
Management of Preoperative Anxiety via Virtual Reality Technology: A Systematic Review

 , , , , , and
, , , , , and
Abstract
1. Introduction
1.1. Effects of Stress on the Body Preoperatively and Postoperatively
1.2. Need for Stress Management
1.3. Technology of Virtual Reality
1.4. Distraction Therapy and Educational Use of VR
1.5. Aim
- To evaluate the effectiveness of VR interventions compared to standard care in reducing preoperative anxiety in adult surgical patients.
- To assess the impact of VR use on other perioperative outcomes, such as postoperative anxiety, patient satisfaction, medication use, and recovery time.
- To explore the feasibility and acceptability of VR among adult surgical patients, including ease of use, technical challenges, and patient satisfaction.
- To identify optimal parameters for VR intervention (e.g., content type, session duration, frequency) to guide future implementation and research.
2. Materials and Methods
2.1. PICO Eligibility Criteria
2.2. Study Selection
2.3. Inclusion Criteria
- (1)
- Patients who were scheduled to undergo surgery.
- (2)
- Studies related to anxiety management.
- (3)
- Studies using VR as a means of stress management.
- (4)
- English-language articles.
- (5)
- Full-page articles.
2.4. Exclusion Criteria
- (1)
- Articles studying the VR intervention in children and adolescents.
- (2)
- Articles that did not study VR exclusively (they also included other non-pharmacological interventions such as music therapy, aromatherapy, etc.).
- (3)
- Articles that were diagnostic procedures (not surgeries) in an outpatient office location with or without local anesthesia.
- (4)
- Protocols, feasibility studies, and pilot studies without full outcome data.
- (5)
- Studies that did not report quantifiable anxiety outcomes (i.e., those lacking validated anxiety scales or measurable anxiety data).
2.5. Search Strategy
2.6. Methodological Quality Assessment
3. Results
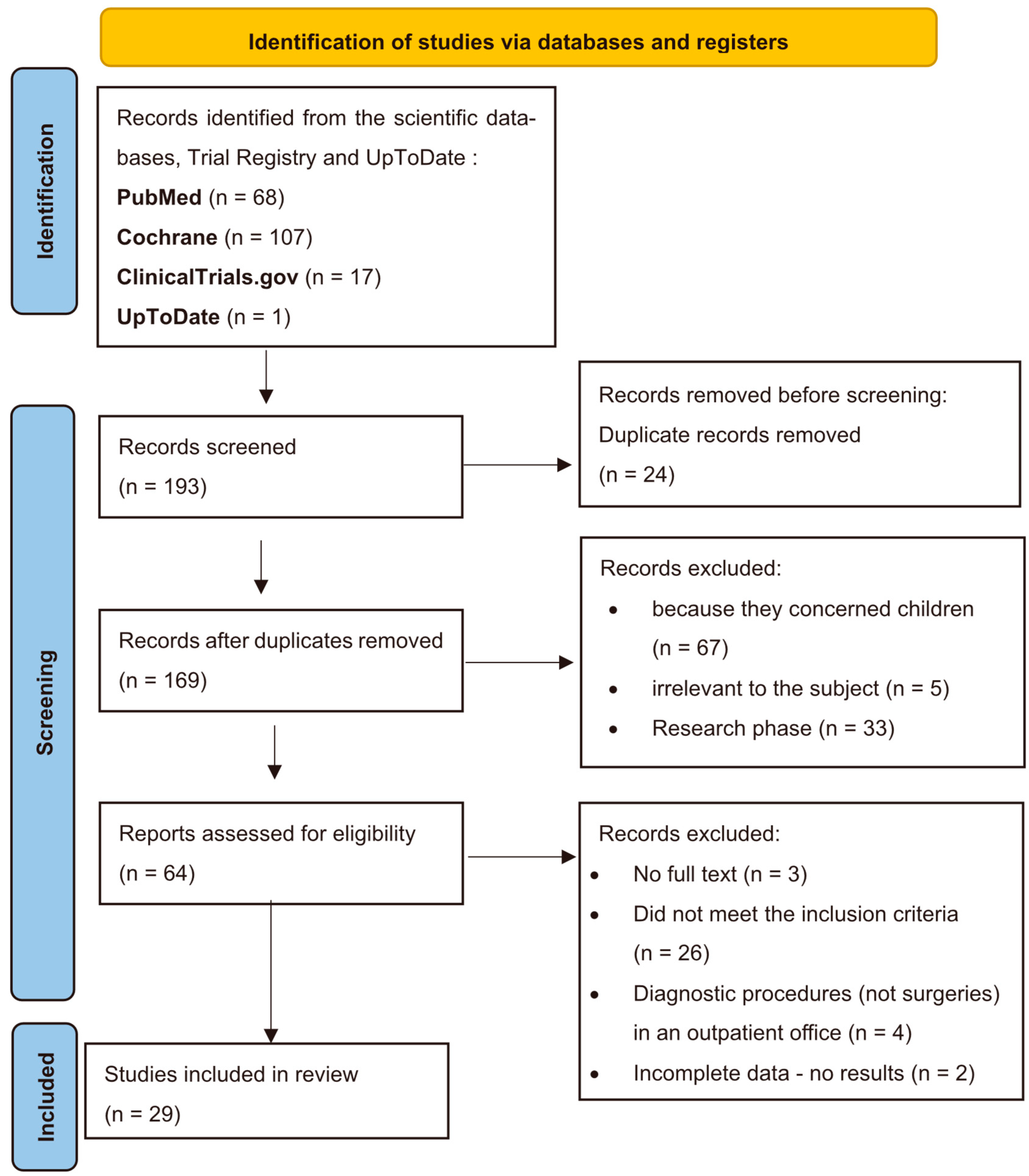
3.1. Study Selection and Measurement Scales
3.2. Characteristics of Included Studies
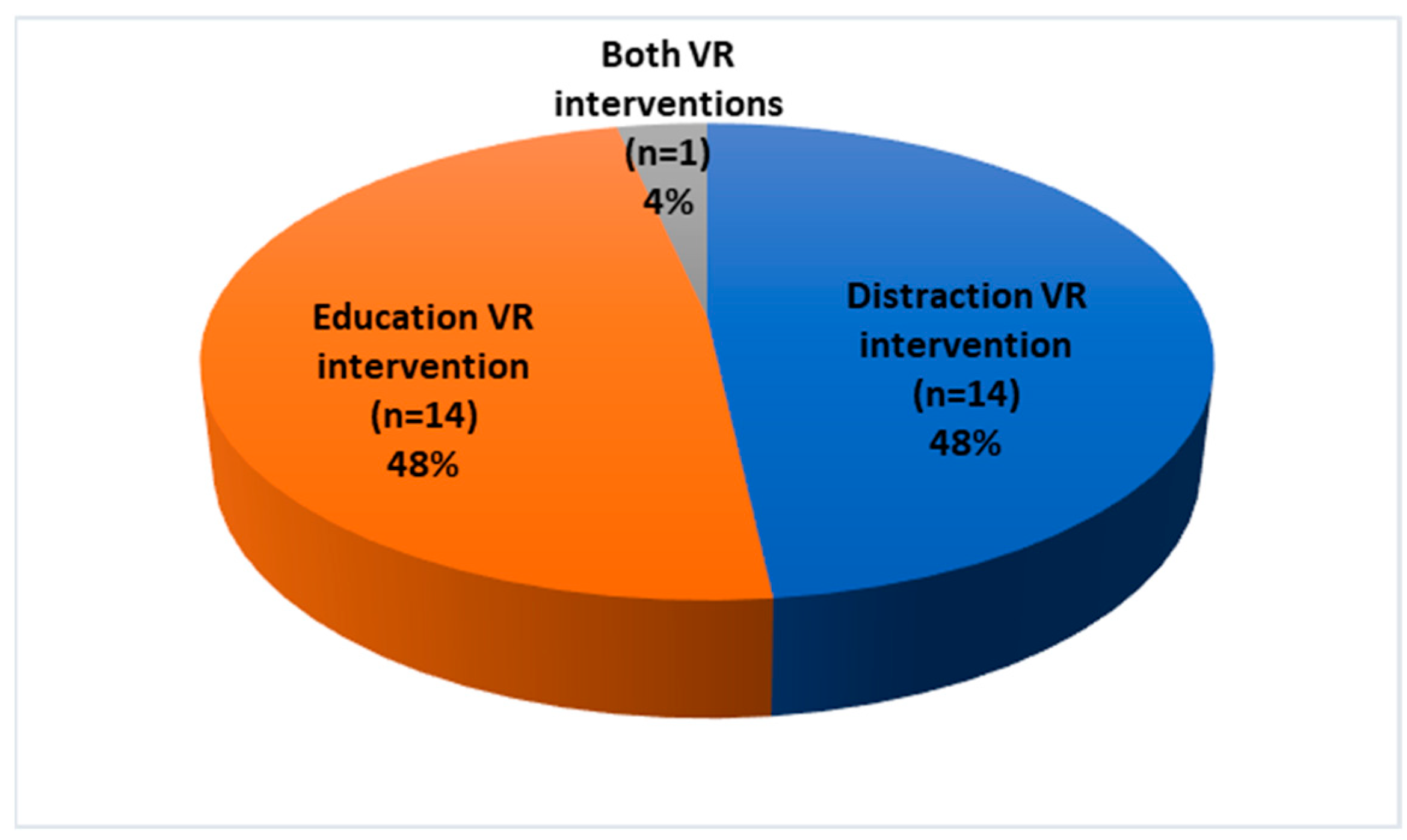
3.3. Type of VR Intervention
3.4. Adverse Effects
3.5. Quality Assessment
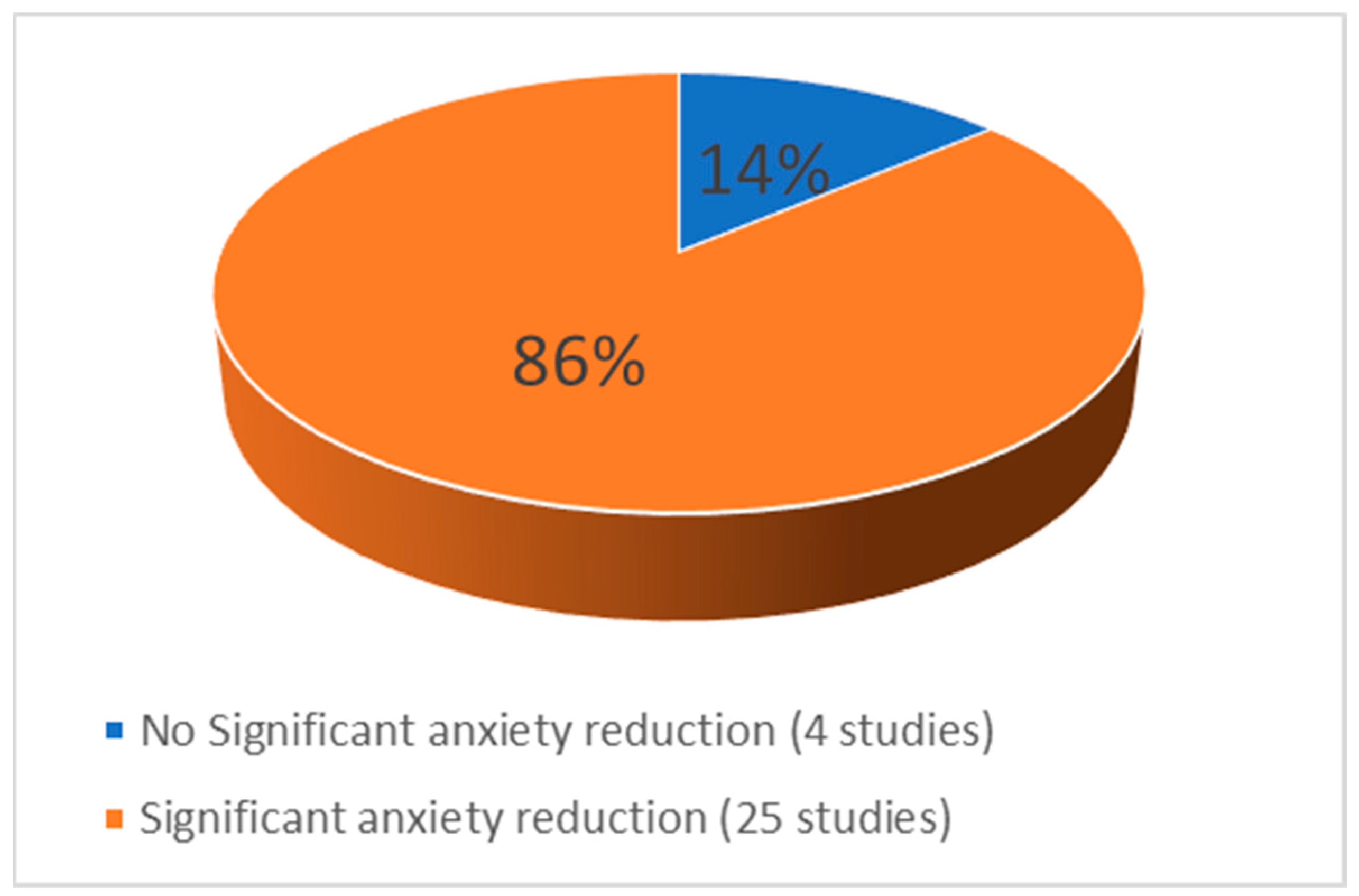
3.6. Effect of VR on Anxiety

{kind=link}
{kind=link}
{kind=link}
| First Author, Country, Year | No of Patients | Scales Used | Intervention Protocol | Type of Surgery | Results | |
|---|---|---|---|---|---|---|
| 1 | El Mathari et al., Netherlands, 2024 [50] [RCT] | 121 patients. Control group (n = 33). VR group (n = 34). | (STAI) (APAIS) | (A) The VR group received educational information in the form of a virtual tour and simulation of the perioperative processes and areas, as well as a 3D animation providing a detailed explanation of the surgical procedure. (B) The control group received standard preoperative care. | Cardiac surgery | There was no difference in the levels of anxiety before surgery between the two groups. The level of satisfaction among patients regarding the information provided was found to be significantly higher among those in the intervention group. |
| 2 | Schmid et al., Australia 2024 [49] [RCT] | 67 patients. Control group (n = 33). VR group (n = 34). | Visual Facial Anxiety Scale (VFAS) | (A) The VR group received standard preoperative care plus 3 min and 34 s of VR educational information through a virtual tour and simulation about the perioperative processes and areas. (B) The control group received standard preoperative care. | Gynecologic oncology Surgeries | Pre-operative anxiety was significantly decreased with VR. The VR intervention reduced anxiety immediately after its administration and also maintained the reduction in fear up until the time of surgery. |
| 3 | Akar et al., Turkey, 2024 [48] [RCT] | 90 patients. Control group (n = 45). VR group (n = 45). | VAS-A SFQ | (A) The VR group watched 6.10 min of VR 360° video with nature sounds. (B) The control group received standard preoperative care. | Open-heart surgery | Nature sounds through VR effectively reduces preoperative surgical fear through SFQ but no statistically significant difference was found between the mean VAS-A scores of the intervention and control groups. |
| 4 | Asiri et al., Australia 2024 [47] [RCT] | 95 patients. Control group (n = 45). VR group (n = 50). | APAIS VAS-A VRSQ VAS-P LPPSQ LOS | (A) The VR group received standard preoperative care plus 10 min of VR nature scenes, sounds, and music. (B) The control group received standard preoperative care. Also, cortisol levels and heart rate were measured. | Elective surgery | Pre-operative anxiety was significantly reduced with VR. However, VR also showed promise in improving postoperative outcomes. |
| 5 | Wang et al., Czech China 2024 [46] [RCT] | 115 patients. Control group (n = 57). VR group (n = 58). | VAS HADS-A HADS-D STAI | (A) The VR group received standard pre-operative care plus 15 min of VR with scenes of nature, sounds, and music. (B) The control group received standard preoperative care. | Laparoscopic gynecology surgery | In female patients undergoing laparoscopic gynecological surgery, VR can reduce preoperative anxiety. |
| 6 | Drozdova et al., Czech Republic 2024 [23] [RCT] | 150 patients—two groups of 75 people. | five-point Likert scale | (A) The VR group watched a 6 min 360° educational video about the procedure. (B) The control group received training from a doctor. | Permanent pacemaker implantation | VR education reduces patient anxiety 92%; it also improves patient understanding levels. |
