
Safety and Efficacy of Tyrosine Kinase Inhibitors in Immune Thrombocytopenic Purpura: A Systematic Review of Clinical Trials


 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
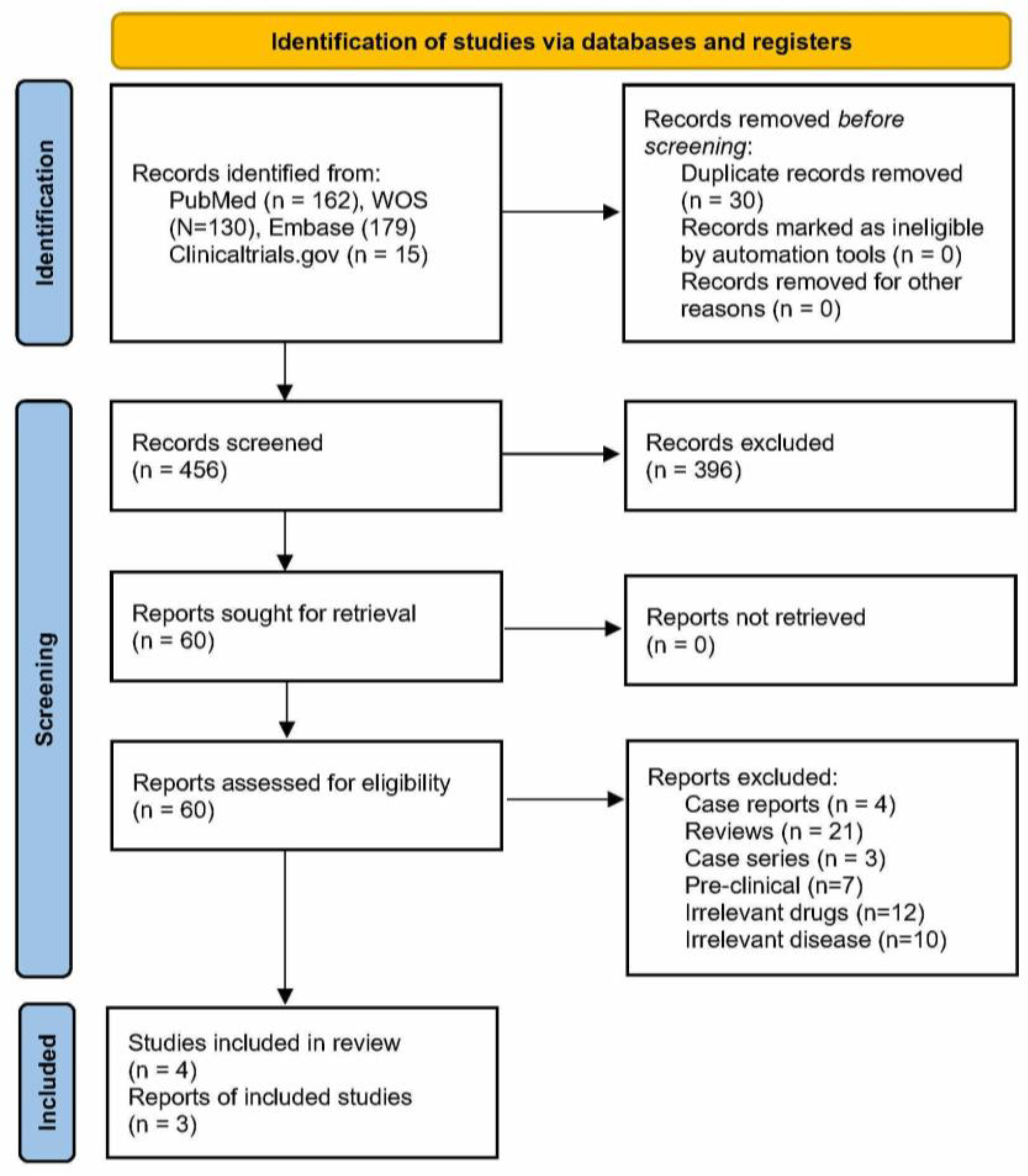
2.1. Search Strategy
2.2. Inclusion and Exclusion of Articles
2.3. Study Selection
2.4. Data Extraction
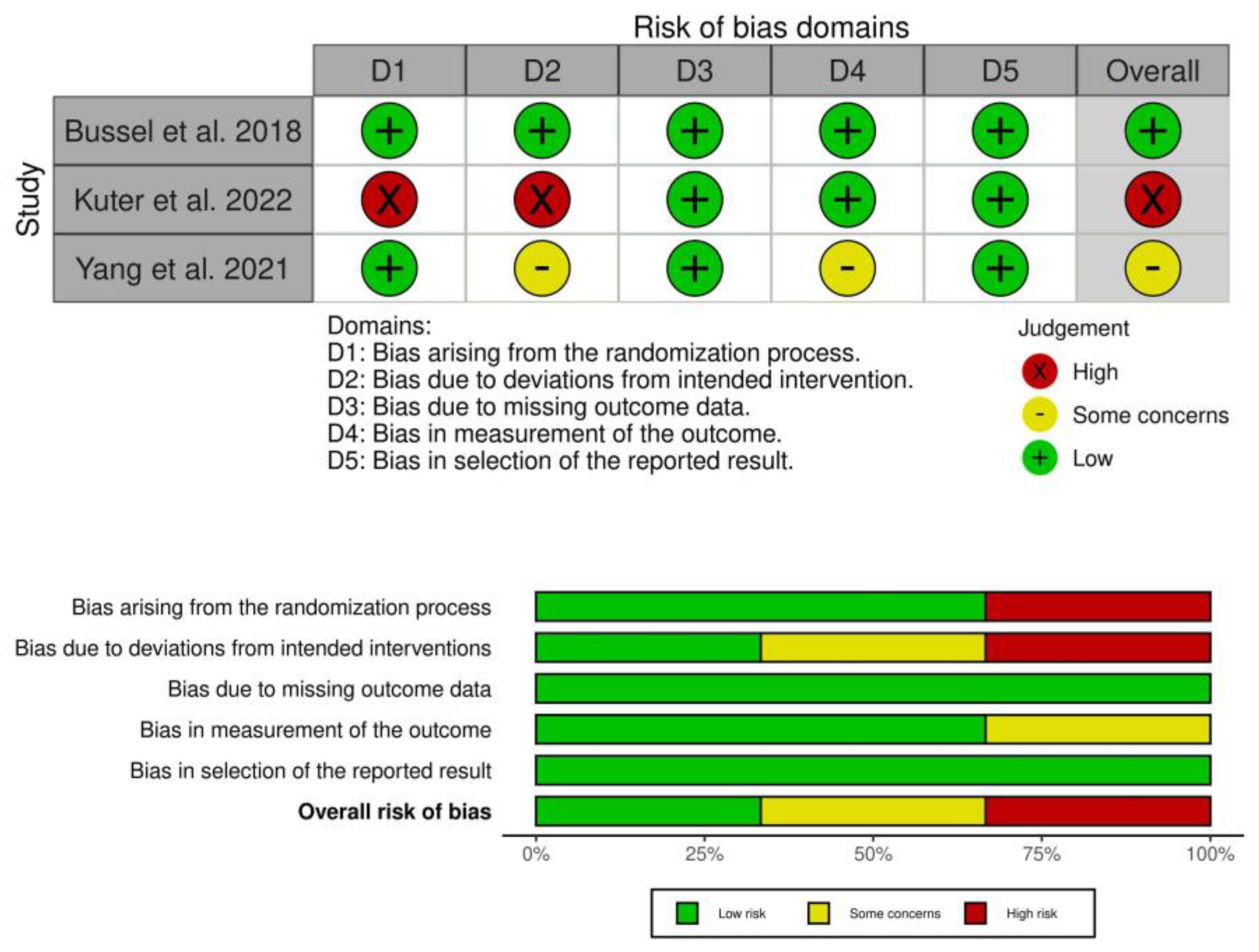
2.5. Risk of Bias (ROB) Assessment
3. Results
3.1. Risk of Bias
3.2. Efficacy and Safety of TKI
3.2.1. Efficacy of Fostamatinib and HMPL-523 (Syk)
3.2.2. Efficacy of Bruton’s TKI (Rilzabrutinib)
3.2.3. Safety
3.3. Ongoing Clinical Trials
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cooper, N.; Ghanima, W. Immune Thrombocytopenia. N. Engl. J. Med. 2019, 381, 945–955. [Google Scholar] [CrossRef] [PubMed]
- Semple, J.W.; Provan, D.; Garvey, M.B.; Freedman, J. Recent progress in understanding the pathogenesis of immune thrombocytopenia. Curr. Opin. Hematol. 2010, 17, 590–595. [Google Scholar] [CrossRef] [PubMed]
- Fogarty, P.F.; Segal, J.B. The epidemiology of immune thrombocytopenic purpura. Curr. Opin. Hematol. 2007, 14, 515–519. [Google Scholar] [CrossRef] [PubMed]
- Arnold, D.M. Bleeding complications in immune thrombocytopenia. Hematology 2015, 2015, 237–242. [Google Scholar] [CrossRef]
- Kohli, R.; Chaturvedi, S. Epidemiology and Clinical Manifestations of Immune Thrombocytopenia. Hamostaseologie 2019, 39, 238–249. [Google Scholar] [CrossRef]
- Cines, D.B.; Bussel, J.B.; Liebman, H.A.; Prak, E.T.L. The ITP syndrome: Pathogenic and clinical diversity. Blood 2009, 113, 6511–6521. [Google Scholar] [CrossRef]
- Singh, A.; Uzun, G.; Bakchoul, T. Primary Immune Thrombocytopenia: Novel Insights into Pathophysiology and Disease Management. J. Clin. Med. 2021, 10, 789. [Google Scholar] [CrossRef]
- Zufferey, A.; Kapur, R.; Semple, J.W. Pathogenesis and Therapeutic Mechanisms in Immune Thrombocytopenia (ITP). J. Clin. Med. 2017, 6, 16. [Google Scholar] [CrossRef]
- Neunert, C.E. Management of newly diagnosed immune thrombocytopenia: Can we change outcomes? Blood Adv. 2017, 1, 2295–2301. [Google Scholar] [CrossRef]
- Ghanima, W.; Khelif, A.; Waage, A.; Michel, M.; E Tjønnfjord, G.; Ben Romdhan, N.; Kahrs, J.; Darne, B.; Holme, P.A. Rituximab as second-line treatment for adult immune thrombocytopenia (the RITP trial): A multicentre, randomised, double-blind, placebo-controlled trial. Lancet 2015, 385, 1653–1661. [Google Scholar] [CrossRef]
