
White Nail as a Static Physical Finding: Revitalization of Physical Examination



{kind=link}
{kind=link}
Abstract
1. Introduction
2. Case Presentation
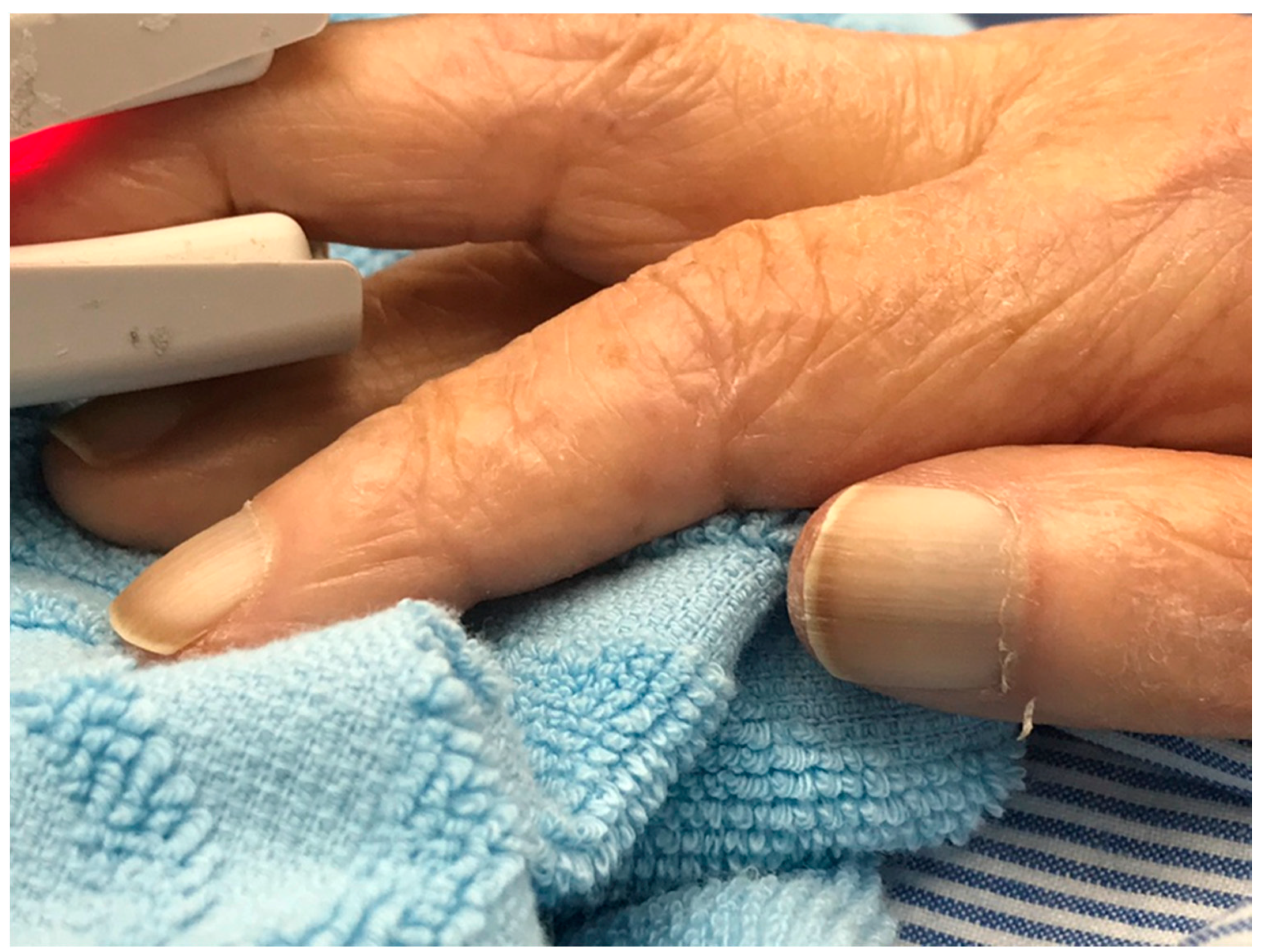
2.1. White Nails in All Nails of the Hands
2.2. White Nails with Sparing of the First Fingernail Bed
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Matsui, K. Physical examinations: Considering their meaning and value. Gen. Med. 2011, 12, 49–50. [Google Scholar] [CrossRef][Green Version]
- Kelly, M.A.; Freeman, L.K.; Dornan, T. Family physicians′ experiences of physical examination. Ann. Fam. Med. 2019, 17, 304–310. [Google Scholar] [CrossRef]
- Mizuno, A.; Kawai, F.; Shimizu, T. Physical examination has been paid less attention to compared to diagnostic imaging: From a bibliometric analysis of PubMed. J. Gen. Fam. Med. 2016, 17, 109–112. [Google Scholar] [CrossRef]
- Iida, J.; Nishigori, H. Physical examination and the physician-patient relationship: A literature review. MedEdPublish 2016, 5, 14. [Google Scholar] [CrossRef]
- Fred, H.L. Hyposkillia: Deficiency of clinical skills. Tex. Heart Inst. J. 2005, 32, 255–257. [Google Scholar] [CrossRef]
- Lee, K.S.; Ahn, K.H. Application of artificial intelligence in early diagnosis of spontaneous preterm labor and birth. Diagnostics 2020, 10, 733. [Google Scholar] [CrossRef]
- Kitamura, S.; Takahashi, K.; Sang, Y.; Fukushima, K.; Tsuji, K.; Wada, J. Deep learning could diagnose diabetic nephropathy with renal pathological immunofluorescent images. Diagnostics 2020, 10, 466. [Google Scholar] [CrossRef]
- Lee, J.-H.; Kim, Y.-T.; Lee, J.-B.; Jeong, S.-N. A performance comparison between automated deep learning and dental professionals in classification of dental implant systems from dental imaging: A multi-center study. Diagnostics 2020, 10, 910. [Google Scholar] [CrossRef]
- Lenfant, M.; Chevallier, O.; Comby, P.-O.; Secco, G.; Haioun, K.; Ricolfi, F.; Lemogne, B.; Loffroy, R. Deep learning versus iterative reconstruction for CT pulmonary angiography in the emergency setting: Improved image quality and reduced radiation dose. Diagnostics 2020, 10, 558. [Google Scholar] [CrossRef]
- Woolf, A.D. How to assess musculoskeletal conditions. History and physical examination. Best Pract. Res. Clin. Rheumatol. 2003, 17, 381–402. [Google Scholar] [CrossRef]
- Tokuda, Y. Diagnostic error in Japan: Call for papers! J. Gen. Fam. Med. 2015, 16, 227–228. [Google Scholar] [CrossRef]
- McGee, S. Evidence-Based Physical Diagnosis, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 154–196. [Google Scholar]
- Fawcett, R.S.; Linford, S.; Stulberg, D.L. Nail abnormalities: Clues to systemic disease. Am. Fam. Physician 2004, 69, 1417–1424. [Google Scholar]