| 7 | Bidgoli et al., Iran, 2023 [24] | 105 patients—three groups of 35 people. | STAI | (A) In-person group visited the operating theatre for 30 min on the day before surgery. (B) The VR group watched a 30-min virtual tour of the operating room the day before surgery. (C) The control group received standard care. | Hernia, cholecystectomy, appendectomy, cesarean section, hysterectomy, hemorrhoidectomy | There was no significant effect on patients’ preoperative anxiety, nor was there any reduction in anxiety levels before and after the interventions. |
| 8 | Amiri et al., Iran, 2023 [25] | 60 patients—two groups of 30 people. | STAI- | (A) The VR group watched a VR film. (B) The control group watched an ordinary video about the physical area and operating room, the day before the operation. Duration was 4 min and 35 s. | Open-heart surgery | The difference in anxiety levels between the VR and ordinary video groups after the intervention was significant. |
| 9 | Pandrangi et al., Oregon, USA, 2023 [26] [RCT] | 32 patients—two groups of 16 people. | VAS | In Group 1, patients played a preoperative 15 min VR game and received a postoperative VR mindfulness experience, while Group 2 had the same interventions in the reverse order. | Head and neck surgery | Different VR experiences appear to be associated with similar reductions in perioperative anxiety in patients. |
| 10 | Liu Y et al., China, 2023 [27] [RCT] | 114 patients. Control group (n = 57). VR group (n = 57). | SΤA-AI | (A) The VR group received a 16 min training video that informed patients about the procedures and was complemented by a sightseeing experience. (B) The control group used a tablet for viewing. | Carotid artery stenting (CAS) | Patients’ anxiety was reduced in both groups, but more significantly in the VR group. |
| 11 | Rougereau G et al., France, 2023 [28] [RCT] | 60 patients—two groups of 30 people. | STAI | (A) The VR group had a 10 min VR distraction of landscapes (sea, beach, or forest). (B) The control group received routine care. | Hallux valgus surgery | A VR hypnosis mask before surgery modestly reduced postoperative and predischarge anxiety. There was a notable decrease in immediate higher-level postoperative analgesics such as morphine or ketamine. |
| 12 | Grab M et al., Germany, 2023 [29] [RCT] | 99 patients. Control (n = 34). 3D-printed (n = 34). VR (n = 31). | VAS STA SAS TAS | Patient education methods were (A) information via printed leaflet (n = 34), (B) 3D printed models (n = 34), and (C) VR models (n = 31). | Coronary artery surgical aortic valve replacement, thoracic aortic aneurysm surgery, and bypass graft | The use of VR significantly reduced the anxiety and improved the understanding of the procedures. Visualization with 3D VR and 3D models contributed significantly to the result. Also, patient satisfaction with the new interventions was increased. |
| 13 | Kwon H et al., South Korea, 2023 [30] [RCT] | 80 patients—two groups of 40 patients. | APAIS | (A) The VR group received preoperative education about preoperative and postoperative processes and their management. (B) The control group received preoperative education with traditional verbal education. | Reduction of facial bone fracture, corrective rhinoplasty, breast augmentation, skin or soft tissue excision, reconstruction, and burn | Compared to verbal education, patients’ anxiety successfully reduced by VR. The level of satisfaction in the VR group was also higher than that of the control group. |
| 14 | Flores A. et al., Switzerland, 2023 [31] | Case Report—1 woman. | GRSs STAI-Y | The patient spent 10 min with no VR vs. 10 min in VR distraction (the treatment order was randomized). There was a 3 min rest period after the first 10 min intervention. | Laparoscopic cholecystectomy | A 67% lower preoperative anxiety was observed during VR intervention. |
| 15 | Martinez-Bernal D. et al., U.S.A., 2023 [32] | 30 patients (17 female and 13 male). | AIM FIM | Patients watched a VR distraction video for 2 min with natural scenes. | Oral—underwent a maxillofacial surgery | The preoperative use of VR was highly accepted by patients. Pre-operative anxiety appears to be statistically significantly reduced (p = 0.003). |
| 16 | Abbasnia F. et al., Iran, 2023 [33] [RCT] | 150 patients—three groups of 50 people. | STAI | (A) Education group and (B) distraction group received two 5 min VR, 2 hours before and 4 hours after surgery. (C) The control group received standard care. | Laparoscopic cholecystectomy | A significant reduction in pre-operative anxiety observed in VR groups. |
| 17 | Hermans ANL et al., Netherlands, 2023 [34] | 134 patients. Control (n = 66). VR (n = 68). | APAIS | (A) The VR group received educational information according to the procedures and standard preprocedural information. (B) The control group received standard preprocedural information. | Atrial fibrillation (AF) ablation | The VR educational video led to better provision of information and knowledge of patients. An increase in patient satisfaction was also observed and reduced anxiety. |
| 18 | Ugras GA. et al., Turkey, 2023 [35] [RCT] | 86 patients—two groups of 43 people. | ASSQ SBP DBP HR RR SpO2 | (A) The VR group received 10 min of five 3D videos with relaxing music. (B) The control group received standard care. | Colorectal and abdominal wall surgery | Anxiety levels were significantly reduced in the VR group and significantly increased in the control group after standard preoperative care. The VR intervention also reduced psychological and physiological responses to PA. |
