
Treatment with Testosterone Therapy in Type 2 Diabetic Hypogonadal Adult Males: A Systematic Review and Meta-Analysis

 , , , and
, , , and
Abstract
1. Introduction
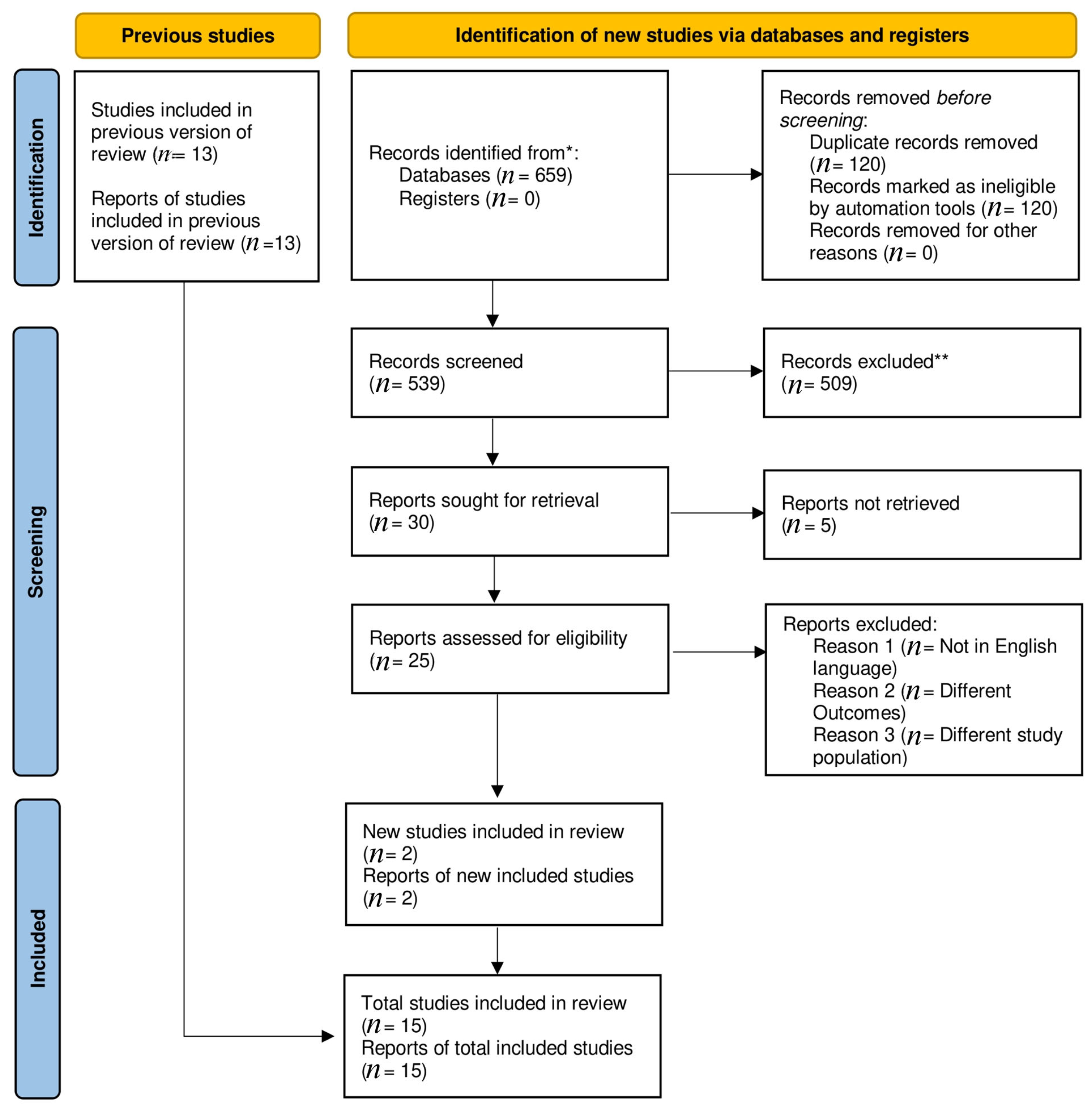
2. Materials and Methods
- English publications.
- Study design: eligible, completed, randomized clinical trials or observational studies were extracted to perform the meta-analysis.
- Patient population: all patients with confirmed type 2 diabetes who met the criteria of hypogonadism.
- Exposure: patients who received testosterone therapy.
- Comparison: this includes the non-TRT group, which received the usual standard of care or placebo.
- Primary outcomes: effects on glucose metabolism and post-treatment hormonal levels.
- Secondary outcomes: cholesterol levels, BMI, waist circumference, body fat, and systolic and diastolic blood pressure.
- No clear definitions of the diagnosis of late-onset hypogonadism and T2DM, population, dosage and method of testosterone administration, or outcome evaluation.
- Insufficient data for estimating a mean difference (MD) with a 95% confidence interval (CI).
- Duplicates of previous publications.
