
Investigating the Interplay of Toxic Metals and Essential Elements in Cardiovascular Disease



Abstract

1. Introduction
1.1. Overview of Cardiovascular Disease
1.2. Common Causes and Risk Factors for Cardiovascular Disease
1.3. Importance of Metals and Essential Metals in Cardiovascular Diseases
2. Materials and Methods
2.1. Participants Sampling and Description
2.2. Essential Element and Metal Quantification
2.3. Measuring Cardiovascular Variables
2.4. Statistical Analysis
2.4.1. Descriptive Statistics
2.4.2. Bayesian Kernel Machine Regression (BKMR)
2.4.3. Weighted Quantile Sum Regression (WQSR)
2.4.4. Quantile g-Computation
3. Results
3.1. Descriptive Analysis of Sex, Ethnicity, and Age
3.2. Correlation Between Variables of Interest
3.3. BKMR Analysis
3.3.1. Posterior Inclusion Probabilities (PIPs)
3.3.2. BKMR Models Showing PIP for Exposure to Metals and Essential Elements and by Health Outcome
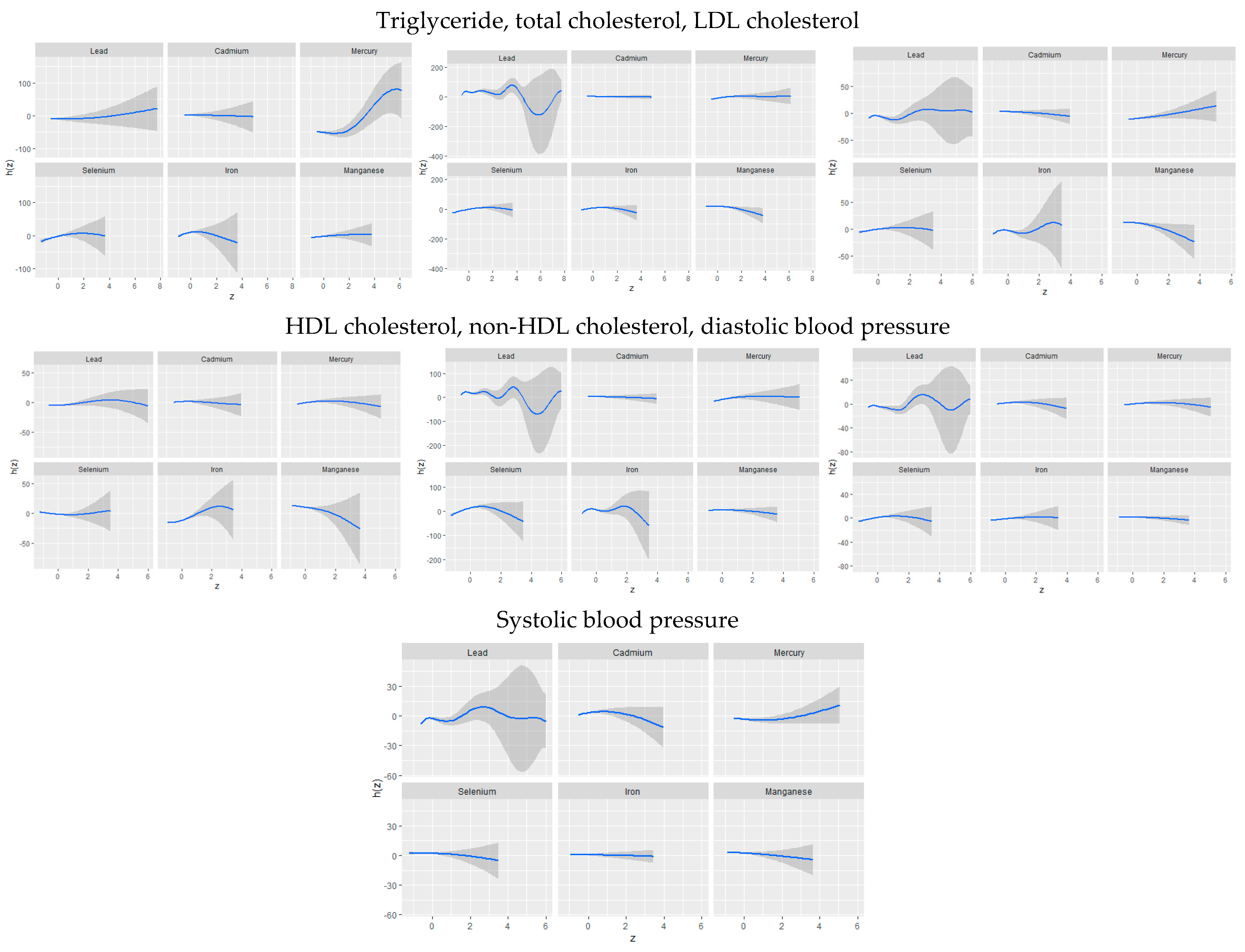
3.3.3. Univariate Association of Toxic Metals and Essential Elements with CVD
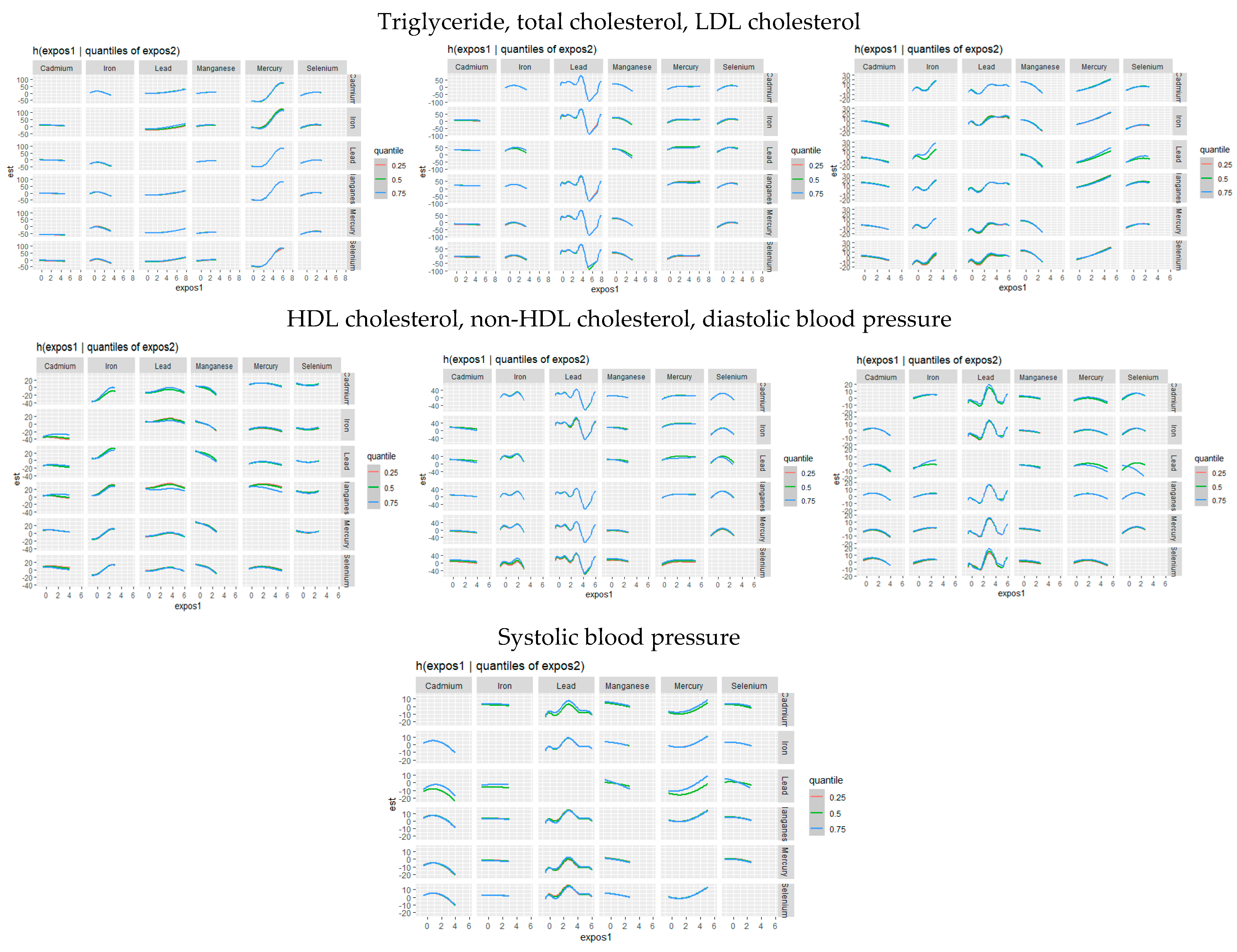