- Kojouri, K.; Vesely, S.; Terrell, D.; George, J.N. Splenectomy for adult patients with idiopathic thrombocytopenic purpura: A systematic review to assess long-term platelet count responses, prediction of response, and surgical complications. Blood 2004, 104, 2623–2634. [Google Scholar] [CrossRef] [PubMed]
- Waleed, G.; Cooper, N.; Rodeghiero, F.; Godeau, B.; Bussel, J. Thrombopoietin receptor agonists: Ten years later. Haematologica 2019, 104, 1112–1123. [Google Scholar]
- Chandler, J.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2019. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inf. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Bussel, J.; Arnold, D.M.; Grossbard, E.; Mayer, J.; Treliński, J.; Homenda, W.; Hellmann, A.; Windyga, J.; Sivcheva, L.; Khalafallah, A.; et al. Fostamatinib for the treatment of adult persistent and chronic immune thrombocytopenia: Results of two phase 3, randomized, placebo-controlled trials. Am. J. Hematol. 2018, 93, 921–930. [Google Scholar] [CrossRef]
- Yang, R.; Zhou, H.; Hu, Y.; Yin, J.; Li, J.; Chen, W.; Huang, R.; Gong, Y.; Luo, C.; Xiaofan, L.; et al. Safety, pharmacokinetics and preliminary efficacy of HMPL-523 in adult patients with primary immune thrombocytopenia: A randomized, double-blind and placebo-controlled phase 1b study. Blood 2021, 138 (Suppl. 1), 16. [Google Scholar] [CrossRef]
- Kuter, D.J.; Efraim, M.; Mayer, J.; Trněný, M.; McDonald, V.; Bird, R.; Regenbogen, T.; Garg, M.; Kaplan, Z.; Tzvetkov, N.; et al. Rilzabrutinib, an Oral BTK Inhibitor, in Immune Thrombocytopenia. N. Engl. J. Med. 2022, 386, 1421–1431. [Google Scholar] [CrossRef]
- Braselmann, S.; Taylor, V.; Zhao, H.; Wang, S.; Sylvain, C.; Baluom, M.; Qu, K.; Herlaar, E.; Lau, A.; Young, C.; et al. R406, an orally available spleen tyrosine kinase inhibitor blocks fc receptor signaling and reduces immune complex-mediated inflammation. J. Pharmacol. Exp. Ther. 2006, 319, 998–1008. [Google Scholar] [CrossRef]
- Newland, A.; Lee, E.-J.; McDonald, V.; Bussel, J.B. Fostamatinib for persistent/chronic adult immune thrombocytopenia. Immunotherapy 2018, 10, 9–25. [Google Scholar] [CrossRef]