- Pitukweerakul, S.; Pilla, S. Terry′s nails and Lindsay′s nails: Two nail abnormalities in chronic systemic diseases. J. Gen. Intern. Med. 2016, 31, 970. [Google Scholar] [CrossRef][Green Version]
- Don, B.R.; Kaysen, G. Serum albumin: Relationship to inflammation and nutrition. Semin. Dial. 2004, 17, 432–437. [Google Scholar] [CrossRef]
- Touma, E.; Bisharat, N. Trends in admission serum albumin and mortality in patients with hospital readmission. Int. J. Clin. Pract. 2019, 73, e13314. [Google Scholar] [CrossRef]
- Ogino, N.; Aridome, G.; Oshima, J.; Shibata, M.; Watanabe, T.; Kume, K.; Yoshikawa, I.; Harada, M. Serum Albumin concentrations predict hypovolaemia caused by polyethylene glycol plus ascorbic acid prior to colonoscopy in elderly patients. Drugs Aging 2016, 33, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Short, N.; Shah, C. Muehrcke′s lines. Am. J. Med. 2010, 123, 991–992. [Google Scholar] [CrossRef] [PubMed]
- Tully, A.S.; Trayes, K.P.; Studdiford, J.S. Evaluation of nail abnormalities. Am. Fam. Physician 2012, 85, 779–787. [Google Scholar] [PubMed]
- Navarro-Triviño, F.J.; Linares-González, L.; Ródenas-Herranz, T. Terry′s nails as the first clinical sign of autoimmune hepatitis. Rev. Clin. Esp. 2019. [Google Scholar] [CrossRef]
- Meegada, S.; Verma, R. Terry′s nails. Clin. Case Rep. 2020, 8, 404–405. [Google Scholar] [CrossRef]
- Witkowska, A.B.; Jasterzbski, T.J.; Schwartz, R.A. Terry′s nails: A sign of systemic disease. Indian J. Dermatol. 2017, 62, 309–311. [Google Scholar] [PubMed]
- Lindsay, P.G. The half-and-half nail. Arch. Intern. Med. 1967, 119, 583–587. [Google Scholar] [CrossRef] [PubMed]
- Holzberg, M.; Walker, H.K. Terry’s nails: Revised definition and new correlations. Lancet 1984, 1, 896–899. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ohta, R.; Sano, C. White Nail as a Static Physical Finding: Revitalization of Physical Examination. Clin. Pract. 2021, 11, 241-245. https://doi.org/10.3390/clinpract11020036
Ohta R, Sano C. White Nail as a Static Physical Finding: Revitalization of Physical Examination. Clinics and Practice. 2021; 11(2):241-245. https://doi.org/10.3390/clinpract11020036
Chicago/Turabian StyleOhta, Ryuichi, and Chiaki Sano. 2021. "White Nail as a Static Physical Finding: Revitalization of Physical Examination" Clinics and Practice 11, no. 2: 241-245. https://doi.org/10.3390/clinpract11020036
APA StyleOhta, R., & Sano, C. (2021). White Nail as a Static Physical Finding: Revitalization of Physical Examination. Clinics and Practice, 11(2), 241-245. https://doi.org/10.3390/clinpract11020036