3. Results
3.1. Baseline Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Total no. of Patients | Hypogonadism Cut off Point | No. of Patients | Age (Mean ± SD) | Waist Circumference (cm) (Mean ± SD) | BMI (Kg/m2) (Mean ± SD) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| TRT | Placebo | TRT | Placebo | TRT | Placebo | TRT | Placebo | ||||
| Dhindsa (2015) [14] | RCT | 34 | FT < 225 pmmol/L | 20 | 14 | 54.6 ± 7.9 | 54.6± 7.9 | 128 ± 20 | 124 ± 30 | 39.0 ± 7.6 | 39.4 ± 7.9 |
| Gianatti (2014) [8] | RCT | 67 | TT < 12 nmmol/L | 37 | 30 | 62 ± 2.5 | 62± 2.5 | 110 ± 4.2 | 115 ± 2.75 | ||
| Hackett (2014) [15] | RCT | 186 | TT < 12 nmmol/L | 91 | 95 | 61.2 ± 10.5 | 62.0 ± 9.3 | 115.1 ± 13.1 | 112.6 ± 13.3 | 33.0 ± 6.1 | 32.4 ± 5.5 |
| Jones (2011) [16] | RCT | 137 | TT < 11 nmmol/L | 68 | 69 | 59.9 ± 9.1 | 59.9 ± 9.4 | 112.7 ± 13.35 | 111.7± 15.23 | 32.76± 6.12 | 31.56 ± 5.87 |
| Gopal (2010) [17] | RCT crossover | 22 | FT < 225 pmmol/L | 22 | 22 | 44.23 ±3.29 | 44.23 ±3.29 | 93.25 ± 7.03 | 84.10 ± 13.86 | 25.44 ± 3.57 | 22.10 ± 4.93 |
| Heufelder (2009) [18] | RCT | 32 | TT < 11 nmmol/L | 16 | 16 | 57.3 ± 1.4 | 55.9 ±1.5 | 107.9 ± 1.3 | 105.7± 1.4 | 32.1 ± 0.5 | 32.5 ± 0.6 |
| Kapoor (2006) [19] | RCT crossover | 27 | TT < 12 nmmol/L | 24 | 24 | 64 ± 1.34 | 64 ±1.34 | 115.1 ± 2.4 | 115.1± 2.4 | 33 ±0.86 | 33 ± 0.96 |
| Boyanov (2003) [20] | RCT | 48 | TT < 15 nmmol/ | 24 | 24 | 57.5 ± 4.8 | 57.5 ± 4.8 | N/A | N/A | 31.08 ± 4.79 | 31.01 ± 4.90 |
| Hackett (2018) [21] | RCT | 537 | TT < 12 nmmol/L | 175 | 362 | 58.3± 11 | 65.5 ± 11.8 | N/A | N/A | 32.6 ± 6.4 | 31.7± 5.9 |
| Yassin (2019) [12] | Observational study | 316 | TT < 12.1 nmol/L | 229 | 87 | 58.2 ± 9.6 | 66.4 ± 7.2 | 104.2 ± 7 | 101.1 ± 9.9 | 30.7 ± 4.1 | 29.8 ± 3 |
| Khirpun (2018) [22] | RCT | 80 | serum levels of total testosterone two times less than 12.1 nmol/L or serum levels of free testosterone two times less than 243 pmol/L in combination with at least two symptoms or complaints of a sexual or psychological nature | 40 | 40 | 53.3 ± 5.4 | 54.1 ± 5.6 | 114.3 ± 9.5 | 114.7 ± 9.8 | 34.0 ± 2.6 | 33.6 ± 2.9 |