3.3.4. Bivariate Exposure–Response Function of Toxic Metals and Essential Elements with CVD
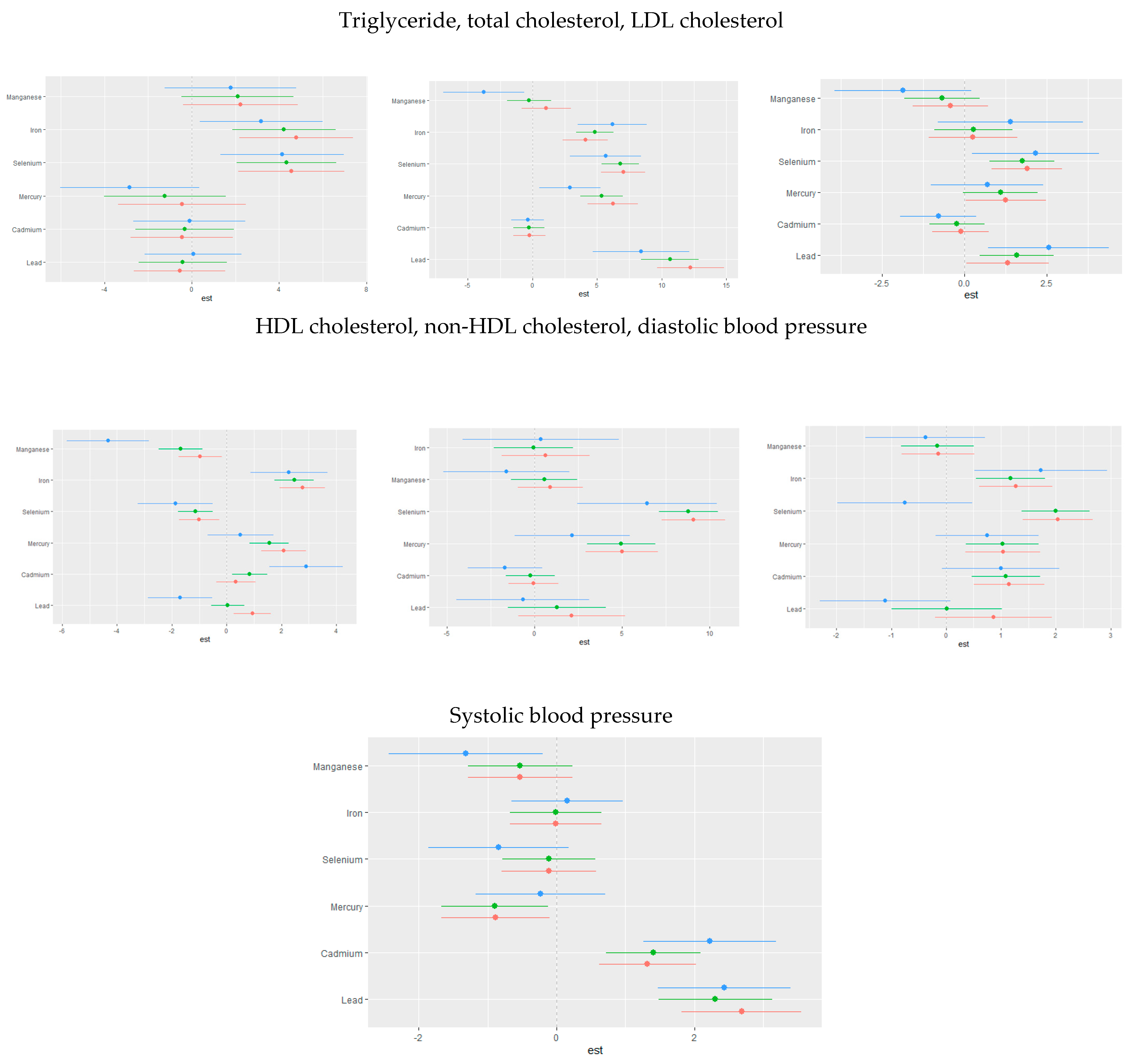
3.3.5. Single-Variable Effects of Toxic Metals and Essential Elements on Cardiovascular-Related Markers
3.3.6. Single-Variable Interaction Terms of Toxic Metals and Essential Elements on Individual CVD-Related Markers
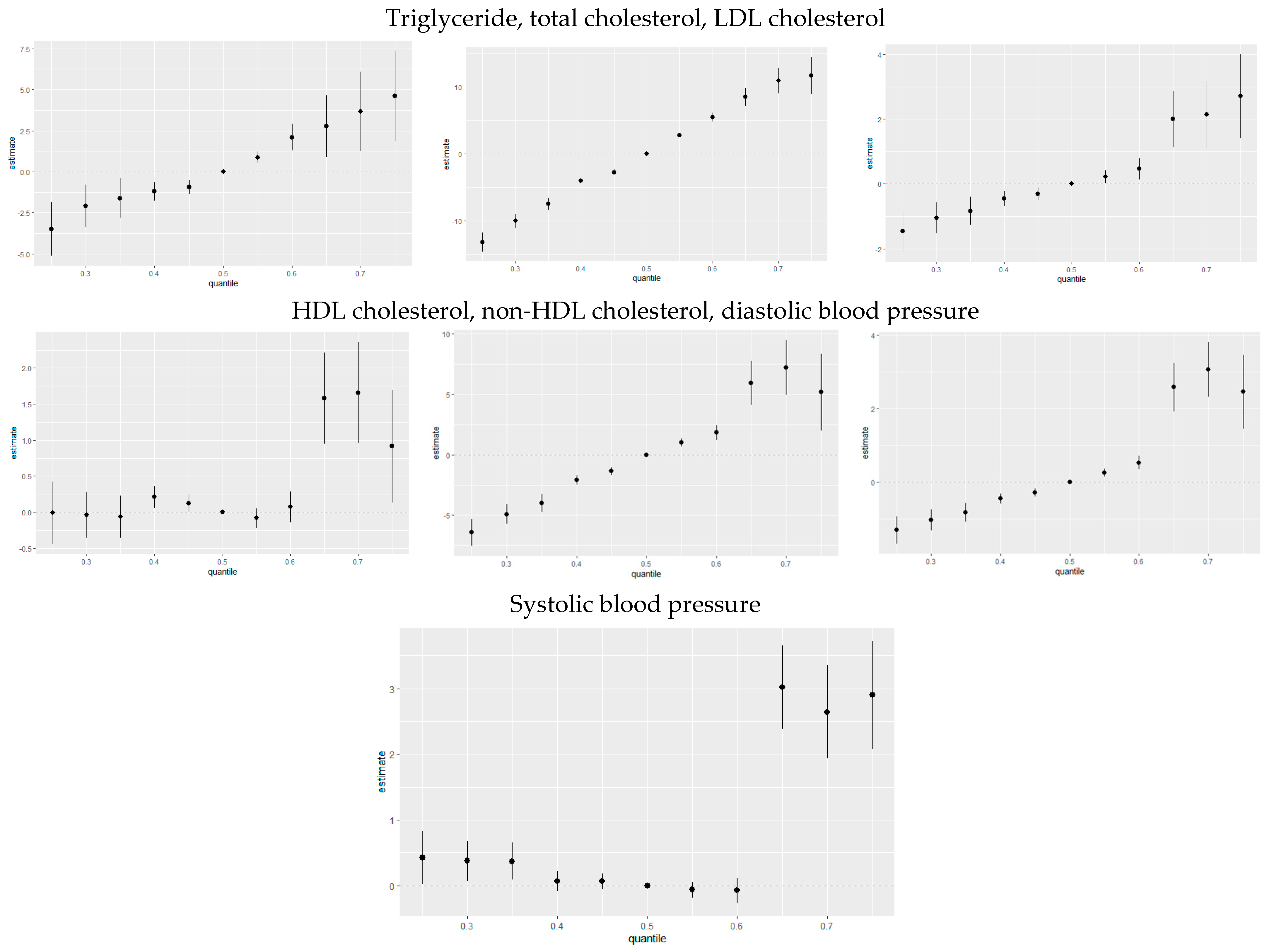
3.3.7. Overall Risk Summary of CVD Levels in Relation to Exposure Percentiles
3.4. Quantile G-Computation
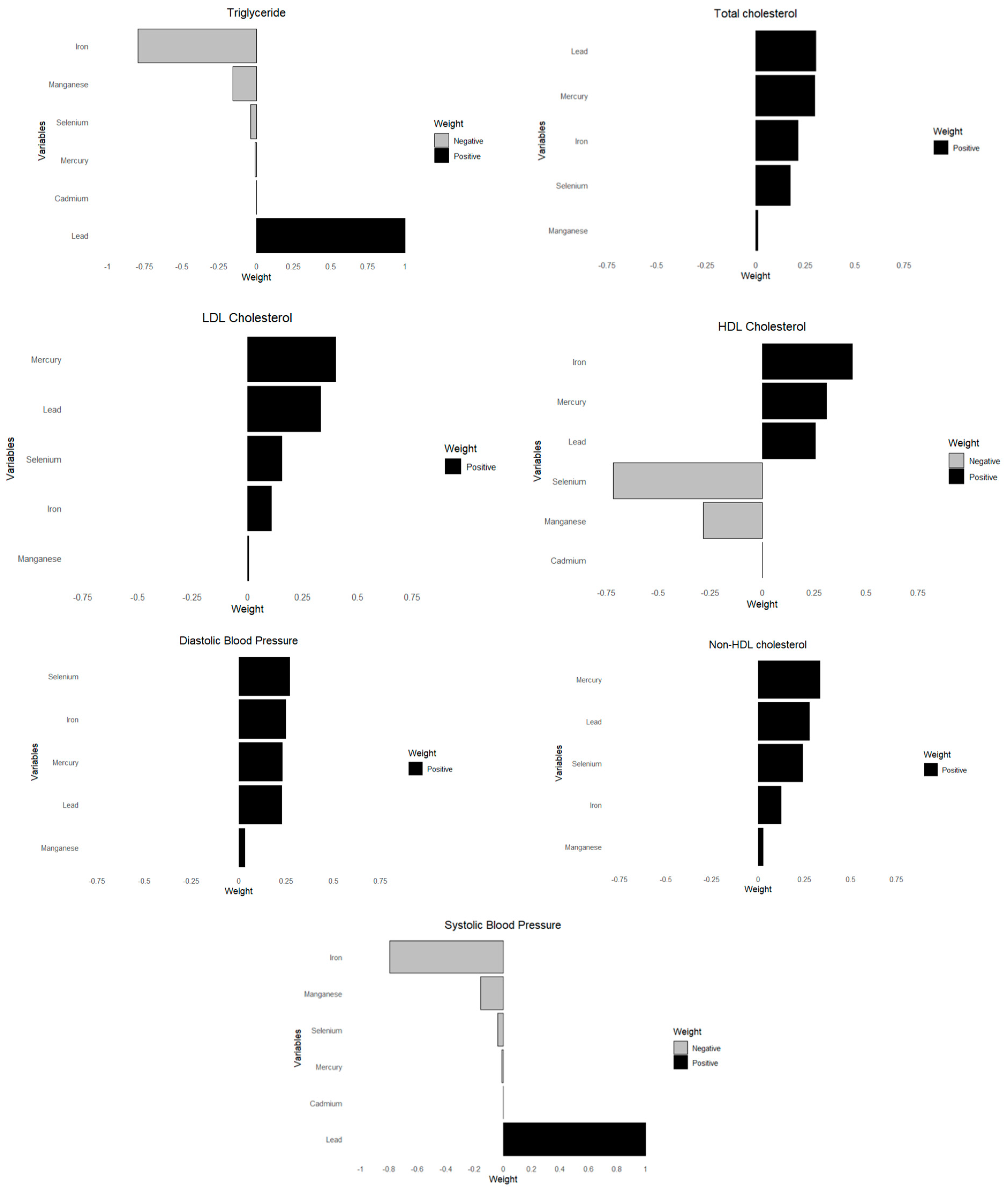
3.5. Weighted Quantile Sum Regression (WQSR)
4. Discussion
4.1. Correlation Analysis
4.2. Bayesian Kernel Machine Regression (BKMR) Analysis
4.3. Univariate and Bivariate Analysis
4.4. Single-Variable Effects at Increasing Quantiles
4.5. Quantile g-Computation and Weighted Quantile Sum Regression (WQSR) Analysis
4.6. Public Health Implications
4.7. Strengths and Limitations
4.8. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Cardiovascular Diseases (CVDs). Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 22 April 2025).
