
Chronological Rehabilitation Treatment Varying by Stage for Constructive Disability

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
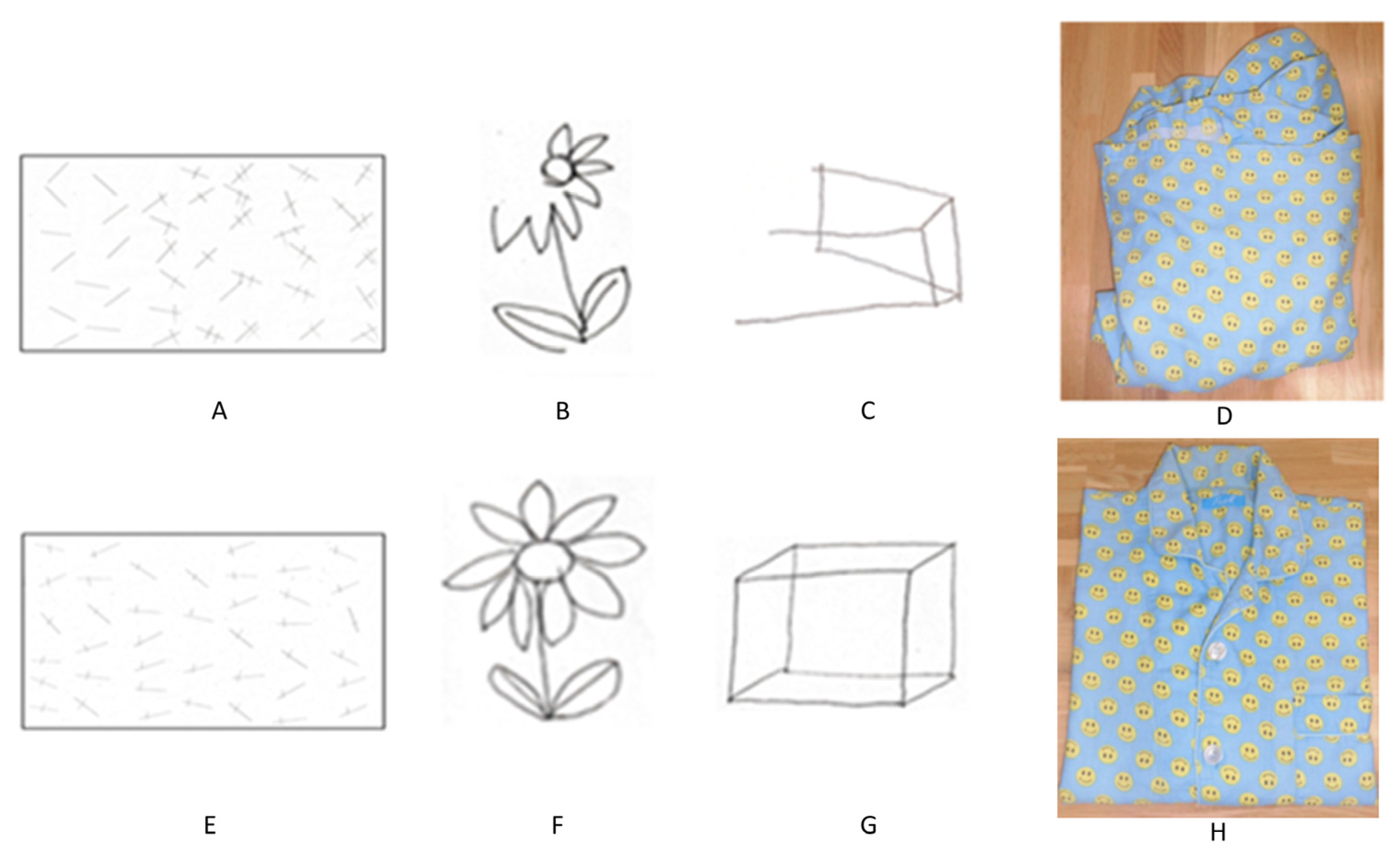
2.1. Initial Evaluation
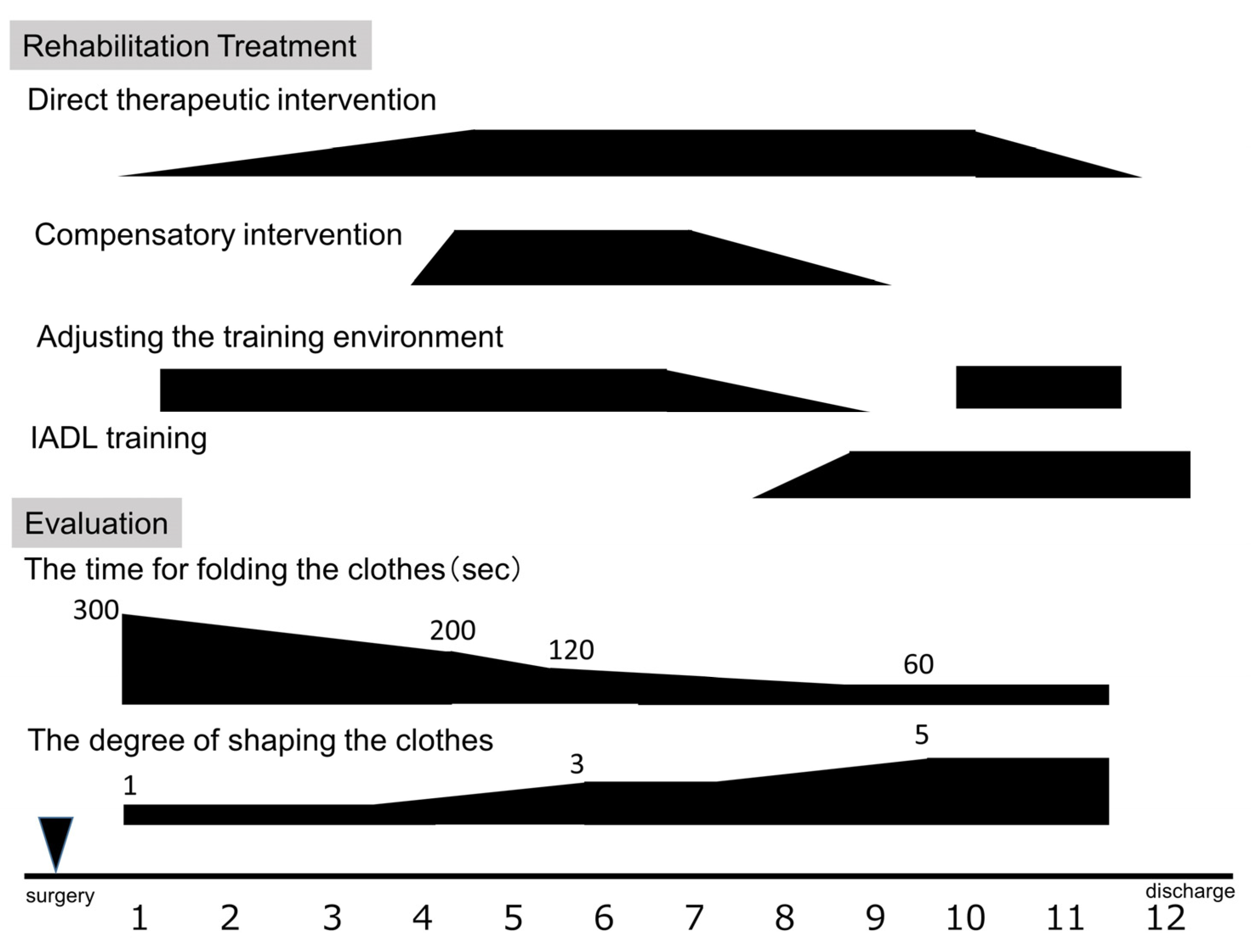
2.2. Intervention
2.3. Occupational Therapy Course
- (1)
- Phase 0
- (2)
- Phase 1
- (3)
- Phase 2
- (4)
- Phase 3
2.4. Final Evaluation
3. Discussion
3.1. Impact of Configuration Disorders on Daily Life
3.2. Evaluation of Constructive Disability
3.3. Rehabilitation Approaches and Techniques
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liepmann, H. Das krankheitsbild der apraxie (“motorischen asymbolie”) auf grund eines falles von Einseitiger apraxie. Monatsschrift Psychiatr. Neurol. 1990, 8, 182–197. [Google Scholar] [CrossRef]
- Gainotti, G.; Trojano, L. Constructional apraxia. Handb. Clin. Neurol. 2018, 151, 331–348. [Google Scholar] [CrossRef] [PubMed]
- Arena, R.; Gainotti, G. Constructional apraxia and visuoperceptive disabilities in relation to laterality of cerebral lesions. Cortex 1978, 14, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Luria, A.R.; Tsvetkova, L.S. The programming of constructive activity in local brain injuries. Neuropsychologia 1964, 2, 95–107. [Google Scholar] [CrossRef]
- Kleist, K. Kriegsverletzungen des Gehirns inihrer Bedeutung fur die Hirnlokalisation und Hirnpathologie. In Handbuch der Arztlichen Erfahrung im Weltkriege, 4; Schjerning, O., Ed.; Leipzig: Berlin, Germany, 1934. [Google Scholar]