| Groti (2020) [5] | RCT | 55 | (total testosterone [TT] below 11 nmol/L and free testosterone below 220 pmol/L) on at least two separate morning measurements after an overnight fast, in addition to exhibiting at least two symptoms of sexual dysfunction (less frequent morning and | 28 | 27 | 58.21 ± 7.94 | 62.19 ± 5.90 | 116.48 ± 5.07 | 115 ± 1.47 | 34.03 ± 4.37 | 32.63 ± 3.67 |
| Groti (2018) [23] | RCT | 55 | total testosterone (TT) level <11 nmol/L and/or free testosterone (FT) level <220 pmol/L | 28 | 27 | N/A | N/A | 116.48 ± 5.07 | 116.64 ± 4.96 | 34.03 ± 4.37 | 32.63 ± 3.67 |
| Wittert (2021) [24] | RCT | 1007 | 13.0 nmol/L | 504 | 503 | 59·8 ± 6·3 | 59·6 ± 6·4 | 118·4 ± 12·6 | 117·8 ± 11·6 | 34·8 (5·1) | 34·6 (5·1) |
| Haider (2020) [13] | Prospective observational | 356 | total testosterone levels ≤12.1 nmol/L (350 ng/dL) and symptoms of hypogonadism | 178 | 178 | 61.5 ± 5.4 | 63.7 ± 4.9 | 116.8 ± 14.3 | 116.9 ± 13.6 | 36.5 ± 4.5 | 33.4 ± 5.3 |
| Study | Fasting Plasma Glucose (mmol/L) (Mean ± SD) | Fasting Serum Insulin pmol/L (Mean ± SD) | HBA1c % | Free Testosterone pmol/L (Mean ± SD) | Total Testosterone nmol/L (Mean ± SD) | HOMA-IR (Mean ± SD) | Mean Total Cholesterol mmol/L (Mean ± SD) | Systolic Blood Pressure mm of Hg (Mean ± SD) | Diastolic Blood Pressure mm of Hg (Mean ± SD) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TRT | Placebo | TRT | Placebo | TRT | Placebo | TRT | Placebo | TRT | Placebo | TRT | Placebo | TRT | Placebo | TRT | Placebo | TRT | Placebo | |
| Dhindsa (2015) [14] | 6.99 ± 0.44 | 6.60 ± 0.55 | 13.6 ± 3 rsul | 11.8 ± 2.2 | 6.8 ± 0.9 | 7 ±1.4 | 156.5 ± 45.11 | 145.74 ± 41.6 | 9 ± 2.9 | 8.3 ± 2.8 | 9 ± 2.9 | 8.3 ± 2.8 | 4.06 ± 0.98 | 4.03 ±0.95 | N/A | N/A | N/A | N/A |