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart Disease and Stroke Statistics—2019 Update: A Report from the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [PubMed]
- World Health Organization. Cardiovascular Diseases. Available online: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1 (accessed on 22 April 2025).
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Mensah, G.A.; Roth, G.A.; Fuster, V. The Global Burden of Cardiovascular Diseases and Risk Factors: 2020 and Beyond. J. Am. Coll. Cardiol. 2019, 74, 2529–2532. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar]
- Centers for Disease Control and Prevention. Stroke Facts. Available online: https://www.cdc.gov/stroke/data-research/facts-stats/?CDC_AAref_Val=https://www.cdc.gov/stroke/facts.htm (accessed on 22 April 2025).
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef] [PubMed]
- Kjeldsen, E.W.; Thomassen, J.Q.; Rasmussen, K.L.; Nordestgaard, B.G.; Tybjærg-Hansen, A.; Frikke-Schmidt, R. Impact of Diet on Ten-Year Absolute Cardiovascular Risk in a Prospective Cohort of 94 321 Individuals: A Tool for Implementation of Healthy Diets. Lancet Reg. Health Eur. 2022, 19, 100419. [Google Scholar] [CrossRef]
- Wahid, A.; Manek, N.; Nichols, M.; Kelly, P.; Foster, C.; Webster, P.; Kaur, A.; Friedemann Smith, C.; Wilkins, E.; Rayner, M.; et al. Quantifying the Association between Physical Activity and Cardiovascular Disease and Diabetes: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2016, 5, e002495. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; Milani, R.V.; Ventura, H.O. Obesity and Cardiovascular Disease: Risk Factor, Paradox, and Impact of Weight Loss. J. Am. Coll. Cardiol. 2009, 53, 1925–1932. [Google Scholar] [CrossRef]
- Lu, Y.; Hajifathalian, K.; Ezzati, M.; Woodward, M.; Rimm, E.B.; Danaei, G. Metabolic Mediators of the Effects of Body-Mass Index, Overweight, and Obesity on Coronary Heart Disease and Stroke: A Pooled Analysis of 97 Prospective Cohorts with 1.8 Million Participants. Lancet 2014, 383, 970–983. [Google Scholar]
- Solenkova, N.V.; Newman, J.D.; Berger, J.S.; Thurston, G.; Hochman, J.S.; Lamas, G.A. Metal Pollutants and Cardiovascular Disease: Mechanisms and Consequences of Exposure. Am. Heart J. 2014, 168, 812–822. [Google Scholar] [CrossRef]
- Commodore-Mensah, Y.; Matthie, N.; Wells, J.; Dunbar, S.B.; Himmelfarb, C.D.; Cooper, L.A.; Chandler, R.D. African Americans, African Immigrants, and Afro-Caribbeans Differ in Social Determinants of Hypertension and Diabetes: Evidence from the National Health Interview Survey. J. Racial Ethn. Health Disparities 2018, 5, 995–1002. [Google Scholar] [CrossRef]
- Tchounwou, P.B.; Yedjou, C.G.; Patlolla, A.K.; Sutton, D.J. Heavy Metal Toxicity and the Environment. In Molecular, Clinical and Environmental Toxicology; Luch, A., Ed.; Springer: Berlin/Heidelberg, Germany, 2012; Volume 3. [Google Scholar]
- Jomova, K.; Valko, M. Advances in Metal-Induced Oxidative Stress and Human Disease. Toxicology 2011, 283, 65–87. [Google Scholar] [CrossRef] [PubMed]
- Harari, F.; Barregard, L.; Östling, G.; Sallsten, G.; Hedblad, B.; Forsgard, N.; Borné, Y.; Fagerberg, B.; Engström, G. Blood Lead Levels and Risk of Atherosclerosis in the Carotid Artery: Results from a Swedish Cohort. Environ. Health Perspect. 2019, 127, 127002. [Google Scholar] [CrossRef]
- Ma, S.; Zhang, J.; Xu, C.; Da, M.; Xu, Y.; Chen, Y.; Mo, X. Increased Serum Levels of Cadmium Are Associated with an Elevated Risk of Cardiovascular Disease in Adults. Environ. Sci. Pollut. Res. 2022, 29, 1836–1844. [Google Scholar] [CrossRef] [PubMed]
- Prashanth, L.; Kattapagari, K.K.; Chitturi, R.T.; Baddam, V.R.R.; Prasad, L.K. A Review on Role of Essential Trace Elements in Health and Disease. J. Dr. NTR Univ. Health Sci. 2015, 4, 75–85. [Google Scholar]
- Henein, M.Y.; Vancheri, S.; Longo, G.; Vancheri, F. The Role of Inflammation in Cardiovascular Disease. Int. J. Mol. Sci. 2022, 23, 12906. [Google Scholar] [CrossRef]
- Soetan, K.O.; Olaiya, C.O.; Oyewole, O.E. The Importance of Mineral Elements for Humans, Domestic Animals and Plants: A Review. Afr. J. Food Sci. 2010, 4, 200–222. [Google Scholar]
- Shaito, A.; Aramouni, K.; Assaf, R.; Parenti, A.; Orekhov, A.; El Yazbi, A.; Pintus, G.; Eid, A.H. Oxidative Stress-Induced Endothelial Dysfunction in Cardiovascular Diseases. Front. Biosci. 2022, 27, 105. [Google Scholar] [CrossRef]
- You, B.; Chen, Z. Association of Blood Manganese and Selenium Levels with Hepatic Steatosis among Adolescents: A Nationwide Cross-Sectional Analysis. Front. Public Health 2025, 13, 1522219. [Google Scholar] [CrossRef]
- Meng, H.; Wang, Y.; Ruan, J.; Chen, Y.; Wang, X.; Zhou, F.; Meng, F. Decreased Iron Ion Concentrations in the Peripheral Blood Correlate with Coronary Atherosclerosis. Nutrients 2022, 14, 319. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Laboratory Procedure Manual. Available online: https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/labmethods.aspx?BeginYear=2017 (accessed on 22 April 2025).