| 19 | Chiu et al., China, 2023 [15] [RCT] | 74 patients. | APAIS and VAS | (A) The VR group received an 8 min educational information video through a virtual tour and simulation about the perioperative process. (B) The control group received standard preprocedural information. | General surgery, functional endoscopic sinus surgery, and arthroscopic surgery | The use of VR can be effective in reducing pre-operative anxiety, stress, and preparedness in adult patients undergoing elective surgery. |
| 20 | Aardoom JJ. et al., Netherlands, 2022 [36] | Eight patients—two groups of four people. | PQ ITQ | All patients received VR for 20 min, some at the hospital and some at home. The VR content was educational information through a virtual tour and images related to cardiac catheterization. | Cardiac catheterization | VR was reported to be effective, contributing to stress management and improving patients’ knowledge of the care process. Negative psychological outcomes after the procedure were reduced. |
| 21 | Touil N. et al., Belgium, 2021 [37] | 48 patients. | APAIS APAIS-A and APAIS-S VAS | All patients experienced a VR clinical hypnosis session for 15 min, with suggestions for muscle relaxation and deep breathing under relaxing music. | Elective hand surgery under local anesthesia | The total anxiety score was significantly reduced with VR. |
| 22 | Baytar AD. et al., Turkey, 2021 [38] | 40 patients. | STAI | All patients received VR for 15 m, with distraction content of nature and meditation music. | Septorhinoplasty | There was a significant decrease in preoperative anxiety with VR application. |
| 23 | Turrado V. et al., Spain, 2021 [39] [RCT] | 126 patients—58 exposed and 68 unexposed. | STAI-S HADS | (A) The VR group experienced a realistic environment educative and informative for 16:34 min, which was created in the facilities of the Hospital. (B) The control group received standard information | Colorectal cancer surgery | After exposure, all anxiety/depression rating scales showed a significant decrease. |
| 24 | Turan AZ. et al., Turkey, 2021 [40] [RCT] | 97 patients;—50 patients in the study group and 47 in the control group. | STAI-TA STAI-SA VAS | (A) The VR group, after spinal anesthesia and during the operation, watched a film with VR glasses. (B) The control group, also under spinal anesthesia, followed the standard procedure without VR. | Lower abdominal, anogenital, urologic, and lower extremity surgeries | VR during surgery reduces perioperative anxiety under spinal anesthesia. |
| 25 | Chan JJI. et al., Singapore, 2020 [41] | 108 patients. | HADS | All patients received a 10 min VR intervention consisted of natural scenes, background meditation music, and breathing exercises. | Minor gynecological surgeries | Statistically significant reduction in pre-operative anxiety and depressive symptoms with VR intervention reported. |
| 26 | Hendricks TM. et al., Mayo Clinic in Rochester, Minnesota, U.S.A., 2020 [42] [RCT] | 20 patients. | STAI | (A) The VR group received both interventions for 20 min each. (B) The control group used a tablet-based game application with audiovisual stimulation. | Cardiac surgery | In the VR group, a superior and significant improvement in the feeling of calmness and a significant reduction in the feeling of stress were observed. |
| 27 | Noben L. et al., Netherlands, 2019 [43] [RCT] | 97 women (49 exposed VR and 48 unexposed). | VAS-A SSQ CPS PCQ | (A) The VR group received educational oral information and VR. (B) The control group received standard information from the doctor. | Cesarean Delivery | No significant decrease in VAS-A score in the VR group (n = 49) in comparison to the control group (n = 48). After viewing the VR video, the VR group reported feeling more prepared for the procedure. |
| 28 | Ganry L. et al., France, 2017 [44] | 20 patients (10 men and 10 women) | APAIS. salivatory cortisol heart coherence (HC) | All groups were virtually immersed in nature for 5 min. There was a wide range of themes available for patients to choose from, which are beneficial for relaxation. | Skin cancer surgery | There was a significant reduction in the VAS score after the VR (p < 0.009) as was the level of salivary cortisol (p < 0.04). Cardiac coherence values remained unchanged |
| 29 | Bekelis K. et al., Lebanon, 2017 [45] [RCT] | 127 patients—64 in the VR group and 63 in the control group. | EVAN-G APAIS | (A) The VR group watched a 5 min VR educative video about the preoperative and postoperative experience on the day of the surgery. (B) The control group had routine audiovisual education. In addition, a physician verbally explained the preoperative experience to them. | Elective craniotomy or spine surgery | Patients who were exposed to the VR experience had a higher level of satisfaction during the preparation for surgery. Also, the VR group had less anxiety in the perioperative period. |
| Study | Age (Years) | Pre-Intervention Anxiety (Mean ± SD/Median [IQR]) | Post-Intervention Anxiety (Mean ± SD/Median [IQR]) | Anxiety Rating Scales | p-Value | |
|---|---|---|---|---|---|---|
| 1 | Schmid et al., 2024 [49] | 57.0 ± 13.9 | VR: 3 [2–5]; Control: 4 [2–5] | VR: 2 [2,3]; Control: 4 [3–5] | Visual Facial Anxiety Scale | Statistically significant reduction of anxiety p < 0.001 |
| 2 | Akar et al., 2024 [48] | 63.79 ± 8.26 | VR: 3 [0–7]; Control: 2.2 [0–7.5] | VR: 2 [0–7.5]; Control: 2.9 [0.5–8.2] | VAS-A | No significant difference between the anxiety levels of the study groups (p > 0.05). |
| 3 | Wang et al., 2024 [46] | VR: 37.2 ± 7.2 Control: 38.7 ± 8.3 | VR: 8.38 ± 4.8 Control: 9.74 ± 5.5 | VR: 3.14 ± 3.9 Control: 9.81 ± 6.1 | HADS | Statistically significant reduction of anxiety p < 0.001 |