| Gianatti (2014) [8] | 9.57 ± 3.78 | 9.11 ± 3.65 | N/A | N/A | 7.7 ± 1.3 | 7.5 ± 1.2 | 187.7 ± 57.0 | 181.2 ± 63.6 | 9.2 ± 3.1 | 8.9 ± 3.8 | 4.1 ± 2.0 | 3.7 ± 2.6 | 4.15± 0.90 | 4.08± 0.9 | 140.2 ± 15.9 | 137.1 ± 13.0 | 79.4 ± 9.4 | 77.5 ± 8.9 |
| Hackett (2014) [15] | 9.05 ± 3.18 | 8.49 ± 2.84 | 20.88 ± 22.83 | 18.17 ± 15.7 | N/A | N/A | 198 ± 49.3 | 202.4 ± 62.1 | 9.2± 2.6 | 9.5± 3.3 | 5.9± 3.8 | 4.9± 3.3 | 4.51± 1.17 | 4.55± 1.01 | 138.6± 17.30 | 136.7± 17.12 | 82.5± 10.23 | 81.6± 9.50 |
| Jones (2011) [16] | 7.9 ± 4.3 | 9.2 ± 3.4 | 12.80 ± 8.95 | 17.86 ± 24.72 | 6.43 ± 2.20 | 7.69 ± 2.77 | 177.57 ± 60.19 | 177.57 ± 60.19 | 10.1 ± 3.7 | 10.1 ± 3.7 | 5.50 ± 6.82 | 6.45 ± 8.75 | 4.7 ± 0.9 | 4.0 ± 1.0 | 115.83 ± 5.15 | 118.40 ± 9.97 | 82.00 ± 6.93 | 79.00 ± 3.16 |
| Gopal (2010) [17] | 7.9 ± 0.2 | 8.3 ± 0.2 | 19.03 ± 0.63 | 16.8 ± 0.87 | 7.5 ± 0.1 | 7.5 ± 0.1 | 200 ± 0.00 | 200 ± 0.00 | 10.5 ± 0.2 | 10.4 ±0.2 | 5.6 ± 0.3 | 6.1 ± 0.4 | N/A | N/A | 104.5± 2.6 | 143.5± 2.1 | 85.6± 0.9 | 85.0± 1.0 |
| Heufelder (2009) [18] | 7.83 ± 0.49 | 7.6 ± 0.43 | 13.68 ± 1.95 | 12.37 ± 1.87 | 7.28 ±0.19 | 7.28 ±0.19 | N/A | N/A | 8.63 ±0.51 | 8.63 ±0.51 | N/A | N/A | 5.11 ±0.17 | 4.95± 0.15 | 127.6± 2.8 | 131± 3.1 | 74± 1.4 | 74± 1.4 |
| Kapoor (2006) [19] | 8.0 ± 2.6 | 8.4 ± 2.8 | N/A | N/A | 10.4 ± 1.6 | 10.3 ± 1.6 | N/A | N/A | 9.56 ± 2.33 | 10.76 ± 3.0 | N/A | N/A | 5.50 ± 1.41 | 5.59 ± 1.49 | 122 ± 8 | 120 ± 8 | 80 ± 4 | 76 ± 6 |
| Boyanov (2003) [20] | N/A | N/A | N/A | N/A | 7.6 ± 1.3 | 7.5 ± 1.5 | 210 ± 124.5 | 175 ± 67.9 | 9.7 ± 4.4 | 8.9 ± 3.2 | N/A | N/A | 4.5 ± 1.1 | 4.1 ± 1.0 | 141.8± 16.1 | 139.4± 16.8 | 81.4 ± 10.4 | 78.2 ± 10.4 |
| Hackett (2018) [21] | 5.3 ± 0.8 | 4.9 ± 1.3 | N/A | N/A | 5.9 ± 0.2 | 5.9 ± 0.2 | N/A | N/A | 8.2 ± 2.1 | 9.6 ± 2.4 | N/A | N/A | 6.9 ± 1.2 | 6.4 ± 1.4 | 136.9 ± 13.5 | 129.8 ± 12.7 | 81.2 ± 8.9 | 84.7 ± 6.7 |
| Yassin (2019) [12] | 8.1 ± 3.7 | 8.7 ± 5.0 | N/A | N/A | 7.8 ± 2.4 | 7.9 ± 2.4 | 208 ± 142 | 223 ± 140 | 9.6 ± 2.7 | 9.9 ± 2.6 | N/A | N/A | 6.1 ± 1.2 | 5.9 ± 1.5 | N/A | N/A | N/A | N/A |