- Park, S.R.; Speranza, G.; Piekarz, R.; Wright, J.J.; Kinders, R.J.; Wang, L.; Pfister, T.D.; Trepel, J.B.; Lee, M.-J.; Alarcon, S.; et al. A multi-histology trial of fostamatinib in patients with advanced colorectal, non-small cell lung, head and neck, thyroid, and renal cell carcinomas, and pheochromocytomas. Cancer Chemother. Pharmacol. 2013, 71, 981–990. [Google Scholar] [CrossRef] [PubMed]
- Cooper, N.; Altomare, I.; Thomas, M.R.; Nicolson, P.L.R.; Watson, S.P.; Markovtsov, V.; Todd, L.K.; Masuda, E.; Bussel, J.B. Assessment of thrombotic risk during long-term treatment of immune thrombocytopenia with fostamatinib. Ther. Adv. Hematol. 2021, 12, 20406207211010875. [Google Scholar] [CrossRef]
- Moezi, M.M.; Peevyhouse, A.; Wood, T.; Kreychman, Y.; Dranitsaris, G. The Safety and Efficacy of Fostamatinib in Patients with Chronic Immune Thrombocytopenic Purpura Treated in a Real-World Community Hematology Setting. Blood 2022, 140 (Suppl. 1), 5135–5136. [Google Scholar] [CrossRef]
- Connell, N.T.; Berliner, N. Fostamatinib for the treatment of chronic immune thrombocytopenia. Blood 2019, 133, 2027–2030. [Google Scholar] [CrossRef]
- Lickliter, J.; Wu, Y.; Hua, Y.; Yuan, I.; Dai, G.; Li, X.; Wang, J.; Sai, Y.; Sun, Z.; Pan, A.; et al. A phase I, randomized, double blind, placebo-controlled, dose escalating study of the safety, tolerability and pharmacokinetics and pharmacodynamics of single and multiple doses of HMPL-523 in australian male healthy subjects. Arthritis Rheumatol. 2016, 68, 2018–2020. [Google Scholar]
- Mingot-Castellano, M.E.; Bastida, J.M.; Caballero-Navarro, G.; Ureña, L.E.; González-López, T.J.; González-Porras, J.R.; Butta, N.; Canaro, M.; Jiménez-Bárcenas, R.; Solano, M.d.C.G.d.C.; et al. Novel Therapies to Address Unmet Needs in ITP. Pharmaceuticals 2022, 15, 779. [Google Scholar] [CrossRef] [PubMed]
- Provan, D.; Newland, A.C. Investigational drugs for immune thrombocytopenia. Expert Opin. Investig. Drugs 2022, 31, 715–727. [Google Scholar] [CrossRef] [PubMed]
- Langrish, C.L.; Bradshaw, J.M.; Francesco, M.R.; Owens, T.D.; Xing, Y.; Shu, J.; LaStant, J.; Bisconte, A.; Outerbridge, C.; White, S.D.; et al. Preclinical Efficacy and Anti-Inflammatory Mechanisms of Action of the Bruton Tyrosine Kinase Inhibitor Rilzabrutinib for Immune-Mediated Disease. J. Immunol. 2021, 206, 1454–1468. [Google Scholar] [CrossRef] [PubMed]
