SARS-CoV-2-Associated Obliterative Arteritis Causing Massive Testicular Infarction

 ,
, 

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
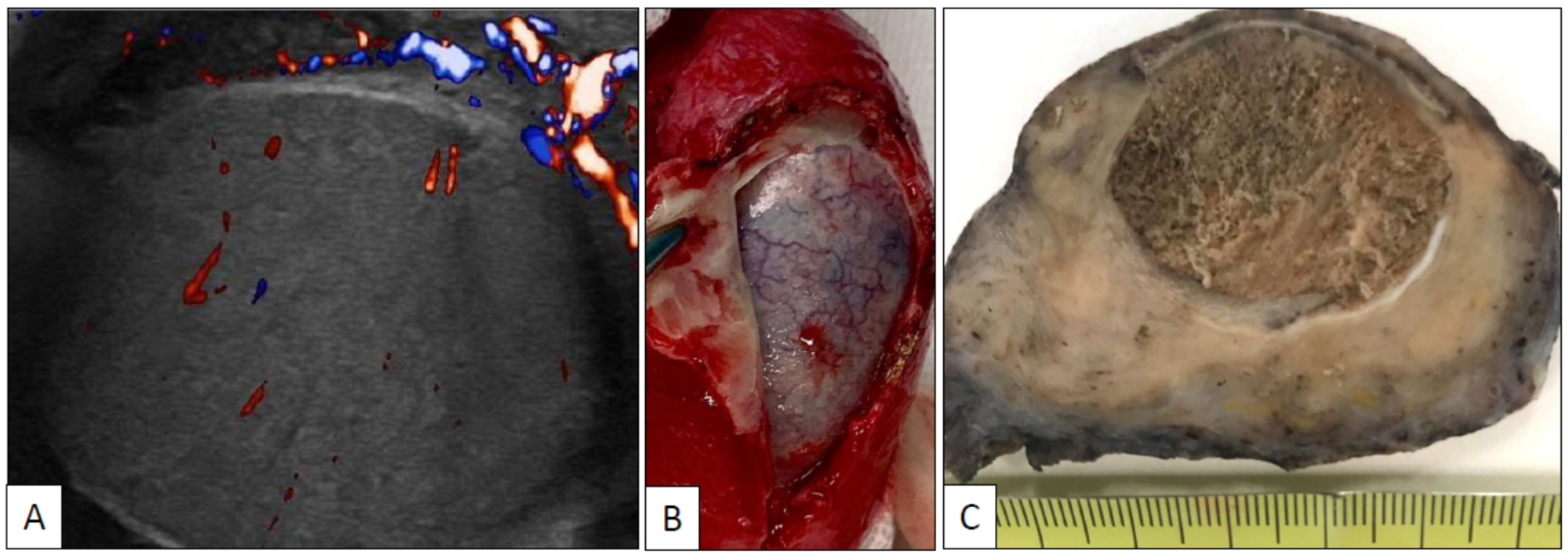
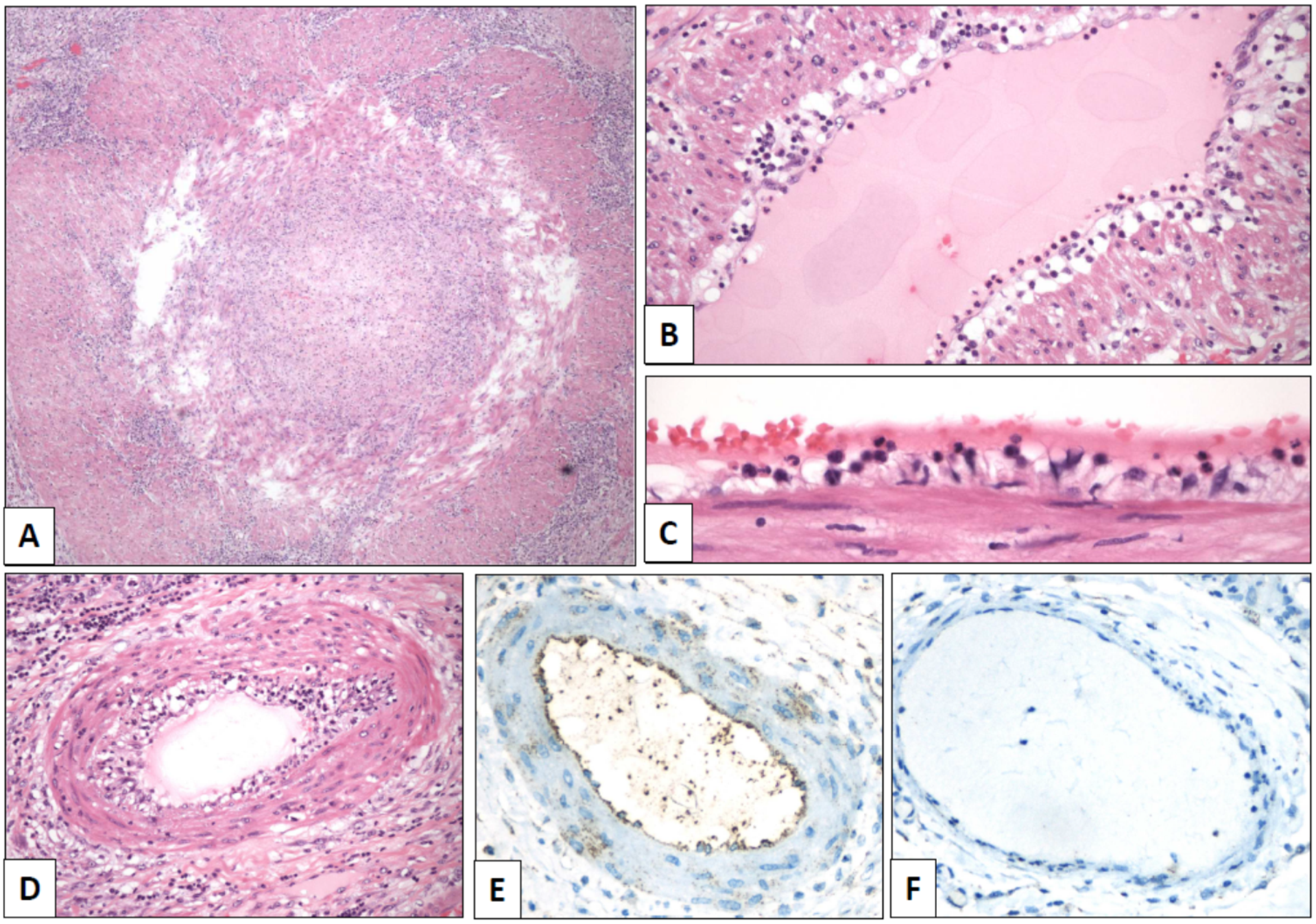
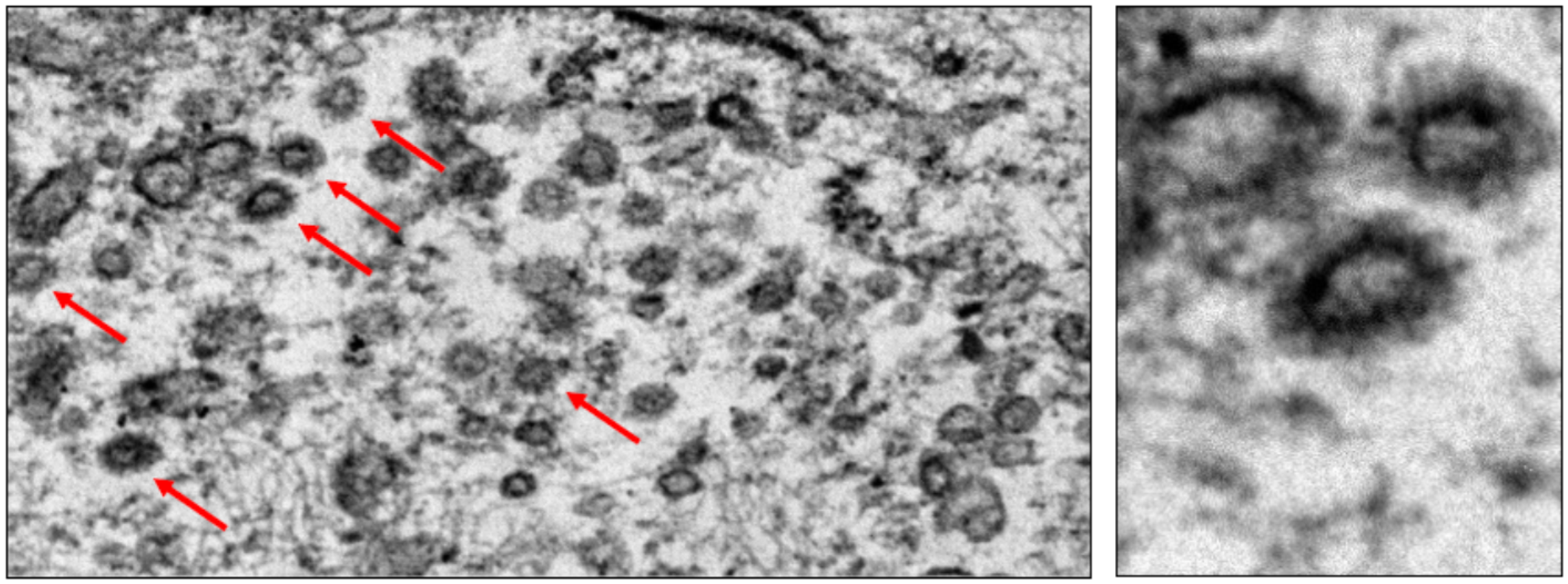
2. Case Report
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Becker, R.C. COVID-19-associated vasculitis and vasculopathy. J. Thromb. Thrombolysis 2020, 50, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Okada, H.; Yoshida, S.; Hara, A.; Ogura, S.; Tomita, H. Vascular endothelial injury exacerbates coronavirus disease 2019: The role of endothelial glycocalyx protection. Microcirculation 2020, e12654. [Google Scholar] [CrossRef] [PubMed]
- Carsana, L.; Sonzogni, A.; Nasr, A.; Rossi, R.S.; Pellegrinelli, A.; Zerbi, P.; Rech, R.; Colombo, R.; Antinori, S.; Corbellino, M.; et al. Pulmonary post-mortem findings in a series of COVID-19 cases from northern Italy: A two-centre descriptive study. Lancet Infect. Dis. 2020, 20, 1135–1140. [Google Scholar] [CrossRef]