| Khirpun (2018) [22] | 10.06 ± 1.44 | 9.77 ± 1.40 | N/A | N/A | 8.12 ± 1.04 | 7.89 ± 0.77 | 208 ± 142 | 223 ± 140 | 7.24 ± 1.97 | 7.96 ± 1.34 | 11.45 ± 7.34 | 10.82 ± 6.52 | 5.31 ± 0.91 | 5.11 ± 0.85 | 134.64 ± 10.71 | 138.15 ± 13.24 | 77.50 ± 5.85 | 78.89 ± 5.25 |
| Groti (2020) [5] | 10.06 ± 1.44 | 9.60 ± 1.44 | 26.03 ± 15.86 | 24.89 ± 13.90 | 8.12 ± 1.04 | 7.89 ± 0.77 | N/A | N/A | 7.24 ± 1.97 | 7.96 ± 1.34 | 11.45 ± 7.34 | 10.70 ± 6.52 | 5.31 ± 0.91 | 5.31 ± 0.97 | 134.64 ± 10.71 | 138.15 ± 13.24 | 77.50 ± 5.85 | 78.89 ± 5.25 |
| Groti (2018) [23] | 10.06 ± 1.44 | 9.60 ± 1.44 | 26.03 ± 15.86 | 24.89 ± 13.90 | 8.12 ± 1.04 | 7.89 ± 0.77 | N/A | N/A | 7.24 ± 1.97 | 7.96 ± 1.34 | 11.45 ± 7.34 | 10.70 ± 6.52 | 5.31 ± 0.91 | 5.31 ± 0.97 | 134.64 ± 10.71 | 138.15 ± 13.24 | 77.50 ± 5.85 | 78.89 ± 5.25 |
| Wittert (2021) [24] | 6·1 ± 0·9 | 6·1 ± 0·9 | N/A | N/A | 5·7 ± 0·5 | 5·7 ± 0·5 | N/A | N/A | 13·4 ± 4·1 | 13·9 ± 4·6 | N/A | N/A | N/A | N/A | 138.52 ± 14.2 | 139.88 ± 14 | 85.45 ± 8.5 | 85.13 ± 8.3 |
| Haider (2020) [13] | 7.8 ± 1.2 | 6.3 ± 0.7 | 28.6 ± 4.0 | 24.9 ± 2.9 | Forest plot | Forest plot | N/A | N/A | 9.3 ± 1.7 | 9.8 ± 1.1 | 9.8 ± 2.0 | 7.1 ± 1.3 | 8.3 ± 1.1 | 7.1 ± 1.2 | 163.0 ± 13.3 | 145.6 ± 14.6 | 97.6 ± 10.8 | 84.8 ± 10.3 |
3.2. Quality Assessment and Publication Bias
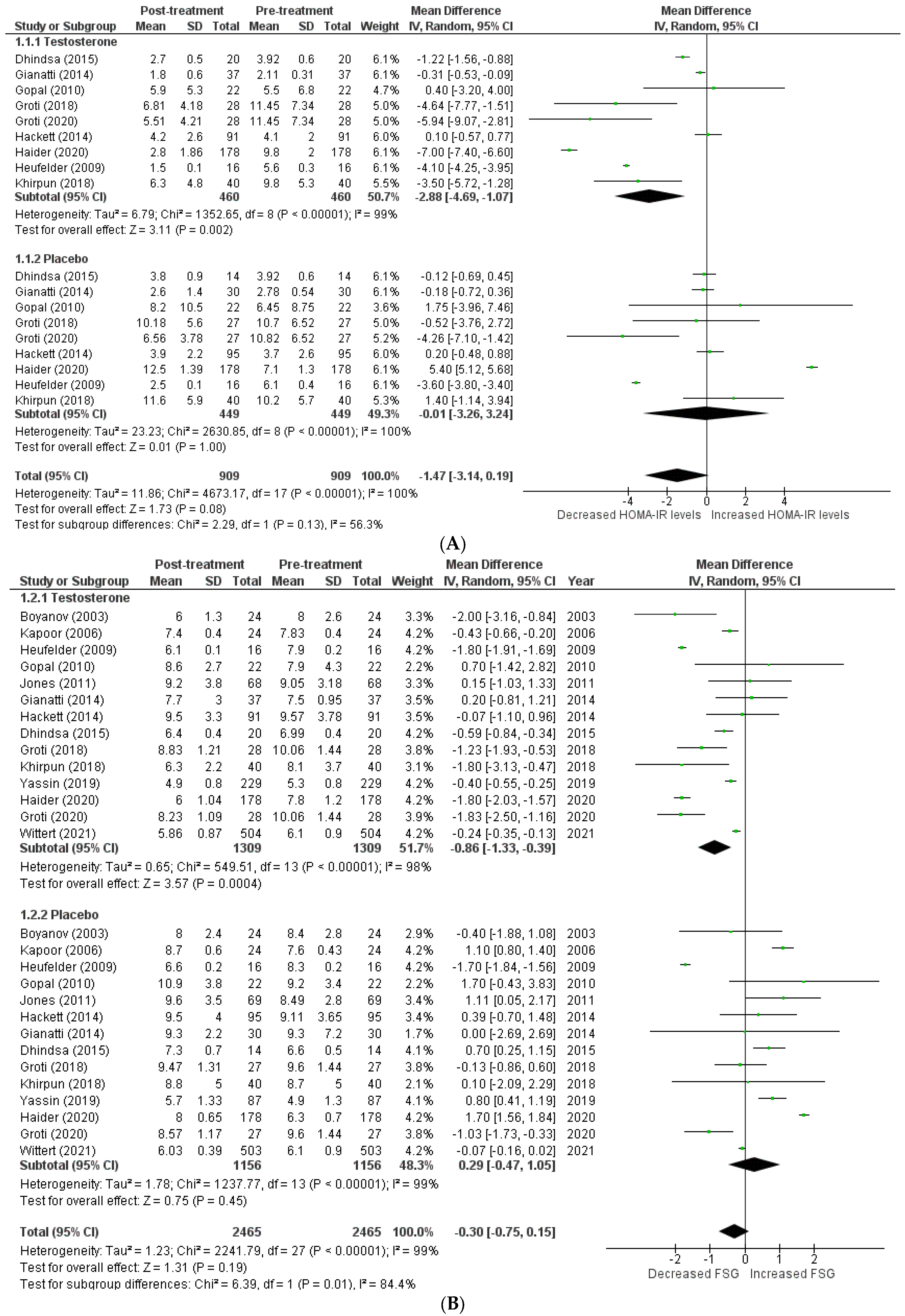
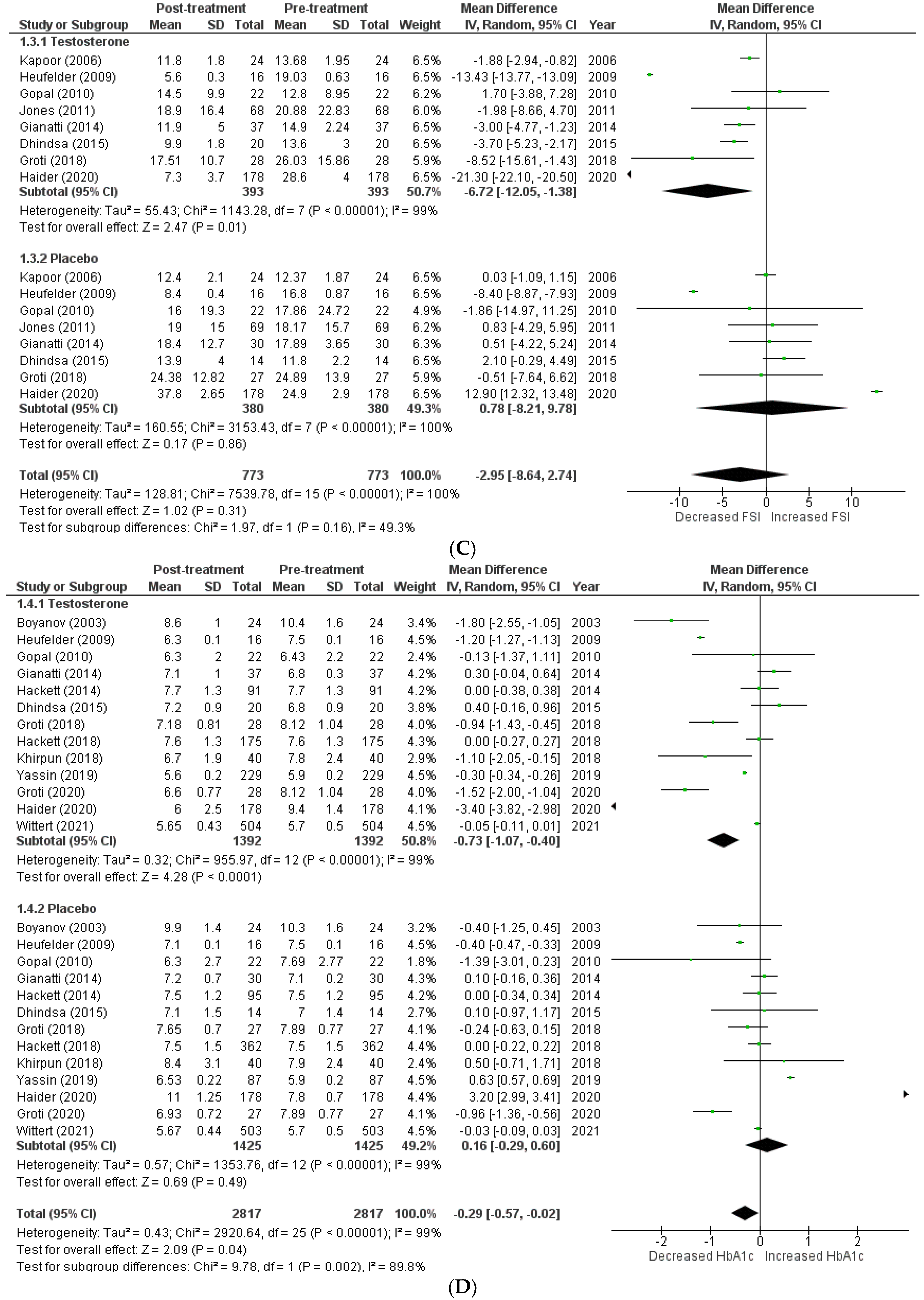
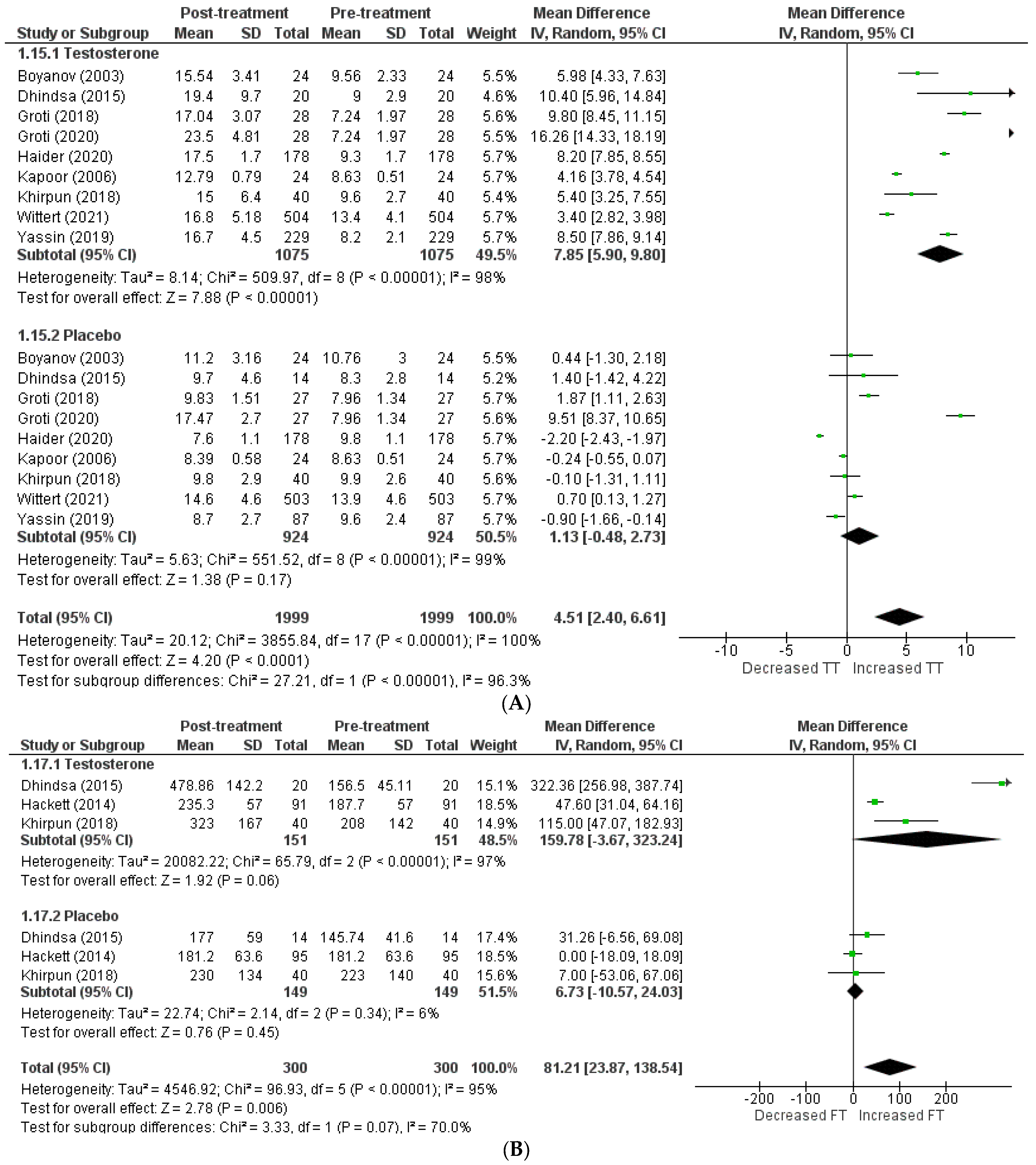
3.3. Primary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bhasin, S.; Brito, J.P.; Cunningham, G.R.; Hayes, F.J.; Hodis, H.N.; Matsumoto, A.M.; Snyder, P.J.; Swerdloff, R.S.; Wu, F.C.; Yialamas, M.A. Testosterone Therapy in Men with Hypogonadism: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2018, 103, 1715–1744. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Miró, M.; Chillarón, J.J.; Pedro-Botet, J. Déficit de testosterona, síndrome metabólico y diabetes mellitus [Testosterone deficiency, metabolic syndrome and diabetes mellitus]. Med. Clin. 2016, 146, 69–73. [Google Scholar] [CrossRef]