| 4 | Asiri et al., 2024 [47] | VR: 51 ± 15 Control: 44 ± 18 | VR: 42 (±2.0), 38–46 Control: 59 (±2.1), 55–64 | VR: 22 (±3.9), 14–29 Control: 29 (±3.9), 21–37 | VAS-A | Statistically significant reduction of anxiety p < 0.001 |
| 5 | Drozdova et al., 2024 [23] | 76 (70–83) | Not available numerically. | Anxiety was reduced in 92% of patients (n = 69) | a five-point Likert scale | Not Available |
| 6 | Turrado et al., 2021 [39] | VR: 64 (41–85) Control: 68 (50–86) | HADS VR: 8.00 (7.00; 11.00) Control: 7.00 (6.00–8.00) STAI-S VR: 20.00 (17.00; 24.00) Control: 22.00 (19.00–24.00) | HADS VR: 5.00 (4.00–6.00) Control: Not measured STAI-S VR: 11.50 (7.00–14.00) Control: Not measured | STAI-S, HADS | Statistically significant reduction of anxiety p < 0.001 |
| 7 | Martinez-Bernal et al., 2023 [32] | Not reported (categorical only) | VR: 5.82 | VR: 3.96 | FIM | Statistically significant reduction of anxiety p = 0.003 |
| 8 | Flores et al., 2023 [31] | 44 (case report) | “moderately anxious” (6 out of 10) “strong fear” (rated 8 out of 10) | Reported 67% lower presurgical anxiety during VR. “mildly anxious” during VR (2 of 10) “no fear” (0 of 10) during VR | STAI-Y | Not Available |
| 9 | Grab et al., 2023 [29] | 64.86 ± 10.90 | VAS: 5.00 | VAS: 4.32 (Δ − 0.68) | VAS | Statistically significant reduction of anxiety p < 0.001 |
| 10 | Abbasnia F. et al., 2023 [33] | 43.85 + 11.78 | VR1 distraction 43.04 ± 11.57 VR2 education 43.04 ± 11.57 Control 51.7.8 ± 15.88 | VR1 distraction 34.97 ± 11.37 VR2 education 32.61 ± 9.88 Control 55.21 ± 20.01 | SSAI | Statistically significant reduction of anxiety p < 0.001 |
| 11 | Baytar et al., 2021 [38] | 32.7 ± 8.7 | STAI-S: 41.9 ± 5.7 40.5 (Median) | STAI-S: 35.1 ± 4.8 34 (Median) | STAI-S | Statistically significant reduction of anxiety p < 0.001 |
| 12 | Ugras et al., 2022 [35] | VR: 44.7 ± 12.9 Control: 43.0 ± 15.8 | VR: 30.9 ± 6.8 Control: 29.0 ± 5.8 | VR: 25.1 ± 6.5 Control: 29.7 ± 6.2 | ASSQ | Statistically significant reduction of anxiety p < 0.001 |
| 13 | Chiu et al., 2023 [15] | 46.34 ± 14.52 | VR: 23.92 ± 2.19 Control: 23.03 ± 3.09 | VR: 15.92 ± 4.67 Control: 20.59 ± 4.82 | APAIS | Statistically significant reduction of anxiety p < 0.001 |
| 14 | Amiri et al., 2023 [25] | 56.1 ± 7.6 | VR: 55.8; Control: 58.33 | VR: 38.6; Control: 45.13 | STAI | Statistically significant reduction of anxiety p < 0.001 |
| 15 | Turan et al., 2021 [40] | 43.8 ± 16.41 | STAI-SA VR: 44 ± 10 Control: 42 ± 10 STAI-TA VR: 48.6 ± 6.7 Control: 47.49 ± 7.17 | VR During operation: VAS VR: 4.1 ± 1.91 Control: 5.19 ± 1.64 | STAI, VAS | Statistically significant reduction of anxiety p < 0.003 |
| 16 | Bekelis et al., 2017 [45] | 55.3 ± 14.0 | APAIS-Difference (95% CI) -Stratified on type of operation 29.9 (24.5 to 35.2) | APAIS VR: 90.7 Control: 60.8 VAS 41.7 points lower in the VR group compared to the control group (–41.7 (–33.1 to –50.2)) | APAIS, VAS | Statistically significant reduction of anxiety p < 0.01 |
| 17 | Ganry et al., 2018 [44] | 56.9 | VAS 3.3 before the VR test | VAS 2.85 after the VR test | VAS | Statistically significant reduction of anxiety p < 0.009 |
| 18 | Noben et al., 2019 [43] | 32.6 ± 3.9 | Control group 3.8 [SD 2.3] VR group 4.1 [SD 2.3] | Control group 4.6 (2.5) VR group 5.6 (2.4) | VAS-A | Νo statistically significant difference p = 0.08 |
| 19 | Hendricks et al., 2020 [42] | VR: 69.5 ± 6.9; Control: 63.4 ± 9.1 | STAI-TA VR: 36 ± 6 Control: 33 ± 8 STAI-SA VR: 19 ± 1.7 Control: 20 ± 2.0 | STAI-SA VR: 15 ± 1.3 Control: 17 ± 2.0 | STAI | Statistically significant reduction of anxiety p < 0.05 |
| 20 | Liu et al., 2023 [27] | 64.8 ± 11.3 | STAI-SA VR: 47.9 ± 10.5 Control: 48.9 ± 9.5 STAI-TA VR: 46.7 ± 11.7 Control: 46.9 ± 9.9 | STAI-SA Post-intervention VR: 40.1 ± 7.8 Control: 43.5 ± 8.5 STAI-SA Post-operation VR: 35.0 ± 6.2 Control: 38.3 ± 6.8 | STAI-S, STAI-T | Statistically significant reduction of anxiety Post-intervention p = 0.036 Post-operation p = 0.014 |
| 21 | Pandrangi et al., 2023 [26] | 47.3 ± 16.7 | Group 1 preoperative VR gaming VR: 3 (18.8) Group 2 preoperative VR mindfulness VR: 4 (25.0) | Group 1 postoperative VR mindfulness: −12.0 [15]; Group 2 postoperative VR gaming: −10.5 [13] | VAS-A | Different VR experiences appear to be associated with similar reductions in perioperative anxiety p = 0.62 |
| 22 | Aardoom et al., 2022 [36] | 67 ± 7.5 | Not measured | 4.0 (0.9) (7/8, 88%) reported VR to be effective. Questionnaire ranged from 1 (totally do not agree) to 5 (totally agree) | 5 scaled questionnaire | Not Available |
| 23 | Touil et al., 2021 [37] | Median: 49 (range: 19–76) | APAIS-A VR: 7 (4, 8) VAS anxiety (0–10) VR: 5 (4, 7) | APAIS-A VR: 3 (3, 5) VAS anxiety (0–10) VR: 2 (1, 6) | APAIS, VAS | Statistically significant reduction of anxiety p < 0.001 |
| 24 | Hermans et al., 2023 [34] | Median: 66 (range: 58–72) | VR: 11 (9–14) Control: 9 (6–12) | VR: 13 (19.1%) Control: 27 (40.9%) Less worries in VR (p = 0.006) | APAIS | Statistically significant reduction of anxiety p = 0.006 |
| 25 | Kwon et al., 2023 [30] | 40.75 ± 15.60 | VR: 15.65 ± 1.96 Control: 15.85 ± 1.31 | VR: 7.73 ± 1.52 Control: 13.00 ± 1.16 | APAIS-A | Statistically significant reduction of anxiety p < 0.001 |
| 26 | Chan JJI. et al., 2020 [41] | 43.56 ± 6.68 | 7.2 ± 3.3 | 4.6 ± 3.0 | HADS | Statistically significant reduction of anxiety p < 0.0001 |
| 27 | Rougereau et al., 2023 [28] | 55 ± 13 | VR: 44.3 ± 5.8 Control: 46.3 ± 5.8 | VR: 42.5 ± 9.7 Control: 45.2 ± 7.9 | STAI | Statistically significant reduction of anxiety p < 0.04 |