- Centers for Disease Control and Prevention. Procedure Manuals. Available online: https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/manuals.aspx?BeginYear=2017 (accessed on 22 April 2025).
- Deaton, C.; Froelicher, E.S.; Wu, L.H.; Ho, C.; Shishani, K.; Jaarsma, T. The Global Burden of Cardiovascular Disease. Eur. J. Cardiovasc. Nurs. 2011, 10 (Suppl. 2), S5–S13. [Google Scholar] [CrossRef] [PubMed]
- Labarthe, D.R.; Dunbar, S.B. Global Cardiovascular Health Promotion and Disease Prevention: 2011 and Beyond. Circulation 2012, 125, 2667–2676. [Google Scholar] [CrossRef]
- Raviglione, M.C.; Snider, D.E.; Kochi, A. Global Health Essentials; Springer: Cham, Switzerland, 2023. [Google Scholar]
- Bobb, J.F.; Valeri, L.; Claus Henn, B.; Christiani, D.C.; Wright, R.O.; Mazumdar, M.; Godleski, J.J.; Coull, B.A. Bayesian Kernel Machine Regression for Estimating the Health Effects of Multi-Pollutant Mixtures. Biostatistics 2015, 16, 493–508. [Google Scholar] [CrossRef]
- Bobb, J.F.; Claus Henn, B.; Valeri, L.; Coull, B.A. Statistical Software for Analyzing the Health Effects of Multiple Concurrent Exposures via Bayesian Kernel Machine Regression. Environ. Health 2018, 17, 67. [Google Scholar] [CrossRef] [PubMed]
- Boafo, Y.S.; Mostafa, S.; Obeng-Gyasi, E. Association of Combined Metals and PFAS with Cardiovascular Disease Risk. Toxics 2023, 11, 979. [Google Scholar] [CrossRef]
- Keil, A.P.; Buckley, J.P.; O’Brien, K.M.; Ferguson, K.K.; Zhao, S.; White, A.J. A Quantile-Based g-Computation Approach to Addressing the Effects of Exposure Mixtures. Environ. Health Perspect. 2020, 128, 047004. [Google Scholar] [CrossRef]
- Adetunji, A.G.; Obeng-Gyasi, E. Investigating the Interplay of Toxic Metals and Essential Elements in Liver Disease. Int. J. Environ. Res. Public Health 2024, 21, 762. [Google Scholar] [CrossRef] [PubMed]
- Webster, T. Analyzing Patterns of Co-Exposure in Exposure Space. In Proceedings of the International Society for Exposure Science 2016 Annual Meeting, Utrecht, The Netherlands, 9–13 October 2016. [Google Scholar]
- Ademuyiwa, O.; Ugbaja, R.N.; Idumebor, F.; Adebawo, O. Plasma Lipid Profiles and Risk of Cardiovascular Disease in Occupational Lead Exposure in Abeokuta, Nigeria. Lipids Health Dis. 2005, 4, 19. [Google Scholar] [CrossRef]
- Obeng-Gyasi, E.; Ford, Y.R. Combined Effects of Environmental Metals and Physiological Stress on Lipid Dysregulation. Med. Sci. 2024, 12, 51. [Google Scholar] [CrossRef]
- Obeng-Gyasi, E. Lead Exposure and Cardiovascular Disease among Young and Middle-Aged Adults. Med. Sci. 2019, 7, 103. [Google Scholar] [CrossRef]
- Bleys, J.; Navas-Acien, A.; Guallar, E. Serum Selenium and Serum Lipids in US Adults. Am. J. Clin. Nutr. 2008, 88, 416–423. [Google Scholar] [CrossRef]
- Chen, C.; Jin, Y.; Unverzagt, F.W.; Cheng, Y.; Hake, A.M.; Liang, C.; Ma, F.; Su, L.; Liu, J.; Bian, J.; et al. The Association between Selenium and Lipid Levels: A Longitudinal Study in Rural Elderly Chinese. Arch. Gerontol. Geriatr. 2015, 60, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Vaziri, N.D. Mechanisms of Lead-Induced Hypertension and Cardiovascular Disease. Am. J. Physiol. Heart Circ. Physiol. 2008, 295, H454–H465. [Google Scholar] [CrossRef]
