [PubMed]
- Valls, J.M.O.; Vallejo, R.; Pais, P.L.; Soto, E.; Rodriguez, D.T.; Cedeno, D.L.; Tornero, C.T.; Rodriguez, M.Q.; Gonzalez, A.B.; Escudero, J.A. Anatomic and Ultrasonographic Evaluation of the Knee Sensory Innervation: A Cadaveric Study to Determine Anatomic Targets in the Treatment of Chronic Knee Pain. Reg. Anesth. Pain Med. 2017, 42, 90–98. [Google Scholar] [CrossRef]
- Tsai, P.B.; Karnwal, A.; Kakazu, C.; Tokhner, V.; Julka, I.S. Efficacy of an ultrasound-guided subsartorial approach to saphenous nerve block: A case series. Can. J. Anaesth. 2010, 57, 683–688. [Google Scholar] [CrossRef]
- Bhatia, A.; Peng, P.; Cohen, S.P. Radiofrequency Procedures to Relieve Chronic Knee Pain: An Evidence-Based Narrative Review. Reg. Anesth. Pain Med. 2016, 41, 501–510. [Google Scholar] [CrossRef]
- Davis, T.; Loudermilk, E.; De Palma, M.; Hunter, C.; Lindley, D.; Patel, N.; Choi, D.; Soloman, M.; Gupta, A.; Desai, M.; et al. Prospective, Multicenter, Randomized, Crossover Clinical Trial Comparing the Safety and Effectiveness of Cooled Radiofrequency Ablation With Corticosteroid Injection in the Management of Knee Pain From Osteoarthritis. Reg. Anesth. Pain Med. 2018, 43, 84–91. [Google Scholar] [CrossRef]
- Pearce, B. Nonoperative treatment of recalcitrant neuritis of the infrapatellar saphenous nerve: A case series. J. Med. Case Rep. 2021, 15, 378. [Google Scholar] [CrossRef]
- Sánchez, M.; Garate, A.; Bilbao, A.M.; Oraa, J.; Yangüela, F.; Sánchez, P.; Guadilla, J.; Aizpurua, B.; Azofra, J.; Fiz, N.; et al. Platelet-Rich Plasma for Injured Peripheral Nerves: Biological Repair Process and Clinical Application Guidelines. In Demystifying Polyneuropathy-Recent Advances and New Directions; Ambrosi, P., Ed.; IntechOpen: London, UK, 2019. [Google Scholar]
- Sanchez, M.; Garate, A.; Delgado, D.; Padilla, S. Platelet-rich plasma, an adjuvant biological therapy to assist peripheral nerve repair. Neural Regen. Res. 2017, 12, 47–52. [Google Scholar]
- de Cortazar, U.G.; Padilla, S.; Lobato, E.; Delgado, D.; Sanchez, M. Intraneural Platelet-Rich Plasma Injections for the Treatment of Radial Nerve Section: A Case Report. J. Clin. Med. 2018, 7, 13. [Google Scholar] [CrossRef] [PubMed]
- Galan, V.; Inigo-Dendariarena, I.; Galan, I.; Prado, R.; Padilla, S.; Anitua, E. The Effectiveness of Plasma Rich in Growth Factors (PRGF) in the Treatment of Nerve Compression Syndromes of the Upper Extremity: A Retrospective Observational Clinical Study. J. Clin. Med. 2022, 11, 4789. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Padilla, S.; Prado, R.; Alkhraisat, M.H. Platelet-rich plasma: Are the obtaining methods, classification and clinical outcome always connected? Regen. Med. 2022, 17, 887–890. [Google Scholar] [CrossRef]
- Sanchez, M.; Anitua, E.; Delgado, D.; Sanchez, P.; Prado, R.; Orive, G.; Padilla, S. Platelet-rich plasma, a source of autologous growth factors and biomimetic scaffold for peripheral nerve regeneration. Expert Opin. Biol. Ther. 2017, 17, 197–212. [Google Scholar] [CrossRef] [PubMed]
- Dellon, A.L.; Mackinnon, S.E. Treatment of the painful neuroma by neuroma resection and muscle implantation. Plast. Reconstr. Surg. 1986, 77, 427–438. [Google Scholar] [CrossRef] [PubMed]
- Schur, M.D.; Sochol, K.M.; Lefebvre, R.; Stevanovic, M. Treatment of Iatrogenic Saphenous Neuroma after Knee Arthroscopy with Excision and Allograft Reconstruction. Plast. Reconstr. Surg. Glob. Open 2021, 9, e3403. [Google Scholar] [CrossRef] [PubMed]
- Novak, C.B.; van Vliet, D.; Mackinnon, S.E. Subjective outcome following surgical management of upper extremity neuromas. J. Hand Surg. Am. 1995, 20, 221–226. [Google Scholar] [CrossRef]
- Aszmann, O.C.; Moser, V.; Frey, M. Treatment of painful neuromas via end-to-side neurorraphy. Handchir. Mikrochir. Plast. Chir. 2010, 42, 225–232. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fahandezh-Saddi Díaz, H.; Ríos Luna, A.; Villanueva Martínez, M.; Cantero Yubero, M.E.; Prado, R.; Padilla, S.; Anitua, E. Surgical Treatment of Saphenous Nerve Injury Assisted by Plasma Rich in Growth Factors (PRGF): Lessons from a Case Report. Clin. Pract. 2023, 13, 1090-1099. https://doi.org/10.3390/clinpract13050097
Fahandezh-Saddi Díaz H, Ríos Luna A, Villanueva Martínez M, Cantero Yubero ME, Prado R, Padilla S, Anitua E. Surgical Treatment of Saphenous Nerve Injury Assisted by Plasma Rich in Growth Factors (PRGF): Lessons from a Case Report. Clinics and Practice. 2023; 13(5):1090-1099. https://doi.org/10.3390/clinpract13050097
Chicago/Turabian StyleFahandezh-Saddi Díaz, Homid, Antonio Ríos Luna, Manuel Villanueva Martínez, María Elena Cantero Yubero, Roberto Prado, Sabino Padilla, and Eduardo Anitua. 2023. "Surgical Treatment of Saphenous Nerve Injury Assisted by Plasma Rich in Growth Factors (PRGF): Lessons from a Case Report" Clinics and Practice 13, no. 5: 1090-1099. https://doi.org/10.3390/clinpract13050097
APA StyleFahandezh-Saddi Díaz, H., Ríos Luna, A., Villanueva Martínez, M., Cantero Yubero, M. E., Prado, R., Padilla, S., & Anitua, E. (2023). Surgical Treatment of Saphenous Nerve Injury Assisted by Plasma Rich in Growth Factors (PRGF): Lessons from a Case Report. Clinics and Practice, 13(5), 1090-1099. https://doi.org/10.3390/clinpract13050097