| 28 | El Mathari et al., 2024 [50] | 67.88 ± 8.56 | STAI (20–80) VR: 38.00 ± 11.99 Control: 39.21 ± 8.76 APAIS VR: 6.00 (4) Control: 6.00 (6) | STAI (20–80) VR: 39.90 ± 11.75 Control: 40.18 ± 9.51 APAIS VR: 5.50 (5) Control: 5.00 (4) | STAI APAIS | Νo statistically significant difference between the two groups (p > 0.05) |
| 29 | Bidgoli et al., 2023 [24] | 40 ± 11 | VR: 54.80 ± 4.63 Control: 55.62 ± 4.89 | VR: 54.48 ± 5.04 Control: 53.42 ± 4.62 | Spielberger’s anxiety questionnaire | Νo statistically significant difference between the two groups (p = 0.10) |
4. Discussion
4.1. Summary of Findings
4.2. Features of Interventions
4.3. Postoperative Pain Management
4.4. Effectiveness of VR on Anxiety
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Acknowledgments
Conflicts of Interest
Abbreviations
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| RCT | Randomized Controlled Trial |
| VR | Virtual Reality |
References
- Weiser, T.G.; Haynes, A.B.; Molina, G.; Lipsitz, S.R.; Esquivel, M.M.; Uribe-Leitz, T.; Fu, R.; Azad, T.; Chao, T.E.; Berry, W.R.; et al. Size and distribution of the global volume of surgery in 2012. Bull. World Health Organ. 2016, 94, 201–209F. [Google Scholar] [CrossRef] [PubMed]
- Stamenkovic, D.M.; Rancic, N.K.; Latas, M.B.; Neskovic, V.; Rondovic, G.M.; Wu, J.D.; Cattano, D. Preoperative anxiety and implications on postoperative recovery: What can we do to change our history. Minerva Anestesiol. 2018, 84, 1307–1317. [Google Scholar] [CrossRef] [PubMed]
- Ki, M.; Kim, D.-C.; You, S.W.; Oh, J.; Jang, J.; Yoo, H.H. Appropriateness of the anxiety subscale of the Hospital Anxiety and Depression Scale for Koreans to measure preoperative anxiety and the effect of preoperative anxiety on postoperative quality of recovery. Anesth. Pain Med. 2023, 18, 260–269. [Google Scholar] [CrossRef]
- Ji, W.; Sang, C.; Zhang, X.; Zhu, K.; Bo, L. Personality, Preoperative Anxiety, and Postoperative Outcomes: A Review. Int. J. Environ. Res. Public. Health 2022, 19, 12162. [Google Scholar] [CrossRef]
- Dibabu, A.M.; Ketema, T.G.; Beyene, M.M.; Belachew, D.Z.; Abocherugn, H.G.; Mohammed, A.S. Preoperative anxiety and associated factors among women admitted for elective obstetric and gynecologic surgery in public hospitals, Southern Ethiopia: A cross-sectional study. BMC Psychiatry 2023, 23, 728. [Google Scholar] [CrossRef]
- Ben-Arye, E.; Segev, Y.; Galil, G.; Marom, I.; Gressel, O.; Stein, N.; Hirsh, I.; Samuels, N.; Schmidt, M.; Schiff, E.; et al. Acupuncture during gynecological oncology surgery: A randomized controlled trial assessing the impact of integrative therapies on perioperative pain and anxiety. Cancer 2023, 129, 908–919. [Google Scholar] [CrossRef]
- El Mathari, S.; Hoekman, A.; Kharbanda, R.K.; Sadeghi, A.H.; Wijngaarden, R.d.L.v.; Götte, M.; Klautz, R.J.; Kluin, J. Virtual Reality for Pain and Anxiety Management in Cardiac Surgery and Interventional Cardiology. JACC Adv. 2024, 3, 100814. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tully, P.J.; Baker, R.A.; Knight, J.L. Anxiety and depression as risk factors for mortality after coronary artery bypass surgery. J. Psychosom. Res. 2008, 64, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Kiecolt-Glaser, J.K.; Page, G.G.; Marucha, P.T.; MacCallum, R.C.; Glaser, R. Psychological Influences on Surgical Recovery: Perspectives from psychoneuroimmunology. Am. Psychol. 1998, 53, 1209–1218. [Google Scholar] [CrossRef] [PubMed]
- Moline, L.R. Patient psychologic preparation for invasive procedures: An integrative review. J. Vasc. Nurs. 2000, 18, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Perks, A.M.; Chakravarti, S.; Manninen, P.M. Preoperative Anxiety in Neurosurgical Patients. J. Neurosurg. Anesthesiol. 2009, 21, 127–130. [Google Scholar] [CrossRef] [PubMed]
- Levandovski, R.; Ferreira, M.B.C.; Hidalgo, M.P.L.; Konrath, C.A.; da Silva, D.L.; Caumo, W. Impact of preoperative anxiolytic on surgical site infection in patients undergoing abdominal hysterectomy. Am. J. Infect. Control. 2008, 36, 718–726. [Google Scholar] [CrossRef] [PubMed]
- Attias, S.; Boker, L.K.; Arnon, Z.; Ben-Arye, E.; Bar’AM, A.; Sroka, G.; Matter, I.; Somri, M.; Schiff, E. Effectiveness of integrating individualized and generic complementary medicine treatments with standard care versus standard care alone for reducing preoperative anxiety. J. Clin. Anesth. 2016, 29, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Duncan, A.E. Hyperglycemia and perioperative glucose management. Curr. Pharm. Des. 2012, 18, 6195–6203. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chiu, P.L.; Li, H.; Yap, K.Y.-L.; Lam, K.-M.C.; Yip, P.-L.R.; Wong, C.L. Virtual Reality–Based Intervention to Reduce Preoperative Anxiety in Adults Undergoing Elective Surgery: A Randomized Clinical Trial. JAMA Netw. Open 2023, 6, e2340588. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ahmadpour, N.; Randall, H.; Choksi, H.; Gao, A.; Vaughan, C.; Poronnik, P. Virtual Reality interventions for acute and chronic pain management. Int. J. Biochem. Cell Biol. 2019, 114, 105568. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Yu, F.; Shi, D.; Shi, J.; Tian, Z.; Yang, J.; Wang, X.; Jiang, Q. Application of virtual reality technology in clinical medicine. Am. J. Transl. Res. 2017, 9, 3867–3880. [Google Scholar] [PubMed] [PubMed Central]
- Anthes, C.; Garcia-Hernandez, R.J.; Wiedemann, M.; Kranzlmuller, D. State of the art of virtual reality technology. In Proceedings of the 2016 IEEE Aerospace Conference, Big Sky, MT, USA, 5–12 March 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 1–19. [Google Scholar] [CrossRef]