- Xu, W.; Park, S.K.; Gruninger, S.E.; Charles, S.; Franzblau, A.; Basu, N.; Goodrich, J.M. Associations between Mercury Exposure with Blood Pressure and Lipid Levels: A Cross-Sectional Study of Dental Professionals. Environ. Res. 2023, 220, 115229. [Google Scholar] [CrossRef] [PubMed]
- Buhari, O.; Dayyab, F.M.; Igbinoba, O.; Atanda, A.; Medhane, F.; Faillace, R.T. The Association between Heavy Metal and Serum Cholesterol Levels in the US Population: National Health and Nutrition Examination Survey 2009–2012. Hum. Exp. Toxicol. 2020, 39, 355–364. [Google Scholar] [CrossRef]
- Luo, X.; Liu, Z.; Ge, X.; Huang, S.; Zhou, Y.; Li, D.; Li, L.; Chen, X.; Huang, L.; Hou, Q.; et al. High Manganese Exposure Decreased the Risk of High Triglycerides in Workers: A Cross-Sectional Study. BMC Public Health 2020, 20, 874. [Google Scholar] [CrossRef]
- Kim, K.; Park, H. Co-exposure to Heavy Metals and Hypertension among Adults in South Korea. Expo. Health 2022, 14, 139–147. [Google Scholar] [CrossRef]
- Cebi, A.; Kaya, Y.; Gungor, H.; Demir, H.; Yoruk, I.H.; Soylemez, N.; Gunes, Y.; Tuncer, M. Trace Elements, Heavy Metals and Vitamin Levels in Patients with Coronary Artery Disease. Int. J. Med. Sci. 2011, 8, 456–460. [Google Scholar] [CrossRef]
- Yang, A.M.; Lo, K.; Zheng, T.Z.; Yang, J.L.; Bai, Y.N.; Feng, Y.Q.; Cheng, N.; Liu, S.M. Environmental Heavy Metals and Cardiovascular Diseases: Status and Future Direction. Chronic Dis. Transl. Med. 2020, 6, 251–259. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (a) | |||||||||
| Variable | Mean (SD) | Minimum | Maximum | ||||||
| Toxic metals | |||||||||
| Lead | 1.06 (1.35) | 0.00 | 42.00 | ||||||
| Cadmium | 0.25 (0.59) | 0.00 | 13.00 | ||||||
| Mercury | 1.07 (2.33) | 0.00 | 64.00 | ||||||
| Essential elements | |||||||||
| Selenium | 186.30 (26.34) | 85.00 | 454.00 | ||||||
| Manganese | 10.32 (3.77) | 2.00 | 52.00 | ||||||
| Iron | 87.28 (36.62) | 10.00 | 476.00 | ||||||
| CVD Biomarkers | |||||||||
| Triglyceride | 107.34 (98.26) | 10.00 | 2684.00 | ||||||
| Total Cholesterol | 179.89 (40.60) | 76.00 | 446.00 | ||||||
| LDL Cholesterol | 108.50 (36.33) | 20.00 | 359.00 | ||||||
| HDL Cholesterol | 53.39 (14.75) | 10.00 | 189.00 | ||||||
| Non-HDL Cholesterol | 126.50 (40.57) | 22.00 | 408 | ||||||
| Diastolic Blood Pressure | 67.79 (15.55) | 0.00 | 135.00 | ||||||
| Systolic Blood Pressure | 120.83 (19.55) | 73.00 | 225.00 | ||||||
| (b) Demographic characteristics, body mass index (BMI), and alcohol use in the study population | |||||||||
| Variables | Description | Frequency | Mean | Percentage | 95% Confidence Interval | ||||
| Gender | 9254 | ||||||||
| Male | 4557 | 37.43 | 49.24 | 36.38 | 38.48 | ||||
| Female | 4697 | 39.38 | 50.76 | 38.12 | 40.64 | ||||
| Ethnicity | 9254 | ||||||||
| Mexican American | 1367 | 14.77 | 27.50 | 31.13 | |||||
| Other Hispanic | 820 | 8.86 | 31.77, | 35.60 | |||||
| Non-Hispanic White | 3150 | 34.04 | 40.00, | 43.34 | |||||
| Non-Hispanic Black | 2115 | 22.85 | 34.68 | 36.98 | |||||
| Non-Hispanic Asian | 1168 | 12.62 | 35.93 | 39.93 | |||||
| Other Races—Including Multi-Racial | 634 | 6.85 | 29.59 | 37.36 | |||||
| BMI | Male | 8878 | 27.45 | 26.91 | 28.00 | ||||
| Female | 8931 | 27.45 | 27.21 | 28.55 | |||||
| Alcohol Use | 5130 | ||||||||
| Yes | 4545 | 88.60 | |||||||
| No | 585 | 11.49 | |||||||