- Caliber, M.; Saad, F. Testosterone therapy for prevention and reversal of type 2 diabetes in men with low testosterone. Curr. Opin. Pharmacol. 2021, 58, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, C.R.; Rittel, A.; Sturdivant, R.X.; Wan, J.; Clerc, P.G.; Manning, E.; Jenkins, L.M.; Wardian, J.L.; Graybill, S.D. Glycemic benefits with adherence to testosterone therapy in men with hypogonadism and type 2 diabetes mellitus. Andrology 2021, 9, 1076–1085. [Google Scholar] [CrossRef] [PubMed]
- Antonič, K.G.; Antonič, B.; Žuran, I.; Pfeifer, M. Testosterone treatment longer than 1 year shows more effects on functional hypogonadism and related metabolic, vascular, diabetic and obesity parameters (results of the 2-year clinical trial). Aging Male 2020, 23, 1442–1454. [Google Scholar] [CrossRef]
- Zhang, J.; Yang, B.; Xiao, W.; Li, X.; Li, H. Effects of testosterone supplement treatment in hypogonadal adult males with T2DM: A meta-analysis and systematic review. World J. Urol. 2018, 36, 1315–1326. [Google Scholar] [CrossRef] [PubMed]
- Gianatti, E.J.; Dupuis, P.; Hoermann, R.; Zajac, J.D.; Grossmann, M. Effect of Testosterone Treatment on Constitutional and Sexual Symptoms in Men with Type 2 Diabetes in a Randomized, Placebo-Controlled Clinical Trial. J. Clin. Endocrinol. Metab. 2014, 99, 3821–3828. [Google Scholar] [CrossRef] [PubMed]
- Gianatti, E.J.; Dupuis, P.; Hoermann, R.; Strauss, B.J.; Wentworth, J.M.; Zajac, J.D.; Grossmann, M. Effect of Testosterone Treatment on Glucose Metabolism in Men with Type 2 Diabetes: A Randomized Controlled Trial. Diabetes Care 2014, 37, 2098–2107. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Pereson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. 2015. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 February 2023).