- Piercy, M.; Hecaen, H.; De Ajuriaguerra, J. Constructional apraxia associated with unilateral cerebral lesions-left and right sided cases compared. Brain 1960, 83, 225–242. [Google Scholar] [CrossRef] [PubMed]
- Russell, C.; Deidda, C.; Malhotra, B.; Crinion, J.T.; Merola, S.; Husain, M. A deficit of spatial remapping in constructional apraxia after right-hemisphere stroke. Brain 2010, 133, 1239–1251. [Google Scholar] [CrossRef] [PubMed]
- Kawahara, D.; Nagata, Y. T1-weighted and T2-weighted MRI image synthesis with convolutional generative adversarial networks. Rep. Pract. Oncol. Radiother. 2021, 26, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Strub, R.L.; Black, F.W. The Mental Status Examination in Neurology, 4th ed.; F.A. Davis Company: Philadelphia, PA, USA, 2000; pp. 101–103. [Google Scholar]
- MacDonald, S.; Shumway, E. Optimizing our evidence map for cognitive-communication interventions: How it can guide us to better outcomes for adults living with acquired brain injury. Int. J. Lang. Commun. Disord. 2022. [Google Scholar] [CrossRef]
- Tajiri, H.; Mitsuya, K.; Nishimura, T. Employment Support for Brain Tumor Patients and Survivors. J. Rehabil. Med. 2019, 59, 637–644. [Google Scholar] [CrossRef]
- Watanabe, S. Interventions aiding return to work in clients with cognitive and behavioral disorders associated with traumatic brain injury. Work 2013, 45, 273–277. [Google Scholar] [PubMed]