- de Sousa, G.C.; de Sousa, T.C.; Sakiyama, M.A.K.; da Silva, J.S.N.L.; de Sousa, E.J.S. Vasculitis-related stroke in young as a presenting feature of novel coronavirus disease (COVID19). Case report. J. Clin. Neurosci. 2020, 79, 169–171. [Google Scholar] [CrossRef] [PubMed]
- Khesrani, L.S.; Chana, K.; Sadar, F.Z.; Dahdouh, A.; Ladjadj, Y.; Bouguermouth, D. Intestinal ischemia secondary to Covid-19. J. Pediatr. Surg. Case Rep. 2020, 61, 101604. [Google Scholar] [CrossRef] [PubMed]
- Bruni, A.; Garofalo, E.; Zuccalà, V.; Currò, G.; Torti, C.; Navarra, G.; De Sarro, G.; Navalesi, P.; Longhini, F.; Ammendola, M. Histopathological findings in a COVID-19 patient affected by ischemic gangrenous cholecystitis. World J. Emerg. Surg. 2020, 15, 43. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Liu, X.; Feng, L.; Xiong, S.; Li, Y.; Chen, L.; Li, Y.; Wang, G.; Li, D.; Fu, B. Impact of SARS-CoV-2 on Male Reproductive Health: A Review of the Literature on Male Reproductive Involvement in COVID-19. Front. Med. 2020, 7, 594364. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Xiao, X.; Zhang, J.; Zafar, M.I.; Wu, C.; Long, Y.; Lu, W.; Pan, F.; Meng, T.; Zhao, K.; et al. Impaired spermatogenesis in COVID-19 patients. EClinicalMedicine 2020, 100604. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parrón, D.; Gartzia, A.; Iturregui, A.M.; Imaz, I.; Manini, C.; García-Olaverri, J.; López, J.I. SARS-CoV-2-Associated Obliterative Arteritis Causing Massive Testicular Infarction. Clin. Pract. 2021, 11, 246-249. https://doi.org/10.3390/clinpract11020037
Parrón D, Gartzia A, Iturregui AM, Imaz I, Manini C, García-Olaverri J, López JI. SARS-CoV-2-Associated Obliterative Arteritis Causing Massive Testicular Infarction. Clinics and Practice. 2021; 11(2):246-249. https://doi.org/10.3390/clinpract11020037
Chicago/Turabian StyleParrón, Dámaso, Ane Gartzia, Ane M. Iturregui, Igone Imaz, Claudia Manini, Jorge García-Olaverri, and José I. López. 2021. "SARS-CoV-2-Associated Obliterative Arteritis Causing Massive Testicular Infarction" Clinics and Practice 11, no. 2: 246-249. https://doi.org/10.3390/clinpract11020037
APA StyleParrón, D., Gartzia, A., Iturregui, A. M., Imaz, I., Manini, C., García-Olaverri, J., & López, J. I. (2021). SARS-CoV-2-Associated Obliterative Arteritis Causing Massive Testicular Infarction. Clinics and Practice, 11(2), 246-249. https://doi.org/10.3390/clinpract11020037