- Yassin, A.; Haider, A.; Haider, K.S.; Caliber, M.; Doros, G.; Saad, F.; Garvey, W.T. Testosterone Therapy in Men with Hypogonadism Prevents Progression from Prediabetes to Type 2 Diabetes: Eight-Year Data from a Registry Study. Diabetes Care 2019, 42, 1104–1111. [Google Scholar] [CrossRef] [PubMed]
- Haider, K.S.; Haider, A.; Saad, F.; Doros, G.; Hanefeld, M.; Dhindsa, S.; Dandona, P.; Traish, A. Remission of type 2 diabetes following long-term treatment with injectable testosterone undecanoate in patients with hypogonadism and type 2 diabetes: 11-year data from a real-world registry study. Diabetes Obes. Metab. 2020, 22, 2055–2068. [Google Scholar] [CrossRef] [PubMed]
- Dhindsa, S.; Ghanim, H.; Batra, M.; Kuhadiya, N.D.; Abuaysheh, S.; Sandhu, S.; Green, K.; Makdissi, A.; Hejna, J.; Chaudhuri, A.; et al. Insulin Resistance and Inflammation in Hypogonadotropic Hypogonadism and Their Reduction after Testosterone Replacement in Men with Type 2 Diabetes. Diabetes Care 2015, 39, 82–91. [Google Scholar] [CrossRef]
- Hackett, G.; Cole, N.; Bhartia, M.; Kennedy, D.; Raju, J.; Wilkinson, P. The BLAST Study Group Testosterone Replacement Therapy Improves Metabolic Parameters in Hypogonadal Men with Type 2 Diabetes but Not in Men with Coexisting Depression: The BLAST Study. J. Sex. Med. 2014, 11, 840–856. [Google Scholar] [CrossRef]
- Jones, T.H.; Arver, S.; Behre, H.M.; Buvat, J.; Meuleman, E.; Moncada, I.; Morales, A.M.; Volterrani, M.; Yellowlees, A.; Howell, J.D.; et al. Testosterone Replacement in Hypogonadal Men with Type 2 Diabetes and/or Metabolic Syndrome (the TIMES2 Study). Diabetes Care 2011, 34, 828–837. [Google Scholar] [CrossRef] [PubMed]
- Gopal, R.A.; Bothra, N.; Acharya, S.V.; Ganesh, H.K.; Bandgar, T.R.; Menon, P.S.; Shah, N.S. Treatment of Hypogonadism with Testosterone in Patients with Type 2 Diabetes Mellitus. Endocr. Pr. 2010, 16, 570–576. [Google Scholar] [CrossRef]
- Heufelder, A.E.; Saad, F.; Bunck, M.C.; Gooren, L. Fifty-two-Week Treatment with Diet and Exercise Plus Transdermal Testosterone Reverses the Metabolic Syndrome and Improves Glycemic Control in Men with Newly Diagnosed Type 2 Diabetes and Subnormal Plasma Testosterone. J. Androl. 2009, 30, 726–733. [Google Scholar] [CrossRef]
- Kapoor, D.; Goodwin, E.; Channer, K.S.; Jones, T.H. Testosterone replacement therapy improves insulin resistance, glycaemic control, visceral adiposity and hypercholesterolaemia in hypogonadal men with type 2 diabetes. Eur. J. Endocrinol. 2006, 154, 899–906. [Google Scholar] [CrossRef]
- Boyanov, M.A.; Boneva, Z.; Christov, V.G. Testosterone supplementation in men with type 2 diabetes, visceral obesity and partial androgen deficiency. Aging Male. 2003, 6, 1–7. [Google Scholar] [CrossRef]
- Hackett, G.; Cole, N.; Mulay, A.; Strange, R.C.; Ramachandran, S. Long-term testosterone therapy in type 2 diabetes is associated with reduced mortality without improvement in conventional cardiovascular risk factors. BJU Int. 2019, 123, 519–529. [Google Scholar] [CrossRef]
- Khripun, I.; Vorobyev, S.; Belousov, I.; Kogan, M.; Zitzmann, M. Influence of testosterone substitution on glycemic control and endothelial markers in men with newly diagnosed functional hypogonadism and type 2 diabetes mellitus: A randomized controlled trial. Aging Male 2019, 22, 241–249. [Google Scholar] [CrossRef]
- Groti, K.; Žuran, I.; Antonič, B.; Foršnarič, L.; Pfeifer, M. The impact of testosterone replacement therapy on glycemic control, vascular function, and components of the metabolic syndrome in obese hypogonadal men with type 2 diabetes. Aging Male 2018, 21, 158–169. [Google Scholar] [CrossRef]
- Wittert, G.; Bracken, K.; Robledo, K.P.; Grossmann, M.; Yeap, B.B.; Handelsman, D.J.; Stuckey, B.; Conway, A.; Inder, W.; McLachlan, R.; et al. Testosterone treatment to prevent or revert type 2 diabetes in men enrolled in a lifestyle programme (T4DM): A randomised, double-blind, placebo-controlled, 2-year, phase 3b trial. Lancet Diabetes Endocrinol. 2021, 9, 32–45. [Google Scholar] [CrossRef]
- Serwaa, D.; Bello, F.A.; Osungbade, K.O.; Nkansah, C.; Osei-Boakye, F.; Appiah, S.K.; Antwi, M.H.; Danquah, M.; Buckman, T.A.; Owusu, E. Prevalence and determinants of low testosterone levels in men with type 2 diabetes mellitus; a case-control study in a district hospital in Ghana. PLOS Glob. Public Health 2021, 1, e0000052. [Google Scholar] [CrossRef]