- Wehman, P.H.; Kreutzer, J.S.; West, M.D.; Sherron, P.D.; Zasler, N.D.; Groah, C.H.; Stonnington, H.H.; Burns, C.T.; Sale, P.R. Return to work for persons with traumatic brain injury: A supported employment approach. Arch. Phys. Med. Rehabil. 1990, 71, 1047–1052. [Google Scholar] [PubMed]
- Diller, L.; Ben-Yishay, Y.; Gerstman, L.; Goodkin, R.; Gordon, W.; Weinberg, J. Training hemiplegics to pass block designs. Rehabil. Monogr. 1974, 50, 1–85. [Google Scholar]
- Gallagher, M.; Wilkinson, D.; Sakel, M. Hemispatial neglect: Clinical features, assessment, and treatment. Br. J. Neurosci. Nurs. 2013, 9, 273–277. [Google Scholar] [CrossRef]
- Halligan, P.W.; Cockburn, J.; Wilson, B. Behavioral assessment of visual neglect. Neuropsychol. Rehabil. 1991, 1, 5–32. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okamoto, T.; Mano, T. Chronological Rehabilitation Treatment Varying by Stage for Constructive Disability. Clin. Pract. 2023, 13, 917-923. https://doi.org/10.3390/clinpract13040084
Okamoto T, Mano T. Chronological Rehabilitation Treatment Varying by Stage for Constructive Disability. Clinics and Practice. 2023; 13(4):917-923. https://doi.org/10.3390/clinpract13040084
Chicago/Turabian StyleOkamoto, Takana, and Tomoo Mano. 2023. "Chronological Rehabilitation Treatment Varying by Stage for Constructive Disability" Clinics and Practice 13, no. 4: 917-923. https://doi.org/10.3390/clinpract13040084
APA StyleOkamoto, T., & Mano, T. (2023). Chronological Rehabilitation Treatment Varying by Stage for Constructive Disability. Clinics and Practice, 13(4), 917-923. https://doi.org/10.3390/clinpract13040084