| Triglyceride | Total Cholesterol | LDL Cholesterol | HDL Cholesterol | Non-HDL Cholesterol | Diastolic Blood Pressure | Systolic Blood Pressure | |
|---|---|---|---|---|---|---|---|
| Lead | 0.3022 | 1.0000 | 0.9564 | 1.0000 | 1.0000 | 1.0000 | 1.0000 |
| Cadmium | 0.3106 | 0.0000 | 0.5020 | 1.0000 | 0.2528 | 0.9612 | 0.9496 |
| Mercury | 0.9782 | 1.0000 | 0.9296 | 0.9892 | 1.0000 | 0.4828 | 0.3608 |
| Selenium | 0.9838 | 1.0000 | 1.0000 | 0.9992 | 1.0000 | 1.0000 | 0.2688 |
| Manganese | 0.3314 | 0.2524 | 0.6556 | 1.0000 | 0.2912 | 0.2192 | 0.3692 |
| Iron | 0.9636 | 1.0000 | 0.8028 | 1.0000 | 1.0000 | 0.9900 | 0.0148 |
| Group | Group PIP | Cond PIP | |
|---|---|---|---|
| Lead | 1 | 0.8900 | 0.0418 |
| Cadmium | 1 | 0.8900 | 0.0674 |
| Mercury | 1 | 0.8900 | 0.8908 |
| Selenium | 2 | 0.9852 | 0.7353 |
| Manganese | 2 | 0.9852 | 0.0057 |
| Iron | 2 | 0.9852 | 0.2590 |
| Group | Group PIP | Cond PIP | |
|---|---|---|---|
| Lead | 1 | 1.0000 | 1.0000 |
| Cadmium | 1 | 1.0000 | 0.0000 |
| Mercury | 1 | 1.0000 | 0.0000 |
| Selenium | 2 | 1.0000 | 1.0000 |
| Manganese | 2 | 1.0000 | 0.0000 |
| Iron | 2 | 1.0000 | 0.0000 |
| Group | Group PIP | Cond PIP | |
|---|---|---|---|
| Lead | 1 | 1.0000 | 0.9556 |
| Cadmium | 1 | 1.0000 | 0.0000 |
| Mercury | 1 | 1.0000 | 0.0444 |
| Selenium | 2 | 1.0000 | 0.8156 |
| Manganese | 2 | 1.0000 | 0.0000 |
| Iron | 2 | 1.0000 | 0.1844 |
| Group | Group PIP | Cond PIP | |
|---|---|---|---|
| Lead | 1 | 1.0000 | 1.0000 |
| Cadmium | 1 | 1.0000 | 0.0000 |
| Mercury | 1 | 1.0000 | 0.0000 |
| Selenium | 2 | 1.0000 | 0.0000 |
| Manganese | 2 | 1.0000 | 0.0000 |
| Iron | 2 | 1.0000 | 1.0000 |
| Group | Group PIP | Cond PIP | |
|---|---|---|---|
| Lead | 1 | 1.0000 | 1.0000 |
| Cadmium | 1 | 1.0000 | 0.0000 |
| Mercury | 1 | 1.0000 | 0.0000 |
| Selenium | 2 | 1.0000 | 1.0000 |
| Manganese | 2 | 1.0000 | 0.0000 |
| Iron | 2 | 1.0000 | 0.0000 |
| Group | Group PIP | Cond PIP | |
|---|---|---|---|
| Lead | 1 | 1.0000 | 1.0000 |
| Cadmium | 1 | 1.0000 | 0.0000 |
| Mercury | 1 | 1.0000 | 0.0000 |
| Selenium | 2 | 1.0000 | 1.0000 |
| Manganese | 2 | 1.0000 | 0.0000 |
| Iron | 2 | 1.0000 | 0.0000 |
| Group | Group PIP | Cond PIP | |
|---|---|---|---|
| Lead | 1 | 1.0000 | 1.0000 |
| Cadmium | 1 | 1.0000 | 0.0000 |
| Mercury | 1 | 1.0000 | 0.0000 |
| Selenium | 2 | 1.0000 | 0.3208 |
| Manganese | 2 | 1.0000 | 0.4025 |
| Iron | 2 | 1.0000 | 0.2767 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adetunji, A.G.; Obeng-Gyasi, E. Investigating the Interplay of Toxic Metals and Essential Elements in Cardiovascular Disease. J. Xenobiot. 2025, 15, 68. https://doi.org/10.3390/jox15030068
Adetunji AG, Obeng-Gyasi E. Investigating the Interplay of Toxic Metals and Essential Elements in Cardiovascular Disease. Journal of Xenobiotics. 2025; 15(3):68. https://doi.org/10.3390/jox15030068
Chicago/Turabian StyleAdetunji, Aderonke Gbemi, and Emmanuel Obeng-Gyasi. 2025. "Investigating the Interplay of Toxic Metals and Essential Elements in Cardiovascular Disease" Journal of Xenobiotics 15, no. 3: 68. https://doi.org/10.3390/jox15030068
APA StyleAdetunji, A. G., & Obeng-Gyasi, E. (2025). Investigating the Interplay of Toxic Metals and Essential Elements in Cardiovascular Disease. Journal of Xenobiotics, 15(3), 68. https://doi.org/10.3390/jox15030068