- Shatzel, J.J.; Olson, S.R.; Tao, D.L.; McCarty, O.J.T.; Danilov, A.V.; DeLoughery, T.G. Ibrutinib-associated bleeding: Pathogenesis, management and risk reduction strategies. J. Thromb. Haemost. 2017, 15, 835–847. [Google Scholar] [CrossRef]
- Musumeci, F.; Greco, C.; Giacchello, I.; Fallacara, A.L.; Ibrahim, M.M.; Grossi, G.; Brullo, C.; Schenone, S. An Update on JAK Inhibitors. Curr. Med. Chem. 2019, 26, 1806–1832. [Google Scholar] [CrossRef]
- Li, M.; Ding, B.; Song, X.; Xia, A.; Han, Y.; Song, Y.; Wei, X.; Zhou, H. Refractory/relapse thrombocytopenia in a patient with Evans’ syndrome successfully treated with zanubrutinib. Br. J. Haematol. 2022, 199, e37–e42. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, S.; Arnold, D.M.; McCrae, K.R. Splenectomy for immune thrombocytopenia: Down but not out. Blood 2018, 131, 1172–1182. [Google Scholar] [CrossRef] [PubMed]
- Gudbrandsdottir, S.; Birgens, H.S.; Frederiksen, H.; Jensen, B.A.; Jensen, M.K.; Kjeldsen, L.; Klausen, T.W.; Larsen, H.; Mourits-Andersen, H.T.; Nielsen, C.H.; et al. Rituximab and dexamethasone vs dexamethasone monotherapy in newly diagnosed patients with primary immune thrombocytopenia. Blood 2013, 121, 1976–1981. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.L.; Mahévas, M.; Lee, S.; Stasi, R.; Cunningham-Rundles, S.; Godeau, B.; Kanter, J.; Neufeld, E.; Taube, T.; Ramenghi, U.; et al. Outcomes 5 years after response to rituximab therapy in children and adults with immune thrombocytopenia. Blood 2012, 119, 5989–5995. [Google Scholar] [CrossRef]
- Arnold, D.M.; Heddle, N.M.; Carruthers, J.; Cook, D.J.; Crowther, M.; Meyer, R.M.; Liu, Y.; Cook, R.J.; McLeod, A.; MacEachern, J.A.; et al. A pilot randomized trial of adjuvant rituximab or placebo for nonsplenectomized patients with immune thrombocytopenia. Blood 2012, 119, 1356–1362. [Google Scholar] [CrossRef] [PubMed]
- Laws, A.; Gomez-Ulloa, D.; Calvo, E.; Stacey, D.; Hamilton, J.; McDonald, V. Comparative Effectiveness of Fostamatinib Vs. Rituximab in Refractory Chronic Immune Thrombocytopenia: A Network Meta-Analysis. Blood 2022, 140 (Suppl. 1), 2687–2688. [Google Scholar] [CrossRef]