- Monash University, Health, Safety and Wellbeing. Safe Use of Immersive Technologies: Virtual Reality (VR), Augmented Reality (AR), Mixed Reality (MR) Guidelines, v1.0 [Internet]. 2022. Available online: http://www.monash.edu.au/ohs/ (accessed on 8 November 2024).
- Palmer, J.A. Decreasing Anxiety Through Patient Education. Plast. Surg. Nurs. 2007, 27, 215–220. [Google Scholar] [CrossRef]
- Atkinson, L.Z.; Cipriani, A. How to carry out a literature search for a systematic review: A practical guide. BJPsych Adv. 2018, 24, 74–82. [Google Scholar] [CrossRef]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef]
- Drozdova, A.; Polokova, K.; Jiravsky, O.; Godula, B.J.; Chovancik, J.; Ranic, I.; Jiravsky, F.; Hecko, J.; Sknouril, L. Comparing Conventional Physician-Led Education with VR Education for Pacemaker Implantation: A Randomized Study. Healthcare 2024, 12, 976. [Google Scholar] [CrossRef]
- Bidgoli, Z.A.; Sadat, Z.; Zarei, M.; Ajorpaz, N.M.; Hosseinian, M. Does a 30-minute introductory visit to the operating room reduce patients’ anxiety before elective surgery? A prospective controlled observational study. Patient Saf. Surg. 2023, 17, 31. [Google Scholar] [CrossRef]
- Amiri, A.; Jalali, R.; Salari, N. The effect of using virtual reality technology on anxiety and vital signs before surgery in patients undergoing open heart surgery. Perioper. Med. 2023, 12, 62. [Google Scholar] [CrossRef] [PubMed]
- Pandrangi, V.C.; Low, G.; Slijepcevic, A.; Shah, S.; Shindo, M.; Schindler, J.; Colaianni, A.; Clayburgh, D.; Andersen, P.; Flint, P.; et al. Use of Perioperative Virtual Reality Experiences on Anxiety and Pain: A Randomized Comparative Trial. Laryngoscope 2024, 134, 1197–1202. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, R.; Zhang, Y.; Feng, L.; Huang, W. Virtual reality psychological intervention helps reduce preoperative anxiety in patients undergoing carotid artery stenting: A single-blind randomized controlled trial. Front. Psychol. 2023, 14, 1193608. [Google Scholar] [CrossRef] [PubMed]
- Rougereau, G.; Sandiford, M.H.; Lévêque, R.; Ménigaux, C.; Bauer, T.; Hardy, A. Management of Anxiety for Ambulatory Hallux Valgus Surgery with a Virtual Reality Hypnosis Mask: Randomized Controlled Trial. Foot Ankle Int. 2023, 44, 539–544. [Google Scholar] [CrossRef]
- Grab, M.; Hundertmark, F.; Thierfelder, N.; Fairchild, M.; Mela, P.; Hagl, C.; Grefen, L. New perspectives in patient education for cardiac surgery using 3D-printing and virtual reality. Front. Cardiovasc. Med. 2023, 10, 1092007. [Google Scholar] [CrossRef]
- Kwon, H.; Lee, J.; Park, Y.S.; Oh, S.-H.; Kim, J. Effects of preoperative education using virtual reality on preoperative anxiety and information desire: A randomized clinical trial. J. Clin. Monit. Comput. 2023, 37, 1401–1407. [Google Scholar] [CrossRef]
- Flores, A.; Hoffman, H.G.; Navarro-Haro, M.V.; Garcia-Palacios, A.; Atzori, B.; Le May, S.; Alhalabi, W.; Sampaio, M.; Fontenot, M.R.; Mason, K.P. Using Immersive Virtual Reality Distraction to Reduce Fear and Anxiety before Surgery. Healthcare 2023, 11, 2697. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Bernal, D.; Cross, W.F.; Hasselberg, M.; Tapparello, C.; Stenz, C.F.H.; Kolokythas, A. A brief virtual reality intervention for pre-operative anxiety in adults. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2023, 137, 209–214. [Google Scholar] [CrossRef]
- Abbasnia, F.; Aghebati, N.; Miri, H.H.; Etezadpour, M. Effects of Patient Education and Distraction Approaches Using Virtual Reality on Pre-operative Anxiety and Post-operative Pain in Patients Undergoing Laparoscopic Cholecystectomy. Pain Manag. Nurs. 2023, 24, 280–288. [Google Scholar] [CrossRef]
- Hermans, A.N.L.; Betz, K.; Verhaert, D.V.M.; Uijl, D.W.D.; Clerx, K.; Debie, L.; Lahaije, M.; Vernooy, K.; Linz, D.; Weijs, B. 360° Virtual reality to improve patient education and reduce anxiety towards atrial fibrillation ablation. EP Eur. 2023, 25, 855–862. [Google Scholar] [CrossRef]
- Ugras, G.A.; Kanat, C.; Yaman, Z.; Yilmaz, M.; Turkmenoglu, M.O. The Effects of Virtual Reality on Preoperative Anxiety in Patients Undergoing Colorectal and Abdominal Wall Surgery: A Randomized Controlled Trial. J. Perianesth. Nurs. 2023, 38, 277–283. [Google Scholar] [CrossRef]
- Aardoom, J.J.; Hilt, A.D.; Woudenberg, T.; Chavannes, N.H.; E Atsma, D. A Preoperative Virtual Reality App for Patients Scheduled for Cardiac Catheterization: Pre–Post Questionnaire Study Examining Feasibility, Usability, and Acceptability. JMIR Cardio 2022, 6, e29473. [Google Scholar] [CrossRef] [PubMed]
- Touil, N.; Pavlopoulou, A.; Momeni, M.; Van Pee, B.; Barbier, O.; Sermeus, L.; Roelants, F. Evaluation of virtual reality combining music and a hypnosis session to reduce anxiety before hand surgery under axillary plexus block: A prospective study. Int. J. Clin. Pract. 2021, 75, e15008. [Google Scholar] [CrossRef]
- Baytar, Ç.; Bollucuoğlu, K. Effect of virtual reality on preoperative anxiety in patients undergoing septorhinoplasty. Braz. J. Anesthesiol. 2023, 73, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Turrado, V.; Guzmán, Y.; Jiménez-Lillo, J.; Villegas, E.; De Lacy, F.B.; Blanch, J.; Balibrea, J.M.; Lacy, A. Exposure to virtual reality as a tool to reduce peri-operative anxiety in patients undergoing colorectal cancer surgery: A single-center prospective randomized clinical trial. Surg. Endosc. 2021, 35, 4042–4047. [Google Scholar] [CrossRef]