- Hackett, G. Metabolic Effects of Testosterone Therapy in Men with Type 2 Diabetes and Metabolic Syndrome. Sex. Med. Rev. 2019, 7, 476–490. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E.; Bassil, N.; Alkaade, S. The benefits and risks of testosterone replacement therapy: A review. Ther. Clin. Risk Manag. 2009, 5, 427–448. [Google Scholar] [CrossRef] [PubMed]
- Reddy, K.; Yadav, S. Effect of testosterone replacement therapy on insulin sensitivity and body composition in congenital hypogonadism: A prospective longitudinal follow-up study. J. Postgrad. Med. 2021, 67, 67–74. [Google Scholar]
- Grossmann, M.; Fui, M.N.T.; Cheung, A.S. Late-onset hypogonadism: Metabolic impact. Andrology 2020, 8, 1519–1529. [Google Scholar] [CrossRef]
- Leutner, M.; Matzhold, C.; Bellach, L.; Wohlschläger-Krenn, E.; Winker, R.; Nistler, S.; Endler, G.; Thurner, S.; Klimek, P.; Kautzky-Willer, A. Increase in testosterone levels is related to a lower risk of conversion of prediabetes to manifest diabetes in prediabetic males. Wien. Klin. Wochenschr. 2022, 134, 1–6. [Google Scholar] [CrossRef]
- Kim, S.H.; Park, J.J.; Kim, K.H.; Yang, H.J.; Kim, D.S.; Lee, C.H.; Jeon, Y.S.; Shim, S.R.; Kim, J.H. Efficacy of testosterone replacement therapy for treating metabolic disturbances in late-onset hypogonadism: A systematic review and meta-analysis. Int. Urol. Nephrol. 2021, 53, 1733–1746. [Google Scholar] [CrossRef]
- Kirlangic, O.F.; Yilmaz-Oral, D.; Kaya-Sezginer, E.; Toktanis, G.; Tezgelen, A.S.; Sen, E.; Khanam, A.; Oztekin, C.V.; Gur, S. The Effects of Androgens on Cardiometabolic Syndrome: Current Therapeutic Concepts. Sex. Med. 2020, 8, 132–155. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.K.; Noh, J.; Chang, Y.; Lee, H.Y.; Park, J.J.; Ryu, S.; Kim, J.H. Association between prostate-specific antigen and serum testosterone: A systematic review and meta-analysis. Andrology 2020, 8, 1194–1213. [Google Scholar] [CrossRef] [PubMed]





| Outcome | Testosterone | Placebo | Effect Size [CI] | Overall p-Value | Heterogeneity |
|---|---|---|---|---|---|
| Total cholesterol | −0.71 [−1.22, −0.21] | 0.10 [−016, 0.35] | −0.32 [−0.64, 0.00] | 0.05 | 87.2 |
| Triglyceride | −0.47 [−0.75, −0.20] | 0.03 [−021, 0.27] | −0.23 [−0.47, 0.00] | 0.05 | 86.6 |
| LDL cholesterol | −0.20 [−1.12, 0.73] | 0.17 [−0.13, 0.46] | −0.02 [−0.52, 0.48] | 0.94 | 0 |
| HDL cholesterol | 0.10 [0.01, 0.20] | 0.03 [−0.07, 0.13] | 0.07 [0.00, 0.13] | 0.04 | 8.7 |
| Body fat | −0.98 [−1.59, −0.38] | −0.54 [−1.12, 0.03] | −0.75 [−1.17, −0.34] | 0.0004 | 6.4 |
| Waist circumference | −3.98 [−6.48, −1.48] | 0.73 [−1.44, 2.89] | −1.68 [3.43, 0.07] | 0.06 | 87.1 |
| BMI | −1.12 [−2.98, 0.74] | 0.05 [−0.51, 0.61] | −0.56 [−1.48, 0.36] | 0.23 | 27.5 |
| SBP | −0.90 [−12.07, 10.26] | −0.19 [−3.19, 2.81] | −0.51 [−6.24, 5.11] | 0.85 | 0 |
| DBP | −3.09 [−5.52, −0.65] | −0.23 [−1.98, 1.52] | −1.68 [−3.16, −0.21] | 0.03 | 71.3 |
| IIEF | 6.98 [3.62, 10.33] | −3.94 [−10.97, 3.10] | 1.66 [−6.75, 10.06] | 0.70 | 86.7 |
| AMS | −16.80 [−26.96, −6.64] | 4.90 [−9.05, 18.85] | −5.94 [−21.87, 9.98] | 0.46 | 83.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumari, K.; Kumar, R.; Memon, A.; Kumari, B.; Tehrim, M.; Kumari, P.; Shehryar, M.; Islam, H.; Islam, R.; Khatri, M.; et al. Treatment with Testosterone Therapy in Type 2 Diabetic Hypogonadal Adult Males: A Systematic Review and Meta-Analysis. Clin. Pract. 2023, 13, 454-469. https://doi.org/10.3390/clinpract13020041
Kumari K, Kumar R, Memon A, Kumari B, Tehrim M, Kumari P, Shehryar M, Islam H, Islam R, Khatri M, et al. Treatment with Testosterone Therapy in Type 2 Diabetic Hypogonadal Adult Males: A Systematic Review and Meta-Analysis. Clinics and Practice. 2023; 13(2):454-469. https://doi.org/10.3390/clinpract13020041
Chicago/Turabian StyleKumari, Kajol, Rohan Kumar, Areeba Memon, Beena Kumari, Moniba Tehrim, Pooja Kumari, Muhammad Shehryar, Hamza Islam, Rabia Islam, Mahima Khatri, and et al. 2023. "Treatment with Testosterone Therapy in Type 2 Diabetic Hypogonadal Adult Males: A Systematic Review and Meta-Analysis" Clinics and Practice 13, no. 2: 454-469. https://doi.org/10.3390/clinpract13020041
APA StyleKumari, K., Kumar, R., Memon, A., Kumari, B., Tehrim, M., Kumari, P., Shehryar, M., Islam, H., Islam, R., Khatri, M., Kumar, S., & Kumar, A. (2023). Treatment with Testosterone Therapy in Type 2 Diabetic Hypogonadal Adult Males: A Systematic Review and Meta-Analysis. Clinics and Practice, 13(2), 454-469. https://doi.org/10.3390/clinpract13020041