- Bonelli, M.M.; Mrak, D.; Perkmann, T.; Haslacher, H.; Aletaha, D. SARS-CoV-2 vaccination in rituximab-treated patients: Evidence for impaired humoral but inducible cellular immune response. Ann. Rheum. Dis. 2021, 80, 1355–1356. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Trial | NCT | Drug Therapy | Trial Phase | N | Median Age (Range) | ITP Classification n (%) | Prior Splenectomy n (%) | Most Common Prior Therapies | Mean Baseline Platelet Count (Range) |
|---|---|---|---|---|---|---|---|---|---|
| Bussel et al. 2018 [17] | NCT02076399 | Fostamatinib (100 mg BID) | Phase III randomized | 51 | 57 (20–88) | Persistent = 3 (6) Chronic = 48 (94) | 20 (39) | Corticosteroids 46 (90), IVIg, or IV Anti-D 33 (65); Thrombopoietic Agents 27 (53); Immunosuppressants 22 (43) | 16,202 (1000–51,000) |
| Placebo | 25 | 57 (26–77) | Persistent = 3 (12) Chronic = 22 (88) | 10 (40) | Corticosteroids 25 (100), IVIg, or IV Anti-D 17 (68); Thrombopoietic Agents 15 (60); Immunosuppressants 12 (48) | 15,844 (1000–48,000) | |||
| NCT02076412 | Fostamatinib (100 mg BID) | Phase III randomized | 50 | 50 (21–82) | Persistent = 3 (6) Chronic = 47 (94) | 14 (28) | Corticosteroids 48 (96), IVIg, or IV Anti-D 19 (38); Thrombopoietic Agents 20 (40); Immunosuppressants 22 (44) | 15,900 (1000–33,000) | |
| Placebo | 24 | 50 (20–78) | Persistent = 1 (4) Chronic = 23 (96) | 9 (38) | Corticosteroids 22 (92), IVIg, or IV Anti-D 10 (42); Thrombopoietic Agents 10 (42); Immunosuppressants 10 (42) | 23,958 (1000–156,000) | |||
| Kuter et al. 2022 [19] | NCT03395210 | Rilzabrutinib (200–400 mg) | Phase I-II Non-randomized | 60 | 50 (19–74) | Chronic = 52 (40) | 15 (25) | Corticosteroids 55 (92), IVIg 26 (43), Thrombopoietin Agent 35 (58) | 15,000 (2000–33,000) |
| 400 twice daily subgroup | 45 | 49 (19–74) | 11 (24) | Glucocorticoids 42 (93), IVIG 21 (47), Thrombopoietin Agent 24 (53) | 15,000 (2000–33,000) | ||||
| Yang et al. 2021 [18] | NCT03951623 | HMPL-523 (100 mg QD) | Phase I b randomized | 6 | 34.5 (20–58) | Concomitant = 1 (16.7) Non- concomitant = 5 (83.3) | NA | Prior therapy 6 (100) | 10,000 (1000–25,000) |
| 200 mg QD | 6 | 33 (18–65) | Concomitant = 1 (16.7) Non-concomitant = 5 (83.3) | Prior therapy 6 (100) | 4500 (3000–22,000) | ||||