- Turan, A.Z.; Yilmaz, M.; Saracoglu, T. The effect of virtual reality glasses on anxiety during surgery under spinal anesthesia: A randomized controlled study. Anaesth. Pain Intensive Care 2021, 25, 170–175. [Google Scholar] [CrossRef]
- Chan, J.J.I.; Yeam, C.T.; Kee, H.M.; Tan, C.W.; Sultana, R.; Sia, A.T.H.; Sng, B.L. The use of pre-operative virtual reality to reduce anxiety in women undergoing gynecological surgeries: A prospective cohort study. BMC Anesthesiol. 2020, 20, 261. [Google Scholar] [CrossRef]
- Hendricks, T.M.; Gutierrez, C.N.; Stulak, J.M.; Dearani, J.A.; Miller, J.D. The Use of Virtual Reality to Reduce Preoperative Anxiety in First-Time Sternotomy Patients: A Randomized Controlled Pilot Trial. Mayo Clin. Proc. 2020, 95, 1148–1157. [Google Scholar] [CrossRef]
- Noben, L.; Goossens, S.M.T.A.; Truijens, S.E.M.; Van Berckel, M.M.G.; Perquin, C.W.; Slooter, G.D.; Van Rooijen, S.J. A Virtual Reality Video to Improve Information Provision and Reduce Anxiety Before Cesarean Delivery: Randomized Controlled Trial. JMIR Ment. Health 2019, 6, e15872. [Google Scholar] [CrossRef] [PubMed]
- Ganry, L.; Hersant, B.; Sidahmed-Mezi, M.; Dhonneur, G.; Meningaud, J.P. Using virtual reality to control preoperative anxiety in ambulatory surgery patients: A pilot study in maxillofacial and plastic surgery. J. Stomatol. Oral Maxillofac. Surg. 2018, 119, 257–261. [Google Scholar] [CrossRef]
- Bekelis, K.; Calnan, D.; Simmons, N.; MacKenzie, T.A.; Kakoulides, G. Effect of an Immersive Preoperative Virtual Reality Experience on Patient Reported Outcomes: A Randomized Controlled Trial. Ann. Surg. 2017, 265, 1068–1073. [Google Scholar] [CrossRef]
- Wang, Y.; Sun, J.; Yu, K.; Liu, X.; Liu, L.; Miao, H.; Li, T. Virtual reality exposure reduce acute postoperative pain in female patients undergoing laparoscopic gynecology surgery: A Randomized Control Trial (RCT) study. J. Clin. Anesth. 2024, 97, 111525. [Google Scholar] [CrossRef] [PubMed]
- Asiri, S.; Guilhermino, M.; Duff, J.; Currie, J.; Guilhermino, M. The Effectiveness of Virtual Reality Technology for Perioperative Anxiety Among Adults Undergoing Elective Surgery. Ph.D. Thesis, Queensland University of Technology, Brisbane, Australia, March 2024. [Google Scholar] [CrossRef]
- Akar, T.E.; Ünver, S. Effectiveness of Virtual Reality Glasses on Surgical Fear and Anxiety in Patients Before Open-heart Surgery: A Double-blind Randomized Controlled Trial. J. Perianesth. Nurs. 2024, 40, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Schmid, B.C.; Marsland, D.; Jacobs, E.; Rezniczek, G.A. A Preparatory Virtual Reality Experience Reduces Anxiety before Surgery in Gynecologic Oncology Patients: A Randomized Controlled Trial. Cancers 2024, 16, 1913. [Google Scholar] [CrossRef] [PubMed Central]
- El Mathari, S.; Kuitert, L.; Boulidam, N.; Shehadeh, S.; Klautz, R.J.M.; de Lind van Wijngaarden, R.; Kluin, J. Evaluating Virtual Reality Patient Education in Cardiac Surgery: Impact on Preoperative Anxiety and Postoperative Patient Satisfaction. J. Clin. Med. 2024, 13, 6567. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wu, J.; Yan, J.; Zhang, L.; Chen, J.; Cheng, Y.; Wang, Y.; Zhu, M.; Cheng, L.; Zhang, L. The effectiveness of distraction as preoperative anxiety management technique in pediatric patients: A systematic review and meta-analysis of randomized controlled trials. Int. J. Nurs. Stud. 2022, 130, 104232. [Google Scholar] [CrossRef]
- Koo, C.-H.; Park, J.-W.; Ryu, J.-H.; Han, S.-H. The Effect of Virtual Reality on Preoperative Anxiety: A Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2020, 9, 3151. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Caumo, W.; Schmidt, A.P.; Schneider, C.N.; Bergmann, J.; Iwamoto, C.W.; Bandeira, D.; Ferreira, M.B.C. Risk factors for preoperative anxiety in adults. Acta. Anaesthesiol Scand. 2001, 45, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.L.; Sit, J.W.H.; Ang, W.W.; Lau, Y. Virtual reality-enhanced interventions on preoperative anxiety symptoms in adults undergoing elective surgery: A meta-analysis and meta-regression. Int. J. Nurs. Stud. 2024, 160, 104886. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Wang, N.; Liu, N. Effectiveness of virtual reality in reducing preoperative anxiety in adults: A systematic review and meta-analysis. J. Adv. Nurs. 2023, 79, 3678–3690. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S.; Folkman, S. Transactional theory and research on emotions and coping. Eur. J. Personal. 1987, 1, 141–169. [Google Scholar] [CrossRef]
- Deveugele, M.; Derese, A.; van den Brink-Muinen, A.; Bensing, J.; De Maeseneer, J. Consultation length in general practice: Cross sectional study in six European countries. BMJ 2022, 325, 472. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Xu, H.; Hou, J.; Zhou, J.; Wang, S. Effects of Virtual Reality on Preoperative Anxiety in Adult Patients: An Updated Meta-analysis. J. Perianesth Nurs. 2024, 40, 422–430. [Google Scholar] [CrossRef] [PubMed]
- El-Gabalawy, R.; Sommer, J.L.; Hebbard, P.; Reynolds, K.; Logan, G.S.; Smith, M.S.D.; Mutter, T.C.; Mutch, W.A.; Mota, N.; Proulx, C.; et al. An Immersive Virtual Reality Intervention for Preoperative Anxiety and Distress Among Adults Undergoing Oncological Surgery: Protocol for a 3-Phase Development and Feasibility Trial. JMIR Res. Protoc. 2024, 13, e55692. [Google Scholar] [CrossRef]