| 300 mg QD | 16 | 40 (24–62) | Concomitant = 9 (56.3) Non-commitment = 7 (43.8) | Prior therapy 16 (100) | 7000 (1000–26,000) | ||||
| 400 mg QD | 6 | 43 (28–57) | Concomitant = 0 Non-concomitant= 6 (100) | Prior therapy 6 (100) | 8000 (2000–29,000) | ||||
| Placebo | 11 | 49 (21–65) | Concomitant = 5 (45.5) Non-concomitant = 6 (54.5) | Prior therapy 11 (100) | 19,000 (4000–32,100) |
| Trial | Drug Therapy | Stable Response * | Modified Stable Response ǂ | Overall Response € | Any Serious Adverse Effect | Serious Diarrhea | Serious Hypertension | Serious Dizziness | Serious Neutropenia | Serious Nausea | Serious Fatigue | Serious Abdominal Pain/Distension |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bussel et al. 2018 [17] | Fostamatinib (100 mg BID) | 9/51 (18%) | NA | 19 (37%) | 16% (9% dose limiting) | 1% | 2% | 1% | 1% | 0% | 0% | 0% |
| Placebo | 0/25 | NA | 2 (8%) | 15% (2% dose limiting) | 0 | 2% | 0 | 0 | 0% | 0% | 0% | |
| Fostamatinib (100 mg BID) | 9/50 (18%) | NA | 24 (48%) | 16% | 1% | 2% | 1% | 1% | 0% | 0% | 0% | |
| Placebo | 1/24 (4%) | NA | 5 (21%) | 15% | 0% | 2% | 0% | 0% | 0% | 0% | 0% | |
| Kuter et al. 2022 [19] | Rilzabrutinib (200–400 mg) | 17/60 (28%) | 24/60 (40%) | NA | 8 (0 = treatment related or dose limiting) | 0% | NA | NA | NA | 0% | 0% | 0% |
| Rilzabrutinib 400 twice daily subgroup | 14/45 (31%) | 18/45 (40%) | NA | 0 | 0% | NA | NA | NA | 0% | 0% | 0% | |
| Yang et al. 2021 [18] | HMPL-523 (100 mg QD) | NA | NA | 3/6 (50%) | No dose-limiting toxicity | 2 (5.9%) £ | NA | 2 (5.9%) £ | 3 (8.8%) £ | NA | NA | 2 (5.9%) £ |
| 200 mg QD | NA | NA | 2/6 (33%) | No dose-limiting toxicity | ||||||||
| 300 mg QD | 5/16 (31%) | NA | 11/16 (68.8%) | No dose-limiting toxicity | ||||||||
| 400 mg QD | NA | NA | 2/6 (33%) | No dose-limiting toxicity | ||||||||
| Placebo | 1/11 (9%) | NA | 1/11 (9%) | No dose-limiting toxicity | NA | NA | NA | NA | NA | NA | NA |
| NCT | Drug | Phase | N | Population | Outcomes | End Date |
|---|---|---|---|---|---|---|
| Bruton tyrosine kinase and Janus kinase inhibitors | ||||||
| NCT04562766 | Rilzabrutinib | Phase III RCT | 224 | Persistent and chronic ITP | Efficacy and safety | 2025 |
| NCT05446831 | Baricitinib | Phase II | 33 | Steroid relapsed/refractory ITP | Efficacy/safety | 2023 |
| NCT05124028 | Orelabrutinib | Phase I/II | 10 | Primary ITP | Efficacy and safety | 2022 |
| NCT05020288 | Orelabrutinib | Phase II | 40 | Refractory ITP | Efficacy and safety | 2024 |
| NCT05232149 | Orelabrutinib | Phase II | 30 | Refractory ITP | Efficacy and safety | 2024 |
| NCT05279872 | Zanubrutinib | Phase I/II | 10 | Primary ITP | Efficacy and safety | 2022 |
| NCT05369377 | Zanubrutinib + eltrombopag | Open label, RCT, phase II | 150 | Refractory ITP | Efficacy and safety | 2025 |
| NCT05369364 | Zanubrutinib + Dexamethasone | Open label, RCT, phase II | 150 | First line ITP | Efficacy and safety | 2025 |
| Spleen tyrosine kinase inhibitors | ||||||
| NCT04056195 | SKI-O-703 | Phase II, RCT | 60 | Refractory ITP | Efficacy and safety | 2022 |
| NCT05509582 | Fostamatinib | Phase II | 20 | Post-transplant ITP | Efficacy and safety | 2028 |
| ITP = immune thrombocytopenia | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, M.A.; Anwar, M.Y.; Aiman, W.; Dhanesar, G.; Omar, Z.; Hamza, M.; Zafar, M.; Rengarajan, H.K.; Maroules, M. Safety and Efficacy of Tyrosine Kinase Inhibitors in Immune Thrombocytopenic Purpura: A Systematic Review of Clinical Trials. J. Xenobiot. 2023, 13, 29-41. https://doi.org/10.3390/jox13010005
Ali MA, Anwar MY, Aiman W, Dhanesar G, Omar Z, Hamza M, Zafar M, Rengarajan HK, Maroules M. Safety and Efficacy of Tyrosine Kinase Inhibitors in Immune Thrombocytopenic Purpura: A Systematic Review of Clinical Trials. Journal of Xenobiotics. 2023; 13(1):29-41. https://doi.org/10.3390/jox13010005
Chicago/Turabian StyleAli, Muhammad Ashar, Muhammad Yasir Anwar, Wajeeha Aiman, Gurneel Dhanesar, Zainab Omar, Mohammad Hamza, Maha Zafar, Harish Kumar Rengarajan, and Michael Maroules. 2023. "Safety and Efficacy of Tyrosine Kinase Inhibitors in Immune Thrombocytopenic Purpura: A Systematic Review of Clinical Trials" Journal of Xenobiotics 13, no. 1: 29-41. https://doi.org/10.3390/jox13010005
APA StyleAli, M. A., Anwar, M. Y., Aiman, W., Dhanesar, G., Omar, Z., Hamza, M., Zafar, M., Rengarajan, H. K., & Maroules, M. (2023). Safety and Efficacy of Tyrosine Kinase Inhibitors in Immune Thrombocytopenic Purpura: A Systematic Review of Clinical Trials. Journal of Xenobiotics, 13(1), 29-41. https://doi.org/10.3390/jox13010005