- Ding, L.; Hua, H.; Zhu, H.; Zhu, S.; Lu, J.; Zhao, K.; Xu, Q. Effects of virtual reality on relieving postoperative pain in surgical patients: A systematic review and meta-analysis. Int. J. Surg. 2020, 82, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Bayrak, A.; Sagiroglu, G.; Copuroglu, E. Effects of Preoperative Anxiety on Intraoperative Hemodynamics and Postoperative Pain. J. Coll. Phys. Surg. Pak. 2019, 29, 868–873. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-Y.K.; Soens, M.A.; Kovacheva, V.P. Less stress, better success: A scoping review on the effects of anxiety on anesthetic and analgesic consumption. J. Anesth. 2022, 36, 532–553. [Google Scholar] [CrossRef] [PubMed]
- Agüero-Millan, B.; Abajas-Bustillo, R.; Ortego-Maté, C. Efficacy of nonpharmacologic interventions in preoperative anxiety: A systematic review of systematic reviews. J. Clin. Nurs. 2023, 32, 6229–6242. [Google Scholar] [CrossRef] [PubMed]
| Assessment Criteria | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All Studies | Quant. Randomized Controlled Trials | Quant. Non -Randomized Controlled Trials | |||||||||||||||
| Author | Study Type | S1. Are There Clear Research Questions? | S2. Do the Collected Data Allow to Address the Research Questions? | 2.1. Is Randomization Appropriately Performed? | 2.2. Are the Groups Comparable at Baseline? | 2.3. Are There Complete Outcome Data? | 2.4. Are Outcome Assessors Blinded to the Intervention Provided? | 2.5 Did the Participants Adhere to the Assigned Intervention? | 3.1. Are the Participants Representative of the Target Population? | 3.2. Are Measurements Appropriate Regarding Both the Outcome and Intervention (or Exposure)? | 3.3. Are There Complete Outcome Data? | 3.4. Are the Confounders Accounted for in the Design and Analysis? | 3.5. During the Study Period, is the Intervention Administered (or Exposure Occurred) as Intended? | Total Metrics | Score % | Risk of Bias | |
| 1 | Drozdova et al. [23] | RCT | Y | Y | Y | Y | Y | N | Y | 4/5 | 80% | Moderate | |||||
| 2 | Bidgoli et al. [24] | Quant non-RCT | Y | Y | Y | Y | Y | CT | Y | 4/5 | 80% | Moderate | |||||
| 3 | Amiri et al. [25] | Quant non-RCT | Y | Y | Y | Y | Y | N | Y | 4/5 | 80% | Moderate | |||||
| 4 | Pandrangi et al. [26] | RCT | Y | Y | Y | Y | Y | CT | Y | 4/5 | 80% | Moderate | |||||
| 5 | Liu Y et al. [27] | RCT | Y | Y | Y | Y | Y | Y | Y | 5/5 | 100% | Low | |||||
| 6 | Rougereau G et al. [28] | RCT | Y | Y | Y | Y | Y | N | Y | 4/5 | 80% | Moderate | |||||
| 7 | Grab M et al. [29] | RCT | Y | Y | CT | Y | Y | Y | Y | 4/5 | 80% | Moderate | |||||
| 8 | Kwon H et al. [30] | RCT | Y | Y | Y | Y | Y | Y | Y | 5/5 | 100% | Low | |||||
| 9 | Flores A. et al. [31] | Case Report | Y | Y | Y | Y | CT | CT | Y | 3/5 | 60% | Moderate | |||||
| 10 | Martinez-Bernal D. [32] | Quant non-RCT | Y | Y | Y | Y | Y | CT | Y | 4/5 | 80% | Moderate | |||||
| 11 | Abbasnia F. et al. [33] | RCT | Y | Y | Y | Y | Y | Y | Y | 4/5 | 80% | Moderate | |||||
| 12 | Hermans ANL et al. [34] | Quant non-RCT | Y | Y | Y | Y | Y | CT | Y | 4/5 | 80% | Moderate | |||||
| 13 | Ugras GA. et al. [35] | RCT | Y | Y | Y | Y | Y | CT | Y | 4/5 | 80% | Moderate | |||||
| 14 | Chiu et al. [15] | RCT | Y | Y | Y | Y | Y | Y | Y | 5/5 | 100% | Low | |||||
| 15 | Aardoom JJ. et al. [36] | Quanti. Descr. | Y | Y | Y | Y | N | N | Y | 3/5 | 60% | Moderate | |||||
| 16 | Touil N. et al. [37] | Quant non-RCT | Y | Y | Y | Y | Y | CT | Y | 4/5 | 80% | Moderate | |||||
| 17 | Baytar AD. et al. [38] | Quant non-RCT | Y | Y | Y | Y | Y | CT | Y | 4/5 | 80% | Moderate | |||||
| 18 | Turrado V. et al. [39] | RCT | Y | Y | Y | Y | Y | N | Y | 4/5 | 80% | Moderate | |||||
| 19 | Turan AZ. et al. [40] | RCT | Y | Y | Y | Y | Y | N | Y | 4/5 | 80% | Moderate | |||||
| 20 | Chan JJI. et al. [41] | Quant non-RCT | Y | Y | Y | Y | Y | CT | Y | 4/5 | 80% | Moderate | |||||
| 21 | Hendricks et al. [42] | RCT | Y | Y | Y | Y | Y | CT | Y | 5/5 | 80% | Moderate | |||||
| 22 | Noben L. et al. [43] | RCT | Y | Y | Y | Y | Y | N | Y | 4/5 | 80% | Moderate | |||||
| 23 | Ganry L. et al. [44] | Quant non-RCT | Y | Y | Y | Y | Y | CT | Y | 4/5 | 80% | Moderate | |||||
| 24 | Bekelis K. et al. [45] | RCT | Y | Y | Y | Y | Y | N | Y | 4/5 | 80% | Moderate | |||||
| 25 | Wang Y et al. [46] | RCT | Y | Y | Y | Y | Y | N | Y | 4/5 | 80% | Moderate | |||||
| 26 | Asiri et al. [47] | RCT | Y | Y | Y | Y | Y | N | Y | 4/5 | 80% | Moderate | |||||
| 27 | Akar et al. [48] | RCT | Y | Y | Y | Y | Y | Y | Y | 5/5 | 100% | Low | |||||
| 28 | Schmid et al. [49] | RCT | Y | Y | Y | Y | Y | N | Y | 4/5 | 80% | Moderate | |||||
| 29 | El Mathari et al. [50] | RCT | Y | Y | Y | Y | Y | N | Y | 4/5 | 80% | Moderate | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alimonaki, E.C.; Bothou, A.; Diamanti, A.; Deltsidou, A.; Paliatsiou, S.; Karampas, G.; Kyrkou, G. Management of Preoperative Anxiety via Virtual Reality Technology: A Systematic Review. Nurs. Rep. 2025, 15, 268. https://doi.org/10.3390/nursrep15080268
Alimonaki EC, Bothou A, Diamanti A, Deltsidou A, Paliatsiou S, Karampas G, Kyrkou G. Management of Preoperative Anxiety via Virtual Reality Technology: A Systematic Review. Nursing Reports. 2025; 15(8):268. https://doi.org/10.3390/nursrep15080268
Chicago/Turabian StyleAlimonaki, Elina Christiana, Anastasia Bothou, Athina Diamanti, Anna Deltsidou, Styliani Paliatsiou, Grigorios Karampas, and Giannoula Kyrkou. 2025. "Management of Preoperative Anxiety via Virtual Reality Technology: A Systematic Review" Nursing Reports 15, no. 8: 268. https://doi.org/10.3390/nursrep15080268
APA StyleAlimonaki, E. C., Bothou, A., Diamanti, A., Deltsidou, A., Paliatsiou, S., Karampas, G., & Kyrkou, G. (2025). Management of Preoperative Anxiety via Virtual Reality Technology: A Systematic Review. Nursing Reports, 15(8), 268. https://doi.org/10.3390/nursrep15080268